
Abstract
This qualitative descriptive study explored how 26 nurses practicing in diverse settings across the United States experienced, understood, and made meaning of nurse-to-nurse bullying, and how these experiences shaped their workplace culture. Analysis of the results of semi-structured interviews revealed three themes: the normalization of bullying through professional language and early socialization, the acceptance of bullying as a rite of passage tied to power and hierarchy, and the need to intentionally disrupt these patterns through nursing education. Participants described how bullying began in nursing school and continued into their clinical practice, contributing to stress, disengagement, and intent to leave the profession. They also emphasized the responsibility of nursing educators to address workplace climates and to prepare students to respond to bullying through the curriculum. Creating learning environments that emphasize communication, reflection, and relational accountability may help challenge the normalization of bullying and foster more supportive and collaborative nursing cultures.
Implications for Knowledge Translation and Practice
Reframing nurse-nurse bullying as a preventable practice issue, not a cultural norm. Integrating proactive communication and bullying response training into nurse education. Positioning educators, preceptors, and leaders as key agents of cultural change.
Bullying in nursing is not a novel topic; the phenomenon is well-documented in nursing research (Anusiewicz et al., 2020; Edmonson & Zelonka, 2019; Gilbert et al., 2016; Granstra, 2015). Nearly 20 years ago, one in three nurses reported that they had experienced bullying to such an extent that they had considered leaving their jobs (Edmonson & Zelonka, 2019). Gilbert et al. (2016) pointed out that the prevalence of the problem has increased over time. As many as “60% of newly licensed registered nurses leave their first nursing jobs within 6 months of hire as a direct result of being bullied” (Gilbert, p. 2). According to RNnetwork (2018), 45% of nurses reported having been verbally harassed or bullied by other nurses, 38% having been harassed or bullied by managers or administrators, and 38% having been verbally harassed or bullied by physicians (Gilbert et al., 2016, p. 2). While nurses have reported being bullied by various people, from their supervisors to the family members of patients, Gilbert et al. (2016) found that the most prevalent form of bullying nurses endured (64%) was “from their nursing peers” (p. 1).
Literature Review
Etienne (2014) explained that lateral violence among nurses refers to “aggression among peers or coworkers at the same organizational level” (p. 6). Bullying is characterized as repeated behavior that involves “an imbalance of power and an intent to cause harm” (Granstra, 2015, p. 250). Lewis (2006) argued that bullying among nurses is a “learned behaviour” (p. 52), suggesting that newly employed nurses may observe and adopt such behaviors to fit in, thereby perpetuating the cycle.
Bullying behaviors may be overt or covert. Gilbert et al. (2016) described overt behaviors as blatant and easily identifiable, including name-calling, fault-finding, gossip, intimidation, shouting, blaming, and the use of put-downs. Equally concerning are covert behaviors, which are often overlooked. These include unfair assignments, sarcasm, eye-rolling, ignoring colleagues, refusing to help, sabotage, isolation, exclusion, and fabrication (Gilbert et al., 2016). Gilbert et al. further noted that the most common forms of nurse-to-nurse bullying involve subtle innuendos, such as facial expressions and eye-rolling, as well as verbal insults like abrupt responses and snide remarks. Regardless of form, both overt and covert bullying have had a significant impact on the nursing profession.
In a profession centered on care, horizontal violence is particularly troubling, raising questions about its causes and consequences. Granstra (2015), through interviews with nurses at Minnesota State University Moorhead, identified several contributing factors, including hierarchical health-care structures and insecurity. Similarly, Etienne (2014) highlighted staff shortages and occupational stress as contributing factors, noting that bullying is often linked to negative performance appraisals for victims, organizational restructuring, and competition over resources. Bullying may also occur when nurses attempt to exert power over colleagues or act out personal stressors unrelated to the workplace.
The prevalence of horizontal violence among nurses can lead to serious physical, psychological, and performance-related consequences. Researchers found that recipients of bullying, harassment, and horizontal violence experienced psychological effects reported across studies included anxiety, panic attacks, depression, irritability, mood swings, and loss of confidence and self-esteem (Liu et al., 2025; Vessey et al., 2011). Victims of bullying may experience sleep disorders, anxiety, post-traumatic stress disorder, substance abuse, and/or suicidal thoughts. Physical symptoms can include headaches, gastrointestinal upset, increased blood pressure, anorexia, and loss of libido (Anusiewicz et al., 2020; Liu et al., 2025; Reguera-Carrasco et al., 2026; Rocker, 2008; Vidal-Alves et al., 2021).
