
Abstract
Neonatal sepsis remains a major cause of morbidity and mortality, with diagnosis complicated by nonspecific clinical signs and limited reliability of conventional laboratory tests. This study aimed to evaluate and compare the diagnostic efficacy of biomarkers tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6), and procalcitonin (PCT) with traditional sepsis screening parameters in neonates. This hospital-based case–control study was conducted in the neonatal intensive care unit of a North Indian tertiary care medical university between September 2023 and March 2025. A total of 300 neonates were screened, of which 100 were diagnosed with sepsis (cases) and the remaining 200 served as controls. Sepsis screening, TNF-α, IL-6, PCT, and blood culture were performed to diagnose neonatal sepsis. Results of this study showed significantly higher levels of all tested biomarkers and sepsis parameters in cases compared with controls. Among biomarkers, TNF-α demonstrated the highest accuracy [area under the curve of the receiver operating characteristic (AUROC) 0.99, sensitivity 94%, specificity 100%], followed by PCT (AUROC 0.82, sensitivity 80%, specificity 82.5%) and IL-6 (AUROC 0.79, sensitivity 86%, specificity 74.5%). The study concludes that TNF-α is the most reliable biomarker for diagnosing neonatal sepsis, although a multimodal approach integrating conventional parameters with cytokines and PCT offers the best diagnostic yield. Combining early biomarkers with standard screening may improve early recognition, reduce unnecessary antibiotic exposure, and strengthen antimicrobial stewardship.
This is a visual representation of the abstract.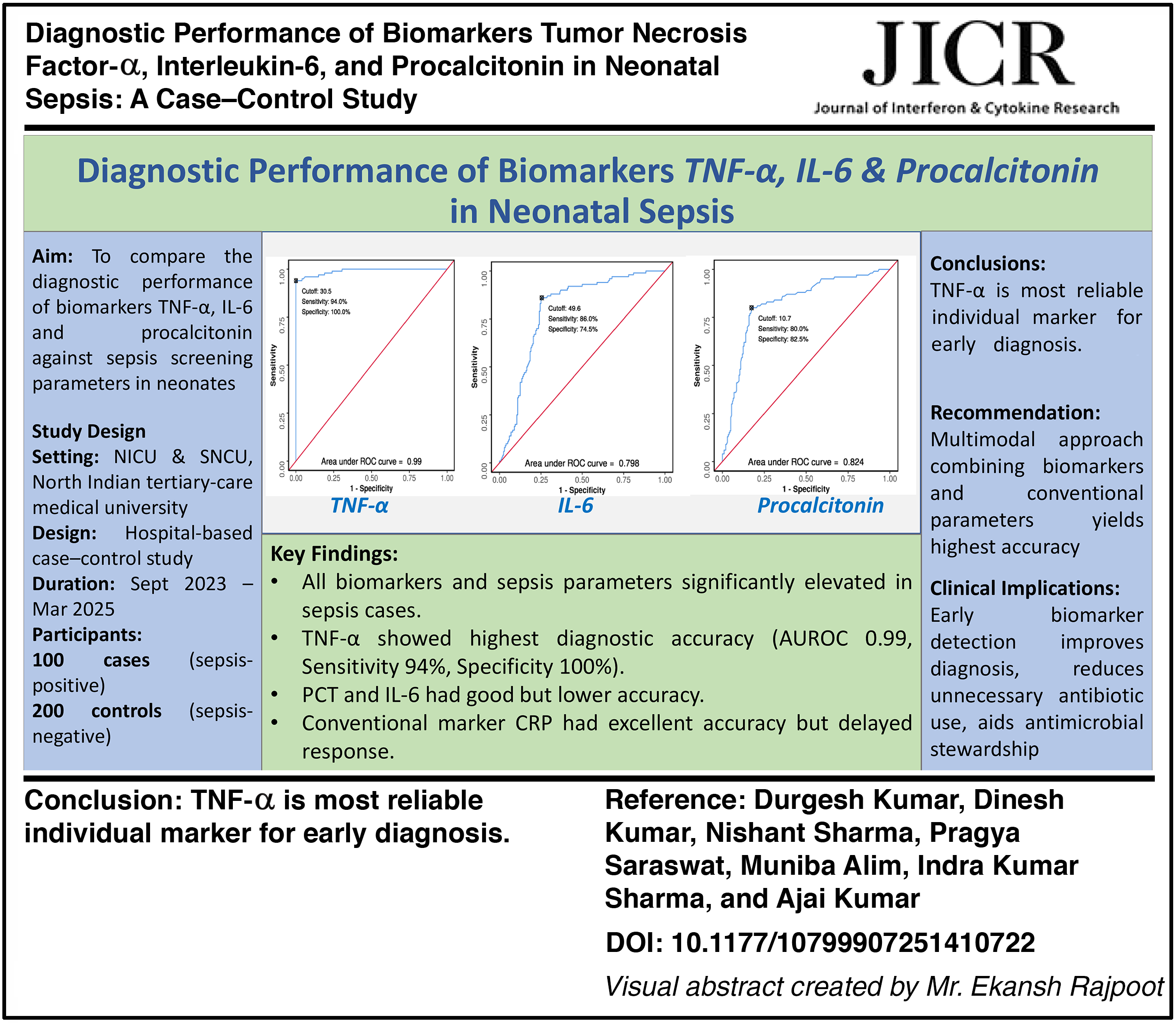
Introduction
Neonatal sepsis remains one of the most significant causes of morbidity and mortality in newborns, particularly in developing countries (Liu et al., 2015; Stoll et al., 2002). It is a condition in which a systemic infection leads to a widespread inflammatory response in the neonate, and if not identified and managed promptly, it can result in severe complications and even death (Shane et al., 2017). Timely diagnosis and appropriate management are crucial in improving outcomes for neonates suspected of sepsis (Polin and Committee on Fetus and Newborn, 2012).
