
Abstract
Introduction
Musculoskeletal injuries from rock climbing are increasing as participation rates rise. It is important to understand climbers’ injury treatment decisions and trust in providers to improve communication, education, and care pathways. The purpose of this study was to examine healthcare-seeking behaviors and healthcare-provider trust among rock climbers following injury.
Methods
A cross-sectional survey was distributed online via social media, email, and flyers. In total, 145 rock climbers who sustained a climbing-related musculoskeletal injury completed the survey. Outcomes included type of provider seen, reasons for provider choice or delay in care, and ratings of trust and satisfaction. Free-text comments were analyzed for themes.
Results
Climbers commonly sought care from physical or occupational therapists (PT/OTs; 31.7%), followed by specialists (24.1%) and primary care providers (PCPs; 16.6%, P<0.001). PT/OTs were more likely to be accessed virtually and through peer recommendation, whereas PCP visits often were assigned by the health system. Delays in care were common (68.3%) and attributed to cost, time constraints, and confidence in self-treatment. Pulley injuries were associated with delayed care and reliance on self-treatment. Trust/satisfaction ratings were highest for PT/OTs (median trust 9, satisfaction 9) and specialists (trust 9, satisfaction 8) compared with PCPs (trust 6, satisfaction 6; P=0.02 and P=0.002, respectively). Free-text responses emphasized the importance of climbing-specific expertise and individualized treatment plans.
Conclusions
Trust and satisfaction with healthcare providers vary based on sport-specific knowledge and treatment recommendations. Delayed care and self-management are common, especially for finger injuries. PT/OTs often serve as both initial and final providers.
Keywords
Introduction
Rock climbing has gained significant popularity over the past decade, highlighted by its debut in the Tokyo 2020 Olympic Games. Participation rates have surpassed 8 million in the United States, driven in part by a 76% increase in indoor climbing gyms from 2014 to 2023. 1 Climbing encompasses a range of disciplines, including outdoor and indoor climbing, lead climbing, top-rope climbing, bouldering, and speed climbing. Although climbing offers substantial physical and mental health benefits,2,3 it also carries a risk of musculoskeletal injury. 4
Recent studies have documented a rising incidence of climbing injuries, with emergency department visits for climbing-related injuries estimated to have doubled between 2010 and 2019.5,6 Although these visits likely represent more severe injuries, climbers also commonly sustain injuries managed outside of the emergency department, such as ankle sprains and rotator cuff tears and climbing-specific injuries involving the digital pulleys and lumbrical muscles.5,6 The unique nature of finger injuries in climbers poses challenges both for injured athletes seeking effective treatment and for healthcare providers who may lack sport-specific expertise.7,8 Indeed, many climbers with chronic injuries avoid medical treatment, citing mistrust of providers due to lack of climbing-specific knowledge. 9
Injured climbers may seek care from a variety of healthcare providers, including primary care providers, orthopedic surgeons, sports medicine physicians, and physical therapists, each with differing levels of familiarity with climbing-related injuries. However, little is known about how climbers navigate these options after injury or how their perceptions of provider expertise influence treatment choices. Understanding the treatment choices rock climbers make after injury, as well as their trust in healthcare providers, may improve patient communication, target educational efforts, and inform effective treatment pathways.
In the United States, some climbers seek care through an emerging network of clinicians who explicitly market climbing-specific rehabilitation services. These include physical therapy practices, online educational platforms, telehealth offerings, and provider directories aimed at helping climbers find clinicians with experience treating climbing-related injuries. As a result, injured climbers may encounter physical therapists who present themselves not only as rehabilitation providers but also as climbing-informed specialists.
The purpose of this study was to explore treatment preferences among adult rock climbers following musculoskeletal injury. We aimed to describe the types of healthcare providers rock climbers seek after injury and their levels of trust and satisfaction with those providers. Given the visibility of climbing-specific physical therapy services, we hypothesized that rock climbers would show greater preference for, and trust in, physical therapists than physicians.
