
Abstract
Snakebites are a critical health issue in remote regions of the Amazon basin. I report a case of Bothrops bilineatus envenomation in a 29-y-old biologist conducting fieldwork in Parque Nacional del Manu, Peru. Following significant logistic delays—including an initial suboptimal antivenom dose and limited access to additional vials—the patient developed progressive edema, necrosis, coagulopathy, and signs of compartment syndrome. Management involved 2 partial doses of antivenom (1 at 1600 and the other at 2100), a subsequent transfer to a tertiary care center, antibiotics, analgesia, and eventually surgical intervention, including debridement and partial amputation. Although the patient received some treatment on the day of the bite, fragmented antivenom dosing and delayed transport likely contributed to worse local injury. This case highlights the importance of prompt, complete antivenom therapy, effective logistics, advanced diagnostic resources, and comprehensive rehabilitation in resource-limited settings.
Introduction
Snakebites represent a major yet underestimated public health issue in tropical and rural regions, particularly in the Amazon basin, where Bothrops species account for most of the envenomations. 1 In remote areas of Peru, limited antivenom availability and a strained healthcare infrastructure exacerbate the risk of severe local and systemic complications. Bothrops bilineatus, known locally as the loro machaco, is an arboreal pit viper whose cytotoxic and hemotoxic venom can lead to tissue necrosis, coagulopathy, thrombocytopenia, and, in rare cases, acute renal failure. Although compartment syndrome has been reported in snake envenomations, it is most often a misdiagnosis caused by transiently elevated intracompartmental pressures associated with significant myositis following moderate to severe local envenomation. True compartment syndrome is rare and tends to occur only when envenomation involves a “tight” anatomic site (eg, the tibial region). Importantly, the decision to perform a fasciotomy should be reserved for patients with unequivocal clinical evidence of true compartment syndrome rather than based solely on isolated pressure measurements.1–5
Early administration of antivenom—ideally within the first 4–6 h—and innovations such as portable ultrasonography can reduce morbidity and disability significantly.6,7 Nevertheless, socioeconomic and logistic constraints often impede timely management, highlighting the need for reliable antivenom distribution pathways, improved training for rural providers, and effective community-level prevention programs.8–12
In this case report, I describe a B bilineatus bite that led to digital amputation, stressing how suboptimal initial dosing and procedural delays can shape clinical evolution.
Case Report
On December 5, 2023 (Day 0) at 0900, a 29-y-old male biologist was bitten on the second finger of his right hand by a B bilineatus while conducting fieldwork in Parque Nacional del Manu (Madre de Dios, Peru). The patient, who recognized the snake from previous herpetologic experience, soon developed severe localized pain, swelling, and mild systemic symptoms such as nausea and dizziness as he sought help. By 1600, after overcoming significant transportation challenges on difficult terrain, he arrived at the Shintuya Health Center, where he received an initial—but suboptimal—dose of antivenom (2 vials) along with tramadol and paracetamol for pain control. Unfortunately, the available antivenom stock was limited, and pain management remained incomplete. At 2100, following further delays due to authorization hurdles and a shortage of doses, the patient was administered an additional 2 vials, although the total quantity still fell short of the typically recommended regimen for moderate to severe envenomation. Later that evening, at 2300, the patient began a prolonged transfer by road and boat to a tertiary care hospital, a journey further impeded by limited emergency transport infrastructure.
On December 6, 2023 (Day 1) at 0300, the patient arrived at Hospital Nacional Adolfo Guevara Velasco in Cusco. On examination, clinicians noted severe edema extending from the bitten finger to the midforearm, incipient necrosis around the puncture site, and a history of anuria for ∼5 h. Laboratory tests revealed thrombocytopenia, coagulopathy with an elevated international normalized ratio, and increased C-reactive protein levels. The patient was promptly admitted to the intensive care unit for comprehensive management, which included an additional 4 vials of antivenom, broad-spectrum antibiotics (piperacillin-tazobactam), potent analgesics (fentanyl and metamizole), intravenous fluids, and diuretics to address acute kidney concerns.
