
Abstract
This investigation examined whether initially elevated serum cytokine concentrations associate with a lower serum 25-hydroxyvitamin D (25(OH)D) increase shortly after initiating supplemental vitamin D. This secondary analysis combined data from separate randomized, double-blind, placebo-controlled studies consisting of reportedly healthy adults and individuals with knee osteoarthritis who received supplemental vitamin D. Subjects were separated into 2 groups based on serum IL-6 concentrations at baseline (Bsl; prior to supplemental vitamin D): (1) non-elevated IL-6 (<2.5 pg/mL; n = 22) or (2) elevated IL-6 (≥2.5 pg/mL; n = 11). Reportedly healthy adults and knee osteoarthritis subjects with elevated IL-6 were matched (1:2) to those with non-elevated IL-6. Matching was based on condition (healthy adults and knee osteoarthritis), age (±3.0 y), sex, body mass index (±3.0 kg/m2), and dose of supplemental vitamin D (cholecalciferol, 4,000 or 8,000 IU/d). Serum cytokine concentrations at Bsl and serum 25(OH)D concentrations at Bsl and following 7 and 28-d of daily vitamin D supplementation are reported here. Serum IL-6 and other cytokines (GM-CSF, IL-10, IL-13, IL-1β, IL-2, IL-4, IL-5, IL-7, IL-8, and TNF-α) were significantly increased in the elevated compared to the non-elevated IL-6 group at Bsl (all P < 0.05). Serum 25(OH)D concentrations at Bsl, 7-d, and 28-d were not significantly different between IL-6 groups. The increase in serum 25(OH)D from Bsl to 7-d (7-dΔ) was significantly lower in the elevated compared to the non-elevated IL-6 group (P < 0.05). The 7-dΔ in serum 25(OH)D displayed modest inverse associations with Bsl serum 25(OH)D (β = −0.46, P < 0.01) and IL-6 (β = −0.43, P < 0.01). However, the 28-dΔ in serum 25(OH)D was inversely associated with Bsl serum 25(OH)D (β = −0.57, P = 0.01) but not with Bsl serum IL-6 (β = 0.10, P = 0.31). We conclude that the serum 25(OH)D response to supplemental vitamin D is temporarily blunted with elevated baseline circulating IL-6 and other cytokines, but this response diminished as supplementation continued.
Introduction
Serum 25-hydroxyvitamin D (25(OH)D) is the most reliable indicator of vitamin D intake, storage, and status. A low serum 25(OH)D concentration is recognized as a causal detrimental in most cases of rickets and osteomalacia (Holick, 2007; Jones, 2008). Observational data also link low serum 25(OH)D concentrations with increased disease risk, morbidity, mortality, and elevated circulating cytokines, such as IL-1β, IL-2, IL-6, IFN-γ, and TNF-α (Amini Kadijani et al., 2021; Amirkhizi et al., 2022; Barker et al., 2013a; Bellia et al., 2013; De Vita et al., 2014; Devaraj et al., 2011; Fu et al., 2021; Inanir et al., 2004; Liu et al., 2025; Riazati et al., 2025; Srikanth et al., 2016; Vayrynen et al., 2016; Wesselink et al., 2020).
The most biologically active form of vitamin D, 1,25-dihydroxyvitamin D (1,25(OH)D) (Holick, 2006), exerts immunomodulatory and anti-inflammatory properties (Hewison, 2011). These physiological processes are moderated through the vitamin D receptor and response elements and more rapidly through membrane receptors and second messengers (Dusso et al., 2005). Based on in vitro anti-inflammatory properties and elevated circulating cytokines with low serum 25(OH)D, it is postulated that increasing serum 25(OH)D lowers systemic inflammation. However, increasing serum 25(OH)D through supplemental vitamin D has produced inconsistent results on circulating cytokine concentrations (Bouillon et al., 2019).
A second premise suggests that inflammation lowers serum 25(OH)D concentrations (Barker et al., 2012b; Henriksen et al., 2014; Louw et al., 1992; Reid et al., 2011; Smolders et al., 2021), which confounds the interpretation of vitamin D status (Duncan et al., 2012; Ghashut et al., 2014). Evidence supporting this hypothesis includes the inverse association between serum IL-6 and other inflammatory indices (e.g., C-reactive protein and neutrophil-to-lymphocyte ratio) with circulating 25(OH)D concentrations (Akbas et al., 2016; Amini Kadijani et al., 2021; Amirkhizi et al., 2022; Barker et al., 2012b; Borgermann et al., 2012; De Vita et al., 2014; Duncan et al., 2012; Fu et al., 2021; Louw et al., 1992; Reid et al., 2011; Riazati et al., 2025; Smolders et al., 2021; Vayrynen et al., 2016). In a small sample size study consisting of male participants, lipopolysaccharide increased plasma IL-6, IL-8, and TNF-α and decreased plasma 25(OH)D concentrations (Smolders et al., 2021). Plasma 25(OH)D concentrations returned to baseline levels following the cessation of LPS infusion, indicating that the reduction in circulating vitamin D induced by inflammation was reversed upon removal of the inflammatory stimulus.
These observations support a dynamic, bidirectional relationship between vitamin D and inflammation (Cannell et al., 2014). Despite these observations, it remains unclear whether baseline inflammation impacts the efficacy of supplemental vitamin D to increase serum 25(OH)D. Therefore, the purpose of this investigation was to examine the early change in serum 25(OH)D following supplemental vitamin D in subjects with disparate serum cytokine concentrations at baseline. We hypothesized that elevated baseline serum cytokine concentrations are associated with an initially blunted serum 25(OH)D increase to supplemental vitamin D. To experimentally examine disparate cytokine concentrations, subjects were stratified based on a serum IL-6 concentration (i.e., < vs ≥ 2.5 pg/mL) demonstrated to increase disability risk and decrease cardioprotection (Beavers et al., 2015; Ferrucci et al., 1999).