Methods
This was a cross-sectional, anonymous survey assessing injury treatment preferences following a climbing-related musculoskeletal injury hosted electronically on REDCap. 10 Eligible participants were self-identified rock climbers who were ≥18 y old, English speaking, and had sustained a climbing-related musculoskeletal injury. The survey queried demographic information and climbing experience. For their most recent or most significant injury, respondents were asked about the nature of the injury, whether they sought professional advice, and their trust in and satisfaction with that advice. Respondents were given the option to provide free-text opinions regarding which types of providers rock climbers should seek after injury.
Participants were recruited between December 2023 and April 2024 via email, social media (Instagram), and flyer distribution by 3 investigators (DCS, TR, and JK) at multiple indoor climbing gyms and outdoor locations across the United States (ie, California, Nevada, and Florida). The study was deemed exempt by the University of California, Davis Institutional Review Board.
To establish a recruitment goal, an a priori power analysis was performed using a χ2 test comparing frequency of consultation across 5 categories of healthcare providers. This analysis dictated a sample size of 133 participants to achieve 80% power at a significance level of 0.05 with an effect size of 30%.
Analysis
Data were summarized using descriptive statistics. For categorical data, χ2 tests were used, with Fisher exact tests for post-hoc pairwise comparisons using a Bonferroni adjustment. For data on a numerical rating scale (0–10), group differences were tested using Kruskal-Wallis tests with post-hoc pairwise Mann-Whitney U tests and a Bonferroni adjustment. Providers were grouped into physical or occupational therapist (PT/OT), primary care provider (PCP), orthopedic surgeon or sports medicine physician (specialist), and other for this analysis given low counts in certain groups. Prior to Bonferroni adjustment, the significance level (alpha) was set at 0.05. Variables not directly related to the prespecified study aims were summarized descriptively to characterize the cohort but were not subjected to hypothesis testing.
All free-text comments about provider experience were combined and analyzed using latent Dirichlet allocation, an automated method for identifying themes in text. Three topics were extracted after cleaning and filtering text using a custom stop-word list that included common climbing-specific terms. For each topic, the top 8 representative words (tokens) were inspected alongside exemplar responses to verify thematic coherence. Latent Dirichlet allocation was performed in Python using the scikit-learn LatentDirichletAllocation package. The authors used ChatGPT-4o to improve the clarity of the writing. The authors take full responsibility for the content of this publication.
Results
Demographic and climbing characteristics of respondents are presented in Table 1, with complete survey responses available in online Supplemental Table 1.
Summary of Respondent Demographics, Climbing History, and Injury Type.
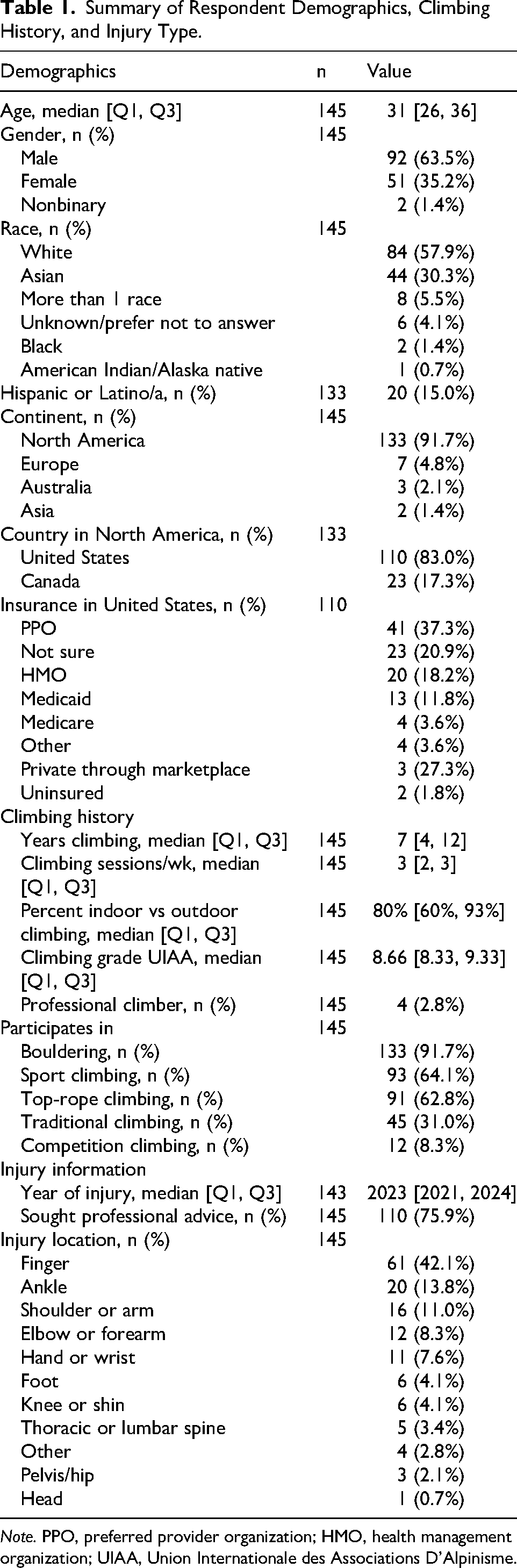
Note. PPO, preferred provider organization; HMO, health management organization; UIAA, Union Internationale des Associations D’Alpinisme.
