
Abstract
Keywords
Objective
To apply experiential learning to teach decision-making bias, fallacies, and heuristics in both the clinical and backcountry settings.
Background
In 2001, behavioral scientist Robin Hogarth theorized the concept of “wicked learning environments” while studying the relationship of feedback and decision-making in the emergency department.1,2 He found that physicians often do not receive adequate feedback on the decisions that they make. When feedback is provided, the feedback is usually short term, variable based on the decision the physician makes, and frequently not present at all. Hogarth goes on to describe this experience of asymmetric, unreliable, and/or inconsistent feedback as a wicked learning environment.
Additionally, the clinical environment is subject to elevated cognitive stress, time constraints, complex and perhaps contradictory decision-making factors, and often incredibly high stakes. This makes the clinical environment highly subject to increased decision-making bias.1-3 Despite the high risk of cognitive bias within the clinical environment, there is very limited teaching on cognitive bias within medical education.3,4 When addressed, medical educators primarily teach decision-making bias in a classroom setting with a lecture format. 4 Our work aimed to illustrate this concept of the clinical environment as a wicked learning environment by employing outdoor experiential techniques in a parallel wicked learning environment, the backcountry. 5 Through the curation of decision-making scenarios in this wicked learning environment, students employed techniques to increase their awareness and combat their own decision-making biases. To date, there is no literature on the design of a cognitive bias teaching session from an experiential learning approach.
Design
We designed a decision-making workshop for first-year medical students with four distinct learning components. Students attended two introductory lectures: the first on decision-making bias, fallacies, and heuristics, and the second on current literature on decision science in backcountry settings (Appendix A). Next, they engaged in an interdisciplinary panel discussion regarding decision-making in both backcountry and clinical settings. For the experiential learning components, students participated in an experiential five-hour backcountry ski tour where content experts facilitated discussion about backcountry and clinical decision-making (Appendix B) and completed longitudinal reflections throughout the workshop experience. During this time, students discussed decision-making biases as they were encountered and outlined clinical scenarios that might also be subject to these biases. Topics of discussion included not only decision-making biases but also heuristics, risk preferences, and decision process theory. For a full outline of the decision-making workshop, please see Appendix C. Finally, at the conclusion of the session, students completed a questionnaire (Appendix D) to better understand how they internalized the program content.
Backcountry skiing was selected because, as a wicked learning environment, the backcountry skiing environment is subject to similar cognitive biases as the clinical environment. 9 Some similar biases experienced in both the clinical environment and the backcountry environment include: authoritative bias, where participants tend to trust the person with the most experience; the bandwagon effect, where participants trust the group behavior without actively participating in critical thinking; and overconfidence bias, where participant's confidence in their decisions is reliably greater than the objective data. 5 This parallel experience makes backcountry skiing an ideal and engaging experiential learning domain for teaching clinical decision-making bias.
