
Abstract
Nautical trauma is a rare event yet characterized by high rates of mortality and morbidity. The management of the victims is complicated by environmental challenges and often remote locations. Another challenge is the absence of a triage tool specifically designed for nautical environments. The Serenissima Overboard Triage and Rescue protocol is a triage tool aimed at improving the management of nautical incidents. This tool was developed for responders in the Venetian Lagoon (Italy). This method uses a step-by-step process. For optimal efficiency, rapid triage should begin while the victims are still in the water. Patients are sorted into 4 triage categories: black (not breathing after airway opening and 5 rescue breaths or injuries incompatible with life), red (respiratory rate >30 breaths/min, unable to talk, stertorous breathing/wheezing, or altered mental status), yellow (respiratory rate <30 breaths/min and alert, floating but not able to swim), and green (purposeful swimming and able to maintain airway). This tool can improve the rapidity and quality of rescue in mass-casualty nautical accidents but will need further validation.
Introduction
Nautical trauma is a rare event compared with other kinds of accidents, but it is characterized by higher rates of mortality and morbidity due to the complications resulting from drowning and hypothermia, challenges of extraction from water, and often remote locations.1,2 Nautical accidents also frequently result in mass-casualty incidents distinguished by multiple victims and a finite number of resources, including responders needed to locate, rescue, and treat multiple patients. 3 Another challenge is that there is not a triage tool specifically designed for nautical environments to accelerate and maximize clinical efforts in these types of environments.
Concept Development
Existing triage tools generally focus on airway and bleeding and are not designed for the specific environment of nautical trauma or for the clinical characteristics of drowning and hypothermia victims. The Simple Triage and Rapid Treatment (START) protocol is the current triage tool for mass-casualty incidents endorsed by the National Health Service (NHS) of the United Kingdom and used globally 4 (Figure 1). START allows only 2 operative procedures: hemostasis by compression of external hemorrhages and opening of the airways. In maritime incidents, to accelerate the process, triage should be started when the casualties are still in water, but despite extensive literature on prehospital triage, there is a striking absence of systematic reviews or validated protocols addressing this situation. The only relatable tool is the In-Water Mass Casualty Triage Tool by Tipton et al, which is based on physiologic precursors to immersion-related deaths. 