Although bullying may be perceived as “an inherent characteristic of the nursing work environment” (Anusiewicz et al., 2020, p. 4158), its impact on both individuals and organizations is profound. Vessey et al. (2011) emphasized that bullying disrupts teamwork by impairing communication, information exchange, and collaborative decision-making, which are critical to patient safety and are associated with decreased medical errors and better patient outcomes. These factors also contribute to job dissatisfaction, professional disengagement, and increased turnover, ultimately affecting the quality of care (Anusiewicz et al., 2020; Liu et al., 2025; Reguera-Carrasco et al., 2026).
The American Nurses Association's (2025) policy recommendations include skills-based training and coaching, ongoing non-confrontational monitoring, systems for assessing staff perceptions of unprofessional behavior, and policies that encourage early reporting without fear of retaliation. Additionally, an integrative review by Sidhu and Park (2018) noted that nursing students often experience bullying as early as their first year of education. This underscores an opportunity for nursing education programs to intervene early in any cases of bullying or a hostile workplace, fostering a professional culture in which bullying is no longer normalized.
Purpose of Study
This study aimed to explore how nurses have experienced or observed nurse-nurse bullying (lateral violence) and to identify proactive strategies to mitigate and prevent such behaviors in the future.
Methodology
This study employs a descriptive qualitative approach to explore workplace climate and bullying in health care among nursing professionals and to explore how to better understand and stop the behavior. According to Doyle et al. (2020), a qualitative descriptive design may be deemed most appropriate for an exploratory study using interviews as it recognizes the subjective nature of a problem and the different experiences participants have had, and can present the findings in a way that directly reflects or closely resembles the terminology used in the initial research question (p. 444). This approach is effective for gauging participants’ perceptions and overall experience with the topic being studied. Therefore, a descriptive qualitative approach was used in this study to investigate the perceptions and experiences of nurses and how they understood their workplace climate.
Method
Recruitment of Participants
Nonprobability sampling (convenience sampling and snowball sampling) was used to identify participants for this study. A call for participants was posted on Facebook, Twitter, and Instagram. The call for participants was also sent to a College of Allied Health and Nursing in Minnesota and a College of Nursing at a university in Wisconsin. The call for participants invited nurses with two years of post-graduate nursing practices that were interested in discussing their experiences with a negative workplace climate.
Participants
The 26 nurses who participated in this study were female; 25 identified as white and one as African American. The nurses had between 3 and 23 years of experience in the nursing field. Seven of the 26 participants entered nursing as a second career. Of the 26 nurses, 19 practiced in the Midwest, three in the Pacific Northwest, one in the South, two in the West, and one in the East (see Table 1 for participant characteristics). Participants were interviewed using a semi-structured interview format. This approach allowed me to ask all participants the same questions while allowing me to adapt to each interviewee as we engaged in the interview process.
