
Abstract
Introduction
Numerous foreign tourists climb Mount Fuji, but the factors influencing falls and the symptoms of acute mountain sickness (AMS) in Japanese and foreign climbers remain unclear.
Methods
A questionnaire survey assessed fall occurrence, AMS symptoms, sex, age, climbing experience, use of a tour guide, awareness of fall risks, trekking-pole use, shoe type and sole condition, fatigue, height, body mass, and a single day or overnight climbing. Multiple logistic regression with Akaike information criterion-based model selection was used to identify predictors, including interaction effects of nationality.
Results
Valid responses were obtained from 693 Japanese and 244 foreign climbers. The fall rate was 27% in both groups. Female sex and greater fatigue were associated with a higher fall risk regardless of ethnicity. Advancing age was associated with a lower fall risk among foreign climbers but a higher fall risk among Japanese climbers. The prevalence of AMS was 47% among Japanese climbers and 32% among foreign climbers. Younger age and higher fatigue increased AMS risk. Foreign climbers without guides had a lower risk of AMS, whereas guide status was not associated with AMS risk among Japanese climbers.
Conclusions
These findings highlight the importance of targeted preventive guidance to reduce fall risk among female climbers, those experiencing greater fatigue regardless of ethnicity, and older Japanese climbers as well as to reduce AMS risk among foreign climbers participating in guided tours on Mount Fuji.
Introduction
Mount Fuji is the highest mountain in Japan (summit altitude 3776 m), with >200,000 visitors climbing it during the summer season (∼2 months), 1 which translates to an average of >3300 climbers per day. Given the large number of visitors, injuries from falls and high altitude illnesses such as acute mountain sickness (AMS) are major safety concerns. These conditions can lead to serious injuries and life-threatening complications, such as fractures and high altitude pulmonary edema, which may require medical treatment and rescue operations in a high-traffic mountain environment.2,3 We have previously conducted questionnaire survey studies on Mount Fuji and reported that ∼35% climbers experienced at least 1 fall4,5 and that ∼35% developed symptoms of AMS.6–8 Because Mount Fuji was registered as a United Nations Educational, Scientific and Cultural Organization World Heritage Site in 2013, the number of foreign climbers is expected to increase. 9
Approximately 25% of all climbers are foreign visitors who do not reside in Japan, representing a diverse range of home countries and native languages. 9 The top 10 nationalities include climbers from Taiwan, the United States, France, South Korea, China, Hong Kong, Germany, the United Kingdom, Spain, Singapore, and Australia. Despite this international presence, signboards along Mount Fuji's ascending and descending routes are displayed in only 3 languages—English, Korean, and Chinese—at selected locations. Although the causal relationship between the effects of signboards and the risks of a fall and AMS is uncertain, this limited-language coverage highlights a potential communication challenge for international climbers from diverse language backgrounds. Consequently, important information related to fall and AMS prevention, such as estimated ascent and descent times, cautions against rapid ascent, and directions at crossroads may be missed. Inadequate communication of these details can contribute to excessive physical or mental fatigue, both of which are known risk factors for slip-related falls.10,11 Additionally, rapid ascent to high altitudes increases the likelihood of AMS.12,13
In this regard, the prevention of falls and/or AMS symptoms is important to ensure safe and comfortable climbing because falls or AMS can lead to serious consequences, such as fractures or high altitude pulmonary edema. Several factors, including but not limited to being female,4,5 increasing age, 5 lack of information regarding fall risks, 14 inappropriate footwear use, 15 nonuse of trekking poles, 16 and obesity, 17 are associated with increased falls. Similarly, younger age 18 or older age, 19 being female,20,21 less climbing experience, 6 overnight staying, 8 and absence of a tour guide 18 are associated with increased AMS. However, no studies have specifically examined the characteristics of injuries and AMS among foreign climbers of Mount Fuji.
Accordingly, we conducted a questionnaire survey comparing Japanese and foreign climbers on Mount Fuji. We hypothesized that foreign climbers would be more likely to experience falls and symptoms of AMS than Japanese climbers and that the risk factors for falls and AMS would differ between groups.
Methods
The questionnaire survey site was established at the Yoshida trailhead sign (altitude 2269 m) and not at the Fuji-Subaru Line parking lot (altitude 2305 m), which is an ∼20-min walk from the survey site. This location was selected because the parking lot is frequented by tourists who do not climb Mount Fuji, making it difficult to distinguish climbers from nonclimbers. In addition, we confirmed whether the participants actually climbed Mount Fuji. According to the Ministry of the Environment, Government of Japan, the estimated ascent time from the survey site to the summit of Mount Fuji is ∼6.5 h for 5.0 km, with a mean gradient of 30%. The descent time from the summit back to the survey site takes ∼3.5 h for 6.4 km, with a mean gradient of 24% (Figure 1).
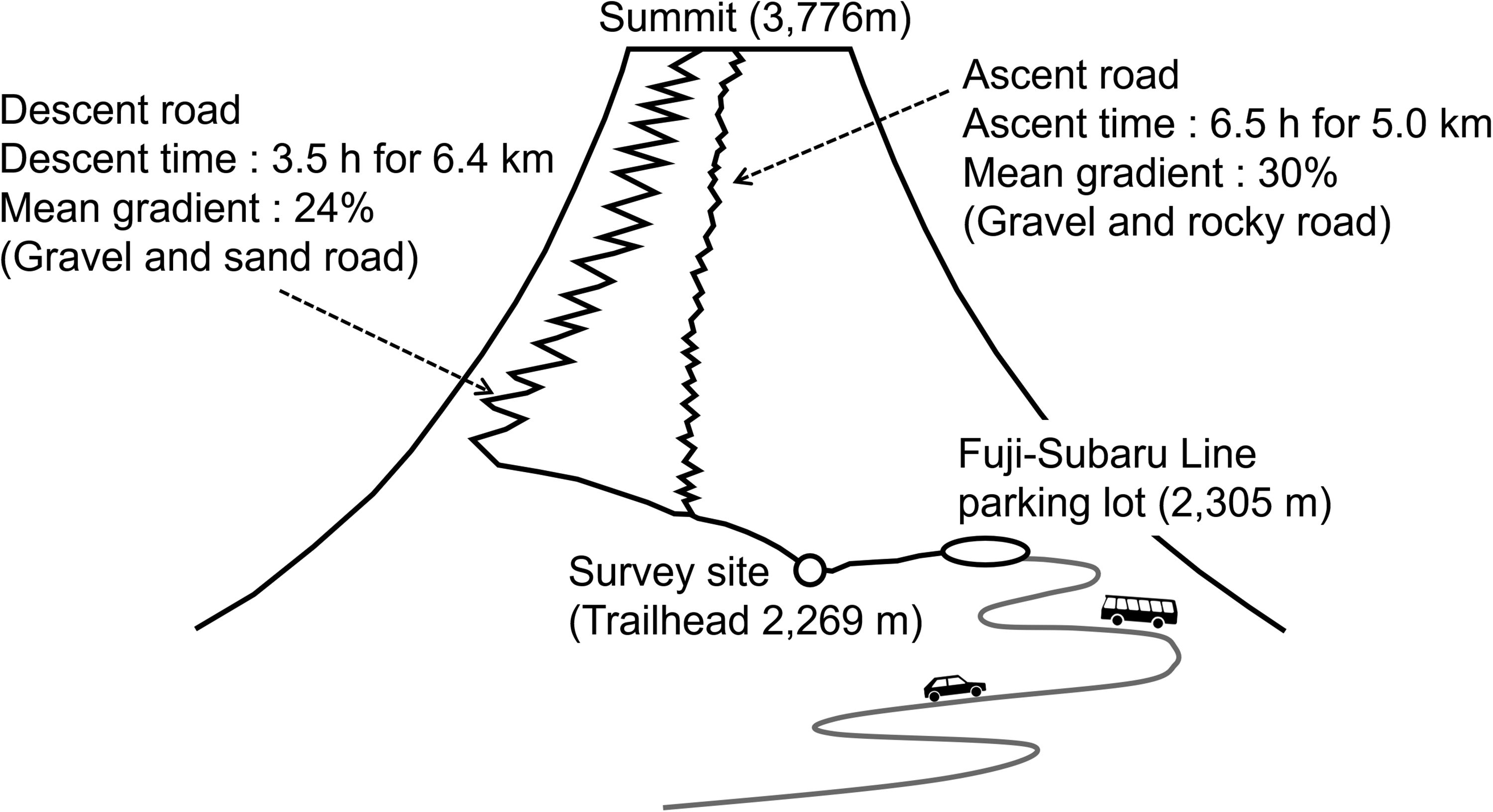
Elevation profile of the ascent and descent routes on Mount Fuji, including the survey site and summit.