Globally, the incidence of neonatal sepsis is estimated at 3930 per 100,000 live births, accounting for nearly 24% of neonatal deaths (Fleischmann et al., 2021). In India, up to 20% of neonates admitted to neonatal intensive care units develop sepsis (Vijayan et al., 2019). The conventional sepsis screen, though widely used, suffers from limited sensitivity and specificity, leading to diagnostic uncertainty (Escobar et al., 2000; Ng et al., 2003). This has driven the search for more reliable biomarkers. Cytokines such as tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and procalcitonin (PCT) have emerged as promising markers for early detection individually (Chiesa et al., 2003; Dulay et al., 2007; Meisner, 2005). These biomarkers not only reflect the host immune response but also offer potential for earlier and more accurate diagnosis. However, their comparative diagnostic utility remains to be explored. This study aims to evaluate and compare the diagnostic performance of IL-6, TNF-α, and PCT against the traditional sepsis screen in neonatal sepsis, with the goal of improving diagnostic accuracy leading to a reduction in neonatal morbidity and mortality.
Materials and Methods
This hospital-based case–control study was conducted in the Neonatal Intensive Care Unit and the Special Newborn Care Unit of a North Indian medical university between June 2023 and December 2024. Term neonates up to 28 days of age with a birth weight ≥2500 g and at least two risk factors for neonatal sepsis were enrolled. The risk factors considered in this study included male sex, outborn admission, unclean vaginal examination during labor, prolonged labor, premature rupture of membranes, and requirement for artificial ventilation. Neonates with a birth weight <2500 g, prior antibiotic exposure before admission, birth asphyxia, congenital malformations, or congenital infections were excluded.
The study protocol received approval from the Institutional Ethics Committee (Ref. No. 54/2023–24), Uttar Pradesh University of Medical Sciences, Saifai, Etawah, India. Written and informed consent was obtained from parents or guardians. Those neonates fulfilling the inclusion criteria and presenting with at least two of the aforementioned risk factors underwent sepsis screening, which comprised five parameters: C-reactive protein (CRP), total leukocyte count (TLC), absolute neutrophil count (ANC), microerythrocyte sedimentation rate (micro-ESR), and immature-to-total neutrophil ratio (I/T ratio). Neonates were considered to have sepsis if any two of these parameters were positive (CRP >1 mg/L, TLC <5000, ANC below the reference range based on Manroe’s chart, micro-ESR >15 mm in the first hour, or I/T ratio >0.2) (Murthy et al., 2019; Agarwal et al., 2023).