Which Healthcare Providers Do Rock Climbers Seek After Injury?
Provider type. Climbers were more likely to see PT/OTs (46 of 110; 31.7%) compared with specialists (35 of 110; 24.1%) or PCPs (24 of 110; 16.6%; P<0.001).
Evaluation setting. The initial evaluation setting differed across providers (P<0.001), with in-person office visits most common overall. However, PT/OT visits were more likely to occur virtually (8 of 46; 17.4%) compared with PCP or specialist visits (0%), which more frequently occurred in urgent care settings (8 of 24 [33.3%] and 6 of 35 [17.1%], respectively). Evaluation setting also varied by injury type (see online Supplemental Table 3). Among the 4 most common injuries, virtual consultation was used only for single pulley strains or partial tears (2 of 19; 10.5%). Ankle fractures were managed through the emergency department (2 of 9; 22.2%), urgent care (3 of 9; 33.3%), or in-person office visits (4 of 9; 44.4%), whereas single pulley ruptures were seen in the emergency department (2 of 8; 25.0%) or in-person office visits (6 of 8; 75.0%).
Reason for choosing a provider. Convenience was a common reason for seeing PCPs (14 of 24; 48.3%) compared with PT/OTs (7 of 45; 15.2%) and specialists (5 of 35; 14.3%; P<0.001). Respondents were more likely to see PCPs because appointments were scheduled by the health system (13 of 24; 54.2%; P<0.001), whereas PT/OTs were more often chosen due to referral from another climber (20 of 46; 43.5%; P<0.001).
Reasons for delay. Those who delayed presentation to a healthcare professional (99 of 145; 68.3%) cited cost, time constraints, and confidence in self-treatment as reasons, with no differences observed between providers. Delays due to confidence in self-treatment were common among patients with pulley strains (20 of 35; 57.1%). Use of online resources was highest among patients with pulley strains (26 of 35; 74.3%), with YouTube used by 17 of 35 respondents (48.6%). There were no differences in rates of delayed care between male and female patients (see online Supplemental Table 2).
Provider specialization and treatment. PT/OTs (32 of 46; 69.6%) more commonly specialized in treating rock climbing injuries than specialists (4 of 35; 11.4%) or PCPs (1 of 24; 4.2%; P<0.001). Treatment recommendations varied by provider type (P<0.001). PT/OTs most often prescribed home rehabilitation programs (32 of 46; 69.6%), whereas PCPs most often advised absence from climbing alone (8 of 24; 33.3%) or referred to a therapist (7 of 24; 29.2%). Specialists were divided among home rehabilitation (6 of 35; 17.1%), referral to a therapist (6 of 35; 17.1%), climbing absence alone (11 of 35; 31.4%), and surgery (10 of 35; 28.6%). Respondents who saw PT/OTs were less likely to have a second consultation (7 of 45; 15.2%; P<0.001) compared with those who saw PCPs (16 of 24; 66.7%) or specialists (22 of 35; 62.9%), who commonly referred patients to therapy.