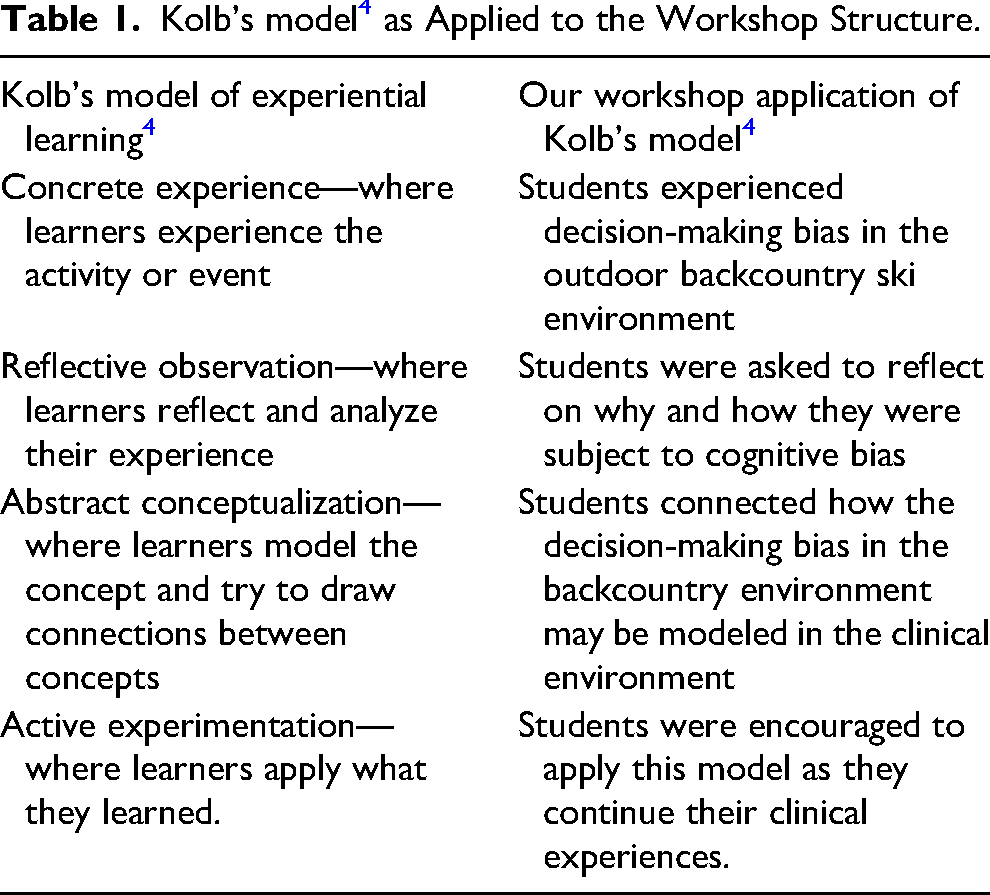
Throughout the experiential learning portion, the content experts guided students through discussions (Appendix B) focused on decision-making pitfalls as the group encountered them. Participants were encouraged to reflect on their clinical correlates throughout. Discussions were inspired by Kolb's model of experiential learning as outlined in Table 1. 6
Kolb's model 4 as Applied to the Workshop Structure.
Description of Themes.
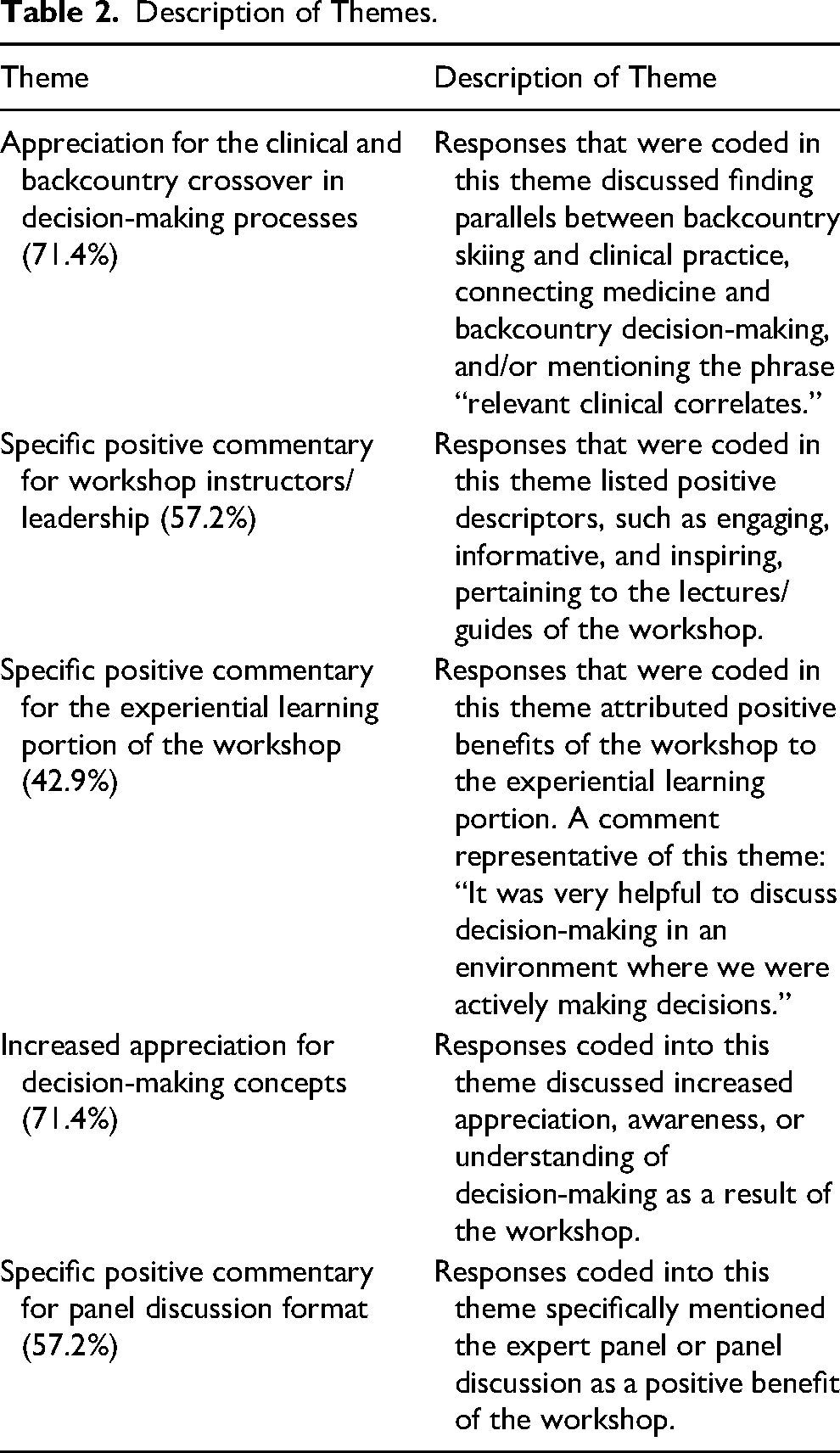
We evaluated the impact of the workshop by asking participants to comment on benefits and barriers in a post-workshop survey immediately following the workshop. Comments were thematically analyzed using two independent researchers; all differences were adjudicated with a third independent researcher. Responses were thoroughly reviewed to identify recurring patterns and key concepts, allowing for the development of initial themes, which were then grouped into broader themes. This qualitative method was selected because the collection of free text feedback would not bias student responses. Additionally, it allowed for a greater understanding of the student experience, reception of the workshop, and areas for the workshop to improve.
Outcomes
Twenty-six students participated in the first and second classroom components, and of those 26, 8 (30.8%) participated in the outdoor experiential day. Seven (26.9%) total students completed the end-of-workshop survey, and 4 students (15.4%) who participated in both the classroom and the experiential learning day completed the survey. When analyzing the positive benefits of the 2-day workshop experience, the following prominent themes emerged: appreciation for the clinical and backcountry crossover in decision-making processes (71.4%), specific positive commentary for the workshop instructors/leadership (57.2%), specific positive commentary for the experiential learning portion of the workshop (42.9%), increased appreciation for decision-making concepts (71.4%), and specific positive commentary for the panel discussion format (57.2%) (Table 2).
Respondents were also asked if there were any barriers to getting the most out of either portion of the workshop. Of the total respondents, 5 of the 7 (71.4%) reported no barriers. The remainder of the respondents requested splitting the group according to familiarity with workshop content (28.6%). Specific to the experiential day, some students felt they wanted more time for the experiential session (28.6%). There was no negative feedback outside of the reported barriers. When asked for any additional feedback or comments for the workshop, 5 of the 7 (71.4%) survey respondents stated that they would participate in the workshop again.