This study was approved by the Ethics Committee of the Mount Fuji Research Institute in Japan in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants after a detailed explanation. We surveyed descending Japanese and foreign climbers who reached the survey site of Mount Fuji on August 10, 11, 21, and 26, 2023, and August 16, 19, 21, 22, and 26, 2024. For foreign climbers, we confirmed whether they were living in a foreign country or visiting as tourists and excluded foreign residents living in Japan. Participants were surveyed between 0800 and 1200 h. We confirmed that all climbers has started their climb from the fifth station parking lot, reaching there by private vehicle or tour bus, and had begun their descent early in the morning. The following criteria were confirmed: 1) It was the first response to the survey, and 2) there was sufficient time (∼10 min) to complete the questionnaire carefully. Participants who completed the questionnaire individually and without consultation with others were included.
The participants were instructed to read the QR codes using their smartphones to respond to all questionnaire parameters. Notably, for Japanese climbers and those from other countries, the QR codes are shown in Japanese and English, respectively. Table 1 lists the questionnaire parameters in this study. Of note, the Japanese questionnaire parameters were translated into English by a professional English editing service, all parameters were combined into Japanese and English versions, and both languages were translated into 1 sheet. Both Japanese and foreign climbers were asked whether they had fallen. In this study, a fall was defined as any unintentional ground contact involving 1 or more body parts (eg, hand, knee, or hip) during ascent or descent.
Questionnaire Survey Sheet Used in This Study.
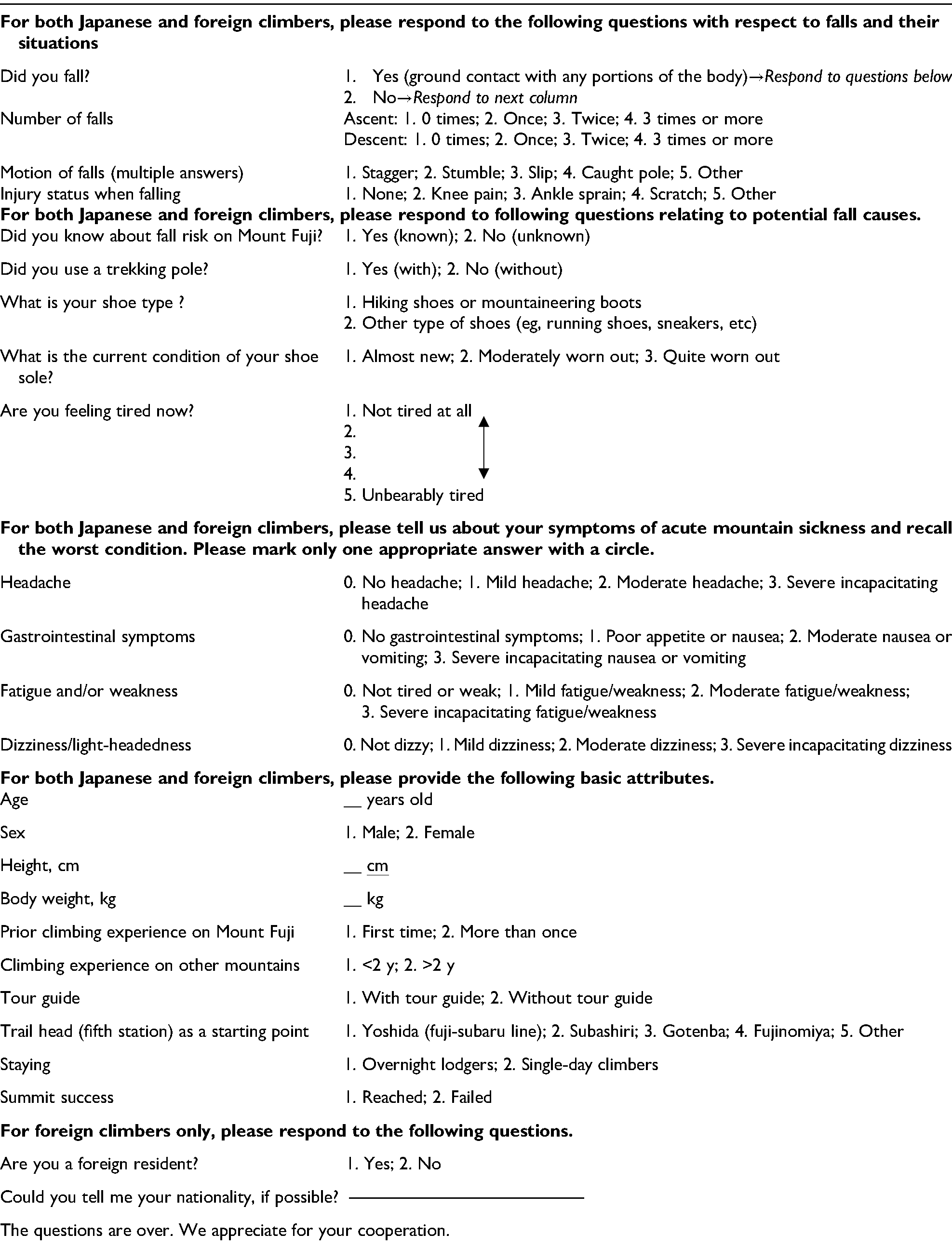
Based on their answers, participants were divided into 2 groups: no fall and fall. Furthermore, the questionnaire included fall-related parameters, such as number of falls, site of falls (eg, ascent or descent), motions of falls (eg, stagger, stumbling, slip, trekking pole, and others), injury status (eg, injured or not, knee pain, sprained ankle, scratch, and others), awareness of fall risk, use of trekking poles, shoe type (1=hiking shoes or mountaineering boots or 2=other type shoes [eg, running shoes or sneakers]), current shoe sole condition (self-reported as 1=almost new, 2=moderately worn out, or 3=quite worn out), and fatigue feeling with 5 choices (eg, not tired at all–unbearably tired). Similarly, symptoms of AMS were assessed using the 2018 Lake Louise Acute Mountain Sickness Score. This scoring system includes 4 subscales—headache, gastrointestinal symptoms, fatigue and/or weakness, and dizziness/light-headedness—with scores of 0 (none), 1 (mild), 2 (moderate), and 3 (severe). Participants with AMS were defined as a total score ≥3 with the presence of headache, and its severity was further classified as mild (3–5 points), moderate (6–9), and severe (10–12). 22 The survey also evaluated the following general attributes: age, sex, body mass index (body mass, kg(m2)–1), climbing experience on Mount Fuji and on other mountains, use of a tour guide, trailhead at the starting point, and whether the climb was a single-day climb or overnight. Only foreign climbers were instructed to respond to the following items: nationality, home-country departure date and its airport, and arrival date in Japan.