5 This tool was developed for use in a military setting and the possibility of being under hostile fire, but it is also applicable in a civilian context. It categorizes casualties from W1 (high) to W4 (low) priority for rescue, and it involves airway management if the airway is under the surface but there are purposeful signs of movement.
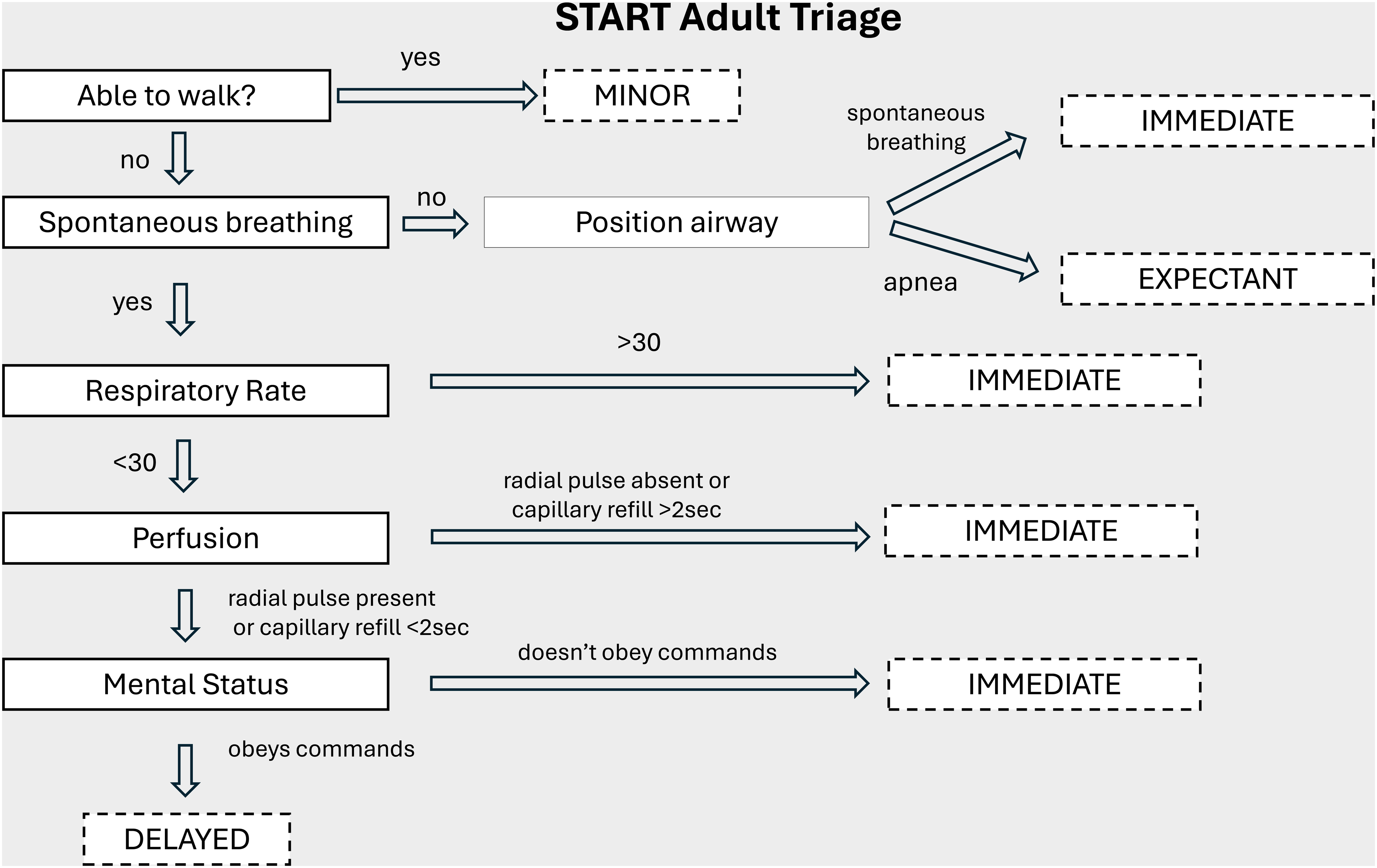
Simple Triage And Treatment (START) is composed by 4 categories. Expectant (black code): The victim is unlikely to survive given severity of injuries, level of available care, or both. Immediate (red code): The victim can be helped by immediate intervention and transport; they require medical attention within minutes for survival (up to 60 min). The code includes compromises to airway breathing or circulation. Delayed (yellow code): The victim's transport can be delayed; the code includes serious and potentially life-threatening injuries, but the victim is not expecting to deteriorate significantly over several hours. Minor (green code): For victims with minor injuries whose status is unlikely to deteriorate over days. Minor codes can be addressed to secondary triage.
Serenissima Overboard Triage and Rescue
The Serenissima Overboard Triage and Rescue (SOTeR) protocol was developed for responders in the Venetian Lagoon (Figure 2). Nautical trauma there is common due to the widespread distribution of water transport for private and public use and the large number of annual visitors, which is amplified during special events and festivals. For example, the annual Festa del Redentore brought ∼30,000 attendees and 4000 boats to the Lagoon in July of 2025. The SOTeR protocol is designed for situations of 2 or more victims, assuming that the water ambulance is the only available means of rescue at the event location. This is the most common scenario of a nautical incident in the setting of the Venetian Lagoon and is similarly applicable to any location where water ambulances are employed (eg, Sweden, Dubai, and Indonesia). Water ambulances are equipped for extrication, trauma care, and Advanced Life Support, but they are not provided with rescue divers to assist with trauma and drowning victims. They can carry a maximum of 2 patients with 1 on a stretcher and 1 in a sitting position 6 (Figures 3 and 4).