Methods
This investigation consisted of a secondary analysis of separate randomized, double-blind, placebo-controlled studies conducted in reportedly healthy adults (Barker et al., 2015) and subjects with knee osteoarthritis (Barker et al., 2019) who underwent a supplemental vitamin D intervention. Some data has been previously reported (Barker et al., 2019; Barker et al., 2015). Pooled data reported here includes new serum 25(OH)D and/or cytokine results and analyses. Subjects were informed of and provided written and verbal consent to the study protocols and procedures. The Urban Central Region Institutional Review Board at Intermountain Health (Salt Lake City, UT, USA) approved these studies.
Pooled cohorts
Reportedly healthy subjects
Reportedly healthy and modestly active (minimum of 30 min of continuous physical activity or exertion at least 3 times per week during the previous year) adults (≥18 y) were recruited to participate in this study, as described (Barker et al., 2015). In brief, subjects were excluded from participation if: they were taking a dietary supplement, using tobacco, using prescribed or recommended medication, reported a known history of any disease or condition requiring medical attention, suffered a leg injury during the previous year that required the use of crutches, were planning on increasing or decreasing the amount of time spent in the sun or tanning bed, traveling south of 37° N in latitude during study participation, or morbidly obese (body mass index (BMI) > 40 kg/m2). Following enrollment, subjects were randomly assigned to 1 of 3 groups: (1) placebo or supplemental vitamin D (cholecalciferol) at (2) 4,000 IU or (3) 8,000 IU. Supplements were taken daily for 35 days. Some of the results have been previously reported (Barker et al., 2015).
Knee osteoarthritis subjects
Modestly active (minimum of 30 min of continuous exercise or physical activity or exertion 3 times per week during the previous year) subjects older than 18 but younger than 60 years of age were initially recruited and consented to study participation, as described (Barker et al., 2019). For brevity, subjects were excluded from participation if: they had a recent (within 2 years) surgery on the involved or non-involved leg, or reported a known history of any disease or condition requiring medical attention. Subjects were also excluded from participation if they were pregnant, using a daily dietary supplement or vitamin during the previous year, morbidly obese, were smokers, planning on increasing or decreasing the amount of time spent in the sun or tanning bed, or traveling south of 37° N in latitude during study participation (Barker et al., 2019).
Each subject provided a fasting blood draw sample during eligibility screening. Subjects with hypo- (total calcium < 8.4 mg/dL) or hypercalcemia (total calcium > 10.4 mg/dL), hypo- (parathyroid hormone < 12.0 pg/mL) or hyperparathyroidism (parathyroid hormone > 72.0 pg/mL), elevated rheumatoid factor (>15 IU/mL), or increased uric acid (females > 7.5 mg/dL; males > 8.5 mg/dL) were excluded from participation (Barker et al., 2019).
Potential subjects were further screened for unilateral knee pain, muscular weakness, and radiographical evidence of knee osteoarthritis. Subjects were excluded from participation if: (1) the Western Ontario and McMaster Universities Osteoarthritis Index pain score was <2 on any of the 5 questions in its subsection, (2) there was no evidence of muscular weakness (i.e., deficit in peak isokinetic knee extension or flexion torque at 60°/sec) in the involved compared to the non-involved leg, and (3) a Kellgren-Lawrence grade < 2 was scored in the involved knee as determined from X-ray images obtained on each knee in the anterior-posterior view at 45° of knee flexion (Kellgren and Lawrence, 1957).
After eligibility screening, subjects were randomly assigned to 1 of 2 supplement groups: (1) placebo or (2) vitamin D (cholecalciferol, 4,000 IU). Supplements were taken daily for 84 days. Some of the results obtained prior to (baseline), during (28-d), and at the conclusion of supplementing with vitamin D have been previously reported (Barker et al., 2019).
Placebo and vitamin D supplements
USANA Health Sciences, Inc. (Salt Lake City, UT, USA) generously donated and provided quality control analysis of vitamin D supplements (Barker et al., 2019; Barker et al., 2015).
Reportedly healthy and knee osteoarthritis subjects
During participation, subjects were asked to keep their diet consistent with their regular eating habits during the previous year and to refrain from the use of dietary supplements. Subjects were also instructed to refrain from physical activity and using aspirin, ibuprofen, naproxen sodium, acetaminophen, or other anti-inflammatory agents 72 h prior to a blood draw (Barker et al., 2019; Barker et al., 2015).
Study design and protocol
Subjects that underwent previous vitamin D supplementation (Barker et al., 2019; Barker et al., 2015) were separated into 2 groups based on baseline (Bsl; prior to supplemental vitamin D) serum IL-6 concentrations: (1) non-elevated IL-6 (NE-IL-6; < 2.5 pg/mL) or (2) elevated IL-6 (E-IL-6; ≥2.5 pg/mL). Reportedly healthy adults with E-IL-6 were matched (1:2) to those with NE-IL-6 based on age (±3.0 years), sex, BMI (±3.0 kg/m2), and dose of vitamin D (cholecalciferol, 4,000 or 8,000 IU/d). Knee osteoarthritic subjects with E-IL-6 were matched (1:2) to knee osteoarthritic subjects with NE-IL-6 based on age (±3.0 years), sex, BMI (±3.0 kg/m2), and dose of vitamin D (cholecalciferol, 4,000 IU/d). Investigators were blinded to serum 25(OH)D and cytokine (other than IL-6) concentrations during the matching process. The final analysis consisted of 33 subjects (NE-IL-6, n = 22; E-IL-6, n = 11).
