
Abstract
Background
Mothers of high-risk neonates often experience reduced confidence, challenges in role adaptation, and lower satisfaction with neonatal care, which may influence maternal well-being and caregiving practices.
Review Question
What is the effectiveness of interventions in improving maternal psychosocial and caregiving outcomes?
Methods
A systematic search was conducted across five electronic databases for articles published from January 2020 through December 2024. Studies eligible for inclusion were randomised controlled trials (RCTs) and quasi-experimental designs focusing on maternal psychosocial and caregiving outcomes. Methodological quality was assessed using the Cochrane Risk of Bias (RoB-2) tool for RCTs and the Joanna Briggs Institute (JBI) checklist for non-RCTs. Due to heterogeneity in intervention types and outcome measures, a narrative synthesis approach was adopted.
Results
A total of 22 studies were included. Interventions were categorized into family-centered care, educational programs, digital health strategies, and home-based or follow-up interventions. Commonly assessed outcomes included maternal self-efficacy, role adaptation, readiness for discharge, resilience, and satisfaction in care. Although many studies reported improvements in maternal outcomes, there was considerable variability in intervention components, duration, delivery methods, and measurement tools. Methodological quality also varied across studies, and the evidence was geographically concentrated, which may limit generalizability.
Conclusion
Interventions showed potential to support maternal outcomes in high-risk neonatal care; however, inconsistencies in design and measurement limit definitive conclusions.
Keywords
Implications for Practice, Education, or Research
Integrating structured, context-sensitive interventions into NICU care, along with standardized outcome measures and rigorous, diverse research is essential for strengthening maternal support across settings.
High-risk neonates, including preterm and low birth weight infants, contribute substantially to global morbidity and mortality, placing significant short- and long-term burdens on individuals, families, communities, and the health-care system (Berhane et al., 2019). The hospitalization of these neonates in the Neonatal Intensive Care Unit (NICU) exposes parents, particularly mothers, to considerable psychological distress, including stress, fear, and depression. These challenges are often exacerbated by environmental stressors, limited health literacy, and inadequate communication with health-care providers (Siva et al., 2023a). Such experiences can adversely affect early parent–infant interactions, which are critical for neonatal growth and emotional and social development (Siva et al., 2025a). Moreover, prolonged exposure to these stressors may predispose parents to long-term psychological conditions such as anxiety, depression, and disruptions in parenting patterns (Khanjari et al., 2021; Siva et al., 2024a).
In this context, enhancing maternal involvement in neonatal care within the NICU has emerged as a crucial strategy to improve maternal self-efficacy and facilitate adaptation to the maternal role (Pouyan et al., 2019; Sohrabi et al., 2021). Maternal confidence and role adaptation during early motherhood are increasingly recognized as essential components of neonatal care (Khalesi et al., 2021; Lorié et al., 2021; Sohrabi et al., 2021). The process of maternal role adaptation is influenced by both individual factors such as emotional distress, self-efficacy, interaction, and isolation, and social factors, including support systems and societal attitudes (Heydarpour et al., 2022). Mothers who demonstrate higher levels of confidence, resilience, and active participation in neonatal care are better positioned to provide emotional support, thereby contributing to improved clinical and developmental outcomes in neonates (Wang et al., 2021).
However, in many low- and middle-income countries (LMICs), institutional policies often limit parental access to NICUs, restricting maternal involvement in neonatal care and negatively impacting maternal well-being and role adaptation (Lorié et al., 2021). Facilitating flexible visitation and encouraging active maternal participation in neonatal care practices can enhance maternal role adaptation and promote positive caregiving behaviors (Heydarpour et al., 2022; Wang et al., 2021). Additionally, such approaches foster better communication between mothers and health-care providers, enabling a clearer understanding of the neonate's condition and improving overall family functioning (Askary Kachoosangy et al., 2020). Empowering mothers through education and information regarding neonatal care further strengthens their ability to make informed decisions and actively engage in caregiving (Siva et al., 2025a, 2026). Health-care providers play a pivotal role in this process by promoting maternal health literacy, psychological well-being, and mother–infant bonding, ultimately supporting neonatal recovery within the NICU (Orr et al., 2023; Siva et al., 2023b). A range of health-care interventions has been developed globally to support mothers and improve maternal and neonatal outcomes across the continuum of care (Siva et al., 2025a, 2026).
Although existing literature on maternal support interventions has expanded considerably, a comprehensive and methodologically rigorous synthesis of their effectiveness is still lacking. This review aims to evaluate the influence of health-care interventions on a range of maternal psychosocial and caregiving outcomes, including self-efficacy, confidence, readiness for discharge, resilience, quality of life, sense of coherence, breastfeeding self-efficacy, maternal role adaptation, and satisfaction among mothers of high-risk neonates. By synthesizing the available evidence, the review seeks to provide insights that can support clinical decision-making, inform policy development, and guide future research on maternal support interventions in high-risk neonatal care settings.
Methods
Research Question
The review is guided by the following research question: What is the effectiveness of interventions in improving maternal psychosocial and caregiving outcomes among mothers of high-risk neonates? Specifically, the review examines outcomes related to maternal self-efficacy, confidence, readiness for discharge, resilience, quality of life, sense of coherence, breastfeeding self-efficacy, maternal role adaptation, and satisfaction. This question was formulated to capture the multidimensional nature of maternal experiences during neonatal hospitalization and the transition to home care, encompassing psychological well-being, caregiving competence, and adaptation to the maternal role.
Design
This systematic review with narrative synthesis was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (see Supplemental File 1).