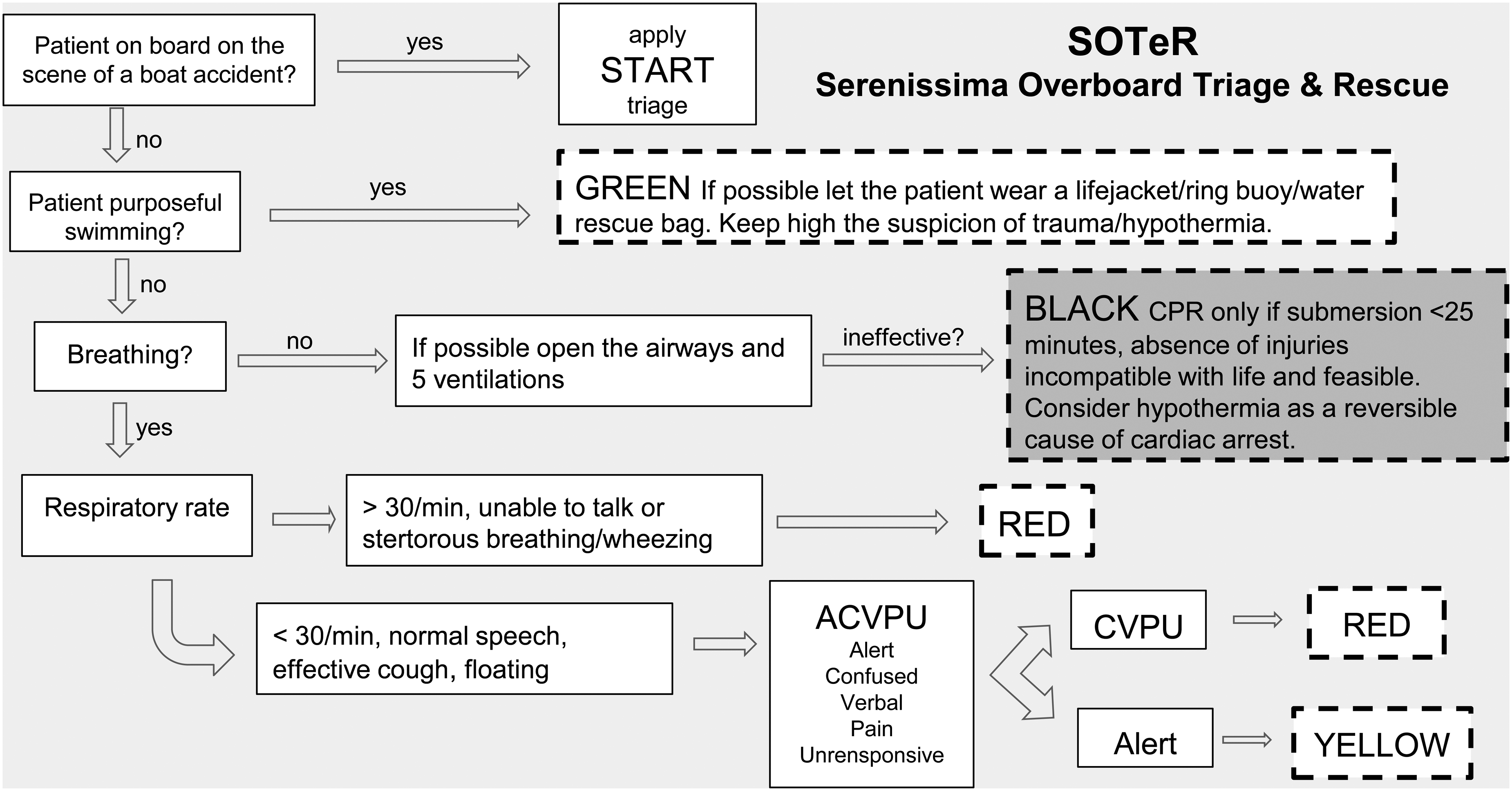
The Serenissima Overboard Triage and Rescue (SOTeR) protocol applies to in-water victims of mass-casualty nautical incidents. The triage categories are defined by purposeful swimming, respiratory rate and efficacy of breathing, and state of consciousness. Black is used for casualties with no signs of life, and cardiopulmonary resuscitation should be started only if submersion time is <25 min and if feasible because it implies extraction of the patient from the water.

Venice Lagoon water ambulance (inside view).

Venice Lagoon water ambulance.
The SOTeR protocol follows a sequential approach, where physical contact occurs only if needed and feasible (ie, environmental conditions and plausible effectiveness of cardiopulmonary resuscitation).