Reported here are results obtained from fasting (10–12 h) blood samples obtained at Bsl and 7- and 28-days after starting daily vitamin D supplementation. Blood was drawn from the antecubital vein. Plasma and serum from non-gel Vacutainers were separated by centrifugation (VWR International, Clinical 50 Centrifuge, Radnor, PA, USA) at 1,068 g for 10 min within 20 min of sample collection. After centrifugation, plasma and serum samples were aliquoted into several different cryotubes and stored at −80°C until later analysis.
Analytical procedures
Serum cytokine concentrations were determined using the multiplex technology of Luminex (MAGPix; Austin, TX, USA) with a high-sensitivity kit (EMD Millipore, Billerica, MA, USA). Serum 25(OH)D concentrations were assessed using high-performance liquid chromatography and tandem mass-spectrometer (Barker et al., 2012a). Serum 25(OH)D concentrations ≤ 20, 21–29, or ≥ 30 ng/mL were classified as vitamin D deficient, insufficient, or sufficient, respectively (Holick et al., 2012). Plasma intact parathyroid hormone (iPTH) with calcium concentrations was measured using an electrochemiluminescent immunoassay (ARUP Laboratories, Salt Lake City, UT, USA).
Baseline (Bsl), 7-d, 7-d Δ (i.e., Bsl to 7-d), and 28-d Δ (i.e., Bsl to 28-d) in serum 25(OH) concentrations were not significantly different between reportedly healthy and knee osteoarthritis subjects after matching (Supplementary Table S1). Therefore, data from the previous supplemental vitamin D groups and cohorts were pooled for the analysis.
Statistical analysis
Data were checked for normality with a Shapiro-Wilk test before statistical analysis. Statistical significance was assessed with t-tests or Mann–Whitney U tests. A Pearson chi-square test was performed to assess the relationship between vitamin D status (i.e., deficient, insufficient, and sufficient) and IL-6 groups. A multiple linear regression was performed to determine the association of baseline serum 25(OH)D and IL-6 with the 7-d and 28-d Δ in serum 25(OH)D concentrations. Serum IL-6 was rank transformed for the multiple linear regression analysis. Statistical significance of serum 25(OH)D concentrations (i.e., baseline, 7-d, 28-d, 7-d Δ, and 28-d Δ) was analyzed using a one-way (previous supplemental vitamin D groups [4,000 IU and 8,000 IU in reportedly healthy adults and 4,000 IU in subjects with knee osteoarthritis]) analysis of variance. Significance was set at P < 0.05. Statistical analyses were performed using SYSTAT (version 13.1, Chicago, IL, USA).
Results
Baseline subject characteristics and serum cytokines
Subject sex, age, height, body mass, BMI, plasma iPTH, and plasma calcium were not significantly different between the NE- and E-IL-6 groups (Table 1). In addition to IL-6, serum concentrations of GM-CSF, IL-10, IL-13, IL-1β, IL-2, IL-4, IL-5, IL-7, IL-8, and TNF-α were significantly increased at Bsl in the E-IL-6 compared to those in the NE-IL-6 group (Table 2). Serum IFN-γ and IL-12 p70 were not significantly different between IL-6 groups.
Subject Characteristics at Bsl
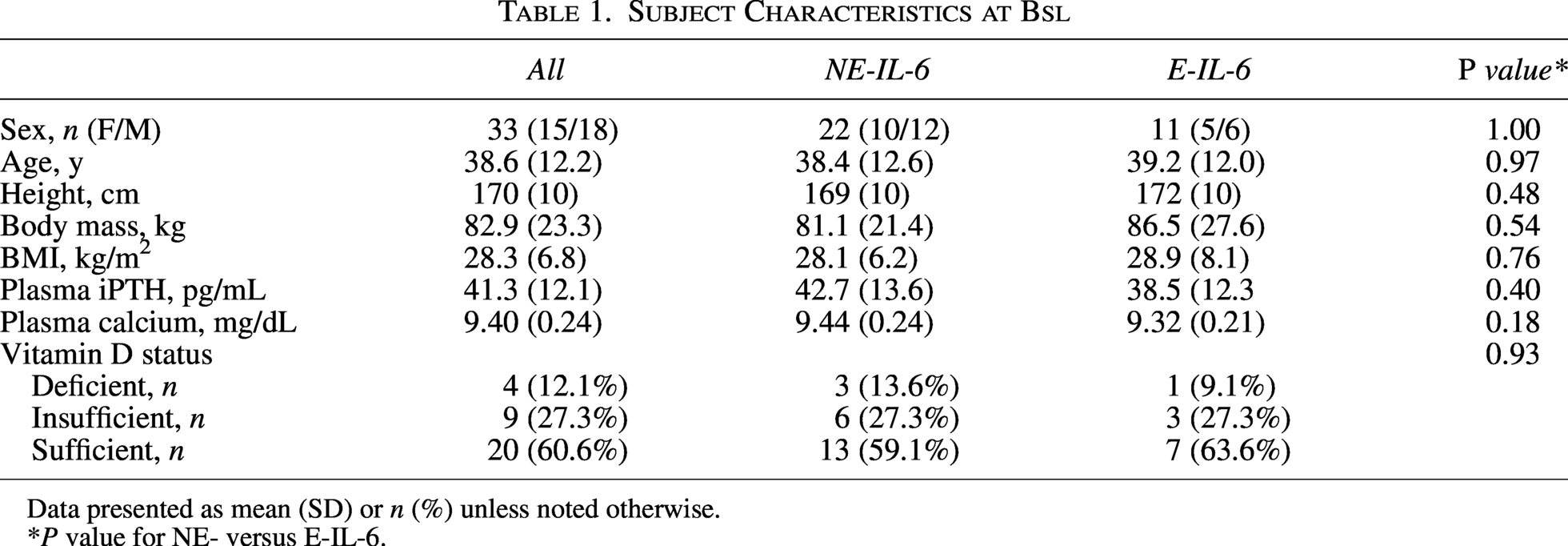
Data presented as mean (SD) or n (%) unless noted otherwise.
