
Abstract
Introduction
In the United States, more than 11.5 million people participate in hunting. Deer hunters commonly use tree stands as tall as 8 m. Falls from tree stands can cause injury and even death. Previous studies have investigated the types of injuries sustained from tree stand falls, but few have investigated patient outcomes. This study investigated patient outcomes related to tree stand falls and analyzed injury types resulting from tree stand falls, and this paper discusses factors that may lead to tree stand falls.
Methods
This study used a retrospective chart review of patients at the same institution between January 1, 2012, and August 31, 2022. Patient information, injury type, fall height, and interventions were collected.
Results
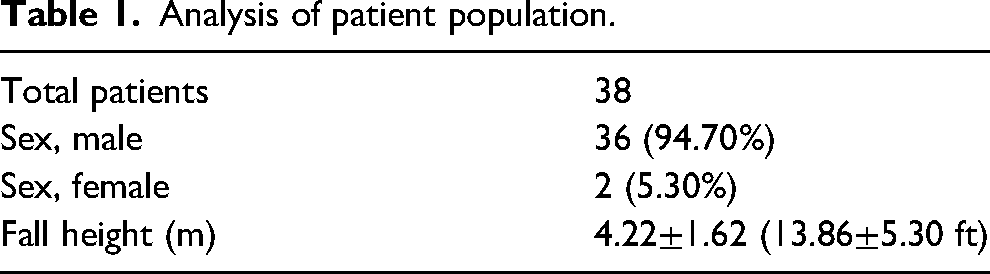
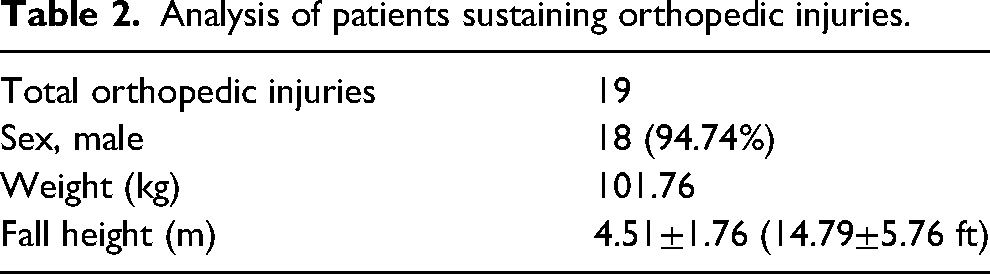
A total of 38 patients were included in the study, 36 males (94.70%) and 2 females (5.30%). The average fall height from a tree stand was 4.22±1.62 m (13.86±5.30 ft). Of the 38 patients, 19 had sustained orthopedic injuries to their upper extremity, lower extremity, spine/pelvis, or multiple areas; the average fall height of this subgroup was 4.51±1.76 m (14.79±5.76 ft). Nonoperative management was the highest used intervention because 12 patients did not require surgery. Orthopedic surgery was used to treat 6 patients, and 1 patient had nonorthopedic surgery.
Conclusions
Although tree stand falls are rare, the injuries they cause can be fatal. Injury severity and outcome are determined by a multitude of factors. This study highlights the significance of these injuries and the importance of practicing safe guidelines while hunting.