Eligibility Criteria
The eligibility criteria for this systematic review were developed using the Population, Intervention, Comparison, and Outcome (PICO) framework (Cochrane Library, 2000) to ensure clarity and methodological rigor.
Population (P): The population of interest included mothers of high-risk neonates admitted to or discharged from NICUs. For this review, high-risk neonates were defined as infants requiring specialized neonatal care due to prematurity, low birth weight, congenital anomalies, birth complications, respiratory distress, medical instability, or other conditions necessitating admission to a NICU. Mothers were included regardless of age, parity, type of delivery, or sociodemographic characteristics. Studies involving neonates admitted only for short-term observation (≤24 h) were excluded, as they did not reflect prolonged NICU exposure. Additionally, mothers diagnosed with prenatal or postnatal psychiatric illnesses, including postnatal depression, were excluded to minimize potential confounding when assessing maternal psychosocial and caregiving outcomes.
Intervention (I): The interventions included in this review comprised non-pharmacological strategies aimed at supporting mothers of high-risk neonates. These interventions included family-centered care, educational and training programs, digital or mobile health (mHealth) interventions, home-based care, home visits, continuity-of-care programs, discharge planning interventions, and follow-up support initiatives designed to enhance maternal involvement in neonatal care.
Comparator (C): Comparator groups consisted of standard or routine care, usual discharge practices, or alternative intervention approaches, where applicable.
Outcomes (O): The primary outcomes of interest were maternal psychosocial and caregiving outcomes, including maternal self-efficacy, confidence, readiness for discharge, sense of competence, resilience, sense of coherence, maternal role adaptation, and satisfaction with neonatal care.
Studies focusing exclusively on paternal outcomes or other family members were excluded to maintain conceptual clarity. Only full-text articles published in English between January 2010 and December 2024 were included. Eligible study designs comprised RCTs, quasi-experimental studies, and other interventional studies with comparison groups. Observational, qualitative, mixed-methods studies, and non-research articles were excluded to ensure a focus on intervention effectiveness.
Search Strategy
A comprehensive and systematic search strategy was developed to identify studies relevant to the review objectives. Guided by the PICO framework, the search incorporated both controlled vocabulary and free-text terms related to high-risk neonates, preterm infants, NICUs, maternal support interventions, self-efficacy, maternal role adaptation, readiness for discharge, resilience, confidence, and satisfaction. Search terms were combined using Boolean operators (AND, OR) and adapted to each database's indexing requirements to maximize search sensitivity and specificity. The electronic databases searched were Cumulated Index in Nursing and Allied Health Literature (CINAHL) (via EBSCOhost), MEDLINE (via PubMed), Scopus, Web of Science, and ProQuest Medical Library. The search covered studies published from January 2010 to December 2024, with the final search conducted in December 2024. The complete search strategy for each database is provided in Supplemental File 2.
In addition to database searching, forward and backward citation tracking of all included studies was undertaken to identify potentially relevant articles not captured through the electronic searches. Grey literature sources and clinical trial registries were not searched. Only studies published in English were included, which may have introduced language bias. These limitations have been acknowledged in the discussion of the review limitations.
Selection Process
All records identified through the search strategy were imported into Rayyan software, which facilitated efficient management of references and removal of duplicate records. The study selection process was conducted in two stages to ensure methodological rigor. In the first stage, two independent reviewers (NS and BV) screened titles and abstracts against the predefined eligibility criteria to identify potentially relevant studies. In the second stage, full-text articles of selected studies were retrieved and assessed independently by the same reviewers. Reasons for exclusion at the full-text stage were documented systematically to ensure transparency and reproducibility of the selection process. Any discrepancies or disagreements between reviewers were resolved through discussion. If consensus could not be reached, a third reviewer (BSN) was consulted to make the final decision.
Quality Assessment
The methodological quality and risk of bias of the included studies were assessed using standardized and validated appraisal tools. RCTs were evaluated using the Cochrane Collaboration's Risk of Bias 2 (RoB-2) tool (Higgins et al., 2011), while non-RCTs were assessed using the Joanna Briggs Institute (JBI) Critical Appraisal Checklist (Munn et al., 2020). These tools assess multiple domains, including selection bias, performance bias, detection bias, attrition bias, and reporting bias. Additionally, aspects such as the validity and reliability of outcome measurement, identification and control of confounding factors, and appropriateness of statistical analyses were evaluated. Two reviewers (NS and BV) independently conducted the quality assessment to ensure objectivity. Any disagreements were resolved through discussion or consultation with a third reviewer (BSN). The results of the quality assessment were used to interpret the strength and reliability of the evidence, but did not serve as exclusion criteria unless studies were found to be methodologically unsound.
Data Extraction
A structured and pre-tested data extraction form was developed to systematically capture relevant information from each included study. Extracted data included study characteristics such as authors, year of publication, country, study design, sample size, and setting. In addition, detailed information on the type of intervention, duration, delivery method, and comparison groups was recorded.
Outcome-related data focused on maternal psychosocial and caregiving outcomes, including maternal self-efficacy, confidence, readiness for discharge, resilience, quality of life, sense of coherence, breastfeeding self-efficacy, maternal role adaptation, satisfaction, and other related indicators of maternal well-being and caregiving competence. The extracted data were further categorized into thematic domains, including intervention characteristics, maternal outcomes, and contextual or environmental factors influencing effectiveness. Data extraction was performed independently by two reviewers (NS and BV) to ensure accuracy and consistency. One reviewer conducted the primary extraction, while the second reviewer cross-checked the extracted data for completeness and correctness.