Discussion
Currently, wilderness medicine education focuses on training that emphasizes specific tangible skills such as rope rescue, hyper/hypothermia management, and wound care. While these trainings are incredibly useful for physicians who go on to practice in wilderness settings, the skills that are taught are relatively limited to a narrow field of practice. We believe that by emphasizing the human factors fundamental to wilderness medicine, such as decision-making, improvisation, and critical thinking, wilderness medicine education can be more broadly utilized across multiple disciplines.
The unique combination of outdoor experiences with medical education allows students to encounter real-world decision-making challenges in a controlled yet unpredictable environment. 7 This hands-on approach enables students to make critical decisions under pressure, reflect on their actions, and discuss their experiences with peers and instructors. Such scenarios are difficult to replicate in a traditional classroom setting, where the lack of real-time, high-stakes decision-making can limit students’ ability to internalize concepts. By integrating outdoor experiential learning, the program encourages deeper self-reflection, resilience, and adaptive thinking. Furthermore, the social cohesion fostered during these experiences can create a supportive learning community, enhancing student engagement and fostering a culture of mutual learning and feedback. 8
The results of our pilot study emphasize this theory by suggesting that this novel experiential learning model provided students with a greater appreciation of how decision-making biases may intersect with practical applications in medical settings. We believe that this workshop is an important step for improving bias within clinical decision-making. Increasing awareness of bias through participation in workshops and learning modules helps providers learn about nonconscious processes that help them reduce bias overall.7,9 Not only does this reduction in bias improve patient care, but it also has a significant impact on medical education at large. 10 While previous work on bias in medical education primarily focused on the impact of decision-making bias on the treatment of racial and ethnic minorities, we believe the in-depth teaching of decision-making bias has implications for clinical decision-making, including and beyond implicit bias. Despite the high yield implications of teaching clinical decision-making and decision-making biases, there is very limited teaching on this topic. We believe that through the use of novel workshops that incorporate outdoor experiential learning, such as the one outlined in our study, we can improve clinical decision-making.
There are several limitations of the current results. First and foremost, the data is extremely limited by the low participation rate and high attrition rate. These rates are likely multifactorial due in part to the timing of the workshop, the high burden of gear required to participate, and the high burden of skill necessary to participate. Students were asked to participate during one of the final days of their winter break and were not offered any form of incentive for participation. The workshop required that students have their own backcountry ski/snowboard equipment to participate and also required that students have a preliminary knowledge of backcountry travel. Future iterations of this course will strive to incentivize participation with course credit offerings and protective academic time and offer equipment to help minimize these burdens and improve attrition.
Furthermore, the response rate was also relatively low among participants. This is also likely multifactorial, due in part to lack of cellphone service/devices during the experiential learning portion, lack of protected time to complete the survey, survey distribution format, and overall lack of emphasis on the post-course survey by course leadership and instructors. In future iterations of this course, the survey will be distributed via paper, and participants will be given time during the workshop to complete the survey, as well as a brief explanation of the importance of survey response. Additionally, given the enthusiastic reception of this program and the short duration between course completion and survey administration, some responses may be affected by post-course euphoria. Post-course euphoria refers to a common phenomenon when students return from the field in an elevated or euphoric state, which may impact their self-reporting. 8
We believe, however, that our results are worth sharing because they provide insight into how outdoor recreation experiences can be combined with experiential learning methods to augment medical education. Additionally, our pilot curriculum can serve as a model for a novel approach to teaching clinical decision-making. Given the very limited teaching of clinical decision-making at baseline, we are encouraged by the largely positive pilot results and are hopeful that as this course is disseminated, the curriculum will continue to evolve.
