
Abstract
Interest in identifying biomarkers that reflect spine condition and support therapy monitoring has grown. Since low-grade inflammation and comorbidities can complicate treatment, they should be considered in research. Vaspin (SERPINA12) has been linked to low back pain (LBP) severity and disability, highlighting its potential as a biomarker connecting LBP and adipose tissue inflammation. The study aimed to assess the effect of traction therapy on serum vaspin levels and compare responses between women with obesity and normal BMI. A secondary aim was to explore associations between vaspin, LBP severity, disability scores, and selected inflammatory markers. It is a prospective clinical trial. Women aged 34–50 years with chronic LBP were divided into two groups: those with normal BMI and those with obesity. Both groups underwent 20 30-min sessions of lumbar traction therapy. At baseline and after therapy, LBP intensity, the Oswestry Disability Index (ODI), and the Roland–Morris Disability Questionnaire (RMDQ) were assessed, and blood samples were collected for analysis of vaspin, RANTES, interleukin (IL)-2, IL-17A, IL-4, and IL-10. After completing the traction therapy, there was a significant decrease in LBP, ODI, and RMDQ and an increase in the circulating levels of IL-10, regardless of BMI. However, vaspin concentration increased significantly only in women with normal BMI. Post-therapy, vaspin negatively correlated with ODI. IL-4 and IL-17A levels also correlated with vaspin, positively in women with normal BMI and negatively in those with obesity. Obesity-related inflammation may alter the biochemical response to traction therapy. Increases in vaspin concentration were found exclusively in women with normal BMI, indicating a possible BMI-dependent association between circulating vaspin concentrations and response to therapy.
Registration: The study was registered at ClinicalTrials.gov with the ID number NCT04507074.
Introduction
Low back pain (LBP) may be a symptom of complex conditions, such as aging, degenerative changes or trauma of the spinal structures, in which the direct cause of pain is often inflammation (Lassiter et al., 2025). The most reliable methods for assessing changes in the spine are imaging techniques, but both degenerative changes and healing processes in spinal structures occur very slowly, making them difficult to detect during short-term therapeutic interventions. For this reason, the search for new biomarkers reflecting the condition of the spine, which could be used to monitor the effects of various therapies, has become a popular subject of research in recent years. Candidates for such biomarkers include numerous proteins detectable in patients’ blood; however, most of these primarily indicate inflammation.
The presence of comorbidities can intensify the inflammatory processes, complicating not only patient treatment, but also the monitoring of their condition. In the context of inflammation, special attention is generally given to two key processes: low-grade inflammation, which accompanies not only certain diseases, but also common conditions such as obesity; and the accumulation of free fatty acids (FFAs) and their derivatives in muscle tissue, which impairs fiber contractility (Carter et al., 2019), and contributes to the development of LBP (Teichtahl et al., 2015). The excessive influx of FFAs in the plasma of individuals with obesity, along with their incomplete β-oxidation, leads to increased production of reactive oxygen species (Tumova et al., 2016) and the transformation of FFAs into lipotoxic derivatives (Carter et al., 2019). These processes—combined with adipocyte hypoxia, cell death, and inflammasomes activation—initiate an inflammatory response in adipose tissue (Zatterale et al., 2019), characterized by a significant increase in the secretion of adipokines and other cytokines (Kawai et al., 2021), thereby affecting the body’s overall inflammatory status.
In LBP therapies, the clinically significant and most important variables for the patient are the level of pain and pain-related functional ability. Lumbar traction has already shown the beneficial effects and a statistically significant reduction in pain and functional improvement scores (Liu et al., 2021). In the present study, we were interested in whether, in patients with chronic LBP, alongside subjectively assessed improvement of their condition, there are detectable changes both in the primary outcomes of treatment, such as the LBP-related functionality, and the secondary outcomes, i.e., in the biochemical milieu. To achieve this aim, we examined two groups of patients with LBP: those with a normal weight (BMI = 18.5–24.9) and those with obesity (BMI ≥ 30). We assumed that the presence of obesity, associated with excess adipose tissue and a higher risk of comorbidities, may be linked to an initially different inflammatory status and a different response to LBP therapy.
Recent studies have shown significant associations between the adipokine vaspin (visceral adipose tissue-derived serine protease inhibitor, SERPINA12) and LBP-related phenotypes, such as LBP severity and LBP disability (Tarabeih et al., 2020), and the occurrence of facet joint osteoarthritis (Tarabeih et al., 2022). Vaspin is an adipokine, but its impact extends far beyond fat tissue. In addition to its proven effect on maintaining insulin sensitivity (Choi et al., 2013), animal studies have shown that vaspin improves the metabolic status of the entire organism and activates osteogenesis (Wang et al., 2020). Its anti-inflammatory effect has also been noted (Bao et al., 2017; Zieger et al., 2018). There is a substantial bulk of scientific evidence showing that the effect of vaspin on the body is positive, and its enhanced secretion probably occurs in various unfavorable health conditions, e.g., in type II diabetes (Wang et al., 2024) or obesity accompanied by other disorders, such as dyslipidemia, insulin resistance or low-grade inflammation (Pilarski et al., 2023). As far as we are aware, there are no published studies examining the effect of physical therapy treatment on circulating vaspin levels in patients with LBP.
The primary aim of the present study, in this connection, was to determine the impact of traction therapy on serum vaspin concentrations and whether this effect differs between women with obesity and those with a normal BMI. We also examined the association between vaspin levels and LBP intensity and disability scores. If the hypothesis—that vaspin concentrations change in conjunction with a decrease in back pain symptoms—is confirmed, the next important step would be to clarify the molecular mechanisms underlying vaspin’s effects, particularly in combination with other factors involved in the healing process of patients with LBP. Therefore, in this study, we attempted to determine whether, in addition to vaspin, the levels of several other inflammatory factors respond to physiotherapy treatment, and whether these changes depend on obesity and correlate with the vaspin levels. The cytokines were selected based on the previous scientific reports demonstrating associations of disc degeneration and/or LBP with the significant changes in the concentrations of the inflammatory factors following treatment (Gruber et al., 2013; Gruber et al., 2014; Wang et al., 2016; Weber et al., 2015). We were, in particular interested in testing the hypothesis that the levels of interleukin (IL)-4 and IL-10—cytokines, associated with healthy adipose tissue (Michailidou et al., 2022)—versus IL-2, IL-17A, and RANTES (regulated on activation, normal T-cell expressed and secreted) linked to the transformation of healthy adipose tissue into inflamed, insulin-resistant tissue (Harford et al., 2011; Schmidt et al., 2022)—change in response to traction therapy.
Material and Methods
The study design
The study design with the available sample sizes and implemented methods of analysis is presented in Figure 1. The data collection was carried out between August 2020 and May 2022. The participants were provided with appropriate study information prior to enrolment and gave written informed consent before the start of the intervention. The study was designed as a prospective clinical trial with two experimental groups and adhered to the standards laid down in the Declaration of Helsinki. The study research protocol was approved by the Ethics Committee at the Poznan University of Medical Sciences in Poland (ref. 958/19) and was registered in the ClinicalTrials.gov database (NCT04507074).