Participant Characteristics. a
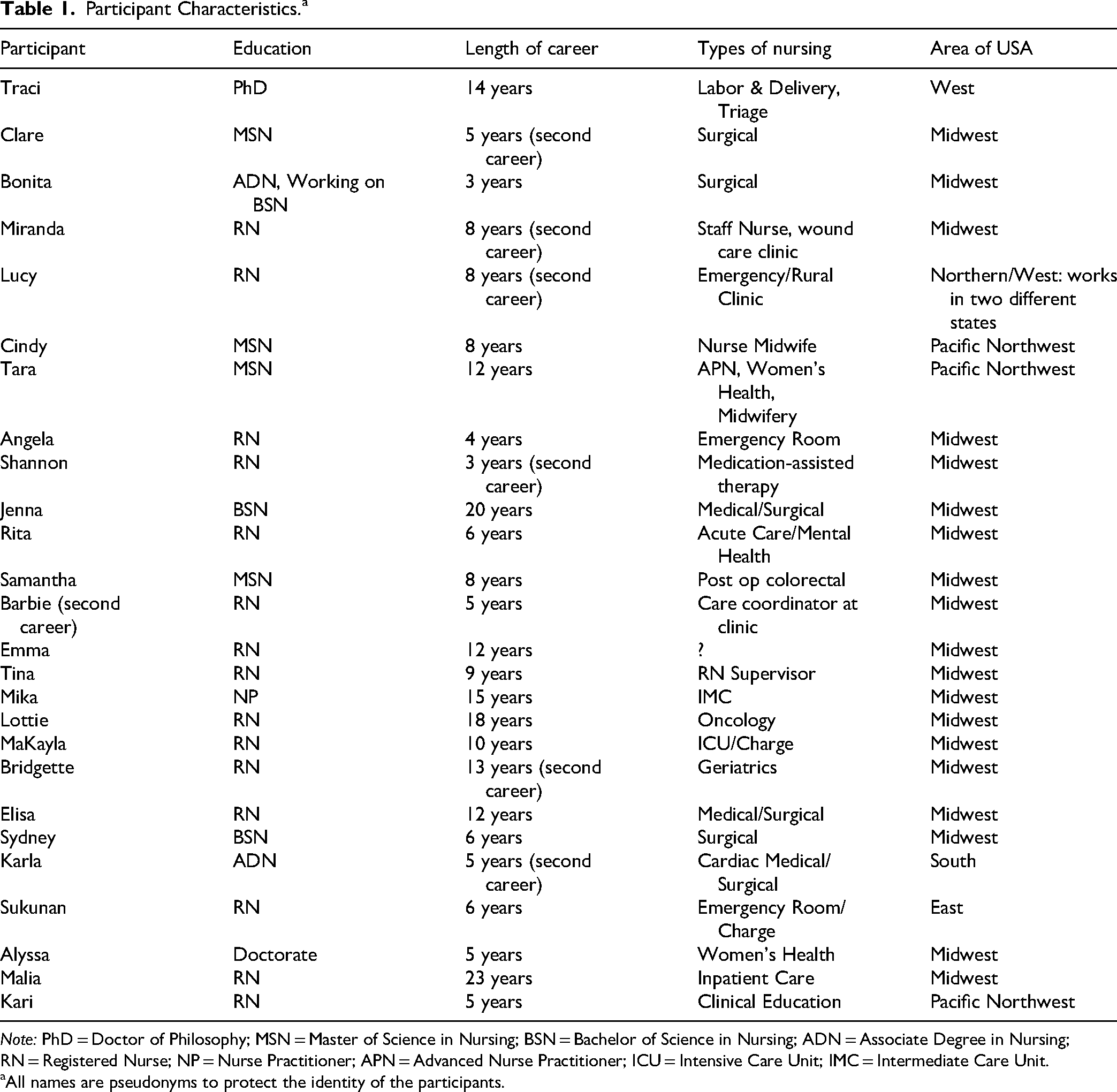
Note: PhD = Doctor of Philosophy; MSN = Master of Science in Nursing; BSN = Bachelor of Science in Nursing; ADN = Associate Degree in Nursing; RN = Registered Nurse; NP = Nurse Practitioner; APN = Advanced Nurse Practitioner; ICU = Intensive Care Unit; IMC = Intermediate Care Unit.
All names are pseudonyms to protect the identity of the participants.
Data Analysis
Online interviews with the 26 participants were conducted between August and November of 2023. The transcripts from the interviews were downloaded and reviewed for accuracy by listening to the recording while reading the transcript of the interviews. Thematic analysis was used to “analytically examine the narrative materials from life stories by breaking the text into relatively small units of content and submitting them to descriptive treatment” (Vaismoradi et al., 2013, p. 400). Thematic analysis “involves the search for and identification of common threads that extend across an entire interview or set of interviews” (p. 400). Specifically, Vaismoradi et al. noted the following processes involved in data analysis and thematic analysis: (1) familiarizing with the data, (2) generating initial codes, (3) searching for themes, (4) reviewing themes, (5) defining and naming themes, and (6) producing the report. Importantly, Vaismoradi et al. noted that the “thematic analysis process is not linear and does not move from one phase to another phase but should be recursive with frequent reviews” (p. 403). The analysis of the interviews followed the process outlined by Vaismoradi et al. As noted above, to ensure the accuracy of the transcripts, the analysis began by reading the transcripts while listening to the interviews being recorded. Initial codes were identified, and themes were generated from the codes.