A total of 300 neonates were screened for sepsis during the study. Among these, 100 neonates tested positive and were categorized as cases, while the remaining 200 who tested negative served as controls. Thus, controls were selected from the same population to prevent the selection bias. Baseline variables, including demographic details, antenatal, perinatal, and postnatal history, physical examination findings, principal diagnosis, and vital signs, were recorded for each neonate. Under strict aseptic precautions, blood samples were obtained and sent for sepsis screening, TNF-α, IL-6, and PCT level, along with blood culture. Serum was separated and centrifuged for PCT analysis, while aliquots for IL-6 and TNF-α were stored at −80°C, as cytokines remain stable for up to 2 years at this temperature (de Jager et al., 2009). Once the collection of all samples was completed, the stored sera were analyzed for IL-6 and TNF-α.
Statistical analysis
The data were compiled, analyzed, and interpreted using appropriate statistical methods with Statistical Package for Social Sciences (IBM SPSS Statistics, Software version 25, United States). Categorical variables were expressed as frequencies and percentages, while continuous variables were summarized as mean with standard deviation. Comparisons between groups were performed using two-sample t-tests (Student’s t-test). Results were stated with 95% confidence interval (CI), and a P value < 0.05 was considered statistically significant. The sensitivity, specificity, PPV, NPV, diagnostic efficiency, and the area under the curve of the test were determined for the optimal cutoff values using ROC analysis.