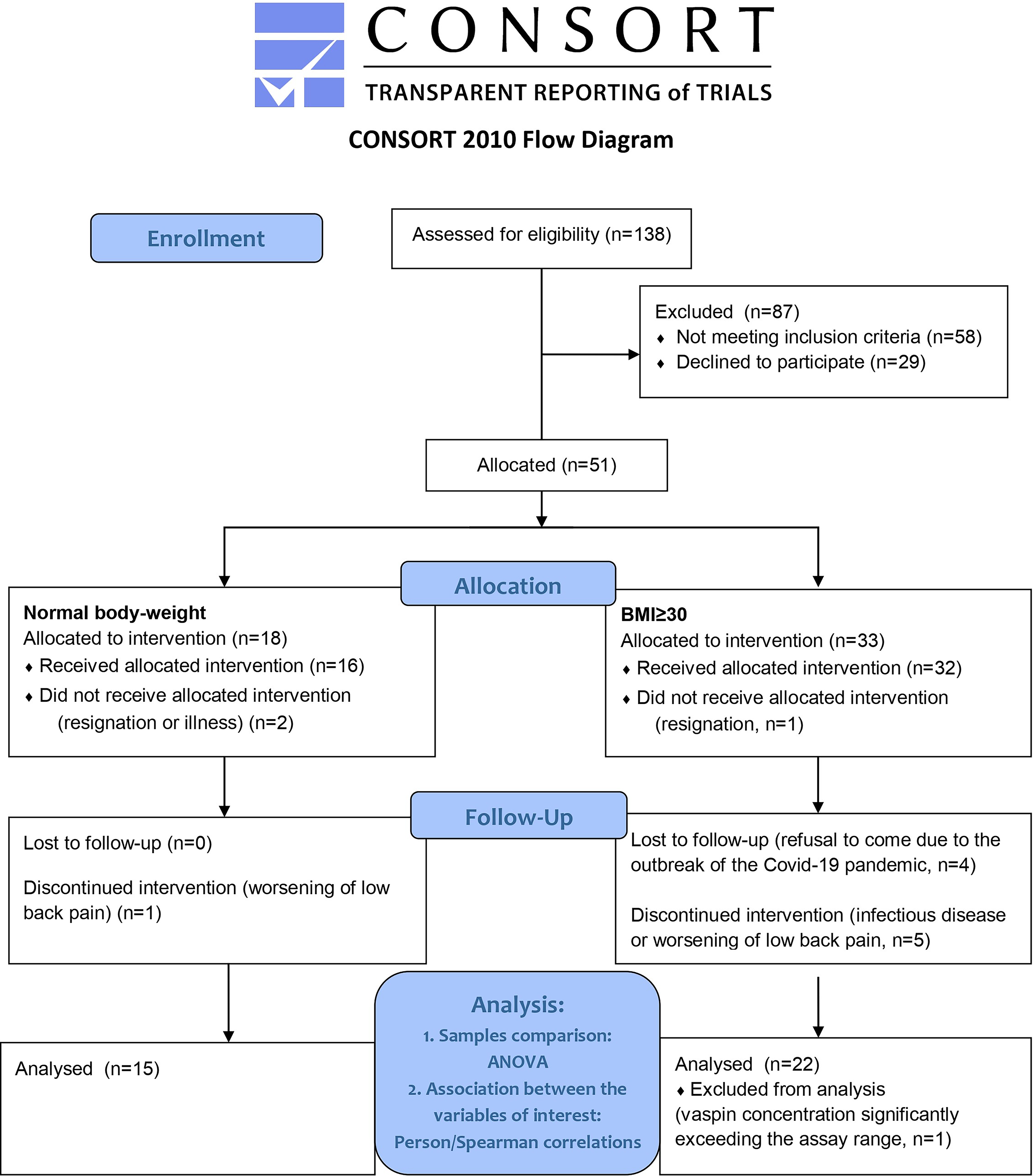
Flow diagram.
Women with chronic LBP were divided into two groups based on body mass index: those with normal BMI and those with obesity. Both groups completed a total of 20 lumbar traction therapy sessions. Apart from the intervention, participants were advised to continue their usual levels of physical activity and dietary habits, which were verified using food diaries and body composition analysis by DXA. Subjective assessments of pain and disability were conducted at baseline and after completion of the 20 therapy sessions, and blood samples were collected at both time points for laboratory analysis. In the same cohort of patients, a study investigating additional biomarkers was also performed; therefore, the description of the participants and the methods used in the present study partially overlap with those reported in a previously published article (Ratajczak et al., 2023b).
Patients
Participants were recruited via social media platforms. Following an initial telephone screening, individuals without contraindications were invited for a preliminary medical assessment at the Department of Obesity Treatment, Metabolic Disorders and Clinical Dietetics of Poznan University of Medical Sciences. Enrollment was based on a comprehensive medical history, physical examination, and any available additional test results. All individuals who completed the initial evaluation were subsequently referred for magnetic resonance imaging, as well as assessments of bone density and body composition. Patients were enrolled in the clinical trial only after confirming the absence of any additional contraindications to traction therapy.
The study included women aged 34–50 years with chronic LBP persisting for at least 6 months, a stable body weight within ± 2 kg over the previous month, and a BMI of 18.5–24.9 for the normal-weight group or ≥ 30 for the obesity group.
The exclusion criteria included menopause or pregnancy, secondary obesity, the presence of pain in another body region that was more severe than the LBP, and any conditions or medications that could influence the balance of pro- and anti-inflammatory factors, such as inflammatory disorders, rheumatoid arthritis, ankylosing spondylitis, or acute infections, as well as other factors described in detail in the previous publication (Ratajczak et al., 2023b). The patients were informed and reminded of the requirement to refrain from taking anti-inflammatory and analgesic medications for at least 48 h before blood collection and throughout the intervention period. Five patients were taking levothyroxine, and one was taking metformin, telmisartan, metoprolol, and ramipril during the intervention.
Intervention
The patients underwent traction therapy, which involved the application of traction forces to stretch the spine. The traction table (Therapy Traction Couches and Packages, ST6567P, SEERSMEDICAL, UK) complied with the requirements of the European Union Directive 93/42/EEC. Traction was administered for 30 min per session, five times per week over a 4-week period, totaling 20 treatment sessions. A continuous traction protocol was applied, beginning at 25% of the patient’s body weight for the first five sessions and progressively increased to 30% thereafter.
Measurements
Magnetic resonance imaging
Magnetic resonance imaging was performed to evaluate the extent of structural changes in the intervertebral discs and surrounding anatomical tissues, using a 1.5 T scanner with a standard three-plane protocol. All images were reviewed by the same experienced radiologist. The imaging was performed prior to the intervention. Several variables were selected for our analysis and are presented as quantitative estimates (scores).
Spinal stenosis
Spinal stenosis was assessed on a scale from 0 to 3: 0—no stenosis, 1—mild stenosis, 2—significant stenosis without compression, and 3—stenosis with compression.