Ethical Considerations
This study received approval from the Institutional Review Board at Minnesota State University, Mankato (IRB #2053857). Written informed consent was obtained from all participants prior to the interviews. To ensure confidentiality, all participant identifiers were removed from the data, and pseudonyms were used in place of actual names when reporting the findings. Participants were informed of they could end participation in this study at any time for any reason; whether that reason was because the participant did not want to continue the interview or whether the participant found the interview questions uncomfortable to answer.
Findings
Three themes emerged from the data analysis. First, all participants were familiar with the phrase “eating their young” and understood its meaning and impact, emphasizing the normalization of bullying in the nursing profession. Second, bullying was widely viewed as a normalized rite of passage, regardless of whether nurses had personally experienced it. Third, participants emphasized the importance of proactively addressing nurse-to-nurse bullying through nursing education to disrupt the belief that such behavior is inevitable.
Theme 1: The Normalization of Bullying
Consistent with arguments from Gillespie et al. (2017) and Vidal-Alves et al. (2021), all participants had encountered the phrase “nurses eat their young,” often long before entering professional practice. A total of 20 of the 26 participants first heard the meme in nursing school, while the remaining participants encountered it early in their careers or through family members in nursing. Across accounts, the phrase functioned less as a critique of harmful behavior and more as a warning—signaling to the new nurses should expect little support. In order to understand what the meme meant to the participants, near the end of the interview, I asked participants who had not discussed “eating their young” if they had heard of the meme and what it meant to them in the nursing profession.
Participants described the phrase as communicating expectations of self-reliance and emotional hardening. Shannon recalled that it meant, “Figure this out because you are on your own … when you’re on the floor, they’re not going to help you.” Melinda framed it as a “weeding out” process, explaining, “If you’re not going to survive this job and be just as callous as everybody else, then you should learn that early.”
Rather than preparing nurses to challenge bullying, these messages emphasized endurance. Rita noted that students were warned but not taught how to respond. Rita argued, “They [nurse educators] don’t teach it in the way you think,” “Hey, don’t be that nurse when you get done [with school].” Instead, she explained, “They teach you that you better know what you are doing when you get on the floor. So, it's really top backwards, you know? Reactive. Reactivity instead of proactivity.”
Participants also highlighted unrealistic expectations placed on new nurses. As Malia explained, “Older nurses just expect people to come out of nursing school and just take over and be confident … We all know that's not the case.” Alyssa expounded on Malia's thoughts, explaining, “You will definitely run into nurses where, if you don’t know something, they’re like, are you even smart, you know? Like more that passive-aggressive, likely bullying attitude.”
Treating lateral violence as an accepted rite of passage, rather than a preventable problem, created environments marked by anxiety, disengagement, and attrition. Unchecked bullying contributes to workforce instability and undermines the profession's future (Etienne, 2014; Kroning & Annunziato, 2023).
Theme 2: The Culture of Bullying as a Rite of Passage
Seventeen participants had personally experienced bullying; 20 participants described bullying as an expected part of becoming a nurse. Many reported being explicitly warned during nursing school and clinical placements to anticipate mistreatment, reinforcing the belief that bullying “comes with the territory.” Cindy reflected this normalization, stating, “I don’t know why they do it, but it's like a rite of passage, almost.”
Power and hierarchy were central to participants’ accounts. Sam described being assigned undesirable tasks by a veteran nurse, interpreting the behavior as an expression of authority rather than mentorship: she was expected to do the “grunt dirty work.” Karla similarly described how experienced nurses asserted dominance by withholding guidance and relying on nonverbal cues: “Lot of body language, lot of tone … really aggressive behavior from veteran nurses.”
Several participants shared the emotional toll of these behaviors. Barbie described repeated dismissal and abandonment by preceptors, noting that eye-rolling and indifference were routine. Ultimately, she left her first position, recalling “Sitting in the parking lot just freaking crying, like day after day before shifts.” Even when participants rejected these behaviors and attempted to disrupt them, they acknowledged that bullying was embedded in both educational and workplace cultures.