Results
A total of 300 neonates with at least two risk factors for sepsis were evaluated. Of these, 100 (33.3%) were diagnosed with neonatal sepsis (cases), while 200 (66.7%) were sepsis-negative (controls). Baseline characteristics are summarized in Table 1. No significant intergroup differences were noted in gender distribution, birth weight category, birth order, or place of delivery. However, neonates with sepsis presented earlier (<72 h) and were more frequently delivered vaginally compared with controls (P < 0.05).
Baseline Characteristics of Study Population (N = 300)
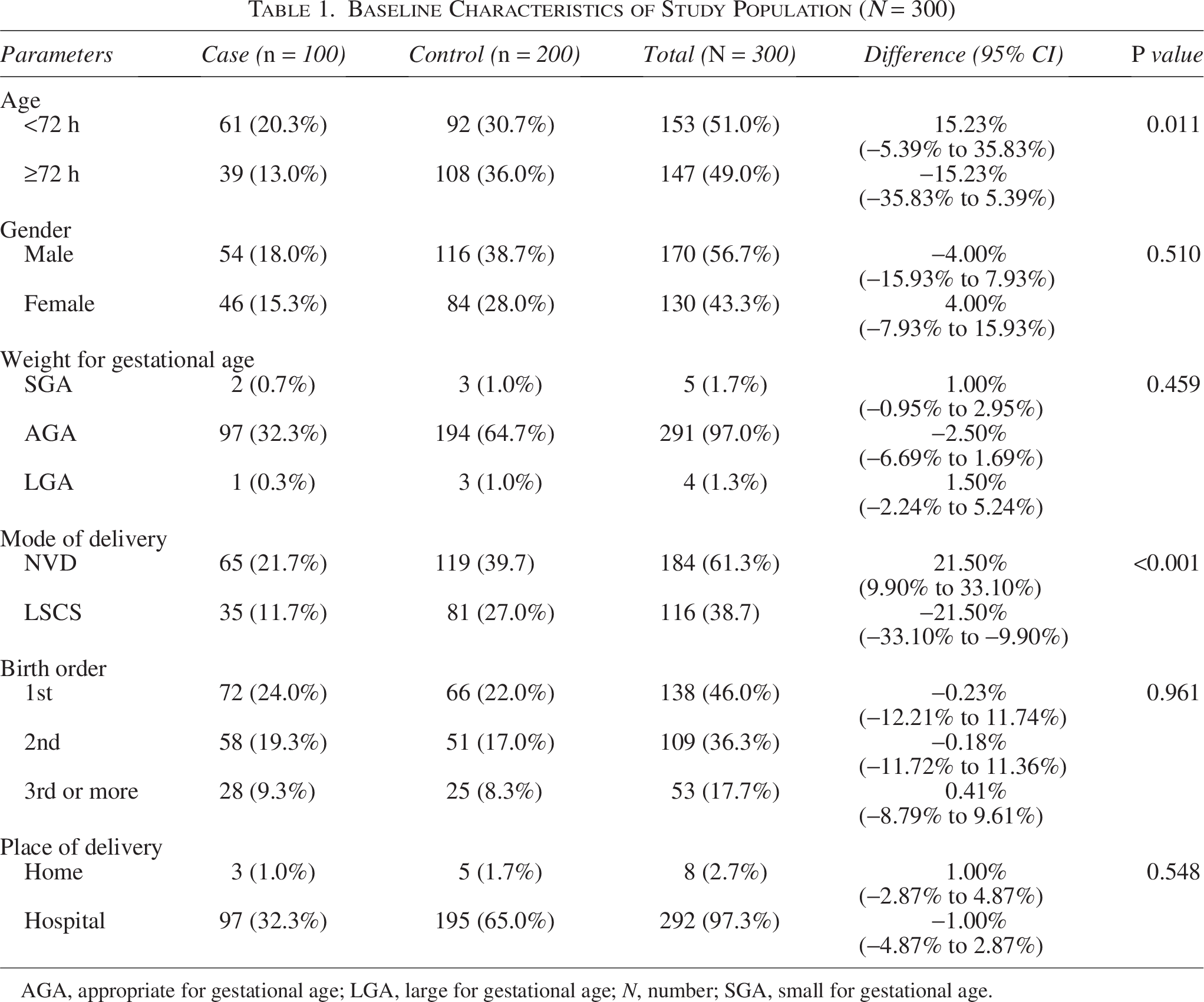
AGA, appropriate for gestational age; LGA, large for gestational age; N, number; SGA, small for gestational age.
Comparison of laboratory parameters demonstrated significantly elevated levels of TNF-α, IL-6, PCT, CRP, TLC, ANC, micro-ESR, and I/T ratio in cases versus controls (all P < 0.001; Table 2).
Comparison of Studied Biomarkers and Sepsis Screening Parameters Between Cases and Controls
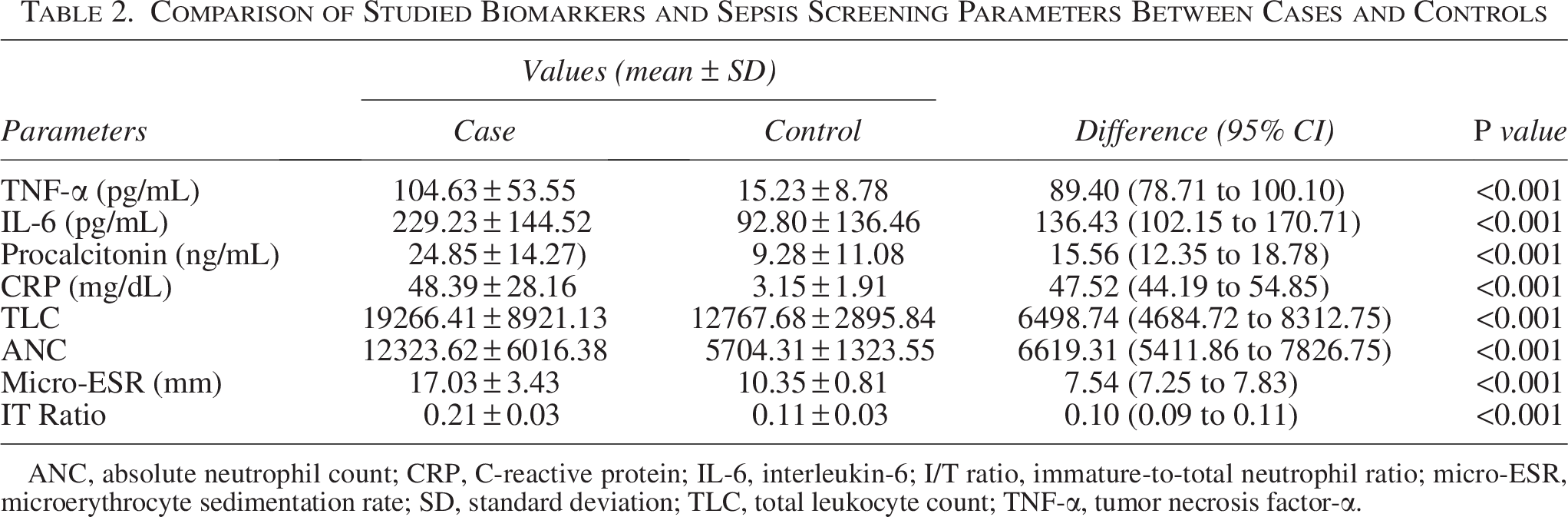
ANC, absolute neutrophil count; CRP, C-reactive protein; IL-6, interleukin-6; I/T ratio, immature-to-total neutrophil ratio; micro-ESR, microerythrocyte sedimentation rate; SD, standard deviation; TLC, total leukocyte count; TNF-α, tumor necrosis factor-α.