The total score represents the sum for all five lumbar vertebrae.
Facet joint osteoarthritis (FJOA)
Each lumbar facet joint was graded on a scale from 0 to 3: 0—no FJOA, 1—mild FJOA, 2—extensive FJOA with joint space narrowing, and 3—severe FJOA with marked joint space narrowing. The total score reflects the sum for all ten lumbar facet joints.
Modic changes
Modic changes were rated on a scale from 0 to 3 for each vertebral body, where 0 is a normal vertebral body, and type I to III describe type of Modic change according to Dudli et al. (2016). The total score represents the sum of the five lumbar vertebrae.
Intervertebral foramen stenosis
Intervertebral foramen stenosis was graded on a scale from 0 to 3: 0—no stenosis, 1—mild stenosis, 2—significant stenosis without nerve root compression, and 3—stenosis with nerve root compression. The total score is the sum of all ten lumbar intervertebral foramina.
Osteophytosis
Each lumbar vertebra was evaluated for osteophyte formation using a scale from 0 to 4: 0—no osteophytes, 1—sharpening of the vertebral body edges, 2—small osteophytes, and 3—large osteophytes, 4—bridging osteophytes. The total score represents the sum of the five lumbar vertebrae.
Dual energy X-ray absorptiometry
Body composition was analyzed using dual-energy X-ray absorptiometry (DXA, Lunar Prodigy device, GE Healthcare, USA). Body weight and height were measured using a medical scale with a stadiometer (Seca 285, Germany) to the nearest 0.1 kg and 0.5 cm, respectively. The BMI was calculated based on weight and height using the standard formula.
All primary and secondary outcomes measurements listed below were made at two appointmnt).
Assessment of the primary outcomes
LBP-related functionality
Participants’ functionality was assessed using the Oswestry Disability Index (ODI) and the Roland–Morris Disability Questionnaire (RMDQ). Both questionnaires measure a patient’s functional disability due to lower back pain, focusing on how it affects physical functioning in daily activities.
The ODI consists of 10 sections, each addressing a different aspect of daily life. The RMDQ is a self-reported tool comprising 24 yes/no items, each describing a limitation in normal activities caused by back pain (e.g., difficulty walking, dressing, or sleeping). Patients check the statements that apply to them on the day of assessment. Each positive response scores 1 point, resulting in a total score range of 0–24, with higher scores indicating greater disability.
These questionnaires were used in the study to monitor changes in disability in response to treatment. Due to their widespread use in clinical practice, the results can be compared with findings from other studies. Both questionnaires are reliable and valid tools for assessing disability and functional status in Polish-speaking patients with LBP (Miekisiak et al., 2013; Opara et al., 2006).
Visual analogue scale
The Visual Analogue Scale (VAS) is a simple, widely used tool for measuring a person’s perceived level of pain. It consists of a 10 cm line on which patients mark a point that best represents their level of pain, ranging from 0 (no pain) to 10 (worst imaginable pain).
The score was measured in millimeters and used in two categories: the maximum LBP experienced in the previous week and the current maximum LBP. Scale was used at the beginning and after therapy. The VAS score has previously been applied to patients with LBP receiving traction therapy and has been shown to be a reliable measure of pain intensity (Shafshak and Elnemr, 2021).
Assessment of the secondary outcomes
Biochemical analysis
The patients were instructed to refrain from taking anti-inflammatory drugs for at least 48 h before the blood sampling. Blood serum samples were collected from the patients twice: before the intervention and 3 days after the last therapeutic session, following an overnight 12-hour fast, and were processed within 4 h of collection. Serum was separated by centrifugation and stored at −80°C until analysis. All samples underwent no more than one freeze–thaw cycle prior to biomarker determination. Serum concentrations of all cytokines investigated were measured using enzyme-linked immunosorbent assays (ELISAs). Detailed information regarding the assays is provided in Table 1. ELISA measurements were performed according to the manufacturers’ protocols. To minimize potential batch effects and ensure identical conditions, all samples were analyzed on the same assay plate on the same day. Calibration standards provided by the manufacturers were included on each plate.
Characteristics of Enzyme-Linked Immunosorbent Assays Used in the Study
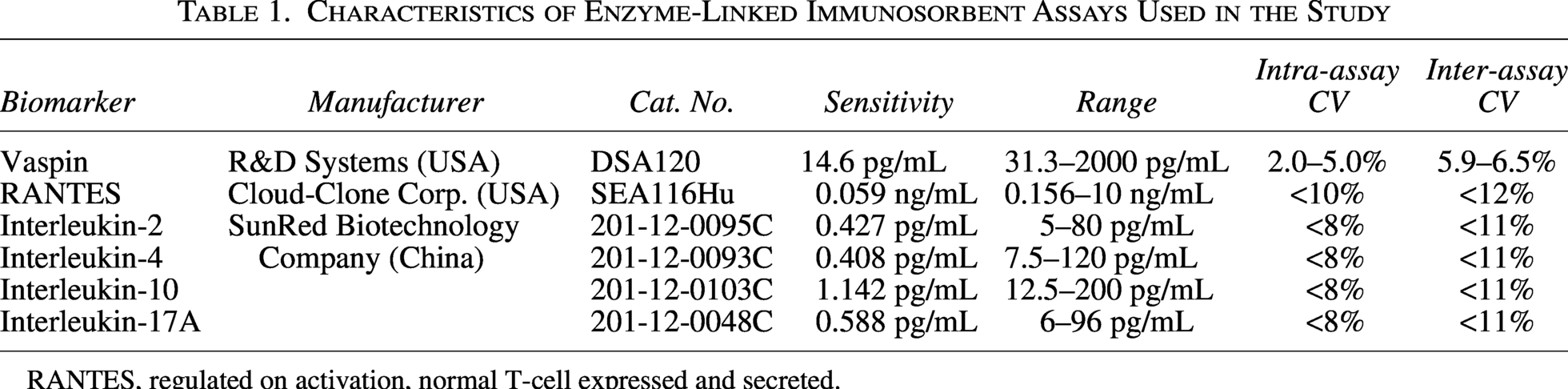
RANTES, regulated on activation, normal T-cell expressed and secreted.
Statistical analysis
Following the aims and the study design (Fig. 1), we conducted the following series of analyses: First, distributions of all the quantitative variables were examined to exclude possible outliers, if any. Then, the Shapiro–Wilk test was used to check the normality of the quantitative variables distribution. For the variables significantly deviating the normality, the baseline clinical characteristics were compared between the groups using the Mann–Whitney U test or the unpaired t-test—otherwise. Chi-squared test was implemented if the data were qualitative.
To meet the main aim of the study and to examine whether the traction therapy (intervention), the BMI difference between the groups, and the interaction between these two main effects affect the levels of the primary and/or secondary outcome variables, a series of two-way repeated measures analysis of variance (RM ANOVA) was implemented. Bonferroni correction for multiple testing was implemented to assess the significance of differences between the pairs of measurements. Data are presented as means and standard deviations (SD).