On December 7, 2023 (Day 2), necrosis continued to progress in the affected finger, raising suspicion of compartment syndrome. The clinical team conducted serial assessments—including evaluations of peripheral pulses, capillary refill, motor and sensory function, and bedside Doppler ultrasound—to monitor tissue perfusion. Despite extensive swelling, no acute arterial compromise or dangerously high compartment pressures were detected, so conservative measures were implemented: The limb was elevated, neurovascular status was closely monitored, and analgesia was maintained rather than proceeding with a fasciotomy.
By December 8, 2023 (Day 3), surgical debridement of the devitalized tissue in the second finger was performed. Although significant edema persisted, there was no further systemic deterioration. Between December 9 and 12, 2023 (Days 4–7), laboratory parameters began to improve, with rising platelet counts and normalization of coagulation markers; however, necrosis continued to progress distally, prompting careful consideration of a partial amputation. On December 13, 2023 (Day 8), with clear demarcation of necrosis in the distal phalanx, a partial amputation of the second finger was performed to prevent further tissue death, infection, or additional functional compromise.
By December 17, 2023 (Day 12), the patient showed progressive wound healing, reduced swelling, and normalized renal function. He was discharged on December 18, 2023 (Day 13) with instructions for physical therapy to restore hand function, along with scheduled follow-up appointments in trauma surgery and continued wound care.
Figure 1 is a timeline graphic of this case report for enhanced clarity, and detailed laboratory and pharmacologic data appear in Tables 1 and 2.
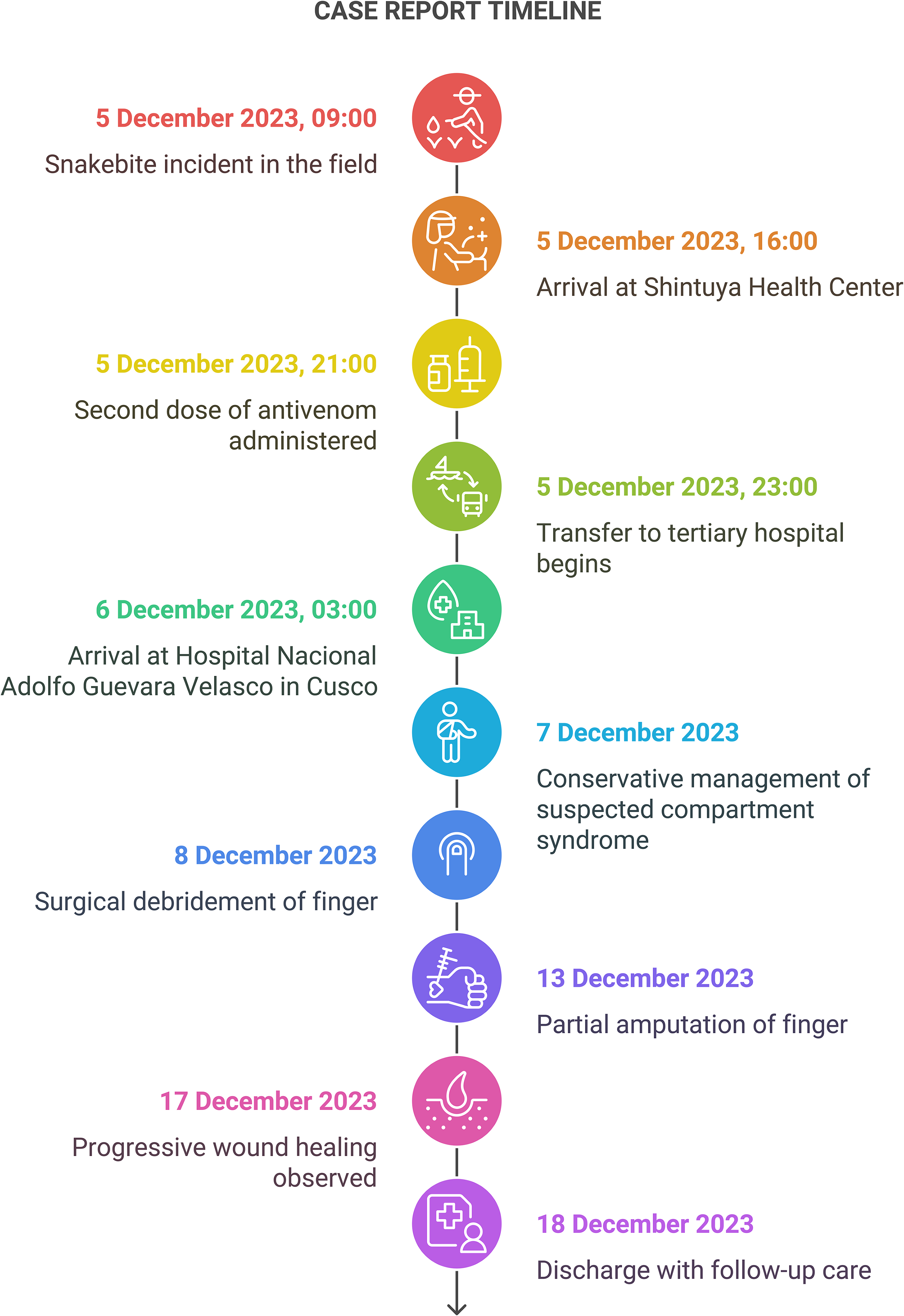
Timeline of this case report.