All analyses were performed using R, version 4.4.1 (R Foundation for Statistical Computing, Vienna, Austria). Continuous variables (eg, age and body mass index) are presented as mean±SD. Ordinal variables (eg, fatigue) are presented as 25th percentile, median, and 75th percentile. Categorical variables (eg, others) are presented as the number and percentages. Multiple logistic regression analysis was performed to identify the factor associated with fall or AMS risk among Japanese and foreign climbers. The dependent variables were no fall or no AMS scored as 0 and fall or AMS scored as 1. For fall risk, the independent variables included 14 items and 13 nationality interaction terms, whereas for AMS risk, these variables included 10 items and 9 nationality interaction terms. (ie, nationality × each variable) (Table 2). Before analysis, we calculated multicollinearity among the 16 independent variables using variance inflation factors because a high correlation between the independent variables can distort the results of multiple logistic regression analysis. All variance inflation factors were <4; therefore, we included all independent variables. To find a prediction model containing parameters that best explained the data, including the interaction effects of nationalities, model selection was performed using backward stepwise elimination using the Akaike information criterion (AIC). AIC estimates the relative quality of statistical models by balancing goodness of fit against model complexity. 23 During this process, the least important variables (lowest P values) were individually removed to obtain lower AIC values, and this process was repeated until the AIC values exceeded those of the prior model. The model with the lowest AIC value can be considered optimal; otherwise, at this final stage, irrespective of the P values (eg, the AIC value is the top priority as a prediction model even if the P values are >0.05). If a nationality interaction was detected, the effect of risk factors was estimated separately for each nationality in the multivariate logistic regression model. To compare weather conditions during the survey days between Japanese and foreign climbers, an unpaired t test was used, and only in this analysis, a P value of <0.05 was considered statistically significant.
Dependent and Independent Variables for Two Kinds of Multiple Logistic Regression Analyses.
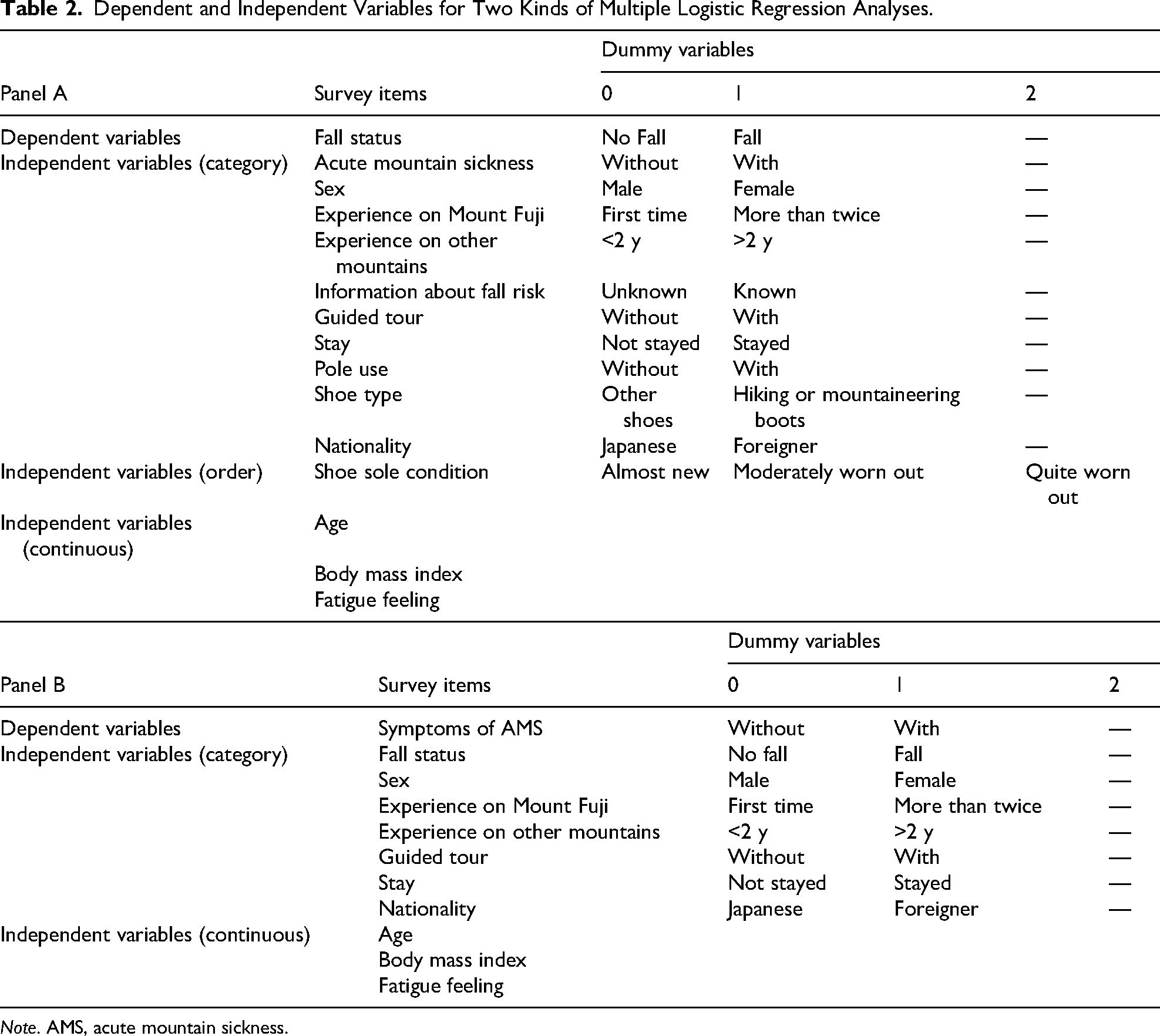
Note. AMS, acute mountain sickness.
Results
According to data from the Japan Meteorological Agency, the ambient barometric pressure at the summit of Mount Fuji ranged from 645 to 653 hPa, ambient temperature ranged from 2.8 to 14.8°C, and relative humidity ranged from 21 to 100% on the survey days. In addition, meteorologic data provided by the Japan Highway Public Corporation indicated that ambient temperature ranged from 10.8 to 19.5°C, mean wind speed ranged from 10.2 to 20.1 m·s–1, and hourly rainfall ranged from 0.0 to 70.0 mm·h–1 at the fifth station on the survey days. However, relative humidity was not recorded at this location.