Based on our initial findings, we plan to improve and scale up the workshop for an entire cohort of medical students. Based on the results of this project, future iterations will allow students to self-select into groups based on their skill set and preferences. Additionally, to better understand how field-based experiential education may enhance medical education, we plan to include a measurement of longitudinal retention of the material. Future iterations of this workshop could improve the participation and attrition by providing elective course credit upon completion and exploring options for providing students with rented backcountry gear to decrease the barrier of access for the ski-touring day. Outdoor activities other than backcountry skiing and non-outdoor wicked learning environments could also be selected when scaling up the experience. Future iterations of this study will employ a pre- and post-test system to evaluate learning, incorporate quantitative metrics, and conduct longitudinal evaluation.
To the best of our knowledge, this program is entirely unique in medical education and may be replicated by other medical schools seeking to add greater depth to student learning outcomes, increase student engagement, and create social cohesion while introducing the science of decision-making.
Conclusion
This pilot study demonstrates the potential of outdoor experiential learning to address critical gaps in medical education by teaching decision-making biases in engaging, high-stakes environments. By leveraging the parallels between clinical and backcountry settings, the workshop fostered additional and broader understanding of how decision-making biases may interfere with practical applications in medical settings. There is clear potential for the programming to be expanded and applied to other forms of the outdoor recreation experience.
Supplemental Material
sj-docx-1-wem-10.1177_10806032251334298 - Supplemental material for Decision-Making in the Backcountry and Its Clinical Applications in Medical Education—a Pilot Experiential Learning Workshop
Supplemental material, sj-docx-1-wem-10.1177_10806032251334298 for Decision-Making in the Backcountry and Its Clinical Applications in Medical Education—a Pilot Experiential Learning Workshop by Sarah Petelinsek, Peilu Zhang, Jorie Colbert-Getz, Theodore Hartridge, Nate Furman and Patrick G. Hughes in Wilderness & Environmental Medicine
Supplemental Material
sj-docx-2-wem-10.1177_10806032251334298 - Supplemental material for Decision-Making in the Backcountry and Its Clinical Applications in Medical Education—a Pilot Experiential Learning Workshop
Supplemental material, sj-docx-2-wem-10.1177_10806032251334298 for Decision-Making in the Backcountry and Its Clinical Applications in Medical Education—a Pilot Experiential Learning Workshop by Sarah Petelinsek, Peilu Zhang, Jorie Colbert-Getz, Theodore Hartridge, Nate Furman and Patrick G. Hughes in Wilderness & Environmental Medicine
Supplemental Material
sj-docx-3-wem-10.1177_10806032251334298 - Supplemental material for Decision-Making in the Backcountry and Its Clinical Applications in Medical Education—a Pilot Experiential Learning Workshop
Supplemental material, sj-docx-3-wem-10.1177_10806032251334298 for Decision-Making in the Backcountry and Its Clinical Applications in Medical Education—a Pilot Experiential Learning Workshop by Sarah Petelinsek, Peilu Zhang, Jorie Colbert-Getz, Theodore Hartridge, Nate Furman and Patrick G. Hughes in Wilderness & Environmental Medicine
Supplemental Material
sj-docx-4-wem-10.1177_10806032251334298 - Supplemental material for Decision-Making in the Backcountry and Its Clinical Applications in Medical Education—a Pilot Experiential Learning Workshop
Supplemental material, sj-docx-4-wem-10.1177_10806032251334298 for Decision-Making in the Backcountry and Its Clinical Applications in Medical Education—a Pilot Experiential Learning Workshop by Sarah Petelinsek, Peilu Zhang, Jorie Colbert-Getz, Theodore Hartridge, Nate Furman and Patrick G. Hughes in Wilderness & Environmental Medicine
Footnotes
Acknowledgments
We would like to express our sincere gratitude to Dr Richard Ingebretsen, MD, PhD, for his support and guidance of this project, as well as Dr Megan Fix, MD, for her passion and enthusiasm in continuing to facilitate this project and connecting the research team with necessary resources.
Author Contribution(s)
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study was funded through the support of AWLS, which allowed for financial compensation of the backcountry touring guides.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.