We also assumed that the changes (if any) in the primary and secondary outcomes detected in the above analyses are not independent. We tested this assumption using the correlation analysis between the vaspin circulating levels and primary outcomes as well as all biochemical markers. Only statistically significant correlations have been presented. Depending on the type of variables, non-parametric Spearman rank-correlation test, or the Pearson correlation test, if the data were normally distributed, was implemented. All the computations and analyses were performed using TIBCO Statistica 13.3 software.
Prior to conducting the above analyses, we used a sample size calculator (G*Power 3.1) to determine the minimum sample size required for ANOVA to detect a therapy effect in reducing maximal pain. The analysis indicated that a minimum of 6 participants was needed to achieve at least 80% power to detect a statistically significant effect at the α = 0.05 level. The sample size for evaluating the effect of the intervention on maximal pain was based on data from a pilot study involving patients with chronic LBP (8 with obesity, 13 without) who underwent the same therapy. We present eta-squared (ƞ2) as a measure of effect size in the results tables.
Results
Before traction therapy, the two groups of patients were compared (Table 2). The main difference between patients with normal BMI and elevated BMI (obesity) was the total fat content, which was highly significant (P < 0.000). Women with normal BMI and women with obesity had similar age, LBP duration, intensity of LBP, level of disability, and similar features in magnetic resonance imaging. The prevalence of IVD herniation was, however, significantly (P < 0.02) higher in the normal BMI group (86.7% vs 45%).
Demographic and Clinical Characteristics of Patients
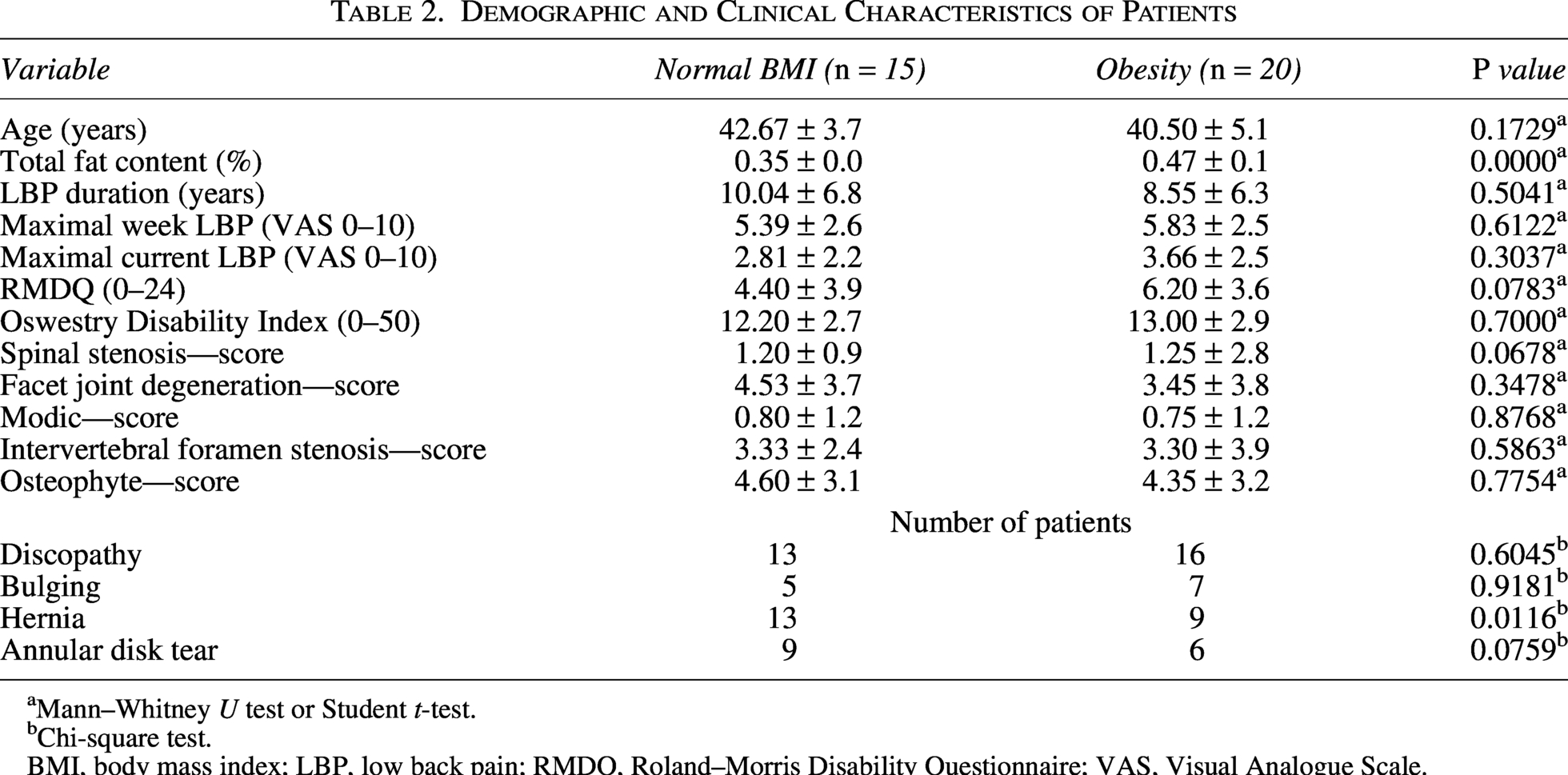
Mann–Whitney U test or Student t-test.
Chi-square test.
BMI, body mass index; LBP, low back pain; RMDQ, Roland–Morris Disability Questionnaire; VAS, Visual Analogue Scale.
Table 3 summarizes the results of the two-way RM ANOVA and indicates that after completion of traction therapy, there was a statistically significant (P < 0.001) improvement in all primary outcomes examined. All tests survived Bonferroni correction, and the adjusted P values remained < 0.001. The degree of disability and pain intensity decreased in both groups, and maximal week LBP and maximal current LBP clearly decreased consistently in both BMI groups. However, BMI differences did not influence the effect of the traction therapy on the primary outcomes. Both the main BMI effect and the interaction terms were statistically not significant (P > 0.05) in all cases.