A total of 693 Japanese and 244 foreign climbers were included in the final analysis. These represented 97% of Japanese and 98% of foreign respondents, respectively. An additional 21 Japanese and 5 foreign climbers were excluded because they were aged <15 years or had missing information. Among the analyzed sample, 30 Japanese climbers and 4 foreign climbers did not reach the summit of Mount Fuji; these participants were retained in the analysis because the primary aim was to examine factors associated with falls and AMS regardless of summit attainment.
Figure 2 shows the distribution foreign participants by nationality. Among the 244 foreign participants, 8 did not report their nationality, leaving data from 236 individuals. The largest group of participants was from Taiwan (25%), followed by climbers from Hong Kong (12%), the United States (10%), Singapore (8%), France (7%), Canada (6%), the United Kingdom (4%), Italy (2%), the Netherlands (2%), and Germany (2%). Additionally, 169 participants (72% of the total foreign participants) were native speakers of 1 of the 3 languages used on Mount Fuji's signboards: English (43% of 169 participants), Chinese (54%), and Korean (2%).
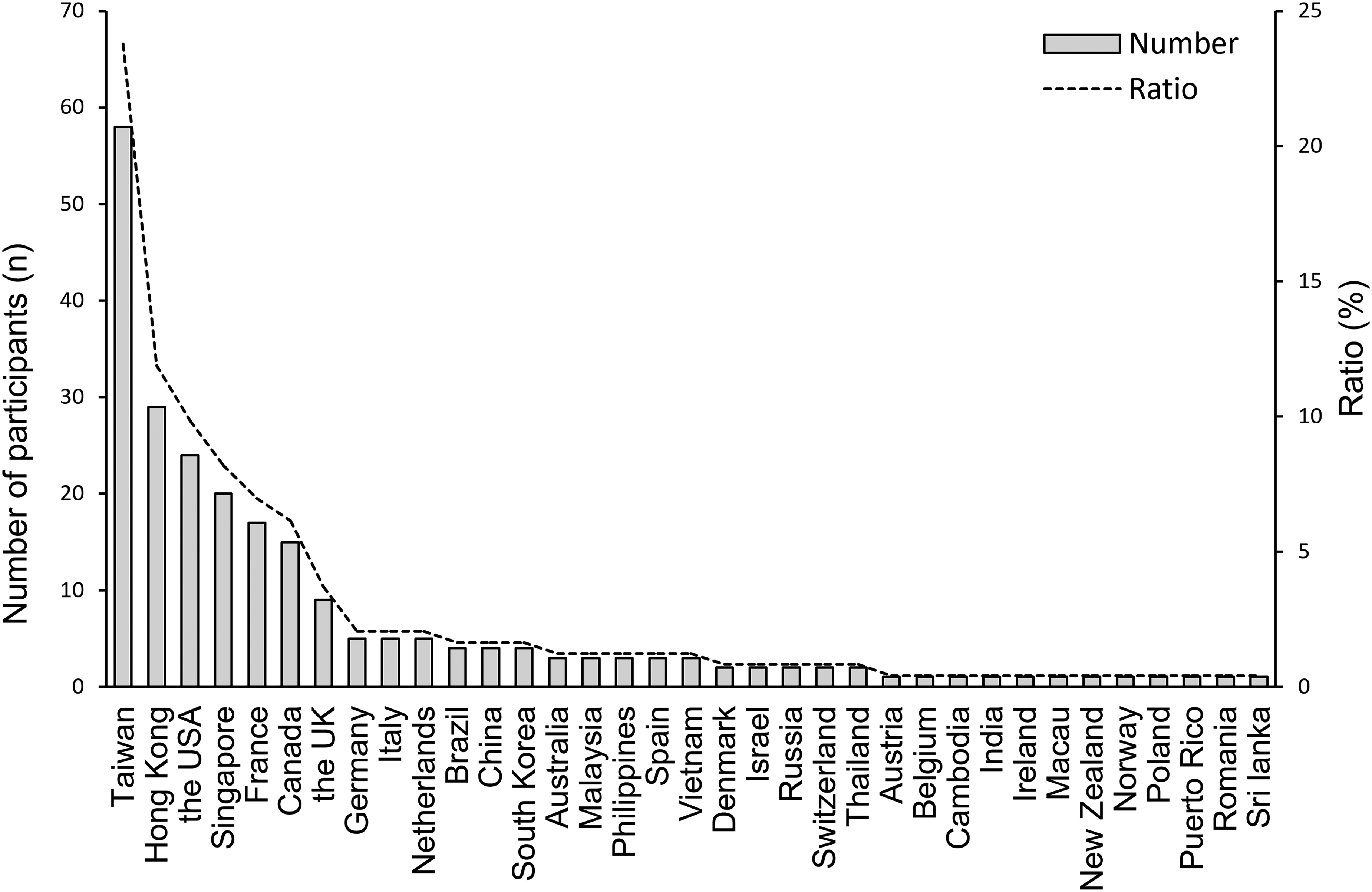
Distribution of foreign climbers. Bar graphs represents the actual number of participants (on the left y-axis), whereas the dotted-line graph indicates the proportion of all foreign climbers (on the right y-axis).
A total of 186 Japanese climbers (27%) and 66 foreign climbers (27%) reported at least 1 fall during the ascent or descent. Similarly, 328 Japanese climbers (47%) and 77 foreign climbers (32%) experienced AMS. Detailed distributions of fall characteristics and severity of AMS are shown in Table 3. The attributes of Japanese and foreign participants in relation to the risk of falls (Table 4) and AMS (Table 5) are summarized. In the final multivariable model, female sex and greater fatigue were associated with a higher risk of falls in both Japanese and foreign climbers (Table 6, upper section, and Figure 3A, B). Moreover, an interaction between nationality and age was observed such that advancing age was associated with a lower fall risk among foreign climbers but a higher fall risk among Japanese climbers (Table 6, upper section, and Figure 3C). For AMS, the final model derived age, an interaction between nationality and tour guide, and an interaction between nationality and fatigue that influenced AMS risk (Table 6, lower section, and Figure 3D–F). Younger age and greater fatigue were associated with a higher risk of AMS (Figure 3D, F), and foreign climbers without tour guides had a lower risk of AMS, whereas guide status was not associated with AMS risk among Japanese climbers (Figure 3E).