*P value for NE- versus E-IL-6.
Serum Cytokine Concentrations at Bsl
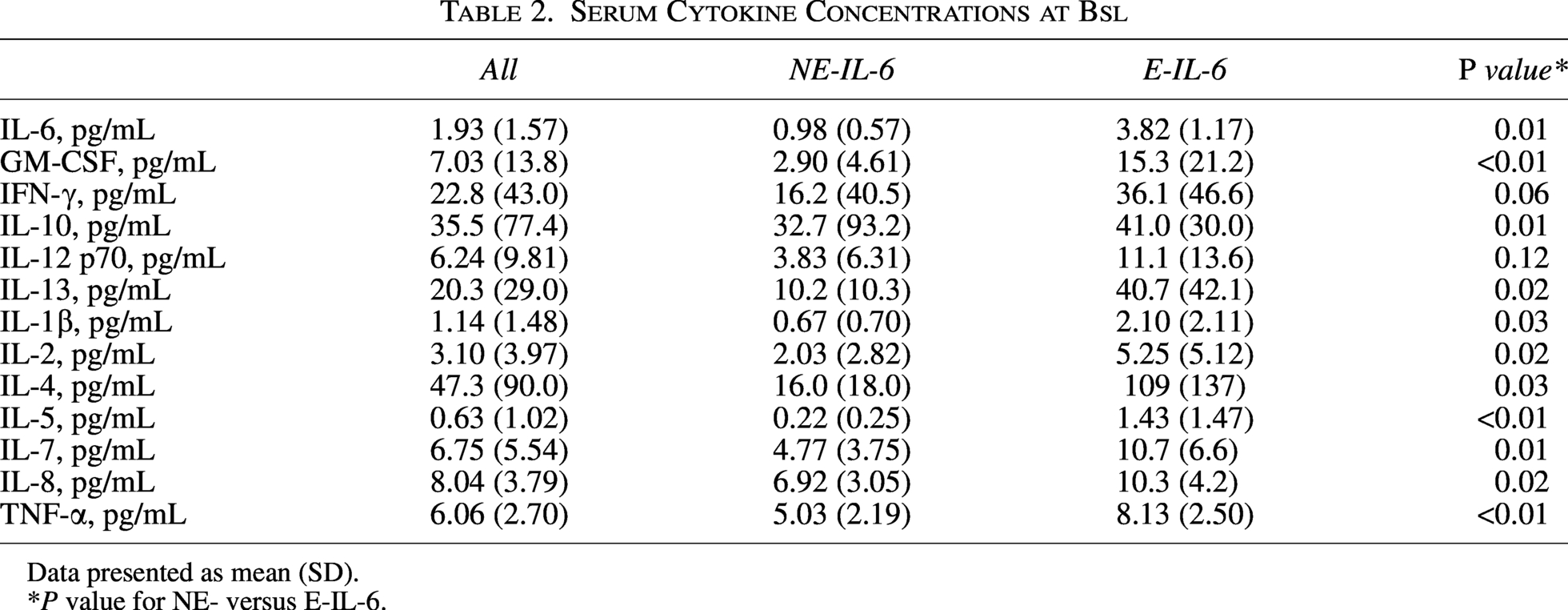
Data presented as mean (SD).
*P value for NE- versus E-IL-6.
Serum 25(OH)D concentrations
Approximately 59% of the subjects in the NE-IL-6 group and 64% of the subjects in E-IL-6 group possessed a serum 25(OH)D concentration deemed vitamin D sufficient at Bsl (P = 0.93, see Table 1). With supplemental vitamin D, serum 25(OH)D concentrations were increased at 28-d compared to Bsl and 7-d (Fig. 1). Serum 25(OH)D concentrations at Bsl, 7-d, and 28-d were not significantly different between IL-6 groups.