Laboratory findings revealed thrombocytopenia, coagulopathy, and elevated inflammatory markers.

Evolution of treatments and medications administered.
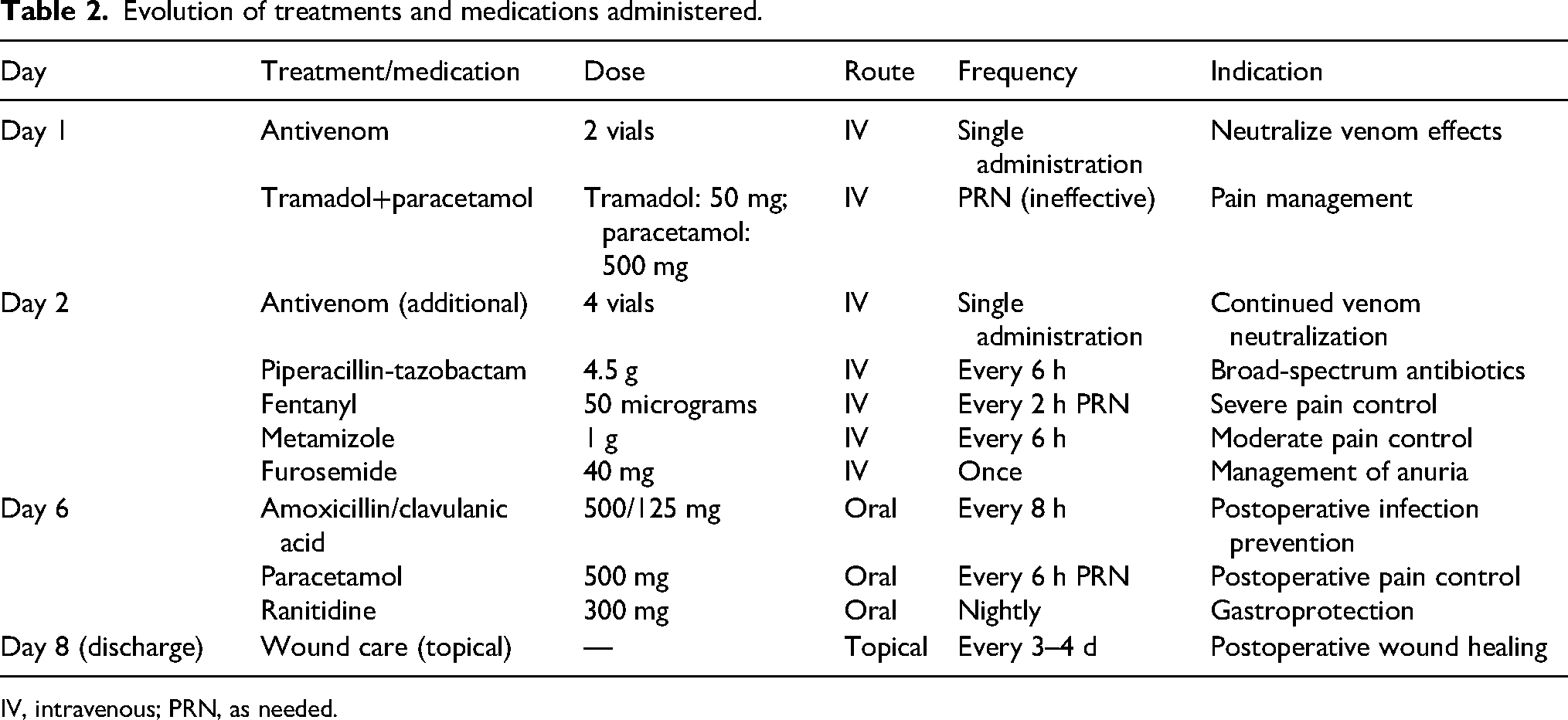
IV, intravenous; PRN, as needed.