The victims are sorted into 4 triage categories:
Black: Not breathing after airway opening and 5 rescue breaths or injuries incompatible with life Red: Respiratory rate >30 breaths /min, unable to talk, stertorous breathing/wheezing, or altered mental status Yellow: Respiratory rate <30 breaths/min and alert, able to float but not able to swim Green: Purposeful swimming and able to maintain airway
This tool was developed taking into consideration a list of items that indicate to the rescuer the presumed state of the victim, assuming that it is not immediately and physically possible to proceed with complete care but only with basic lifesaving procedures following an attempt at a physical approach.
These items include motor activity intended as purposeful swimming, respiratory rate and efficacy of breathing, and level of consciousness. Airway management will be provided as indicated in the START protocol, but neither the capillary refill time nor the radial pulse will be taken into consideration. This exclusion is due to the peripheral vasoconstriction effect of both the victim and the operators in contact with cold water and to the environmental challenge of reaching the in-water victim without rescue divers. In these situations, rescuers can initiate chest compressions and rescue breathing without an initial pulse check because pulse checks can be inaccurate and might delay resuscitation. 7 The items included in the protocol can be easily and quickly evaluated by a trained team from the elevated point of view of a rescue boat. The SOTeR protocol assumes that the scene is free from any kind of hazards such as fire or impending sinking of the boat involved in the accident (in which case a rapid extrication would be needed). A rapid rescue is also mandatory in case of storm, strong gales, or rough seas. Another necessary assumption is that the temperature of the water has already been assessed by the operators.
SOTeR Protocol Step-by-Step
1. Patient on Board on the Scene of a Boat Accident
The patients may be on board the boat involved in the accident or on board a boat that came to the rescue. In these circumstances, START can be applied. The START protocol should be undertaken similarly if the patients are found on dry land.
2. Patient Purposefully Swimming
If the patient is purposeful swimming and can keep their head above the surface of the water, they will be classified as code green. The green code does not rule out trauma or hypothermia, and drowning is still a risk, which is why a life jacket or other flotation device should be provided. Reassessment should be recurrent if maritime support is delayed.
3. Patient Spontaneously Breathing
If the patient is not spontaneously breathing yet is reachable by the operators, opening airway procedures should be undertaken followed by an attempt of 5 ventilations. Ventilation is a priority during resuscitation in cardiac arrest following drowning and generally can be provided by bag-mask ventilation or an advanced airway (the latter involves transferring the victim on board). 7 If the ventilations are ineffective, the victim should be boarded to start cardiopulmonary resuscitation if the submersion lasted <25 min and if there is a sufficient number of operators. 8 If clearly lethal injuries or rigor mortis is found when the patient is on board, no resuscitation should be attempted.
4. Respiratory Rate
If the patient is breathing with a respiratory rate of 30 breaths/min or more, unable to talk, or presents stertorous breathing or wheezing, they will be designated code red and will require emergent medical treatment. Otherwise, a quick evaluation of mental status will be required via the ACVPU (Alert, Confused, Verbal, Pain, and Unresponsive) scale because new-onset confusion and a deteriorating level of consciousness are indications for serious illness and require urgent treatment. 9
5. ACVPU
The patient will be classified by the ACVPU scale as alert, confused, verbal, in pain, or unresponsive. A patient who is is alert and oriented will be coded as yellow; otherwise, the appropriate code will be red.
Conclusions
We described the development of SOTeR protocol, a new triage tool that aims to improve the rapidity and quality of rescue in mass-casualty nautical accidents in which more victims are in the water and the number of rescuers is limited. This triage tool is integrated with basic lifesaving procedures.
A limitation of this tool is that the submersion time could not have been exactly calculated by the witnesses or the dispatcher. Another possible limitation is the lack of hemorrhage control in the triage phase caused by the difficulty of seeing blood in seawater, especially at nighttime or during adverse weather conditions. In addition, respiratory rate also can be tricky to evaluate in a strong gale or heavy seas.
The SOTeR protocol will need further validation, so a pilot study in a controlled environment with simulated patients will take place in the short term to assess the effectiveness and efficiency of this tool.
Footnotes
Acknowledgments
We wish to thank Daniele Pomiato (ULSS3 Serenissima) and the local firefighters association Corpo Nazionale Vigili del Fuoco (Comando Provinciale di Venezia Nucleo Sommozzatori) for their input and advice in this project.
Author Contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.