The diagnostic performance of individual parameters is presented in Table 3 and Figure 1. Among conventional markers, CRP achieved nearly perfect diagnostic accuracy [area under the curve of the receiver operating characteristic (AUROC) 0.991, sensitivity 96%, specificity 99.5%]. Among studied biomarkers, TNF-α displayed the highest discriminative ability (AUROC 0.990, sensitivity 94.0%, specificity 100%), followed by IL-6 and PCT. TLC and ANC also demonstrated fair diagnostic utility, though with lower sensitivity.
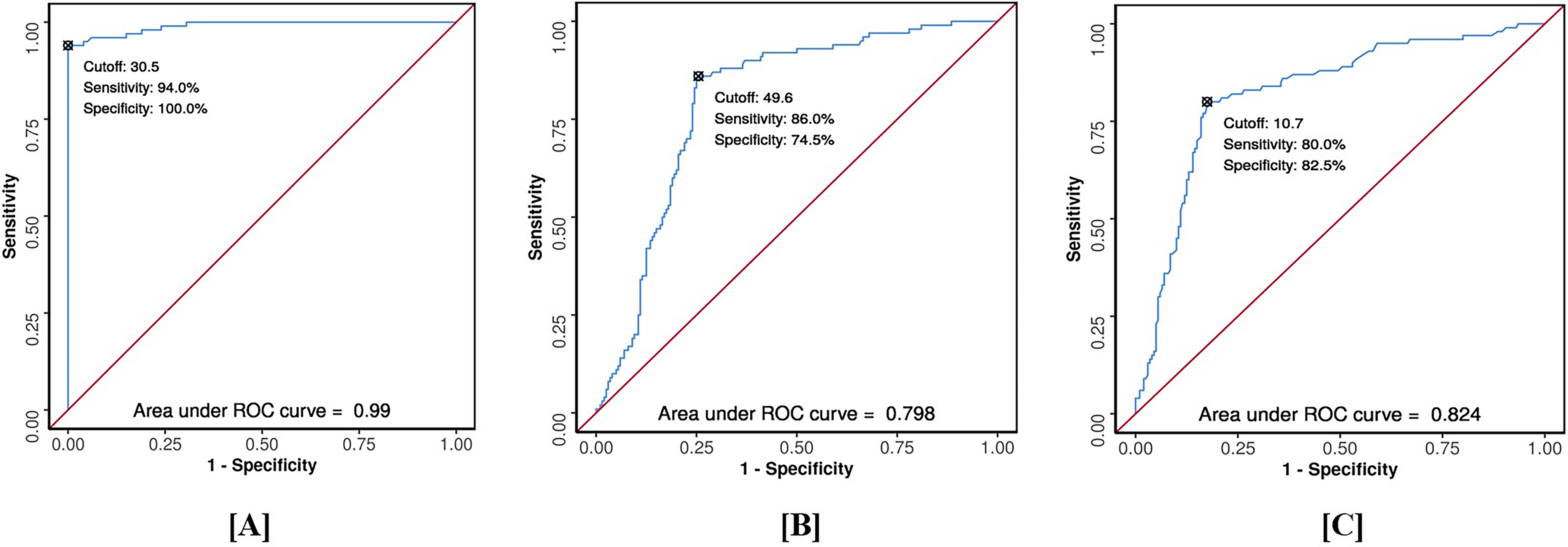
The highest diagnostic performance of tumor necrosis factor-α
Diagnostic Performance of Studied Biomarkers and Sepsis Screening Parameters
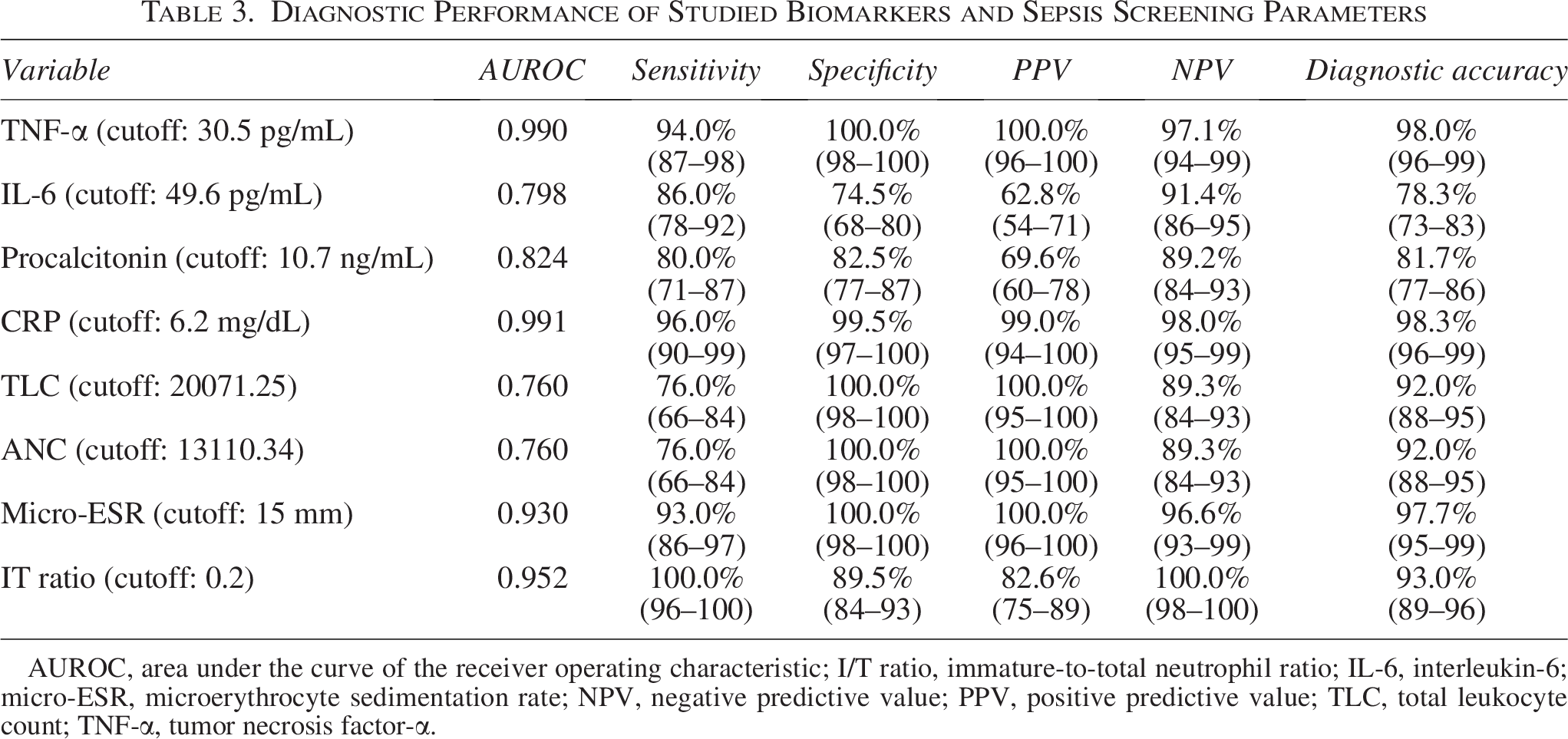
AUROC, area under the curve of the receiver operating characteristic; I/T ratio, immature-to-total neutrophil ratio; IL-6, interleukin-6; micro-ESR, microerythrocyte sedimentation rate; NPV, negative predictive value; PPV, positive predictive value; TLC, total leukocyte count; TNF-α, tumor necrosis factor-α.