Data Synthesis
Due to substantial heterogeneity in study designs, intervention characteristics, outcome measures, and assessment instruments, statistical pooling through meta-analysis was not feasible. Therefore, a narrative synthesis approach was employed to systematically summarize, compare, and interpret the findings across studies. The synthesis focused on examining patterns in intervention characteristics and their influence on maternal psychosocial and caregiving outcomes, including self-efficacy, confidence, readiness for discharge, resilience, quality of life, sense of coherence, breastfeeding self-efficacy, maternal role adaptation, and satisfaction. Findings were organized according to intervention type and outcome domains to facilitate a comprehensive understanding of the available evidence and identify areas requiring further research.
Results
Study Selection
The systematic search across five electronic databases identified 815 records. After removal of 176 duplicates, 639 records remained for title and abstract screening. Following this screening, 58 articles were identified as potentially eligible for full-text review. However, full-text reports for four articles could not be retrieved despite repeated attempts through available library resources. Consequently, 54 full-text articles were assessed for eligibility. Of these, 32 articles were excluded for not meeting the predefined inclusion criteria. Ultimately, 22 studies, comprising a total sample of 3,475 participants, were included in the narrative synthesis. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Page et al., 2021) study selection process is presented in Figure 1.

PRISMA flow chart of study selection.
Study Characteristics
The included studies were conducted across diverse geographical settings. A majority were from Iran (n = 11), followed by the United States (n = 5), South Korea (n = 2), and one study each from Finland, China, Turkey, and Thailand. This distribution reflects a concentration of evidence from specific regions, particularly middle-income countries, with relatively limited representation from other global contexts. In terms of methodological design, the evidence base predominantly consisted of quasi-experimental studies (n = 12), followed by RCTs (n = 5). Additionally, four studies employed pre–post intervention designs, and one study utilized a three-group experimental approach. These variations highlight heterogeneity in methodological rigor and study design across the included literature. Detailed study characteristics are reported in Supplemental File 3.
Sample Characteristics
The included studies demonstrated variability in both neonatal and maternal characteristics. Neonatal participants primarily ranged between 27.4 and 43 weeks of gestational age, with birth weights spanning from 1135 to 5380 grams. Maternal age ranged from 18 to 44 years, indicating representation across a wide reproductive age group. Educational status varied considerably across settings. In low- and middle-income contexts such as Iran, 40% to 68% of mothers had completed high school education, whereas studies conducted in developed countries reported that approximately 60% of mothers had attained education beyond diploma or graduation levels.
Regarding obstetric characteristics, a notable proportion of participants were first-time mothers, with 54% to 56% identified as primigravida and around 15% as primiparous. Occupational status indicated that approximately 52% of mothers were self-employed, while 48% were homemakers. A subset of studies also reported NICU stay durations, which ranged from 7 to 10 days.
Types of Interventions
The included studies implemented a wide range of non-pharmacological interventions, which were categorized into four major groups based on their nature and delivery approach. A detailed description of individual interventions is provided in Supplemental File 4.
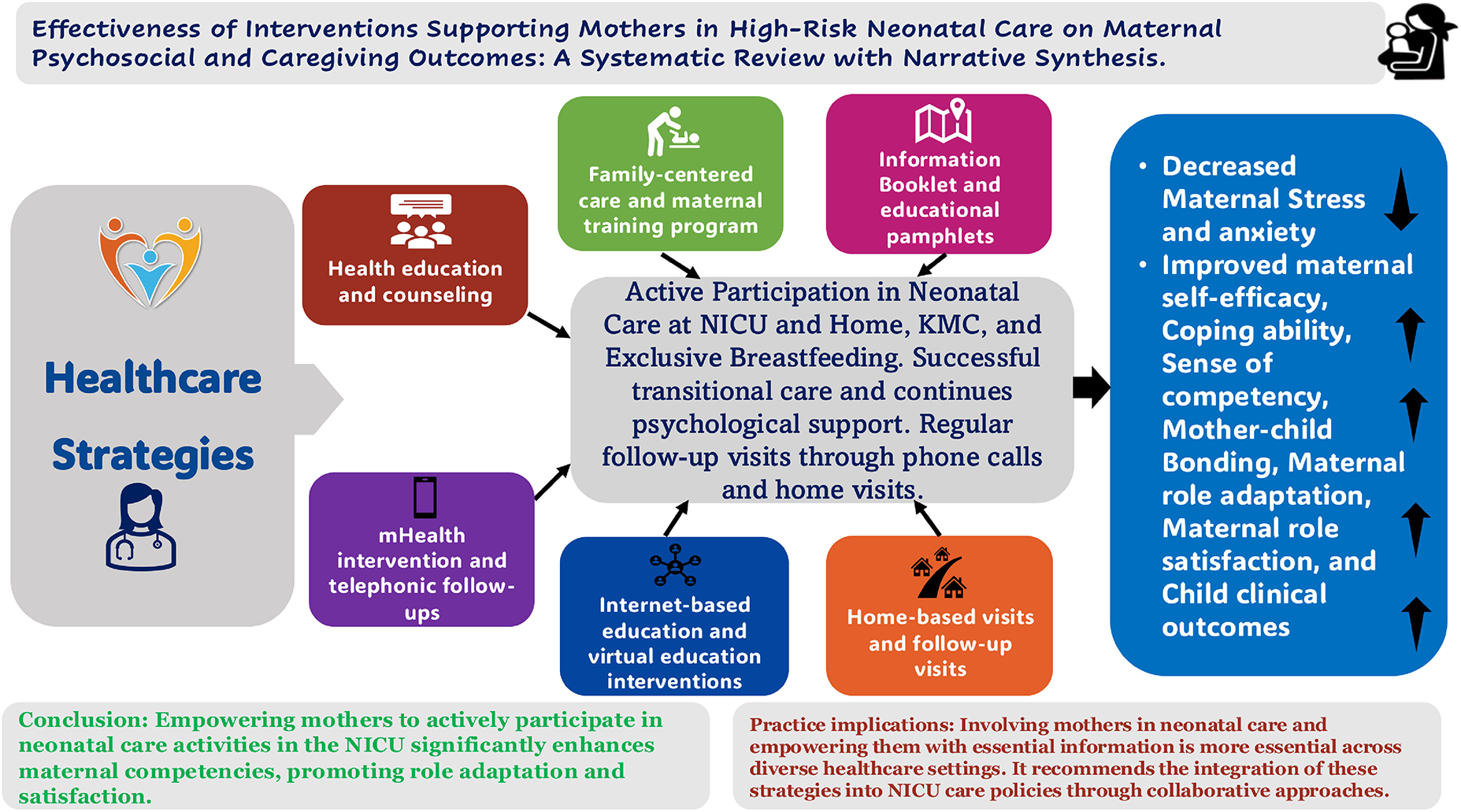
The impact of health-care strategies to improve maternal self-efficacy, role adaptation, and satisfaction with neonatal care is depicted in Figure 2.