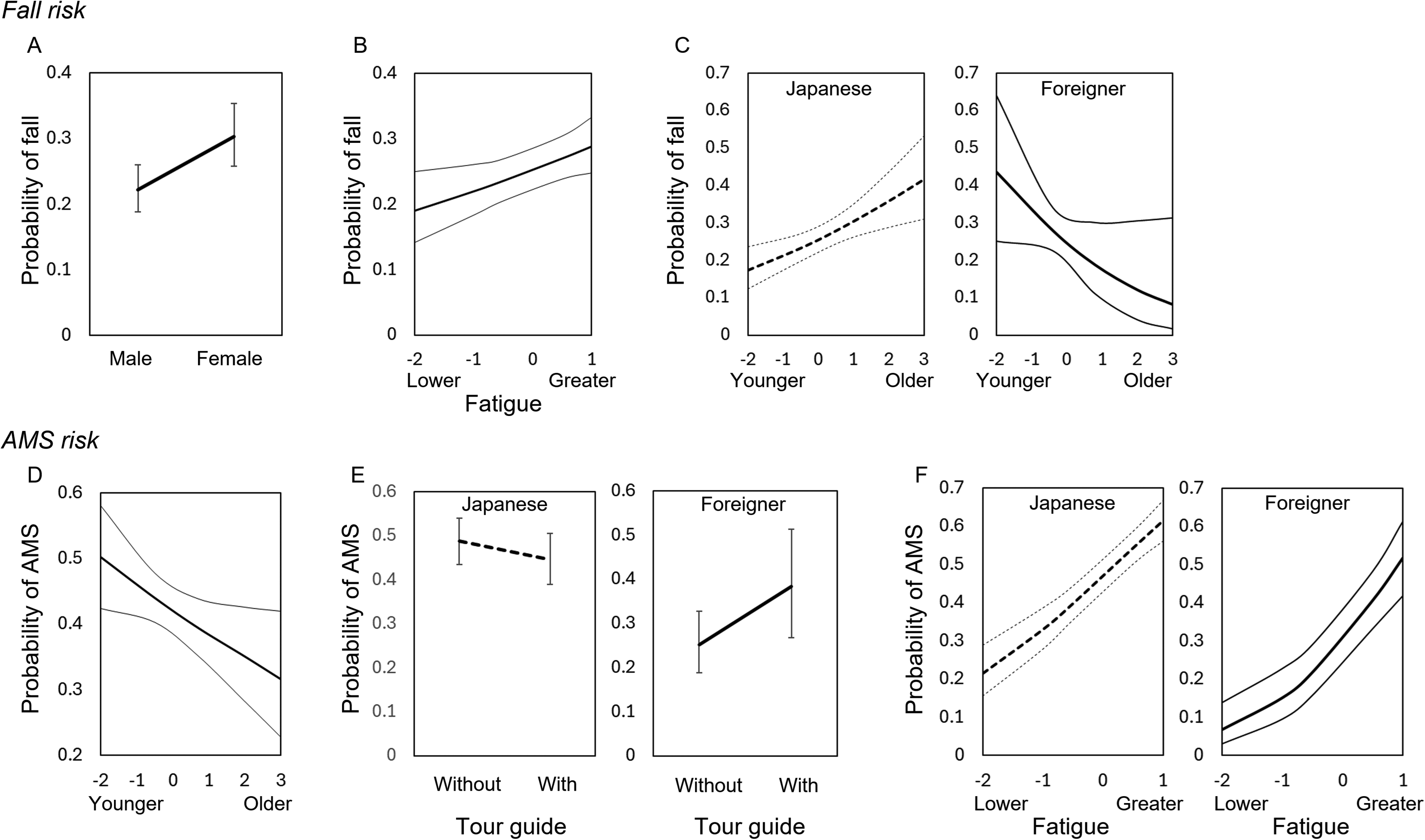
Significant predictors for fall (panels A–C) and AMS (panels D–F) risk. AMS, acute mountain sickness. In each panel, bold solid or dotted lines indicate mean of fall or AMS probability, and error bars (panels A and E) and thin solid or dotted lines indicate 95% confidential interval.
Summary of Fall Numbers, Fall Motions, and Fall-Related Injury Status and Severity of Acute Mountain Sickness (AMS) Among Japanese and Foreign Climbers.
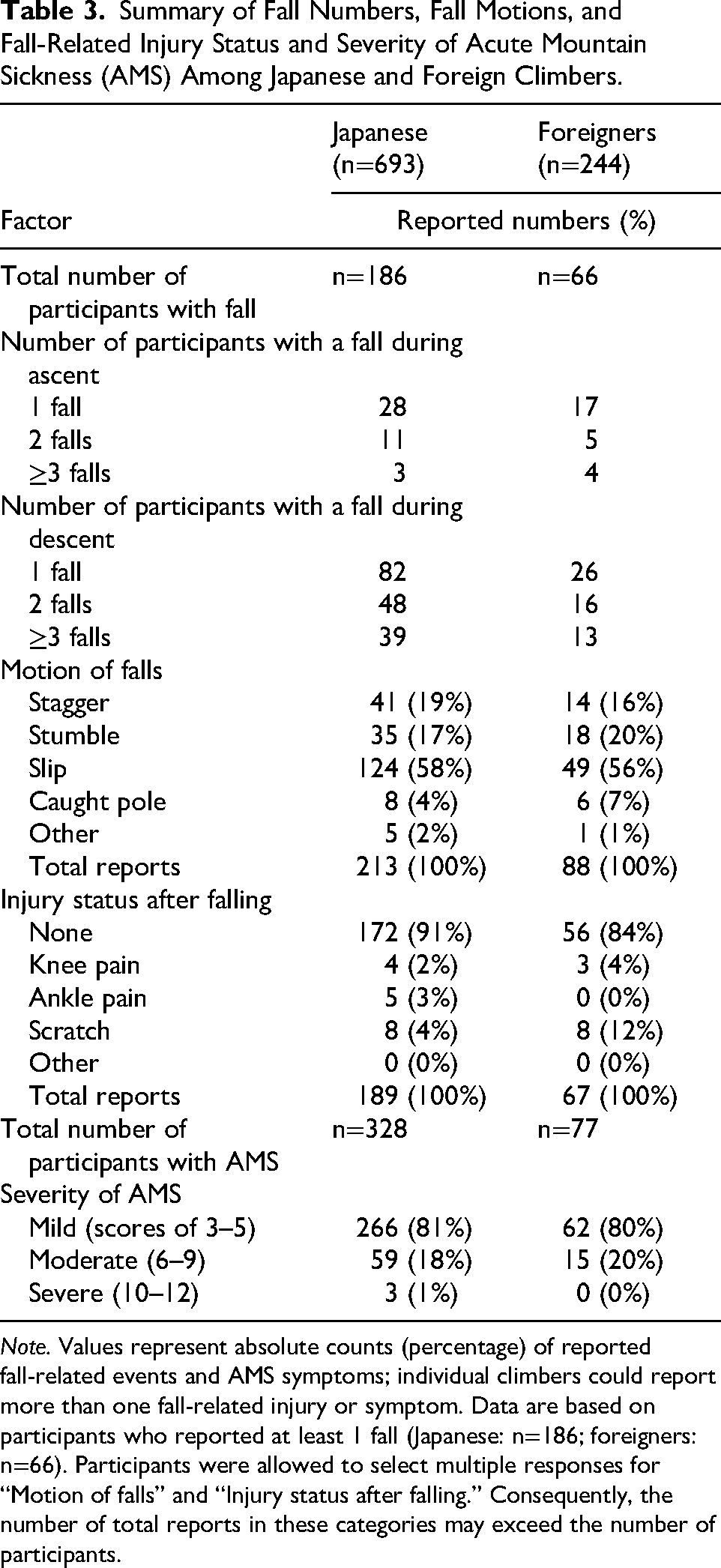
Note. Values represent absolute counts (percentage) of reported fall-related events and AMS symptoms; individual climbers could report more than one fall-related injury or symptom. Data are based on participants who reported at least 1 fall (Japanese: n=186; foreigners: n=66). Participants were allowed to select multiple responses for “Motion of falls” and “Injury status after falling.” Consequently, the number of total reports in these categories may exceed the number of participants.