Discussion
This case underscores the severity of B bilineatus envenomation in a remote Amazonian region as well as the impact of fragmented and delayed antivenom administration on clinical outcomes. Although the patient did receive some antivenom relatively early (7 h after the bite, at 1600), the incomplete dosing and ensuing logistic delays meant that a full therapeutic regimen was not achieved until nearly 18 h after the bite.
Although the first dose occurred 7 h after the bite (which can be considered moderately delayed in an optimal scenario), the real issue may be that the total recommended antivenom dose was not administered promptly. Previous research confirms that effective, complete antivenom therapy within the first 4–6 h is crucial to limit venom activity and subsequent tissue injury.2,6 In such situations, partial doses may reduce symptom progression but remain insufficient to avert severe complications such as necrosis or compartment syndrome.
In crotaline snakebites, apparent pseudo-compartment syndrome can occur due to edema and inflammation, although true vascular compromise is less common.4,5 Here, despite severe swelling and pain, repeated neurovascular checks showed adequate perfusion, allowing the team to avoid fasciotomy. This conservative approach aligns with newer recommendations to reserve fasciotomy for documented ischemia or intractably high compartment pressures measured directly via needle manometry.
This case highlights persistent healthcare barriers in the Amazon—namely limited antivenom stocks at remote outposts, bureaucratic obstacles to obtaining additional doses, and challenging transport logistics. Improved distribution strategies, a refined cold-chain system, and standardized triage protocols could reduce the time from bite to complete antivenom therapy.8,11,12
Furthermore, postdischarge care, including physical and psychosocial rehabilitation, remains vital. Studies indicate that coordinated rehabilitation and psychological support significantly enhance long-term functional recovery and quality of life in snakebite survivors.10,13
Limitations
A key limitation of this case report is that the snake species was identified solely based on the account provided by the bitten patient and was not formally verified through expert analysis or laboratory confirmation. It is important to acknowledge that arboreal crotaline viperids can exhibit considerable variation in appearance, and even experienced field biologists occasionally may misidentify them. However, the patient in this case was highly familiar with the local herpetofauna, with extensive practical experience in the region, which supports the reliability of his identification. Despite this, the potential for misidentification remains a noteworthy limitation.
Conclusions
This case of B bilineatus snakebite in Peru's Amazon region demonstrates the implications of partial and delayed antivenom administration. Despite receiving an initial dose 7 h after the bite, the patient ultimately required partial amputation of the affected digit due to progressive necrosis. Sustained swelling also raised concern for compartment syndrome, although no fasciotomy was performed after thorough clinical evaluations ruled out true vascular compromise. To mitigate such outcomes, early and complete antivenom dosing, streamlined transport logistics, advanced diagnostic assessments, and robust rehabilitation services are essential—especially in low-resource settings. Ongoing endeavors to improve antivenom availability and distribution, reinforce regional referral systems, and expand community awareness will be pivotal in reducing the burden of snakebite envenomation in remote locales.
Footnotes
Consent for Publication
Written informed consent for publication was obtained from the patient. All identifying details have been anonymized where necessary to protect patient confidentiality.
Data Availability
All relevant data supporting this case report are contained within this report. Additional information is available on reasonable request from the author.
Ethical Considerations
This report is a retrospective case description and does not involve interventional research on human subjects.
Financial/Material Support
This work did not receive any specific funding or financial support from funding agencies in the public, commercial, or not-for-profit sectors.