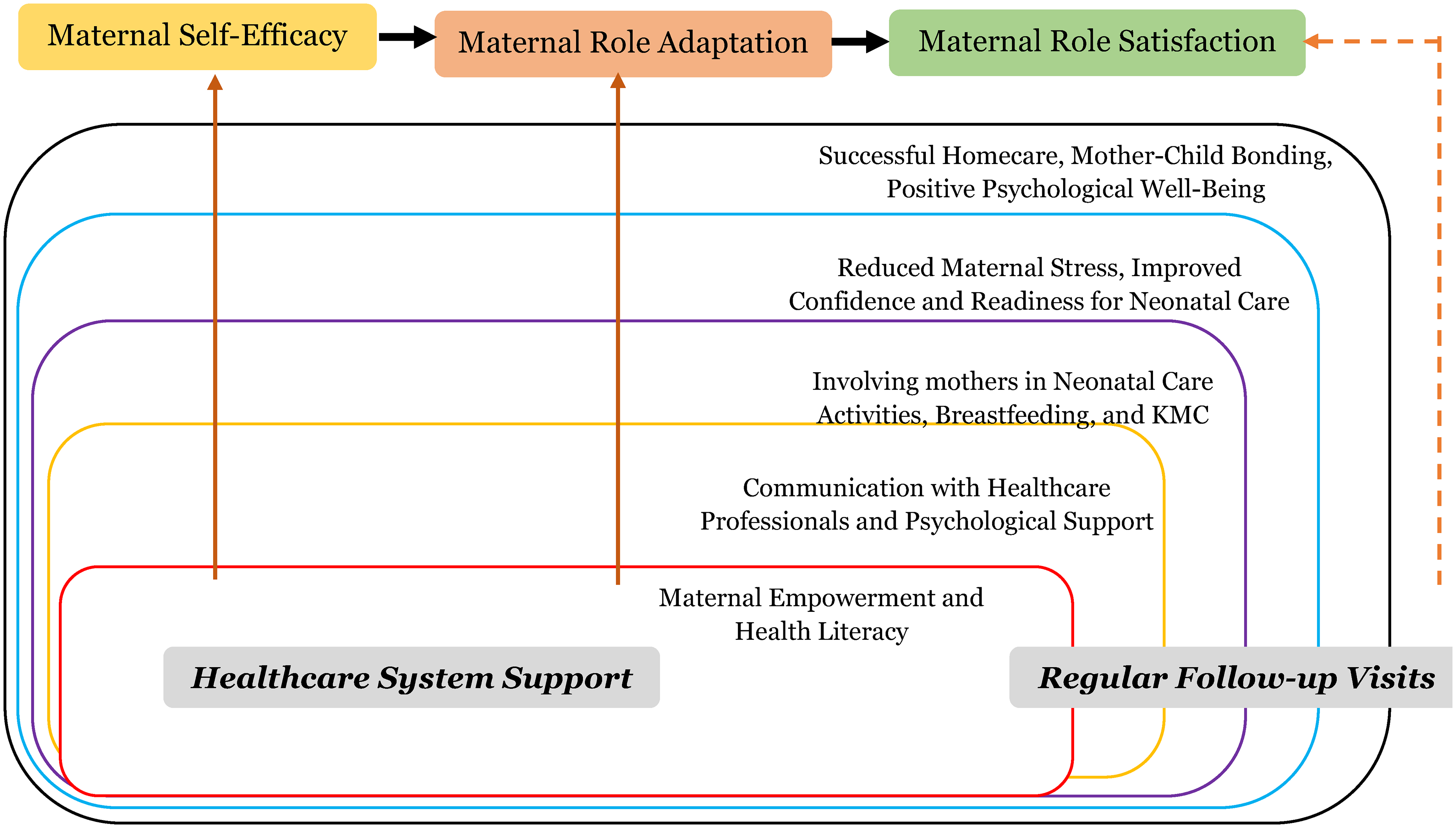
Framework of health-care strategies’ effects on maternal psychological health outcomes.