Pre- and Post-Intervention Primary Outcomes in Women with Normal BMI and Obesity Subjected to Lumbar Traction Therapy
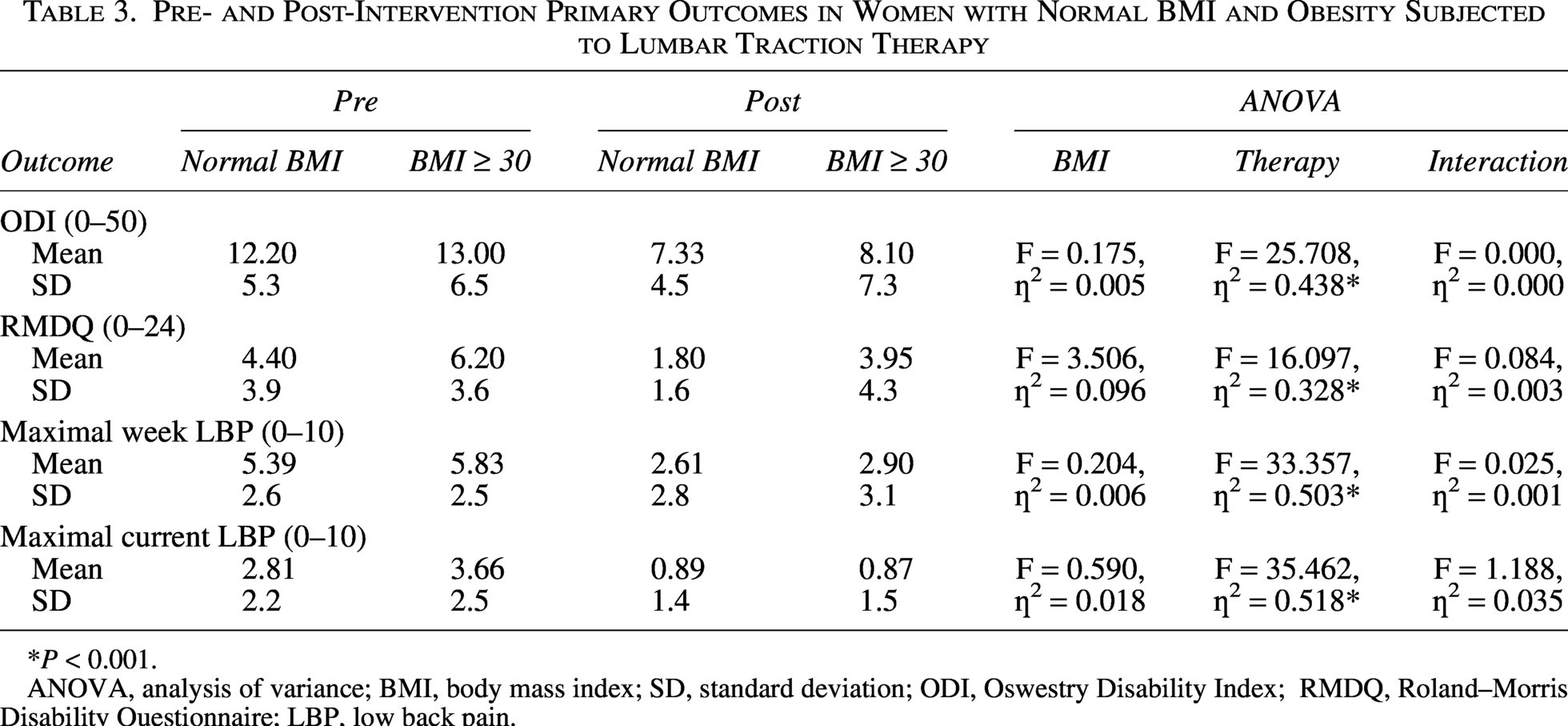
P < 0.001.
ANOVA, analysis of variance; BMI, body mass index; SD, standard deviation; ODI, Oswestry Disability Index; RMDQ, Roland–Morris Disability Questionnaire; LBP, low back pain.
When the effect of the treatment on the secondary outcomes was tested, the circulating levels of vaspin and IL-10 increased significantly (Table 4).
Pre- and Post-Intervention Secondary Outcomes in Women with Normal BMI and Obesity Subjected to Lumbar Traction Therapy
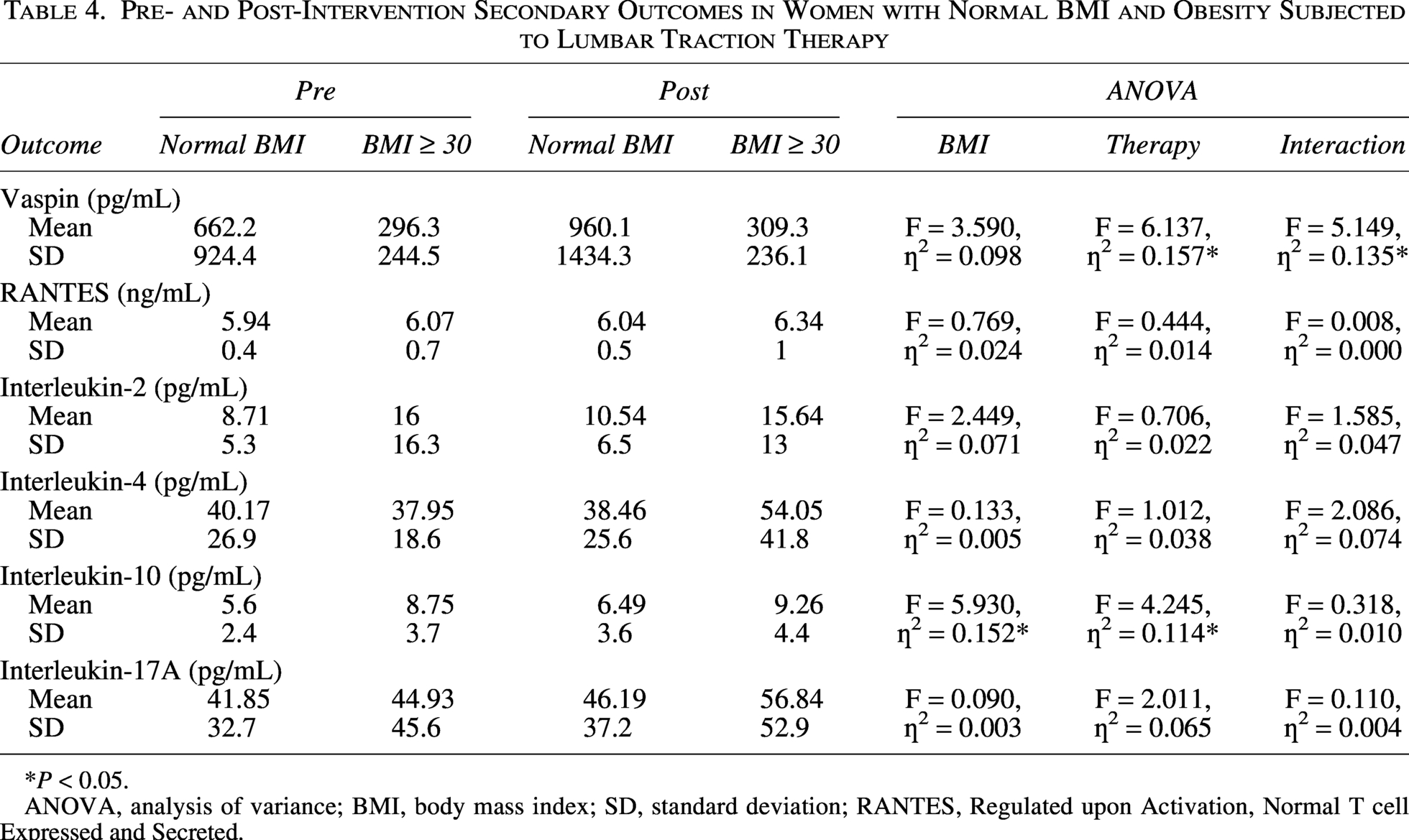
*P < 0.05.