Theme 3: Disrupting the Norm Through Education
Despite the normalization of bullying, participants consistently identified nursing education as a critical leverage point for change. All participants rated education on workplace climate and bullying as extremely important. Miranda summarized this consensus succinctly: “A 10, and you can crank that 10 up to 1,000.”
Fourteen participants described nursing education as punitive and hierarchical, often mirroring the same power dynamics experienced in practice. Cindy characterized nursing school as an initiation into hazing, explaining that it felt like “my indoctrination into this world of hazing … started from the very first week.” Others echoed this sentiment, describing rigid expectations and a lack of trust that undermined their development as adult learners.
To counter these patterns, participants advocated for proactive skill-building in nursing curricula. Many emphasized simulations and role-play as key strategies for preparing students to navigate difficult interactions. Clare described simulations as creating “muscle memory, mind memory” that equips nurses to respond effectively to bullying. Sukyun similarly suggested scenarios in which students practice standing up for themselves, with educators modelling both harmful and appropriate behaviors.
Participants also stressed the importance of teaching boundary-setting and self-advocacy. As Malia explained, nurses must learn how to communicate limits safely, “Just drawing the line and not being pushed to do more.” Collectively, these recommendations point toward a shift from warning students about bullying to equipping them with tools to actively disrupt it.
Discussion
Throughout the interviews, it was evident from the participants that bullying is understood to be taught as something that is normal and expected as part of the nursing culture. Shannon, who experienced “eating their young” at several points in her career, expressed that it was most evident during her course work. Shannon explained, “It was figure this out because you are on your own. We’re not going to help you. We’re not going to point you on which chapter your questions is, we’re not going to help you at all with anything because when you’re on the floor they’re not going to help you.”
Makayla experienced bullying from her preceptor when she was a new nurse nearly 10 years ago. She explained that she felt incompetent—always being told she was doing things wrong or making the preceptor's life more difficult. Similarly, Tracy recalls a veteran nurse who continually put her down with negative comments when she first started. Tracy reflected on a specific night when she was working “really hard—physically and mentally—just working my butt off, and she made a comment that alluded to me being lazy.” Although I included questions about the phrase “eating their young” in my interview protocol, nearly half of the 26 participants raised nurses “eating their young” when discussing their nursing education or workplace experience before being asked about it in the interview protocol.
Beyond exploring nurse-to-nurse bullying experiences, this study aimed to offer solutions to combat lateral bullying in the workplace. Participants offered approaches that could be implemented within the college classroom to promote positive workplace climates, environments where nurse-nurse bullying was neither a norm nor an expectation. Treinen et al. (2022) argued that “Trust must be built at every level of health care, and it begins with nurses and their educators engaging in relationships rooted in communication, connection, and the ability to engage in productive dialogue” (p. 163). The strongest suggestion was to have a classroom where effective communication is taught and practiced, boundaries are explored, and students can engage in demonstrations of proactive behaviors in response to bullying by their instructors, preceptors, and future colleagues.
Alberts (2022) argued that educators play a central role in addressing incivility and bullying with students. Providing curriculum that specifically addresses bullying provides students with the tools and resources needed to “manage bullying and bring change within health care” (p. 436). Alberts (2022) suggests using “management strategies, simulation training and focused reflective discussions” to bring awareness to prevention and management and provide students with the confidence to stand up for themselves should they be faced with bullying in the workplace. Alberts (2022) suggestions are reflective of Sidhu and Park (2018), who found eight concepts that could be integrated into the nursing curriculum to successfully help nursing students address bullying: empowerment, self-efficacy, awareness about self, awareness about bullying, support, communication, collaboration, and socialization. Sidhu and Park (2018) argued that “these concepts and their intricate relationships in fostering student empowerment can all be conceptualized at the individual, interpersonal, and structural/system levels. Empowerment was a common concept threaded throughout these levels” (p. 171).
Ulrich et al. (2017) studied the use of role-playing among nursing students to reflect on current problems in the field of nursing. They found that role-playing could be implemented without additional costs to students or faculty members. More importantly, the desired student learning outcome was achieved by examining the experience and outcomes of simulated bullying. Students described numerous responses and actions reflecting affective learning, an area often overlooked in nursing education (p. 205). Sowko et al. (2019) explored an innovative strategy to integrate simulation in a study examining how to “teach effective communication in response to difficult workplace conversations” (p. 538). While lectures and viewing scenarios were used to help students understand how to effectively confront difficult conversations, students also created smartphone “trigger videos.” Sowko et al. (2019) found these videos allowed the students to “visualize real time workplace situation addressing a difficult conversation and increased active class participation with instruction of effective communication techniques” (p. 541). The smartphone videos allowed for coaching and modeling effective communication skills.