Outcome Measures
The included studies assessed a range of maternal outcomes using both validated and study-specific instruments. Maternal self-efficacy and confidence were most commonly measured using tools such as the parenting sense of competence (PSOC) scale, perceived maternal parenting self-efficacy (PMP-SE), Pharis's Self-Confidence Scale, and WBPL-R questionnaire. Maternal role adaptation and psychosocial adjustment were evaluated using adaptation scales, parental appraisal tools, and stress-related questionnaires. Broader aspects of well-being were assessed using instruments such as the Rosenberg self-esteem scale, WHO quality of life (WHO QoL), and sense of coherence (SoC) scale. Maternal satisfaction was measured using the Maternal Satisfaction Scale, Modified Maternal Satisfaction Questionnaire, and Parent Satisfaction Questionnaire. Readiness for discharge was assessed using tools such as the Readiness for Hospital Discharge Scale (RHDS), RHDS-parent form, Quality of Discharge Teaching Scale (QDTS), and Parent Discharge Readiness Questionnaire. Resilience was measured using the Connor–Davidson Resilience Scale (CD-RISC) and breastfeeding self-efficacy questionnaires. Overall, there was considerable variability in the instruments used and timing of assessments across studies, limiting direct comparability of findings.
Quality Assessment (Risk of Bias)
The methodological quality of included studies was assessed using the RoB-2 tool for RCTs and the JBI critical appraisal checklist for quasi-experimental studies. Domain-level assessments for RCTs included the randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selection of reported results. Although all five RCTs were classified as having an overall low risk of bias, some studies demonstrated concerns in individual domains, particularly related to outcome measurement and reporting processes. For quasi-experimental studies, quality assessment considered the clarity of cause-and-effect relationships, presence of comparison groups, similarity of participants, consistency of care provided, outcome measurement procedures, completeness of follow-up, and appropriateness of statistical analyses. Among the 17 quasi-experimental studies, 10 were rated as low risk, five as having some concerns, and two as moderate-to-high risk of bias.
Common methodological limitations included absence of control groups, lack of randomization, incomplete follow-up, and potential confounding. The results of the quality appraisal were incorporated into the synthesis and interpretation of findings. Greater emphasis was placed on evidence from studies with a lower risk of bias, while findings from studies with methodological limitations were interpreted cautiously. Detailed domain-level assessments are provided in Supplemental File 5.
Maternal Self-Efficacy in High-Risk Neonatal Care
Evidence related to maternal self-efficacy was derived from both randomized controlled trials and quasi-experimental studies and showed varying levels of support across intervention types. Digital health interventions demonstrated promising findings in the short term. Mothers receiving the NICU2HOME mobile application reported significantly higher parenting sense of competence (PSOC) scores than controls, with greater application engagement associated with higher scores (Garfield et al., 2022). Similarly, home-based educational interventions incorporating practical caregiving skills, home visits, and video-assisted learning were associated with improvements in perceived maternal self-efficacy (Khoshnood et al., 2023).
However, findings were not consistent across all studies. Internet-based interventions improved cognitive, behavioral, and affective domains of self-efficacy, but no statistically significant between-group differences were observed in overall self-efficacy scores at follow-up (Salonen et al., 2011). Likewise, community-based follow-up programs demonstrated higher mean parenting efficacy scores in intervention groups, although these differences did not reach statistical significance (Ji & Shim, 2020). Educational interventions focused on high-risk neonatal care and maternal bonding were also associated with positive trends in maternal confidence and caregiving competence (Gómez-Cantarino et al., 2020; Kadiroğlu & Güdücü Tüfekci, 2022). Overall, the evidence suggests that educational, digital, and home-based interventions may improve maternal self-efficacy, although findings vary according to intervention characteristics and study design.
Maternal Readiness for Discharge
Three studies examined maternal readiness for discharge and consistently reported favorable outcomes following structured discharge preparation programs. Interventions involving discharge booklets, educational sessions, home visits, and telephone follow-up were associated with higher levels of maternal preparedness and caregiving confidence during the transition from hospital to home (Kaewwimol et al., 2022). Similarly, lecture-based and video-assisted educational programs demonstrated significant improvements in discharge readiness scores compared with routine care (Chen et al., 2016). Empowerment-based interventions that combined education with hands-on skill training also reported positive effects on both practical caregiving competence and emotional preparedness (Peyrovi et al., 2016). Although findings were consistently favorable, the evidence is based on a limited number of studies with relatively short follow-up periods.
Maternal Sense of Competence, Resilience, 3and Related Outcomes
Several interventions were associated with improvements in maternal competence, resilience, and related psychosocial outcomes. The COPE program demonstrated significant improvements in maternal sense of competence that were maintained at one-month follow-up (Askary Kachoosangy et al., 2020). Multi-phase educational interventions focusing on breastfeeding and neonatal care were similarly associated with increased maternal confidence after discharge (Jang & Ju, 2020).
Evidence regarding resilience was more heterogeneous. Virtual educational and supportive interventions improved selected resilience domains, including positive acceptance of change and secure maternal–infant bonding; however, other resilience dimensions showed no statistically significant changes (Khoshnood et al., 2023). Kangaroo Mother Care interventions were associated with improvements in resilience and breastfeeding self-efficacy, particularly when interactive teaching methods were used (Mohammadi et al., 2022). Longer-term follow-up studies of mobile health interventions also reported improvements in maternal quality of life and sense of coherence at three months post-intervention (Khanjari et al., 2021). Overall, the available evidence suggests that empowerment, educational, and technology-based interventions may contribute to improvements in maternal competence and psychosocial well-being, although findings remain heterogeneous and should be interpreted cautiously.