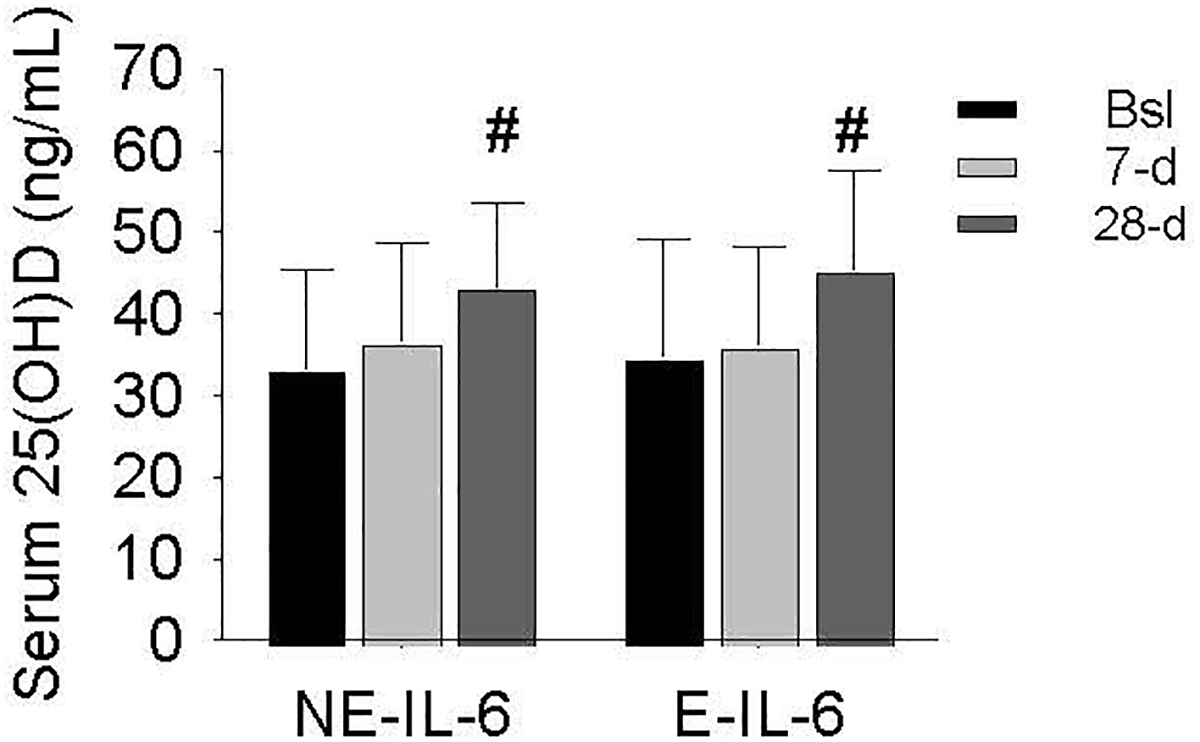
Serum 25(OH)D concentrations in the E- and NE-IL-6 groups. Serum 25(OH)D concentrations were significantly increased at 28-d (#P < 0.01 vs Bsl and 7-d). Serum 25(OH)D concentrations were not significantly different between IL-6 groups. Data presented as mean (SD).
Serum 25(OH)D concentrations changes
The 7-d Δ in serum 25(OH)D was significantly lower in E-compared to the NE-IL-6 group (Fig. 2A). However, the 28-d Δ in serum 25(OH)D was not significantly different between IL-6 groups (Fig. 2B).
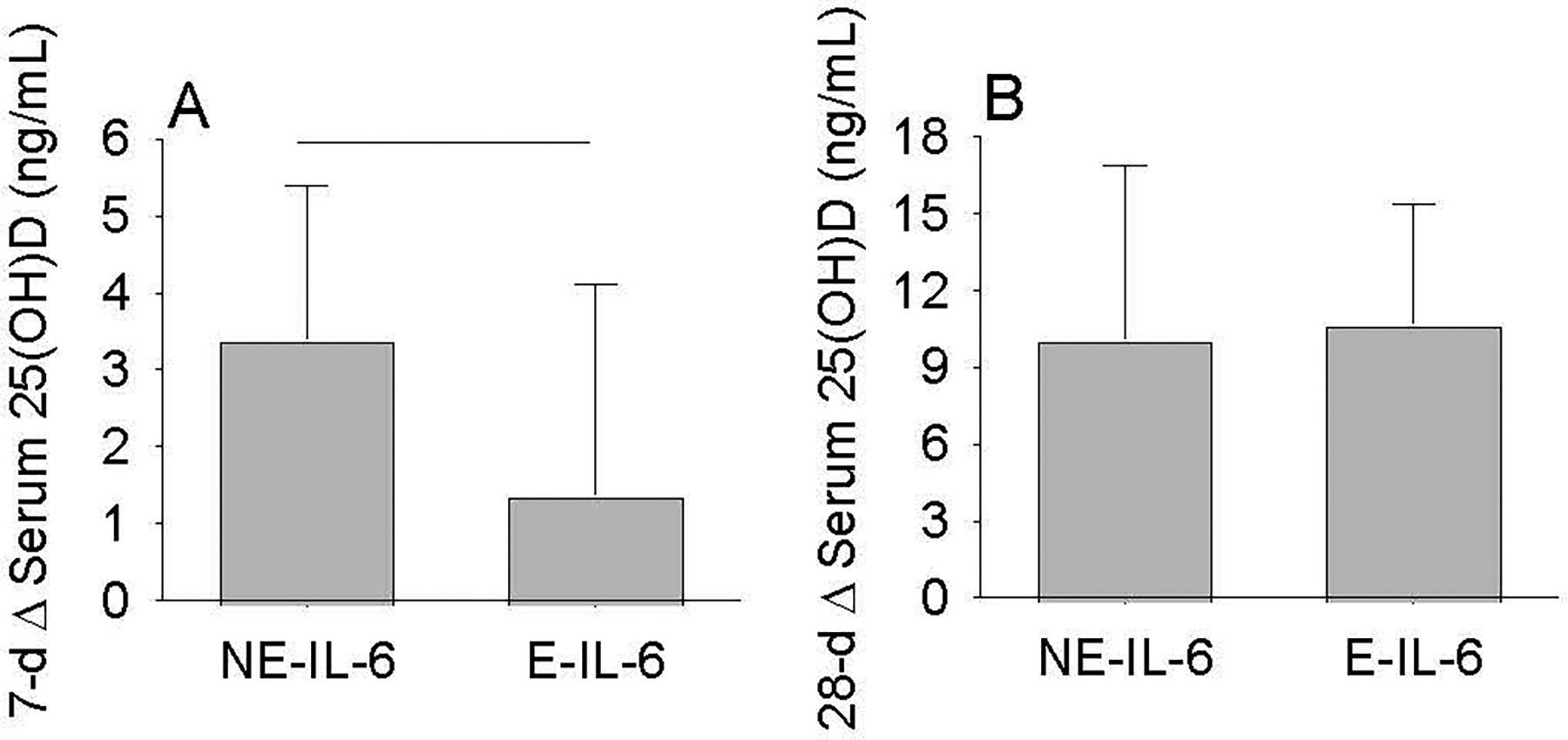
The 7- and 28-d Δ in serum 25(OH)D concentrations between IL-6 groups.