Introduction
In 2016, ∼11.5 million people in the United States reported participating in hunting activities. 1 More than 70% of hunters participate in deer hunting, and deer hunters commonly use tree stands to improve their field of vision and increase their odds of a successful hunt.2,3 With the height of a tree stand ranging from 1 m to >8 m (3.28–26.25 ft), falls from these structures can lead to serious injury or even death.2–4
Prior literature has shown that these patients sustain a wide range of injuries on all parts of the body and are often delayed in arriving at an emergency department, leading to ICU admissions, multiple operative interventions, and overall functional impairment.2–4 Orthopedic injuries encompass the majority of these injuries, with most patients sustaining multiple fractures in a given incident.2–4 Prior orthopedic literature has focused on the epidemiology and distribution of injury type, especially focusing on spinal injuries. There is a sparsity of literature dedicated to discussing management options for orthopedic injuries, including extremity injuries, in this population. Shoulder and upper extremity injuries account for roughly 21% of the injuries reported, highlighting the need for further exploration of whether these patients often require surgery due to their injuries. 4
This study aimed to better understand injury patterns and the need for operative intervention in patients sustaining orthopedic tree stand injuries. First, this patient population, given their chosen recreational activity, has marked treatment outcome goals for return to sport, which would affect operative planning. Second, given that permitted areas for hunting are primarily in remote locations, these patients often have delays in care, complicating their initial evaluation, and further research is required to understand the acuity of these injuries. Furthermore, this study highlights the need for proper management of orthopedic trauma cases in remote areas while seeking to raise awareness to promote tree stand safety.
Methods
Institutional review board approval was obtained prior to initiation of this study. Patients eligible for this study were identified through a retrospective review of electronic health records (EHRs) for individuals who sustained a tree stand injury from falling between January 1, 2012, and August 31, 2022, at a single institution. Patients met the inclusion criteria if they were adults (≥18 y old) who sustained a tree stand injury. All patients under the age of 18 y in our study cohort were excluded; no additional exclusion criteria were applied.
Data Collection
All data were compiled and reviewed by the investigators via accessing the patient's EHR with their medical record number. Data extracted from the patient's chart included demographics, weight, fall height, injury location, and drug screen results. Patients were assessed for operative vs nonoperative management, the type of intervention received, length of stay, and discharge disposition.
Results
The review of the EHRs identified 642 patients to be analyzed for meeting the study criteria. Of the 642 patients who presented to the medical facility, a total of 38 met the inclusion criteria as outlined. A total of 36 males accounted for 94.74% of the patient population, and 2 females accounted for the remaining 5.3% (Table 1). The average patient fell from a height of 4.22 m (13.86 ft) with a standard deviation of 1.62 m (5.30 ft). For the 19 patients sustaining orthopedic injuries, 94.74% were male and had an average fall height of 4.51±1.76 m (Table 2).
Analysis of patient population.
Analysis of patients sustaining orthopedic injuries.
Injuries
The EHRs of the 38 patients included in the study were analyzed for an orthopedic injury; these included injuries to the upper extremities, lower extremities, spine, pelvis, and back. The average fall height of someone who sustained an orthopedic injury was 4.51 m (14.80 ft), which is 6.8% higher than the average fall height of all the patients in this study. The average weight of patients sustaining an orthopedic injury was 101.76 kg.
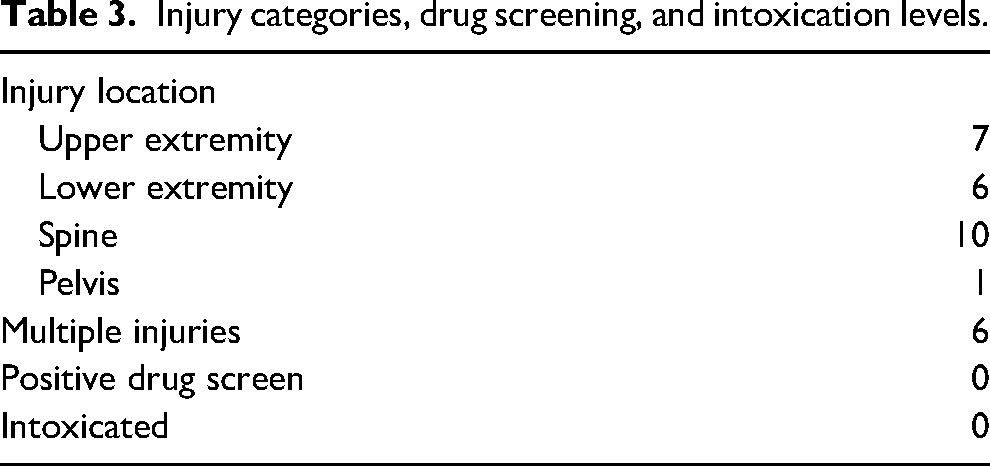
Screening of the patients having sustained an orthopedic injury identified 7 upper extremity injuries, 6 lower extremity injuries, and 11 spinal cord or pelvis injuries (Table 3). The greater number of orthopedic injuries than patients is due to 6 patients having sustained injuries to 2 or more of the categories. Notably, no patients included in this study had positive drug or intoxication screens at the time of treatment.