Maternal Role Adaptation and Satisfaction
Evidence regarding maternal role adaptation and satisfaction was generally positive, although the strength of findings differed across studies. Educational interventions involving structured teaching, breastfeeding support, and practical demonstrations were associated with improvements in maternal role adaptation and caregiving skills, with several studies reporting statistically significant benefits (Heydarpour et al., 2017; Sohrabi et al., 2021). Notably, some studies found that improvements emerged over time rather than immediately after the intervention, suggesting that maternal adaptation is a gradual process. Family-centered care interventions were associated with increased maternal participation in NICU care and higher satisfaction levels compared with routine care (Bastani et al., 2015). Similarly, discharge education and digital support programs reported positive trends in maternal satisfaction related to caregiving preparedness and communication with health-care providers (Balasundaram et al., 2022). However, not all interventions demonstrated significant advantages. For example, internet-based education programs showed satisfaction scores comparable to those of control groups (Salonen et al., 2011).
Educational interventions of varying duration were generally associated with improvements in maternal satisfaction, although the magnitude of benefit varied across studies. Two studies reported significantly higher satisfaction scores among mothers receiving structured educational programs compared with routine care, suggesting that education may support positive maternal experiences during NICU hospitalization (Kadivar et al., 2017; Weiss et al., 2010). However, differences in intervention content, duration, and outcome assessment limit direct comparisons. Similarly, comparative interventions such as auditory, tactile, visual, and vestibular stimulation (ATVV), Kangaroo Care (KC), and maternal education produced mixed findings. Although overall differences between intervention groups were not consistently significant, mothers receiving the ATVV intervention reported higher satisfaction scores than those in comparison groups (Holditch-Davis et al., 2013). These findings suggest that sensory-based interventions may provide additional benefits; however, the evidence remains limited and should be interpreted cautiously.
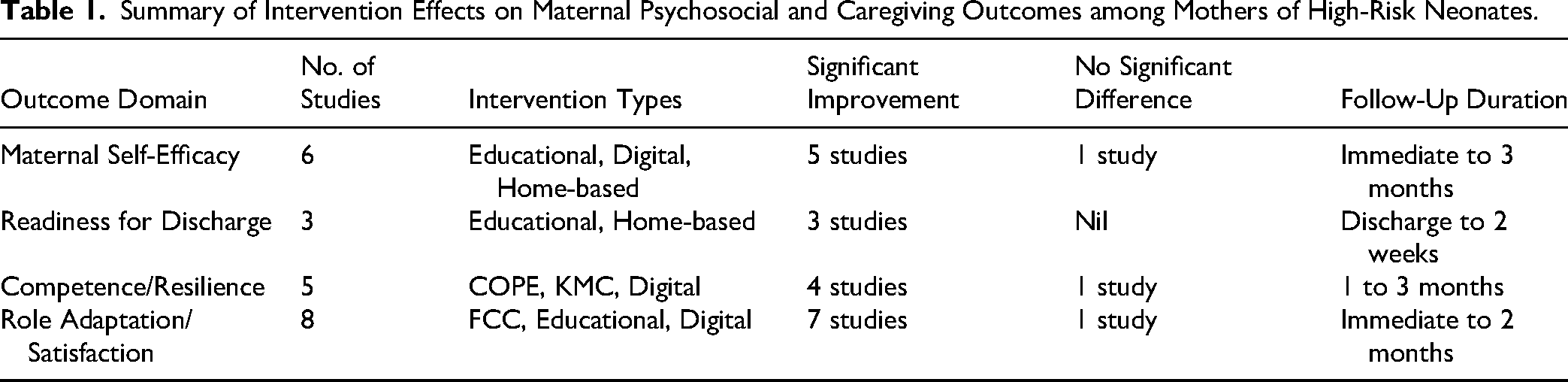
A summary of the evidence by outcome domain, including intervention characteristics and the direction of reported findings, is presented in Table 1 to support the narrative synthesis and interpretation of results.
Summary of Intervention Effects on Maternal Psychosocial and Caregiving Outcomes among Mothers of High-Risk Neonates.
Certainty of Evidence
The overall certainty of evidence was considered low to moderate. Although several randomized and quasi-experimental studies reported favorable maternal outcomes, confidence in the evidence is limited by methodological variability, heterogeneity of interventions, differences in outcome measurement tools, and relatively short follow-up periods. Inconsistencies in intervention content, delivery methods, and assessment timing further reduced comparability across studies. Additionally, the predominance of studies from specific geographic regions may limit the transferability of findings to other health-care settings. Therefore, while the available evidence suggests that family-centered, educational, digital, and home-based interventions may support maternal psychosocial and caregiving outcomes, further high-quality multicenter studies with standardized outcome measures and longer follow-up are needed to strengthen the certainty of evidence.
Discussion
This systematic review provides a structured synthesis of intervention-based evidence addressing maternal outcomes in high-risk neonatal care, with particular emphasis on maternal self-efficacy, role adaptation, readiness for discharge, resilience, and satisfaction. In contrast to a purely outcome-focused interpretation, the present review maps key evidence characteristics, including study designs, intervention types, and outcome measures, while critically examining methodological quality, heterogeneity, and contextual influences across settings.