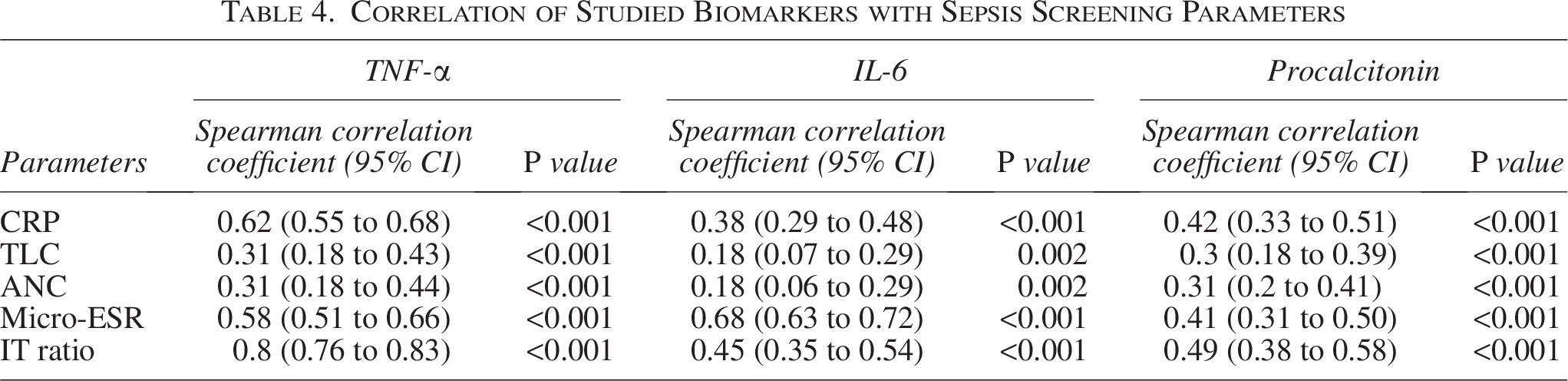
Correlation analysis (Table 4) revealed that TNF-α correlated strongly with CRP (r = 0.62) and I/T ratio (r = 0.80). IL-6 showed the strongest correlation with micro-ESR (r = 0.68) and a moderate correlation with I/T ratio (r = 0.45). PCT exhibited moderate associations with CRP (r = 0.42), I/T ratio (r = 0.49), and ANC (r = 0.31).
Correlation of Studied Biomarkers with Sepsis Screening Parameters
Discussion
This study evaluated the diagnostic performance of the biomarkers TNF-α, IL-6, and PCT against the conventional sepsis screen components in neonates with suspected sepsis. All three biomarkers were significantly elevated in septic neonates compared with controls, highlighting their potential as adjuncts to conventional screening.
Tumor necrosis factor-α
TNF-α levels were markedly higher in neonates with sepsis compared with controls, with an AUROC of 0.99 and excellent diagnostic accuracy (sensitivity 94%, specificity 100%). These findings are consistent with previous studies, which have also demonstrated high diagnostic utility across both early- and late-onset sepsis (Lv et al., 2014; Mishra et al., 2006; Kocabaş et al., 2007; Ye et al., 2017).
The rapid release of TNF-α within 1–2 h of infection, preceding a rise in CRP, makes it particularly attractive for early diagnosis. Its high specificity also reduces the risk of false positives. However, its short half-life necessitates careful timing of sample collection, and the cost and limited availability of ELISA-based assays may restrict widespread use. The robust accuracy observed in our study may, in part, reflect the carefully determined cutoff value and a well-powered control group, strengthening the case for TNF-α as a dependable early marker. Its levels might correlate with the severity of sepsis, potentially helping in risk assessment.
Interleukin-6
IL-6 is a key pro-inflammatory cytokine in the acute-phase response. In our cohort, mean IL-6 levels were significantly higher in septic neonates (229.23 pg/mL vs. 92.8 pg/mL in controls, P < 0.001), with an AUROC of 0.79. At a cutoff of ≥ 49.6 pg/mL, IL-6 showed high sensitivity (86%) but modest specificity (74%). Previous literature paints a similar picture, although with some variations, concluding that IL-6 is a valid and accurate marker but stressing the need to combine it with other lab tests and clinical signs (Chiesa et al., 2001; Sharma et al., 2018; Hofer et al., 2012; Eichberger and Resch, 2022). Interestingly, IL-6 levels did not correlate strongly with TNF-α, suggesting these cytokines peak at different stages of sepsis progression (Kocabaş et al., 2007). This temporal variability may explain discrepancies across studies and highlights the potential value of serial measurements. Although IL-6 alone lacks the specificity needed for definitive diagnosis, its rapid elevation makes it useful in combination with other markers for early detection.