The 7-d Δ in serum 25(OH)D was significantly lower with vitamin D insufficiency and sufficiency compared to those with deficiency (Fig. 3A). The 28-d Δ in serum 25(OH)D was significantly lower with vitamin D sufficiency compared to vitamin D deficiency (Fig. 3B).
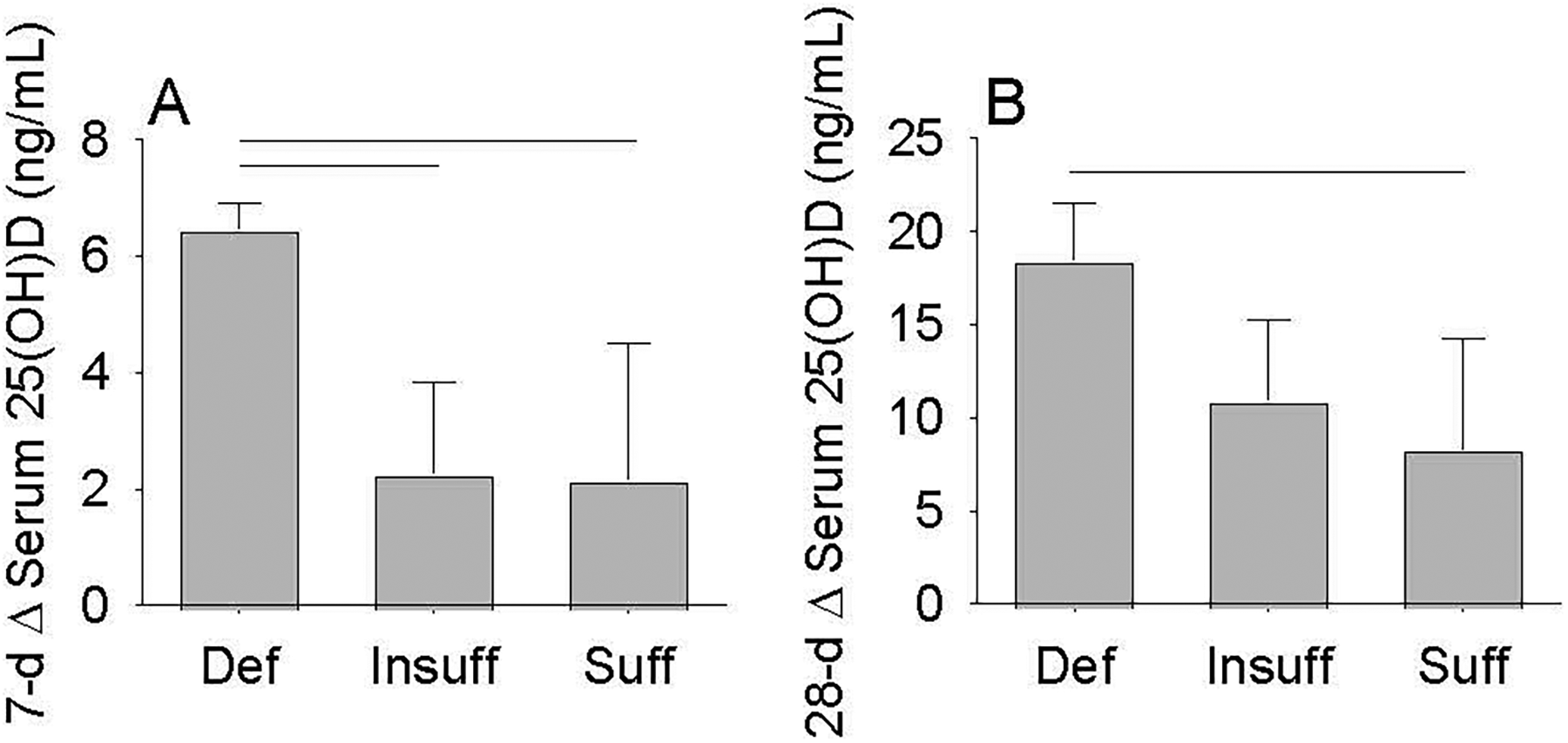
The 7- and 28-d Δ in serum 25(OH)D concentrations between vitamin D status groups.
The 7-d Δ in serum 25(OH)D displayed a modest inverse association with Bsl serum 25(OH)D and IL-6 (Table 3), while the 28-d Δ in serum 25(OH)D was inversely associated with Bsl serum 25(OH)D but not with Bsl serum IL-6 (Table 4).
Bsl Serum 25(OH)D and IL-6 Inversely Associated with the 7-d Δ in Serum 25(OH)D During Supplemental Vitamin D
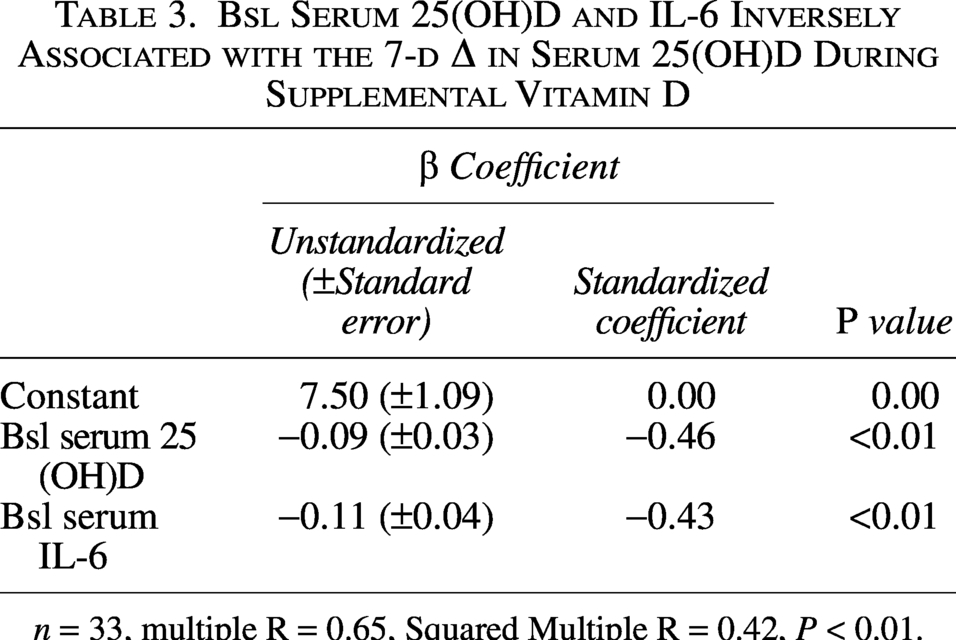
n = 33, multiple R = 0.65, Squared Multiple R = 0.42, P < 0.01.