Injury categories, drug screening, and intoxication levels.
Management of patients with an orthopedic injury.
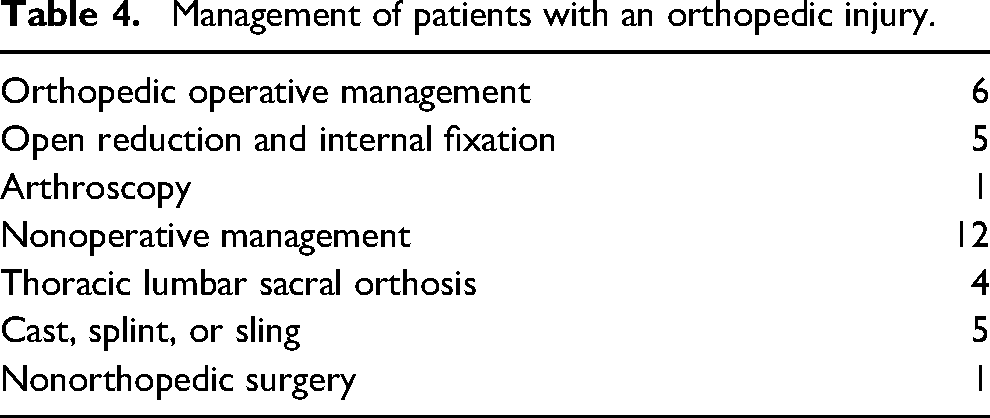
Operative management was used in 6 patients (31.59%); 12 patients (63.16%) were managed through nonoperative measures; and 1 patient (5.25%) underwent nonorthopedic surgery (Table 4).
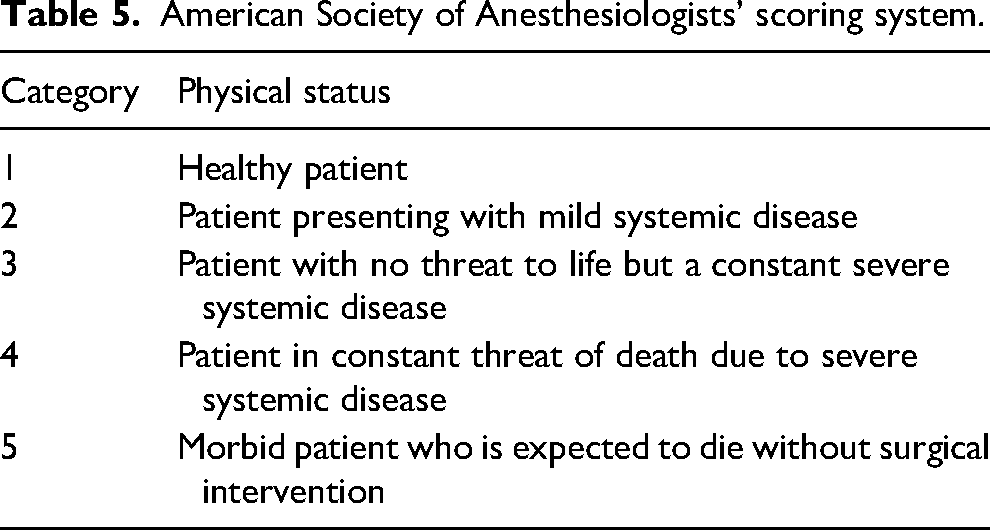
Open reduction and internal fixation was the most prevalent orthopedic surgerical procedure performed on patents because it accounted for 83.33% of the total orthopedic surgeries. A singular arthroscopy was performed, which accounted for 16.67% of orthopedic surgeries. Nonoperative management of the orthopedic injuries was the most used therapy for patients who sustained an orthopedic injury; 63.16% of the total number of patients were treated this way. Instructions were given to 4 patients to wear a thoracic lumbar sacral orthosis brace, and an additional 5 patients were suited with either a cast, splint, or brace. A single patient who underwent neurosurgery as part of therapy for their injury accounted for the 1 nonorthopedic surgery. The average American Society of Anesthesiologists’ scoring system score, which is a subjective assessment of the overall health of a patient, 5 of the patients who underwent both orthopedic and neurosurgery was 2.3. Table 5 shows the 5 different classifications recognized in the American Society of Anesthesiologists’ scoring system.