What Is the Level of Trust and Satisfaction with Healthcare Providers?
Overall satisfaction. When seeking professional consultation (n=110), satisfaction (0–10) with PT/OTs (median 9; interquartile range [IQR] 7.25–10; P=0.002) was higher than with PCPs (median 6; IQR 4.5–7.25), whereas there was no difference compared with specialists (median 8; IQR 6–9). Trust scores (0–10) also differed (P=0.02), with PT/OTs being rated higher (median 9; IQR 7.25–10) than PCPs (median 6; IQR 5–8.25) but not specialists (median 9; IQR 7–10). Overall satisfaction at the end of treatment (P=0.07) and self-reported adherence to treatment (P=0.56) did not differ by provider type. There also was no difference in the likelihood of changing providers if respondents perceived that the provider did not understand the demands of rock climbing (P=0.09).
Satisfaction by diagnosis. Across the 4 most common diagnoses, initial satisfaction (0–10) differed by injury type (P=0.03), with patients with pulley ruptures (median 8; IQR 8–8.5) reporting higher satisfaction than those with ankle sprains (median 7; IQR 2.5–7, left skewed) but not differing from patients with pulley strains (median 8; IQR 6.5–9) or ankle fractures (median 8; IQR 7–9). Trust with providers, adherence to treatment, and end-of-treatment satisfaction did not differ across diagnoses (all P≥0.38).
Opinions on Treatment Decisions
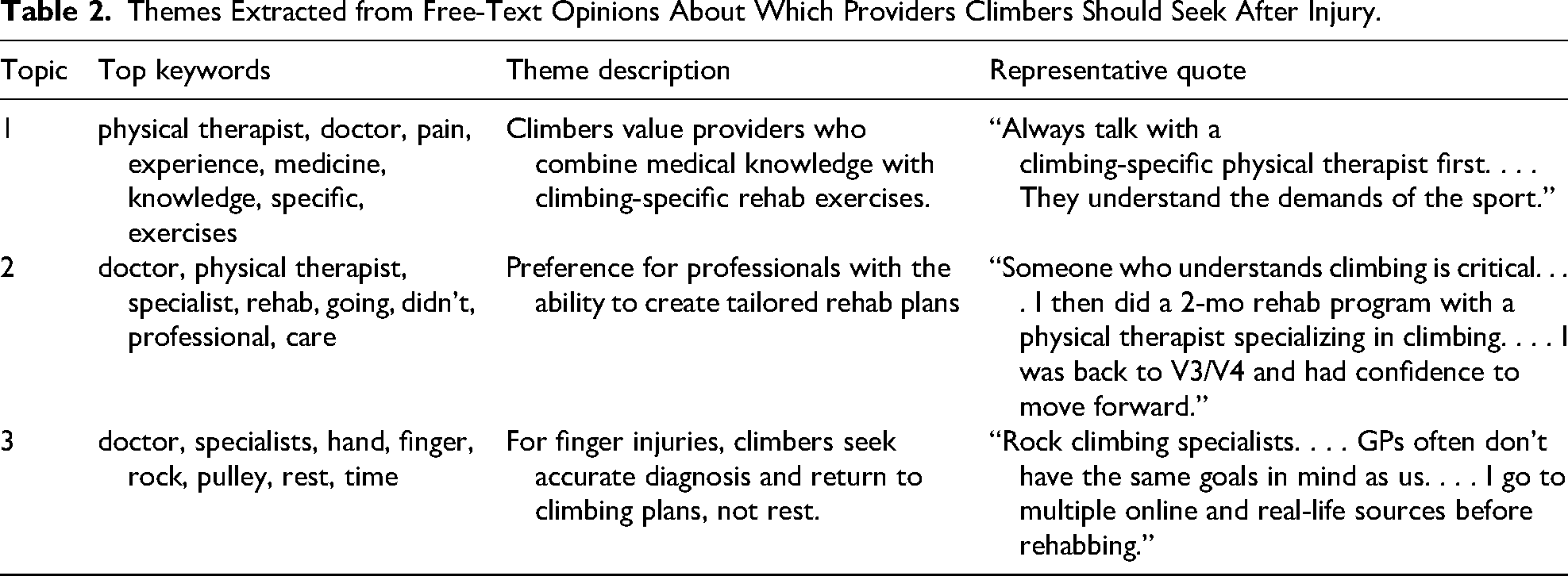
Analysis of 75 free-text comments regarding whom climbers should see after injury revealed overlapping themes, emphasizing a preference for providers with climbing-specific knowledge and treatment expertise, able to provide tailored return-to-climbing plans rather than advising rest alone (Table 2).