Bsl Serum 25(OH)D but Not Bsl IL-6 Inversely Associated with the 28-d Δ in Serum 25(OH)D During Supplemental Vitamin D
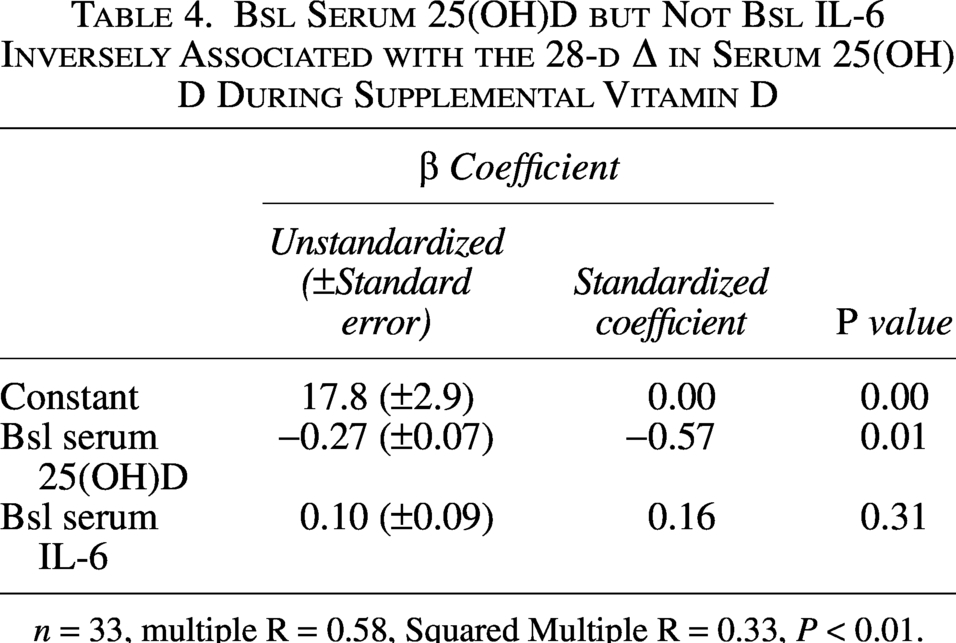
n = 33, multiple R = 0.58, Squared Multiple R = 0.33, P < 0.01.
Discussion
This investigation provides novel evidence that individuals with initially elevated serum IL-6 exhibit an increase in other serum cytokines at baseline and a temporarily blunted increase in serum 25(OH)D with supplemental vitamin D. The change in serum 25(OH)D, however, was not significantly different following 28-d of supplemental vitamin D between groups stratified by baseline serum IL-6 concentrations. These preliminary findings suggest that the efficacy of supplemental vitamin D to increase serum 25(OH)D was temporary blunted with elevated IL-6 and other cytokines at baseline in reportedly healthy adults with or without knee osteoarthritis.
Evidence demonstrates that IL-6 exposure increases DNA methyltransferase expression and activity (Hodge et al., 2001; Liu et al., 2015), which could contribute to a diminished serum 25(OH)D response to supplemental vitamin D through greater baseline DNA methylation of CYP2R1 (Zhou et al., 2014). Additionally, elevated serum IL-6 with low serum 25(OH)D concentrations has been associated with reduced CYP2R1 and increased CYP24A1 levels in children with sepsis (Huang et al., 2024), as well as decreased 1α-hydroxylase protein expression in vascular endothelial cells from middle-aged and older adults without clinical disease (Jablonski et al., 2011). These observations collectively indicate that elevated IL-6 may lower circulating 25(OH)D by suppressing its synthesis and/or accelerating its conversion to 1,25(OH)2D or 24,25-dihydroxyvitamin D. However, it is important to acknowledge that an elevated IL-6 alone is probably not the sole contributor to the attenuated serum 25(OH)D increase with supplemental vitamin D, as multiple cytokines capable of modulating vitamin D metabolism were concurrently increased in the E-IL-6 group.
In the E-IL-6 group, several cytokines were simultaneously increased, including IL-2, IL-4, IL-13, and TNF-α. Exposure to IL-2, IL-13, or TNF-α increases 1α-hydroxylase expression (mRNA and/or protein) and enzyme activity in various cell types (Hewison et al., 2003; Pryke et al., 1990; Reichel et al., 1987; Schrumpf et al., 2012; Zehnder et al., 2002), thereby enhancing the conversion of 25(OH)D to 1,25(OH)2D and reducing circulating 25(OH)D. Furthermore, IL-4 has been reported to promote the catabolism of 25(OH)D to 24,25-dihydroxyvitamin D through the upregulation of CYP24A1 (Edfeldt et al., 2010). Thus, it is plausible that the attenuated increase in serum 25(OH)D shortly after initiating supplemental vitamin D in the E-IL-6 group was influenced by the systemic elevation of multiple cytokines involved in the metabolism of vitamin D.