ANOVA, analysis of variance; BMI, body mass index; SD, standard deviation; RANTES, Regulated upon Activation, Normal T cell Expressed and Secreted.
However, vaspin concentration increased statistically significantly only in women with normal BMI, which was confirmed by a significant interaction term, and remained significant after Bonferroni correction (P = 0.018). The IL-10 levels tended to increase after therapy relatively equally in both BMI groups, i.e., both main effects displayed nominally statistically significant terms (P < 0.05), while the interaction term was not significant (P > 0.05). It is worth mentioning that IL-17A also showed a consistent trend to increase, but did not reach a statistically significant level. Individual changes in vaspin and IL-10 concentrations are presented in Figure 2.
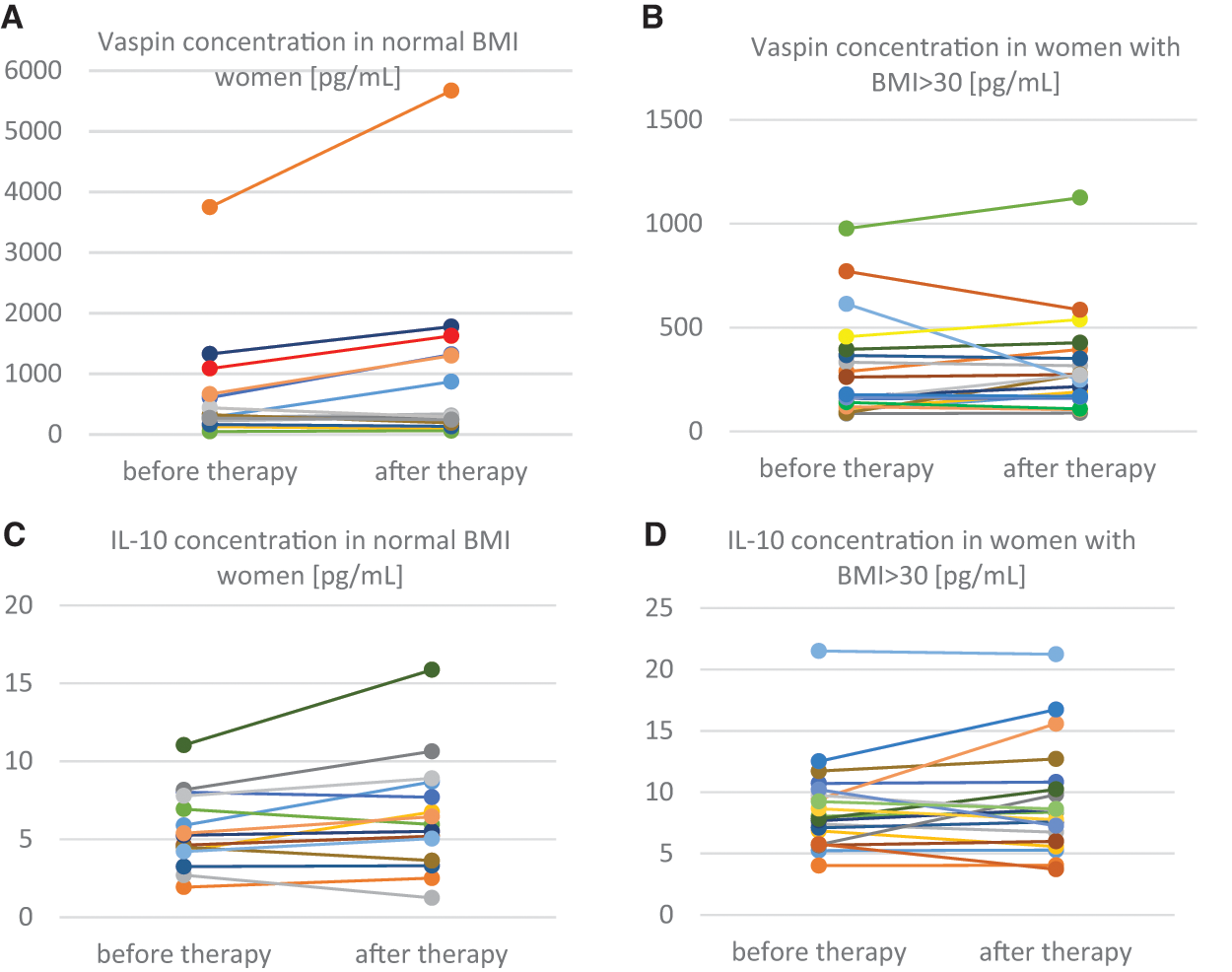
Individual changes in vaspin
Moreover, while the levels of vaspin tended to be lower in the BMI > 30 group, all other cytokines showed the opposite trend, as expected. The cytokine-specific differences, however, were not statistically significant, probably due to insufficient sample size. Yet, implementing the Fisher combined probability test (Zhang and Wu, 2023) yields P < 0.005, suggesting that the observed consistent trend is statistically significant.
At the next stage of the study, we were interested in whether there is an association between the improvement in primary outcomes and changes in circulating vaspin levels. Since the latter showed a significant increase in the normal BMI group, we analyzed the associations between vaspin and all four primary outcomes in this group only. Only the ODI showed a significant negative Spearman’s correlation with vaspin (rs = −0.54, P = 0.036) and only after therapy. This correlation, however, became not significant after Bonferroni correction.
Following our additional aim, we examined whether the changes in vaspin levels correlate with other selected inflammatory factors. Remarkably, although the levels of IL-4 and IL-17A did not change significantly after therapy, their concentrations correlated significantly with the levels of vaspin after therapy. Figure 3A shows significant positive correlations between vaspin concentrations and both cytokines in the normal weight group. The opposite trend was observed in women with obesity, where vaspin correlated negatively with concentrations of both cytokines (Fig. 3B). RANTES, IL-10, and IL-2 concentrations did not correlate with vaspin either before or after therapy (Supplemental Data).