Themes Extracted from Free-Text Opinions About Which Providers Climbers Should Seek After Injury.
Discussion
This study provides insight into the healthcare-seeking behaviors and treatment preferences of rock climbers following injury. Building on prior findings that climbers are reluctant to consult healthcare providers after injury,9,11 this study demonstrates that when climbers do seek care, they consult a range of providers, often influenced by convenience or health system referrals. Further, climbers show a clear preference for and greater trust in providers with sport-specific knowledge. These findings have important implications for musculoskeletal care delivery in this growing athletic population.
Delays in Treatment
Nearly 70% of climbers delayed seeking care, consistent with prior findings in climbers and other recreational athlete populations.9,11–13 A prior survey of climbers after injury found that only 36% sought formal medical care. 11 In our study, reasons for delays included cost, time constraints, and confidence in self-treatment. Gender also may play a role because several studies show that females seek care sooner than males.9,14 For example, in a study of adolescent climbers, male climbers took an average of 163 d to seek care after injury compared with 92 d for females. 14 Although we did not observe significant gender differences in rates of delayed care, we did not specifically assess time to presentation, which may account for this discrepancy. Patients with pulley injuries were particularly prone to delayed care and self-management, with 74% of climbers turning primarily to online resources such as YouTube. This finding is consistent with a previous study reporting that 70% of climbers consulted some form of online medical information, with YouTube being the most common platform. 15 While this reflects the autonomy and digital engagement of the climbing community, it also highlights a gap in reliable sport-specific medical guidance. The issue may be less of the availability of healthcare in general and more whether climbers perceive available care as relevant to their injury. This may explain why prior the investigation showed that having health insurance or a PCP was not associated with seeking medical care after climbing injuries. 13
Treatment Preferences After Injury
Climbers sought care from a variety of providers, but routing was fragmented and driven largely by logistical considerations. In this sample, PT/OTs frequently served as both the entry point and endpoint of care and often managed injuries without further referral. Convenience was a major factor in choosing PCPs, with nearly half of visits selected for this reason and more than half assigned by the health system. In contrast, referrals to PT/OTs often were guided by peer recommendation, demonstrating how trust within the climbing community influences care. Care patterns also appeared to vary by injury type. More acute lower extremity injuries, such as ankle fractures and sprains, were commonly managed through the emergency department or urgent care, whereas pulley strains and tears more often were evaluated in office settings or virtually. Despite similar sample demographics and injury patterns, McDonald et al found that climbers most frequently presented to PCPs (27.9 vs 16.6% in this study) followed by the emergency department (19.9 vs 7.6%). 11 These differences suggest potential regional, temporal, and injury-specific heterogeneity in care patterns.