Procalcitonin
PCT was significantly elevated in septic neonates (24.85 ng/mL vs. 9.28 ng/mL in controls, P < 0.001) with good diagnostic accuracy (AUROC 0.824). At a cutoff ≥ 10.7 ng/mL, it achieved 80% sensitivity and 82% specificity, comparable to previous reports (Bharti et al., 2020; Charles et al., 2018; Eschborn and Weitkamp, 2019; Sastre et al., 2007). PCT demonstrated moderate correlations with CRP, I/T ratio, and ANC, but not with TNF-α or IL-6, suggesting it reflects a different phase of the host response.
PCT offers practical advantages over conventional markers: its early rise within 2–4 h of infection, peak at 6–12 h, and rapid decline with recovery provide dynamic diagnostic and monitoring utility. Moreover, its high negative predictive value supports antibiotic stewardship by enabling earlier discontinuation of therapy. However, physiological elevations in the first 48 h of life, as well as false positives in conditions such as asphyxia or intracranial hemorrhage, must be considered.
Synergistic use of biomarkers and sepsis screen parameters
Our findings support the view that no single biomarker is sufficient for reliably diagnosing neonatal sepsis. A multimodal approach combining conventional markers with cytokines and PCT appears most effective. In our study, CRP, micro-ESR, TNF-α, and I/T ratio individually demonstrated very high diagnostic accuracy (AUROC > 0.90), while IL-6 and PCT provided additional value when used in combination.
Previous studies have also advocated such strategies. Lam and Ng (2008) reported improved sensitivity with combined IL-6 and CRP, while Eichberger et al. (2022) showed enhanced diagnostic yield with PCT plus IL-6 or CRP. Cortese et al. (2016) and Hincu et al. (2020) likewise endorsed dual-marker approaches for early and reliable detection.
Variability in biomarker levels in neonatal sepsis rests on the complex and dynamic nature of the neonatal immune response and metabolic changes during infection. Neonatal sepsis triggers a highly regulated cascade involving immune cell activation, which varies based on the pathogen type, host genetic factors, and presence of comorbidities, affecting the reliability of biomarker-based assessments. Understanding these sources of variation is essential for accurate interpretation and clinical utility. Similarly, findings from our study confirm that individual biomarkers lack sufficient standalone diagnostic power; TNF-α correlated strongly with CRP and I/T ratio, IL-6 with micro-ESR, and PCT with I/T ratio, suggesting these markers reflect complementary aspects of the inflammatory cascade. Cost and accessibility remain limitations in many low-resource settings. Integrating these biomarkers into diagnostic workflows could not only improve early recognition and management but also reduce unnecessary antibiotic exposure, an essential step in mitigating antimicrobial resistance.
Limitations
This study was conducted at a single tertiary care center, which may limit the generalizability of its findings to wider neonatal populations. Although the sample size was adequate for statistical analysis, it may not fully capture the heterogeneity of neonatal sepsis across different clinical settings. Serial biomarker measurements were not performed, precluding assessment of their dynamic trends during disease progression or treatment response. We did not include pathogen-specific data, though different organisms may affect cytokine levels. Furthermore, preterm neonates were excluded, restricting the applicability of these findings to this high-risk group, in whom biomarker kinetics often differ. Finally, the limited sensitivity of blood culture, the diagnostic gold standard, raises the possibility of misclassification of some cases.
Conclusion
This study underscores the diagnostic value of TNF-α, IL-6, and PCT in neonatal sepsis, with TNF-α demonstrating the highest accuracy among the biomarkers evaluated. While conventional markers such as CRP and the I/T ratio retain clinical utility, their delayed response limits their role in early detection. Our findings suggest that combining early-phase cytokines with established screening tools provides a more comprehensive and practical diagnostic framework. Incorporating these biomarkers into routine clinical practice has the potential to enhance early recognition of sepsis, facilitate timely initiation of antibiotic therapy, and improve survival outcomes. Equally important, their judicious use may enable earlier discontinuation of antibiotics in nonseptic neonates, thereby contributing to antimicrobial stewardship and reducing the burden of resistance.
Authors’ Contributions
Durgesh K.: Conceptualization, methodology, resources, and writing—original draft. Dinesh K.: Project administration and formal analysis. N.S.: Validation, formal analysis, and investigation. P.S.: Formal analysis and investigation. M.A.: Writing—review and editing. I.K.S.: Supervision, project administration, and funding acquisition. A.K.: Project administration and investigation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors declare that this study has not received any financial grant or sponsorship.