American Society of Anesthesiologists’ scoring system.
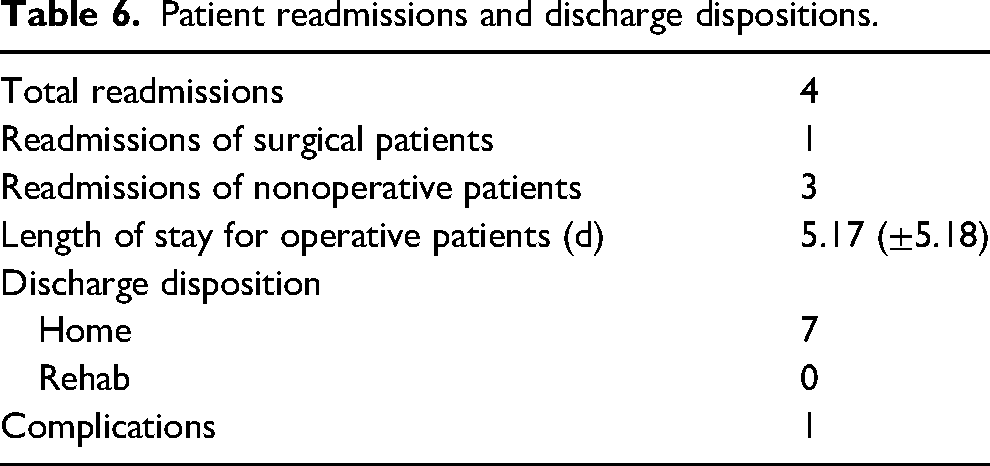
There was a total of 4 patient readmissions to the hospital; only 1 of these patients was managed operatively. The average length of stay for a patient who underwent an operation was 5.17 d with a standard deviation of 5.18 d. Table 6 displays the findings and the discharge dispositions of the patients.
Patient readmissions and discharge dispositions.
Discussion
Falls from tree stands with a vertical deceleration injury pattern remain rare. Because deer hunters account for 70% of all hunters and commonly use tree stands, the use of tree stands raises the likelihood of sustaining an injury from falling compared with not using one.2,3 Injuries to the spine, pelvis, or extremities have been estimated to be as high as 73% among hunters who fall from tree stands. 6 Most of the patients in this study were male and fell from ∼4.57 m (15 ft). These findings align with previous data.2,6,7
Patients were most likely to injure their spine/pelvis, followed by upper extremity, and lastly, lower extremity. Prior literature demonstrates that tree stand falls can cause a wide range of injuries to all parts of the body and that patients are often delayed in arriving at an emergency department due to the remote nature of the injury's geographic location. Importantly, this study is based on a small sample size, and differences in the data between this study and previous literature may be attributable to background variability. Spine injuries occurred in 53% of patients, comparable with previous studies finding thoracic and lumbar spine fractures in up to 52% of patients. 8 In contrast, 68% of our patients had extremity injuries, which is slightly higher than previous estimates of 40 to 47%. 9 Shoulder and upper extremity injuries account for roughly 21% of the injuries reported in our study. These injury patterns are likely related to how the patient fell from the tree stand, how they landed, and if they attempted to catch themselves in the process. Previous research regarding orthopedic injuries sustained by vertical deceleration is more focused on paratrooping or falls from buildings. These studies have found foot injuries to be the most common injury,10,11 suggesting that the mechanism of injury in tree stand is distinct in comparison with these other vertical deceleration patterns of injury.