The included studies predominantly employed quasi-experimental and randomized controlled designs, reflecting a strong focus on interventional research. However, this restriction may have limited the breadth of evidence by excluding qualitative and mixed-methods studies that could provide insights into maternal experiences and contextual barriers. In terms of intervention types, four major categories were identified: family-centered care, educational interventions, digital health approaches, and home-based or follow-up strategies. Educational interventions were the most frequently reported, highlighting the emphasis on improving maternal knowledge and caregiving skills (Askary Kachoosangy et al., 2020; Chen et al., 2016; Gómez-Rocha & Ospina-Romero, 2023; Heydarpour et al., 2022; Holditch-Davis et al., 2013; Jang & Ju, 2020; Kadiroğlu & Güdücü Tüfekci, 2022; Peyrovi et al., 2016; Pouyan et al., 2019; Sohrabi et al., 2021; Weiss et al., 2010). Digital and home-based interventions, although less common, indicate a growing shift toward continuity of care beyond the NICU (Balasundaram et al., 2022; Garfield et al., 2022; Ji & Shim, 2020; Kadivar et al., 2017; Kaewwimol et al., 2022; Khanjari et al., 2021; Khoshnood et al., 2023; Koochakzai et al., 2018; Salonen et al., 2011). The outcomes assessed across studies were relatively consistent, with maternal self-efficacy, confidence, and role adaptation being the most frequently measured constructs. Additional outcomes included readiness for discharge, resilience, and satisfaction. However, substantial variability was observed in the measurement tools, timing of assessments, and operational definitions of these outcomes. This lack of standardization limits comparability across studies and underscores the need for validated and consistent outcome measures in future research.
The implementation of maternal support interventions in high-risk neonatal care faces several challenges that are inconsistently addressed across studies. Variations in intervention duration, intensity, and delivery modes (face-to-face, digital, or home-based) may affect feasibility in routine practice. Resource constraints, particularly in low- and middle-income settings, can limit the implementation of time-intensive programs and follow-up support due to staffing and infrastructure limitations (Gondwe et al., 2022; Siva et al., 2025b). Digital interventions, although promising, may be hindered by issues such as limited technological access, low digital literacy, and reduced user engagement (Manisha et al., 2025).
Mechanistically, most interventions appear to function by improving maternal knowledge, caregiving skills, and emotional support; however, these pathways are rarely clearly defined or evaluated (Siva et al., 2024b). Interventions involving repeated interactions, hands-on training, and follow-up support may enhance skill retention and confidence through reinforcement (Siva et al., 2025b). Family-centered approaches may further strengthen maternal involvement through provider–parent collaboration. However, the lack of clarity on key active components limits optimization and scalability (Siva et al., 2025c).
A critical aspect of this review is the evaluation of methodological quality. Using standardized appraisal tools, the included studies showed variability in rigor. RCTs were largely categorized as low risk of bias, whereas quasi-experimental studies demonstrated greater methodological limitations, particularly related to the absence of control groups, lack of randomization, potential confounding, and incomplete follow-up. While outcome measurements were generally reported as reliable, inconsistencies in study design elements were evident. These methodological differences influenced the interpretation of findings, as studies with lower rigor may overestimate or underestimate observed changes. Therefore, although all studies were included to maintain comprehensiveness, findings from studies with a higher risk of bias were interpreted with caution.
Considerable heterogeneity was observed across studies in terms of intervention content, duration, delivery methods, and outcome assessment. Interventions ranged from single-session educational programs to multi-component strategies incorporating training, counseling, and follow-up support. This diversity reflects the complexity of maternal support needs but also poses challenges for synthesis and generalization. Furthermore, the mechanisms underlying these interventions were not consistently explored. While improvements in maternal outcomes may be linked to enhanced knowledge, skill acquisition, and emotional support, few studies explicitly examined these pathways. This limits understanding of how interventions function and which components are most effective in specific contexts.
An important finding of this review is the geographical concentration of studies, with a substantial proportion conducted in Iran. This concentration raises concerns regarding the transferability of findings to other settings. Cultural norms related to maternal roles, family involvement, and health-care interactions may influence both the implementation and outcomes of interventions. Additionally, differences in health-care infrastructure, resource availability, and policies governing NICU access may further affect the applicability of these findings. For example, family-centered care models may be more feasible in settings with flexible visitation policies, whereas resource constraints in other regions may limit implementation. Therefore, caution is required when generalizing findings, and future research should aim to include more diverse geographic and cultural contexts. Implementation challenges were also insufficiently addressed across studies. Factors such as health-care provider workload, training requirements, technological accessibility, and cultural acceptability may influence the feasibility and sustainability of interventions. Addressing these factors is essential for translating evidence into practice, particularly in low-resource settings.
Implications
Implications for Practice: The findings suggest that maternal support in NICU settings should incorporate structured, multifaceted interventions that combine education, skill-based training, and follow-up support. Family-centered care approaches that actively involve mothers in neonatal care may enhance engagement and caregiving confidence. Additionally, digital and home-based interventions can support continuity of care beyond discharge, but their implementation should consider resource availability and contextual feasibility.
Implications for Research: Future research should focus on improving methodological rigor through well-designed randomized controlled trials and standardized reporting of interventions. There is a need to develop and adopt consistent, validated outcome measures to enhance comparability across studies. Long-term follow-up studies are also essential to assess the sustainability of maternal outcomes. Furthermore, research across diverse geographic and cultural settings is required to improve generalizability and understand contextual influences.
Implications for Education: Nursing and health-care education programs should emphasize training in family-centered care, communication skills, and maternal support strategies in NICU settings. Incorporating evidence-based practices into curricula can enhance health-care providers’ ability to support mothers effectively. Additionally, training on the use of digital health tools and culturally sensitive care approaches is important to improve implementation in diverse health-care environments.