Alraja et al. (2025) explored an intervention created to “raise awareness and self-efficacy among nursing students” (p. 1). They developed and tested three interactive online modules that defined bullying, introduced various forms of bullying and the implications of bullying, and presented strategies to intervene in bullying situations. Alraja et al. (2025) argued that “addressing bullying at the student level is critical to breaking the vicious cycle of bullying in nursing by fostering respectful and supportive environment early in their career” (p. 2). Urstad et al. (2018) studied nursing students’ experiences using student-created digital storytelling as a tool in the context of clinical placement studies. Although the study found that instructors must consider students’ vulnerability in sharing stories, they also found that digital storytelling contributed to a student-active learning environment by triggering student engagement, promoting ownership of the reflection, and encouraging a deeper understanding of the experienced situation.
Strengths and Limitations of Study
This study aimed to explore how nurses have experienced or observed nurse-nurse bullying and identify proactive strategies to mitigate and prevent such behaviors in the future. A strength of this study was that all 26 participants agreed on the importance of incorporating strategies to address bullying within nursing curricula and challenging the normalization of such behavior. The limitations of this study included the number of participants, which may be too small to make broad generalizations about the findings. The lack of demographic diversity in terms of gender and race also limits the application of this study. Because I used non-probability sampling (convenience sampling and snowball sampling), selection bias was likely to occurs. While most would agree to the existence of lateral bullying, nurses who have not experienced this type of behavior would be less likely to respond to the call for participants.
Implications for Research and Education
Addressing lateral violence in nursing is essential to not only the retention of nurses, but also to attracting new nurses to our higher education institutions. A toxic work environment for nurses can lead to poor patient care (Houck & Colbert, 2017). Exploring lateral violence encourages nurses to advocate for educational changes to nursing programs. As a result, substantive changes to workplace violence could become a reality; nurses no longer have to “take it” until “they have gained more nursing experience, were promoted to leadership role or leave the unit altogether” (Anusiewicz et al., 2020, p. 4152).
Based upon the findings of this research, future studies may examine what positive workplace environments look like for nurses. What policies are in place that create a welcoming and supportive climate for new nurses? In what ways do nurses seek to support their co-workers when faced with workplace bullying? This study also suggested ways that nursing programs could start to not only discuss nurse bullying in the workplace as something that is inherent in the workplace environment, but work toward finding solutions to the problem. Studying these strategies could inform best practices to help mediate nurse–nurse bullying in the workplace.
Conclusions
While the pervasive issue of nurse-to-nurse bullying is not new and has been readily studied, Gilbert et al. (2016) argued that it is “underestimated and under reported” (p. 1). This project sought to add to the existing literature on lateral violence in the nursing profession and offer a space for nurses to voice their experiences of facing a negative workplace environment. Furthermore, the study engaged these participants in finding solutions based on their experiences, offering a unique perspective to inform programmatic changes in nursing education. As noted by Kroning and Annunziato (2023), “civility is vital to the success of our nursing schools, students, educators and patient safety” (p. 50). Success can be found when nurse faculty “focus on effective collaboration instead of competition to improve nursing programs” (p. 50). The findings of this study suggest that the normalization of bullying contributes to undue stress, job dissatisfaction, and negative impacts on patient care. Gilbert et al. (2016) argued that it is imperative to address the “elephant in the room as nurse-to-nurse bullying results in toxic workplace environments, reduced nurse and patient satisfaction, poor recruitment and retention, increased medical costs, and poor patient outcomes” (p. 10). To address these issues, it is imperative to listen to the voices of those who have experienced bullying. Through storytelling and simulations/role-playing, our future nurses can shift the expectation from workplace bullying to an environment of collaboration, support, and care.
Footnotes
Ethical Approval and Informed Consent Statement
This study was approved by the Internal Review Board of Minnesota State University Mankato. The approval number is: IRBNET#2053857.
Author contribution(s)
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.