Characteristics of the Surveyed Independent Variables in Fall-Related Factors Between Japanese and Foreign Climbers.
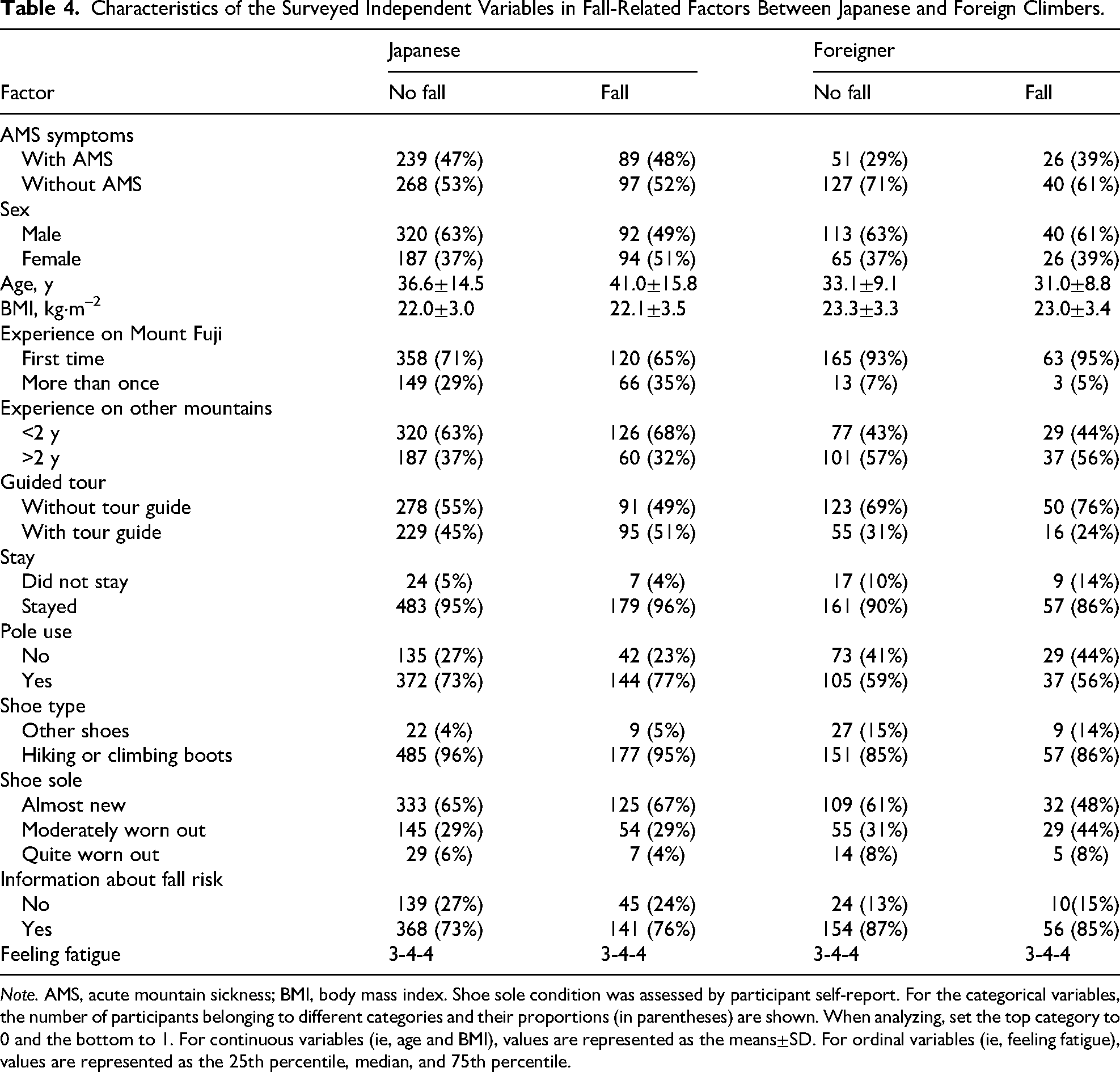
Note. AMS, acute mountain sickness; BMI, body mass index. Shoe sole condition was assessed by participant self-report. For the categorical variables, the number of participants belonging to different categories and their proportions (in parentheses) are shown. When analyzing, set the top category to 0 and the bottom to 1. For continuous variables (ie, age and BMI), values are represented as the means±SD. For ordinal variables (ie, feeling fatigue), values are represented as the 25th percentile, median, and 75th percentile.
Characteristics of the Surveyed Independent Variables in AMS-Related Factors Between Japanese and Foreign Climbers.
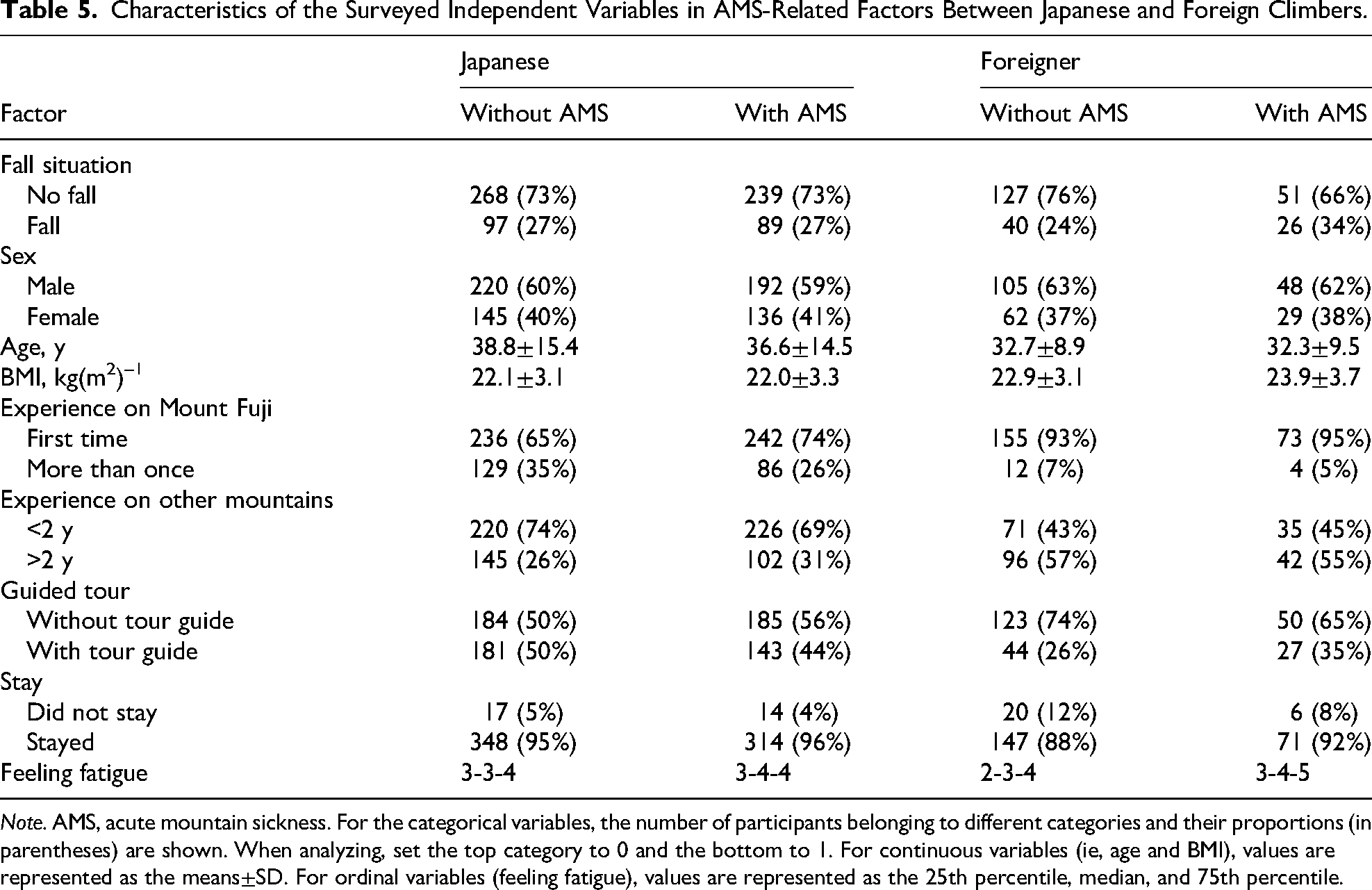
Note. AMS, acute mountain sickness. For the categorical variables, the number of participants belonging to different categories and their proportions (in parentheses) are shown. When analyzing, set the top category to 0 and the bottom to 1. For continuous variables (ie, age and BMI), values are represented as the means±SD. For ordinal variables (feeling fatigue), values are represented as the 25th percentile, median, and 75th percentile.