In conjunction with inflammatory-derived mediators, other factors may contribute to the findings of the present investigation. Calcium and phosphorus metabolism regulated by parathyroid hormone, dietary intake of vitamin D, sun exposure, body composition, race, and genetics are a few examples of other potential mediators that might influence the serum 25(OH)D response to supplemental vitamin D and warrant consideration in future research. In addition, it should be noted that it remains unknown whether the mechanisms underlying the decrease in serum 25(OH)D during inflammation similarly contribute to the blunted serum 25(OH)D response to supplemental vitamin D under inflammatory conditions, as cautiously suggested in this context.
The inverse association between the change in serum 25(OH)D with supplemental vitamin D and baseline serum IL-6 at 7-d but not at 28-d was expected and reasonably explained by several underlying determinants. First, this study consisted of reportedly healthy adults and otherwise healthy adults with knee osteoarthritis, cohorts presumably characterized with low or minimal inflammation. As a result, it was anticipated that the impact of an initially elevated systemic IL-6 (and/or other cytokines) on the serum 25(OH)D response to supplemental vitamin D would be temporary. Second, as supplementation duration continues, the anti-inflammatory and immune-modulatory properties of vitamin D could be accentuated by progressively increasing endogenous vitamin D levels that abrogate the initial deleterious impact of elevated IL-6 on the serum 25(OH)D response. Lastly, most participants (∼87.3%) had a baseline serum 25(OH)D concentration ≥ 21 ng/mL, which based on data provided elsewhere (Barker et al., 2013b; Trang et al., 1998), dampens the serum 25(OH)D response to supplemental vitamin D. Thus, the early and temporarily blunted increase in serum 25(OH)D with elevated IL-6 and other cytokines could reflect an initially mild or low inflammatory status and rising endogenous vitamin D levels with continued supplementation under physiological conditions, highlighting the importance of inflammation status when interpreting and predicting short-term vitamin D responses in clinical practice. The short-term findings here in otherwise healthy adults provide the basis for future investigations examining the impact of a greater inflammatory burden on the long-term serum 25(OH)D response to supplemental vitamin D in pathophysiological conditions. Investigations pursuing this objective would generate data to assist in the clinical decision-making process regarding appropriate vitamin D dosing strategies to achieve a desired serum 25(OH)D concentration in disease and illness characterized by hyper- and/or chronic inflammation.
In addition to those above, there are other limitations to this study worthy of discussion. The serum IL-6 concentration delineating elevated from non-elevated was based on studies conducted in different cohorts (Beavers et al., 2015; Ferrucci et al., 1999). Whether alternative IL-6 thresholds, or thresholds based on other cytokines, would provide more biologically relevant discrimination within the present cohorts remains unknown. Another limitation of this study is the relatively small sample size. Although subjects were matched by dose of supplemental vitamin D and stringent subject inclusion and exclusion criteria were previously implemented (Barker et al., 2019; Barker et al., 2015), it is unknown whether larger sample size studies would elicit similar results. Additionally, despite excluding subjects with a known disease (other than knee OA) or condition requiring medical attention, it is unknown whether baseline immune status, underlying chronic disease burden, and drug metabolism confounded study results and should be considered with future investigations. Sample size constraints also limited the number of variables included in the multiple linear regression analyses; only baseline serum 25(OH)D and IL-6 were selected a priori as predictors of the changes in serum 25(OH)D. Finally, differentiating vitamin D insufficiency from sufficiency was based on traditionally recognized serum 25(OH)D concentrations (Holick et al., 2011; McAlindon et al., 1996), as the absence of consensus among major professional organizations hinders the definition of an actionable vitamin D status across different cohorts and disease states (Demay et al., 2024; McCartney et al., 2024).
Conclusion
The serum 25(OH)D response to supplemental vitamin D was blunted with elevated baseline circulating IL-6 and other cytokines. The blunted increase in serum 25(OH)D diminished as supplementation continued. These findings collectively suggest that a systemic, multi-factorial hyper-inflammatory state might delay the early serum 25(OH)D response to supplemental vitamin D in otherwise healthy adults. Research examining the short- and long-term impact of a high-grade, chronic inflammation on the serum 25(OH)D response to supplemental vitamin D in various pathophysiological or disease states is desired.
Authors’ Contributions
T.B.: Conceptualization, methodology, formal analysis, investigation, resources, writing—original draft, writing—review and editing, visualization, supervision, project administration, and funding acquisition. V.E.R.: Methodology, validation, formal analysis, investigation, data curation, and writing—review and editing. V.T.H.: Methodology, investigation, data curation, and writing—review and editing.
Statements and Declarations
This study was conducted in accordance with the Declaration of Helsinki and The Urban Central Region Institutional Review Board at Intermountain Health (Salt Lake City, UT USA; IRB #1024174 on January 19th, 2017 and #1023358 on May 4, 2011) approved this study.
Consent to Participate
Subjects were informed of and provided written and verbal consent to the study protocols and procedures.
Data Availability
The datasets generated and analyzed during this study are not publicly available due data containing potentially identifying or sensitive patient information but are available from the corresponding author upon reasonable request.
Footnotes
Author Disclosure Statement
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The studies reported here were funded in part by the Intermountain Research and Medical Foundation (Intermountain Health, Salt Lake City, UT USA) and USANA Health Sciences, Inc. (Salt Lake City, UT USA). Data was collected at The Orthopedic Specialty Hospital (Intermountain Health, Salt Lake City, UT USA).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.