Limitations of Review
This systematic review has several limitations. First, there was considerable heterogeneity in intervention types, duration, intensity, delivery methods, and outcome assessment, which limited comparability across studies and precluded quantitative synthesis through meta-analysis. Second, variability in outcome measures and assessment tools, including the use of different validated and non-validated instruments, reduced consistency and restricted direct comparison of findings. Third, most studies reported short-term outcomes, with limited long-term follow-up, making it difficult to assess the sustainability of intervention effects. Fourth, methodological quality varied across studies, particularly among quasi-experimental designs, which were more susceptible to bias due to lack of randomization, absence of control groups, and potential confounding. Fifth, a substantial proportion of studies were conducted in a single country (Iran), which may limit the generalizability and transferability of findings to other health-care settings. Additionally, only English-language studies were included, introducing the possibility of language bias. The review did not include grey literature or trial registry searches, which may have contributed to publication bias. Furthermore, the review focused primarily on interventions targeting mothers and maternal outcomes, with limited consideration of the roles of fathers, partners and other family members who may significantly influence maternal well-being, caregiving participation, stress, and adaptation during an infant's NICU stay. Future research should examine family-centered approaches that account for these broader support systems and their impact on maternal and neonatal outcomes. Finally, the exclusion of qualitative and mixed-methods studies may have limited insights into contextual factors, implementation challenges, family dynamics, and maternal experiences relevant to real-world practice.
Conclusion
This systematic review synthesizes evidence on non-pharmacological interventions designed to support mothers of high-risk neonates in NICU settings. The included studies identified educational, family-centered, digital health, and home-based interventions that were generally associated with improvements in maternal psychosocial and caregiving outcomes, including self-efficacy, role adaptation, readiness for discharge, resilience, and satisfaction. However, substantial heterogeneity in intervention characteristics, outcome measures, follow-up periods, and methodological quality limits the consistency and generalizability of the evidence. Therefore, the findings should be interpreted cautiously. While these interventions show promise in supporting mothers of high-risk neonates, further high-quality studies using standardized outcome measures and longer follow-up periods are needed to strengthen the evidence base and inform implementation across diverse health-care settings.
Supplemental Material
sj-docx-1-cng-10.1177_10784535261464216 - Supplemental material for Effectiveness of Interventions Supporting Mothers in High-Risk Neonatal Care on Maternal Psychosocial and Caregiving Outcomes: A Systematic Review with Narrative Synthesis
Supplemental material, sj-docx-1-cng-10.1177_10784535261464216 for Effectiveness of Interventions Supporting Mothers in High-Risk Neonatal Care on Maternal Psychosocial and Caregiving Outcomes: A Systematic Review with Narrative Synthesis by N. Siva, Baby S. Nayak, Binil Velayudhan, Leslie Edward S. Lewis and Anice George in Creative Nursing
Supplemental Material
sj-docx-2-cng-10.1177_10784535261464216 - Supplemental material for Effectiveness of Interventions Supporting Mothers in High-Risk Neonatal Care on Maternal Psychosocial and Caregiving Outcomes: A Systematic Review with Narrative Synthesis
Supplemental material, sj-docx-2-cng-10.1177_10784535261464216 for Effectiveness of Interventions Supporting Mothers in High-Risk Neonatal Care on Maternal Psychosocial and Caregiving Outcomes: A Systematic Review with Narrative Synthesis by N. Siva, Baby S. Nayak, Binil Velayudhan, Leslie Edward S. Lewis and Anice George in Creative Nursing
Supplemental Material
sj-docx-3-cng-10.1177_10784535261464216 - Supplemental material for Effectiveness of Interventions Supporting Mothers in High-Risk Neonatal Care on Maternal Psychosocial and Caregiving Outcomes: A Systematic Review with Narrative Synthesis
Supplemental material, sj-docx-3-cng-10.1177_10784535261464216 for Effectiveness of Interventions Supporting Mothers in High-Risk Neonatal Care on Maternal Psychosocial and Caregiving Outcomes: A Systematic Review with Narrative Synthesis by N. Siva, Baby S. Nayak, Binil Velayudhan, Leslie Edward S. Lewis and Anice George in Creative Nursing
Supplemental Material
sj-docx-4-cng-10.1177_10784535261464216 - Supplemental material for Effectiveness of Interventions Supporting Mothers in High-Risk Neonatal Care on Maternal Psychosocial and Caregiving Outcomes: A Systematic Review with Narrative Synthesis
Supplemental material, sj-docx-4-cng-10.1177_10784535261464216 for Effectiveness of Interventions Supporting Mothers in High-Risk Neonatal Care on Maternal Psychosocial and Caregiving Outcomes: A Systematic Review with Narrative Synthesis by N. Siva, Baby S. Nayak, Binil Velayudhan, Leslie Edward S. Lewis and Anice George in Creative Nursing
Supplemental Material
sj-docx-5-cng-10.1177_10784535261464216 - Supplemental material for Effectiveness of Interventions Supporting Mothers in High-Risk Neonatal Care on Maternal Psychosocial and Caregiving Outcomes: A Systematic Review with Narrative Synthesis
Supplemental material, sj-docx-5-cng-10.1177_10784535261464216 for Effectiveness of Interventions Supporting Mothers in High-Risk Neonatal Care on Maternal Psychosocial and Caregiving Outcomes: A Systematic Review with Narrative Synthesis by N. Siva, Baby S. Nayak, Binil Velayudhan, Leslie Edward S. Lewis and Anice George in Creative Nursing
Footnotes
Acknowledgements
The authors appreciate the technical assistance and resources provided by the Manipal Academy of Higher Education (MAHE), Manipal, and the Indian Council of Medical Research, Senior Research Fellowship (ICMR SRF), for supporting this research work.
Author Contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This paper is a part of an intervention program developed for a study funded by the Indian Council of Medical Research (ICMR) Senior Research Fellowship (IRIS Number – 2021- 8364).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
Dr.
Dr.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.