Summarized Results of Multiple Logistic Regression Analysis Using Backward Stepwise Method for the Risk of Falls and AMS.
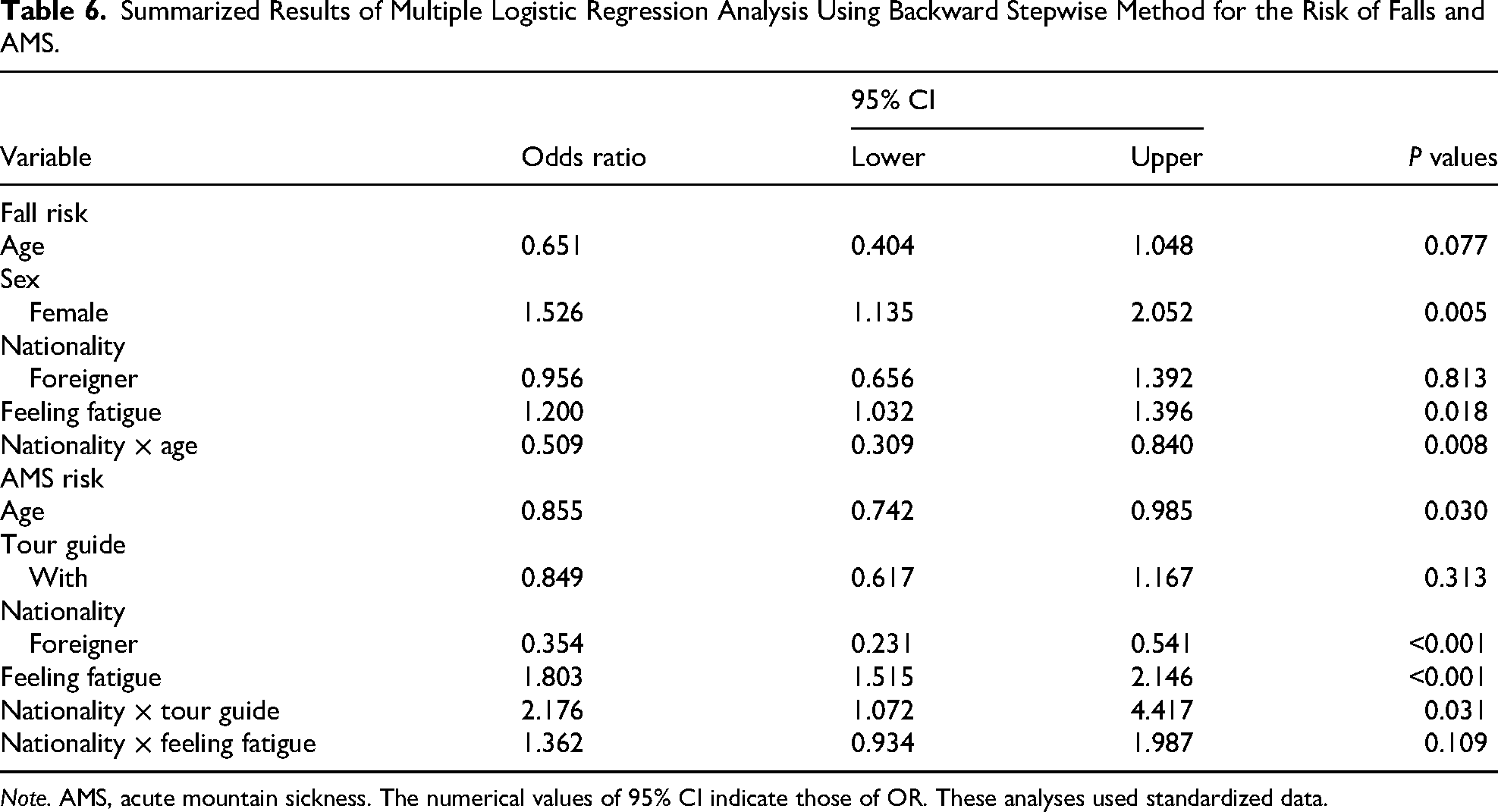
Note. AMS, acute mountain sickness. The numerical values of 95% CI indicate those of OR. These analyses used standardized data.
Among the 244 foreign climbers included in the main analysis, 19 were excluded from this subanalysis because of missing information on length of stay in Japan and jet lag duration; therefore, data from 225 foreign climbers were analyzed. There was no significant difference in the length of stay in Japan between climbers with (8±7 d, n=69) and without AMS (11±16 d, n=156; P=0.133). In contrast, foreign climbers with AMS had a greater time-zone difference (ie, jet lag) between their home country and Japan than those without AMS (7±7 h, n=69 with AMS vs 5±6 h, n=156 without AMS; P=0.020).
Discussion
The major findings of this study are as follows: 1) The prevalence of falls was nearly identical between Japanese and foreign climbers; 2) advancing age appears to increase fall risks among Japanese climbers, whereas younger age was associated with a higher fall risk among foreign climbers; 3) the prevalence of AMS was significantly lower among foreign climbers than among Japanese climbers; and 4) foreign climbers without guides had a lower risk of AMS, whereas guide status was not associated with AMS risk among Japanese climbers. Although sex and age are not modifiable, they may be useful for identifying climbers at higher risk and for guiding targeted preventive strategies across ethnic groups.