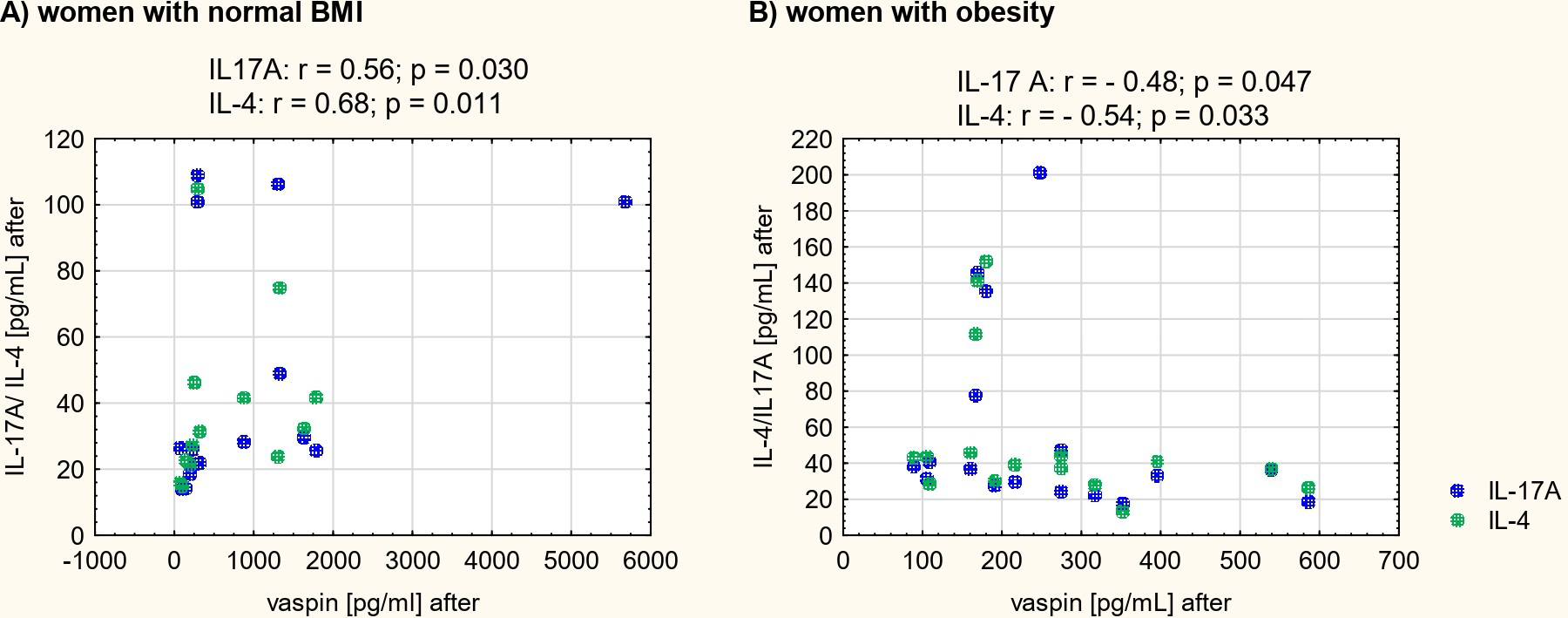
Spearman’s correlation coefficients (r) and P values for significant correlations observed between interleukins 4 and 17A and vaspin concentrations in women with normal BMI
Discussion
Identifying circulating blood-soluble molecules that can be used to monitor the effects of LBP therapy is of considerable importance but remains challenging, particularly when candidate biomarkers are involved in inflammatory and metabolic processes such as obesity. Accordingly, our study deliberately included patients with both normal BMI and obesity to assess whether changes in pain intensity (VAS), LBP-related functional outcomes, and biomarker profiles were associated with physiotherapy and influenced by adiposity. To address this objective, we measured serum vaspin levels and selected inflammation-related cytokines before and after lumbar traction therapy.
Statistically significant improvements were observed in both maximum and current VAS scores, as well as in functional measures. To date, very few reliable studies—with a control group, a clearly described intervention, and follow-up assessments—have examined reductions in these outcomes among patients with LBP. Nevertheless, a recent controlled study supports the effectiveness of traction therapy in reducing VAS and ODI scores, with benefits maintained at 6-month follow-up (Liu et al., 2021). Traction-related changes in RMDQ scores have also been reported, demonstrating significant improvement after four weeks of therapy; however, the absence of a control group limits the strength of those conclusions (Beattie et al., 2008). With respect to differential responsiveness to traction therapy in patients with obesity versus normal BMI, our recent study found no significant between-group differences in treatment effects (Ratajczak et al., 2025).
Chronic LBP is increasingly recognized as not only a musculoskeletal condition but also an inflammatory disorder, in which low-grade, persistent inflammation contributes to pain maintenance and impaired recovery (Farley et al., 2024). This inflammatory milieu is often amplified in obesity, where adipose tissue acts as an active endocrine organ, producing pro-inflammatory cytokines and adipokines that can exacerbate systemic and local inflammatory responses (Kawai et al., 2021). In this context, vaspin, an adipose-derived serine protease inhibitor, has been proposed as a modulator of inflammatory balance (Radzik-Zając et al., 2023; Ren et al., 2022), while IL-10 serves as a potent anti-inflammatory cytokine that can counteract tissue damage and pain sensitization (Canlı et al., 2022; Pinto et al., 2023). In the present study, a statistically significant increase in IL-10 concentration from pre- to post-therapy was observed in both obese and non-obese women, suggesting that the applied therapeutic regimen effectively enhanced anti-inflammatory signaling regardless of adiposity. In another study, IL-10 has been shown to strongly correlate with a reduction in LBP in patients undergoing epidural steroid injections, but its concentrations did not change following the injections (Weber et al., 2015). In contrast, among non-pharmacologic therapies, neuro-emotional techniques have been shown to decrease IL-10 concentrations, while balneotherapy has been found to increase them (Puerto Valencia et al., 2024). Our study, therefore, contributes to the limited body of research on the effects of various LBP therapies on changes in IL-10 levels.
In recent years, several adipokines have been studied in the context of their association with the occurrence of LBP, its duration and severity, disability, and the degree of spinal degeneration. In a previous study, we observed that the concentrations or changes in concentrations of leptin and adipsin correlated with the severity of morning LBP in women with normal body weight undergoing traction therapy (Ratajczak et al., 2023b). More recently, special attention has been given to vaspin because its concentrations have been associated with disability, the duration of LBP, and its severity (Tarabeih et al., 2020), and additionally with a common cause of LBP—the degree of facet joint osteoarthritis (Tarabeih et al., 2022). It was suggested that circulating concentrations of vaspin could serve as a biomarker for LBP severity and associated complications (Tarabeih et al., 2020). In our study, vaspin concentrations were found to increase only in the group of women with normal BMI. In women with obesity, vaspin levels tended to remain low, despite consistently elevated levels of other studied cytokines.
It is intriguing to understand what caused this divergent response between the groups and whether the increase in vaspin could be a factor that provides an advantage and a better prognosis for patients with normal BMI. Vaspin is secreted by both muscle and adipose tissue (Nicholson et al., 2019). Although higher mRNA expression is typically observed in tissues of obese individuals compared to lean individuals, serum vaspin concentrations have been reported not to differ between lean and obese subjects. However, a significant positive correlation of serum vaspin levels with BMI was observed in females (Nicholson et al., 2019). Furthermore, in obese mice fed a high-sucrose, high-fat diet, recombinant vaspin administration reduced the expression of tumor necrosis factor-α (TNF-α) (Hida et al., 2005), a key cytokine promoting the development of a Th1-type pro-inflammatory pathway (Pesce et al., 2022). According to Pilarski et al. (Pilarski et al., 2023), elevated vaspin levels may indicate its compensatory role against metabolic disorders in patients with obesity. In Figure 2A, we noticed that the higher the baseline vaspin level, the steeper the slope. In other words, the degree of increase in vaspin levels in non-obese individuals appears to depend on baseline levels. Given these findings, we ask: Was the vaspin increase in normal BMI women a favorable response? Could the opposing vaspin trends reflect pro-inflammatory dominance in obesity and regulatory immune responses in normal BMI? While further research is needed, our correlation analyses suggest a positive answer. In our study, vaspin levels were negatively correlated with disability (ODI), but only in women with normal BMI—higher vaspin was linked to lower ODI after 20 therapy sessions. This seems to contradict the study by (Tarabeih et al., 2020), who found a positive correlation between vaspin and disability using the RMDQ. However, it should be noted that in the aforementioned study, the sample included both lean individuals and those with abnormally high BMI. Nevertheless, the authors reached the same conclusions, suggesting that elevated vaspin plays a protective role in LBP.