In this study, 33% of patients required operative management after falling from a tree stand, which is significantly higher than the previously reported percentage of 10% by Smith et al 2 but lower than that reported by Hughes et al, 4 who found that 50% of patients required orthopedic surgeries. This discrepancy is likely multifactorial. First, this study only looked at patients with an orthopedic injury, which could unfairly select for patients who are more likely to need surgery. Among patients with orthopedic injuries, there is an increased prevalence of operative management of certain fractures seen in the patients of this study, including distal radius 12 and clavicle 13 fractures, compared with standard practice performed during previous studies. Alcohol also has been demonstrated to be a significant risk factor for falling from tree stands. Based on the mandatory blood alcohol screen for trauma patients, none of the patients in this study were intoxicated when they were treated. According to Metz et al,14 leading factors causing tree stand injuries include structural failure, alcohol use, and entering/exiting the tree stand. Additionally, up to 66% of hunters who use tree stands use homemade tree stands, and their failure likely underlies several of the injuries in our patient population. 7 Furthermore, the average weight of patients included in this study was 101 kg higher than the average male in the United States (∼90 kg). 15 Previous studies have shown that patients with higher body mass indexes have increased fracture risk, 16 which is supported in this study and is likely exacerbated in a rural population, where patients are more likely to be obese. Ultimately, there are several factors that influence the likelihood of a hunter falling from a tree stand.
All patients were able to go home postoperatively and did not require rehabilitation, suggesting a lower severity of injuries. The average admission for patients requiring operative management was 5.29 d, similar to previous studies finding admission framing from 3 to 6 d. 9 Injuries in younger age groups also make it more favorable for patients to return home postoperatively. Level of height fallen is a good predictor of morbidity and mortality in injuries due to fall. 17 Tree stands are generally 1 m to >8 m high, heights that can even lead to death.2–4 Patients in this study fell from an average of 4.57 m (15 ft); thus significant injury is expected that may be more or less severe than seen in previous studies depending on the height from which the patients fell. Thus, fall height is an important factor to consider in patient prognosis after sustaining a tree stand injury.
Up to one fourth of hunters report falling out of tree stands. 2 Thus, public education is needed to minimize injuries to these patients. Public safety campaigns should include the risk of falling out of tree stands, use of safety harnesses, and safe stand construction. Previous public education campaigns have reduced tree stand injuries. 18 Permitted areas for hunting are typically in remote locations, and these patients often have delays in care, complicating their initial evaluation and necessitating swift decision making in the emergency department and in the operating room. In many cases, injuries that occur in rural areas result in worse patient outcomes, have longer patient rehabilitation times, and are more likely to lead to death than similar injuries that do not occur in rural areas. 19 Tree stand fall injuries are more likely to occur in rural areas, where hunting is more prevalent.
Limitations
There are several notable limitations to this study. Because tree stand fall injuries are rare, we have a small sample size. These injuries are likely underreported due to the rural patient population. The lack of data regarding the different types of tree stands used by the patients, the patients’ level of tree stand safety knowledge, and the causes of the fall are all limitations to this study.
Conclusion
Tree stand injuries remain a rare injury, although they can cause substantial orthopedic injury. The patient outcomes of those who sustain a tree stand fall injury are determined by a multitude of factors. Hunters who use tree stands should be familiar with proper tree stand protocols, safety equipment, and emergency contacts. Public education can provide hunters with the necessary information and help to prevent injuries.
Footnotes
Author Contribution(s)
AL: creation and execution of project; MO: writing of manuscript; RS: review of manuscript; CC: review of manuscript; SA: data collection; AG: data collection; JC: oversight and supervision.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.