The higher risk of falls for female climbers among both Japanese and foreign participants (P=0.005; see Table 6 and Figure 3A) is consistent with previous studies on Mount Fuji.4,5 Reduced dynamic stability after prolonged eccentric muscle contractions during downhill walking, 24 which tends to be lower in females than in males 25 may partly explain this finding.
Higher levels of self-reported fatigue were associated with an increased risk of falls in both Japanese and foreign climbers (Figure 3B). This indicates that the association between fatigue and fall risk was broadly similar across groups. Both mental 11 and physical 10 fatigue have been recognized as risk factors for slip-induced falls, supporting our findings.
Our finding that advancing age increased fall risk among Japanese climbers is consistent with previous work showing that advancing age and failure to reach the summit were associated with increased rescue requirements on Denali. 26 However, the reason that older foreign climbers have a lower fall risk remains unclear. One possible explanation is that traveling overseas to climb Mount Fuji requires substantial preparation (eg, time, financial cost, and physical training), which may lead to a self-selection of older foreign climbers who are more cautious, physically prepared, and potentially more experienced or skilled.
The reasons for the different prevalence of AMS between Japanese (47%) and foreign climbers (32%) remains unclear, but factors not assessed in this study, such as the use of AMS prophylactic medication, 2 prior history of experience of headache/AMS, or the effects of rapid ascent 27 may partly contribute to this observed difference. Although advancing age was associated with a lower risk of AMS in both groups (P=0.03; see Table 6 and Figure 3D), the effect of age on AMS risk remains controversial in the literature. Several studies have reported a higher risk of AMS among young people,28–30 whereas others have identified older age as a risk factor.19,31 Conversely, other studies have found no significant association between age and AMS prevalence.20,27,32,33 There are several explanations for our finding. Rapid ascent is a well-established risk factor for AMS.12,13,27 During mountain trekking, oxygen consumption reached ∼80% of maximal oxygen uptake in older adults. 34 Aerobic capacity decreases with age,35,36 which may limit their ascent rate. In contrast, higher aerobic capacity in younger climbers could enable quicker ascent, thereby increasing their AMS risk. Thus, at least in this study, the lower AMS risk among older climbers may be explained by slower ascent.
Guided tour was not associated with AMS risk among Japanese climbers, but foreign climbers without guides had a lower prevalence of AMS (P=0.031; see Table 6 and Figure 3E). Because awareness of AMS risk factors, preventive strategies, and early symptoms may help reduce the likelihood of developing AMS among climbers,27,37,38 this finding remains controversial. There are several possible explanations for these findings. First, there are ∼200 Japanese tour guides on Mount Fuji, some of whom speak limited English, but none are native English speakers or speak other languages (except Japanese and English). In this study, 43% of the foreign climbers were native English speakers. Therefore, some foreign climbers may struggle to claim their individual physical conditions in English or misinterpret the English spoken by Japanese tour guides for reducing the risk of AMS. Another possible explanation is related to individual walking speeds. The preferred walking speed on rough terrain varied among individuals and was often slower than the speed that minimizes energy expenditure. 39 If climbers in the guided groups were required to walk at a pace that was different from their natural rhythm, possibly because of miscommunication or misunderstanding, this could have increased their physical exertion, ultimately leading to a higher prevalence of AMS. Additionally, climbers with less experience may be more likely to participate in guided tours, meaning that guide use may partly reflect differences in experience level rather than a direct effect of guide presence on AMS risk.
An interaction between nationality and fatigue was observed, with foreign climbers appearing more sensitive to AMS risk in response to fatigue (Figure 3F). One possible explanation is that the Lake Louise Scoring System for assessing AMS includes the item of “fatigue and/or weakness” as one of its criteria. 22 Thus, the climber's responses to the Lake Louise Scoring System questionnaire and their self-reported “subjective fatigue” may have overlapped, potentially leading to confounding results. Notably, a previous review recommended limiting altitude gain to no more than 500 m·d–1 to reduce the risk of AMS. 40 However, most climbers in this study gained ∼1500 m during the course of a single overnight stay. Consequently, ∼80% of climbers in this study experienced mild AMS (Table 3). Therefore, the current findings should be interpreted in the context of mild AMS cases.
Our findings suggest that greater time-zone differences may be associated with an increased risk of AMS. Jet lag gradually resolves over 4 to 6 d, but recovery time is prolonged with a greater number of time zones crossed. 41 Notably, jet lag symptoms—including headache, sleep disturbances, daytime fatigue, and gastrointestinal discomfort—closely resemble those of AMS, potentially compounding climbers’ perceived symptoms. However, these associations should be interpreted with caution. First, the observed findings that people with AMS had a greater jet lag time than those without AMS may be coincidental rather than causal. Second, our dataset did not include sufficient detail regarding travel schedules, direction of travel, or acclimatization behaviors to determine a specific recommendation (eg, number of days per time zone crossed). Future studies specifically designed to evaluate the interaction between jet lag recovery and altitude exposure are warranted to establish practical guidelines for foreign climbers.
Although this analysis treated AMS and falls as separate dependent outcomes, each model included the other condition as an independent variable. This approach allowed examination of potential interactions. No direct association between AMS and fall occurrence was identified, indicating that these risks may operate through distinct physiologic and behavioral mechanisms.
Limitations
Several factors limited the interpretation of our results. First, the sample size, particularly for foreign climbers, was limited. Future studies with larger samples are needed to confirm these findings. Second, data were collected only from descending climbers between 0800 and 1200 h; therefore, climbers who descended earlier or later, including those with severe injuries or AMS or those rescued by professional teams, may not have been captured. Additionally, because we could not track the number of climbers who declined to participate, nonresponse bias cannot be excluded. Third, falls and AMS symptoms were assessed retrospectively by questionnaire, which may introduce recall bias and limits the ability to determine the precise timing of events. Fourth, although the questionnaire was available in Japanese and English, this may not have fully captured responses from climbers whose primary language was neither Japanese nor English, potentially leading to underrepresentation of some foreign climbers. Finally, the limited number of questionnaire items prevented evaluation other factors related to fall risk, such as muscle strength and balance ability42,43 or individual maximum gait speed. 44 Similarly, AMS-related factors, including a history of previous AMS, migraine,27,45–47 sleep disturbances, detailed climbing schedule (eg, rapid vs slow ascent),8,12,13,27 and the effects of jet lag on foreign climbers, 48 which have been pointed out previously, were not evaluated. Future studies incorporating these parameters are warranted.
Conclusions
These findings highlight the importance of targeted preventive guidance to reduce fall risk among female climbers, those experiencing greater fatigue regardless of ethnicity, and older Japanese climbers as well as to reduce AMS risk among foreign climbers participating in guided tours on Mount Fuji. However, these interpretations should be considered within the limitations of this questionnaire-based survey.
Footnotes
Acknowledgments
The authors thank all participants who took their time and effort to contribute to this study. The authors thank Chieko Takiguchi, Mie Matsuyama, and Yasuhiro Tsukada for their technical assistance in collecting the data.
Author Contribution(s)
Financial/Material Support
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Japan Society for the Promotion of Science, (grant number 20K12450).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.