The cytokine analyses further illuminate the complexity of vaspin’s role. Post-therapy, vaspin correlated with IL-4 and IL-17A, but in opposite directions by BMI group: in women with obesity, lower vaspin levels were linked to higher IL-4 and IL-17A. Typically, for people with obesity, the inflammatory response seemed to be exacerbated (Longo et al., 2019; Tanimura et al., 2016). Despite the high adipose tissue content in the BMI > 30 group, vaspin concentrations did not increase. On the contrary, in women with normal BMI, vaspin concentration correlated positively with the concentrations of IL-4 and IL-17A. We have previously shown that high levels of IL-4 can serve as a predictor of beneficial traction therapy effects, including reduced pain and improved spinal erector activity. Moreover, the greater the increase in IL-17A serum concentration in patients, the better the spinal erector activity pattern they achieved (Ratajczak et al., 2023a). Although IL-17A is sometimes described as pro-inflammatory (McGeachy et al., 2019), it may be helpful during the healing process, as was already suggested (Tian et al., 2015).
Even if vaspin secretion is somehow associated with IL-4 and IL-17A secretion, it remains unclear which of these proteins promotes the secretion of the other. Some studies suggest that decreased vaspin levels may trigger pro-inflammatory cytokines (e.g., TNF-α, IL-1β, IL-6, IL-8), while IL-17 combined with TNF-α can suppress vaspin expression (Saalbach et al., 2016). In our BMI > 30 group, elevated IL-17A levels post-therapy may explain the stable vaspin levels. IL-17A itself can be induced by cytokines like IL-6 (Polak-Szczybyło and Tabarkiewicz, 2022) or adipokines such as leptin (Orlova and Shirshev, 2014) in inflamed adipose tissue, suggesting mutual regulation of the related proteins. It is also possible that vaspin’s relationship with IL-17 and IL-4 resembles its relationship with IL-6. This association can be negative, as seen in women with a BMI over 40, where vaspin appears to reduce inflammation (Auguet et al., 2011) or positive, where vaspin production increases as a compensatory response to inflammation (Yin et al., 2019).
Regarding the cytokines analyzed in this study—IL-2, IL-4, IL-10, IL-17A, and RANTES—their concentrations did not differentiate the therapeutic response between women with a normal BMI and those with a BMI over 30. To conclude, a positive association between vaspin and IL-4 and IL-17 in non-obesity women suggests that vaspin may act not as a selective inhibitor or promoter of inflammation, but rather as a broader modulator of immune tone. Such dual associations could reflect an adaptive balancing act, in which vaspin interacts with multiple arms of the immune response to maintain homeostasis during the resolution phase of inflammation. In obese women, by contrast, negative correlations of vaspin with IL-4 and IL-17A after therapy could indicate a fundamentally different mode of regulation in the obese state, potentially reflecting a feedback mechanism aimed at dampening immune activation. However, the absence of a vaspin rise in these women suggests that the feedback loop is either ineffective or overridden by chronic metabolic-inflammatory crosstalk. Adipose tissue inflammation (Kalinkovich and Livshits, 2017; Kawai et al., 2021) changes in circulating immune cell profiles in obesity (Rohm et al., 2022), and altered vaspin receptor expression (Tindall et al., 2024) may all contribute to this blunted or even dysfunctional regulatory relationship. More research is certainly needed to determine whether the relationship between these markers is causal or simply reflects the underlying obesity-inflammatory context.
It is also noteworthy that IL-10 levels and their changes were not correlated with circulating vaspin. Given the known pro-inflammatory pressure of obesity (Soták et al., 2025), it is plausible to suggest that obesity-related metabolic stress might alter vaspin expression or activity as part of a compensatory response to inflammation, potentially influencing immune cell behavior and cytokine production. Yet, in the current findings, this compensatory link, if present, did not translate into measurable associations with IL-10 levels. This dissociation suggests that IL-10 and vaspin operate through independent, possibly complementary, mechanisms in modulating inflammation. The absence of a vaspin–IL-10 link under therapeutic conditions implies that vaspin’s role may be more strongly shaped by obesity-related metabolic stress, whereas IL-10 can be directly enhanced by anti-inflammatory therapy regardless of adiposity. Together, these findings suggest that the interplay between adipokine regulation and inflammatory cytokine profiles in LBP is influenced by obesity status.
Monitoring the effects of therapy in the general population using vaspin remains challenging, as its concentration varies across disease states and is partly genetically determined (Tarabeih et al., 2020). Nevertheless, in individuals with a normal BMI suffering solely from LBP, the changes in vaspin concentrations should be confirmed in studies incorporating a control group with LBP and normal BMI that does not receive therapy or undergo sham traction. To establish causality, focusing on repeated measurements of biomarker concentrations to determine how long biochemical changes persist in the blood after the completion of therapy is also warranted. In addition to the lack of a control group not undergoing therapy and the absence of follow-up measurements, our study has other limitations. The sample size is relatively small, and pain intensity and degree of disability were assessed using validated, yet inherently subjective tools. Furthermore, we did not measure established markers of low-grade inflammation, such as C-reactive protein, which would have enabled the exclusion of patients with an ongoing acute inflammatory condition. Future studies in cell cultures derived from individuals with different BMI values and suffering from LBP, involving either measurement of vaspin levels or its use as a stimulus, may help elucidate the mechanisms of vaspin action.
Conclusions
Although women in our study, regardless of BMI, achieved similar post-therapeutic reductions in pain and disability, the data suggest that the enhanced inflammation associated with obesity may substantially modify the blood biochemical profile during traction therapy and potentially contribute to faster symptom recurrence, an issue warranting further investigation. Adipose tissue inflammation is likely to influence not only traction therapy outcomes but also the effectiveness of other treatment modalities for LBP. At present, monitoring therapy effects in the general population using vaspin is not feasible. Nevertheless, changes in vaspin levels observed only among women with normal BMI suggest a BMI-dependent association between circulating vaspin concentrations and response to therapy.
Authors’ Contributions
M.R.: Conceptualization, data curation, formal analysis, funding acquisition, investigation, methodology, project administration, supervision, writing—original draft. A.K.: Writing—original draft, formal analysis, validation. G.L.: Supervision, formal analysis, methodology, writing—review & editing.
Consent to Participate
All subjects provided written informed consent before participation.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Footnotes
Acknowledgments
The authors thank physiotherapist Michał Wendt for performing the lumbar traction sessions.
Funding Information
This work was supported by the National Science Centre, Poland (grant numbers 2020/04/X/NZ7/00021).
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.