Trust and Satisfaction
Climbers demonstrated greater trust and satisfaction with PT/OTs and specialists, including sports medicine physicians and orthopedic surgeons. In our cohort, median trust was 9 of 10 (90%) for both PT/OTs and specialists compared with 6 of 10 (60%) for PCPs. By comparison, Kanter et al reported mean trust in one's own physician of 20.5 of 25 (82%) in a national US sample, whereas trust in the medical profession overall was 15.4 of 25 (62%), suggesting that the trust observed here for PT/OTs and specialists was high, whereas trust in PCPs was closer to broader published benchmarks. 16 Similarly, Ludvigsson and Enthoven found that patients assessed by physical therapists reported higher confidence in their provider's ability to evaluate musculoskeletal disorders than those assessed by general practitioners, which may help explain the relatively higher trust ratings for PT/OTs in our study. 17
Prior climbing literature from Norway also has suggested that perceived provider unfamiliarity with climbing injuries may be a barrier to care, particularly for chronic injuries. 9 In that study, 24% of climbers with a chronic injury who did not seek healthcare reported that they did not think health professionals knew enough about climbing-related injuries. 9 Our findings suggest that climbers may respond to this concern by actively seeking providers perceived to have climbing-specific expertise. Among respondents who saw PT/OTs, nearly 70% reported that their provider specialized in treating climbers, and PT/OTs were more often selected through referral from another climber, coach, or friend. However, our survey did not directly determine whether providers were chosen primarily due to their professional designation or because of their climbing-specific reputation, online presence, or community referral. Thus, the higher proportion of PT/OTs reported to have climbing-specific knowledge likely reflects, at least in part, patient selection of known climbing specialists rather than a baseline difference in climbing knowledge across the profession. In contrast, PCPs were more often selected because the appointment was assigned by the health system or dictated by insurance, suggesting that access pathways and insurance structure also influence provider choice. Respondents highly valued sport-specific knowledge, particularly the ability to provide return-to-climbing plans rather than advising rest alone, which is consistent with current management principles for many tendon and pulley injuries.18–20
Limitations
Limitations include the retrospective and self-reported nature of the survey, which may introduce recall bias. Although the survey was shared across diverse climbing settings and online modalities, respondents were largely from the United States, so findings should be interpreted in the context of its healthcare system. Although insurance status may influence access to care and provider choice, this study was not powered to evaluate outcomes stratified by both insurance type and provider category. Future studies designed for this purpose are warranted. Climbers who are engaged online may have been more likely to participate, which could limit generalizability to the broader population of climbers. Notably, most reported injuries did not require surgical treatment, and therefore, trust and satisfaction scores may not reflect preferences in operative cases.
Due to the categorical design of the survey, certain responses may have been underreported or may have introduced bias. For example, when asking respondents about their treatment course, an “other” category was available that allowed respondents to enter a free-text response, but this was only used in 4.1% of responses. Treatments such as corticosteroid injections, which were not presented as response categories, may have been underreported. Finally, differences in injury type between provider groups were not controlled for, limiting direct comparisons and analysis of acute vs chronic conditions.
Conclusions
Climbers prioritize provider expertise in climbing-related injuries and demonstrate greater trust in those with specialized knowledge. Delays in seeking care are common and are driven primarily by cost, time constraints, and confidence in self-treatment, particularly for finger injuries. These findings suggest a need for more accessible, sport-informed educational resources and greater awareness of climbing-related injury management across healthcare providers.
Supplemental Material
sj-docx-1-wem-10.1177_10806032261447193 - Supplemental material for Sport-Specific Expertise Drives Provider Choice Among Injured Rock Climbers
Supplemental material, sj-docx-1-wem-10.1177_10806032261447193 for Sport-Specific Expertise Drives Provider Choice Among Injured Rock Climbers by Daniel C. Santana, MD, MS, Taylor Rakauskas, MS, Jack Kornfeld, MD, and Zachary C. Lum, DO in Wilderness & Environmental Medicine
Supplemental Material
sj-docx-2-wem-10.1177_10806032261447193 - Supplemental material for Sport-Specific Expertise Drives Provider Choice Among Injured Rock Climbers
Supplemental material, sj-docx-2-wem-10.1177_10806032261447193 for Sport-Specific Expertise Drives Provider Choice Among Injured Rock Climbers by Daniel C. Santana, MD, MS, Taylor Rakauskas, MS, Jack Kornfeld, MD, and Zachary C. Lum, DO in Wilderness & Environmental Medicine
Supplemental Material
sj-docx-3-wem-10.1177_10806032261447193 - Supplemental material for Sport-Specific Expertise Drives Provider Choice Among Injured Rock Climbers
Supplemental material, sj-docx-3-wem-10.1177_10806032261447193 for Sport-Specific Expertise Drives Provider Choice Among Injured Rock Climbers by Daniel C. Santana, MD, MS, Taylor Rakauskas, MS, Jack Kornfeld, MD, and Zachary C. Lum, DO in Wilderness & Environmental Medicine
Supplemental Material
sj-docx-4-wem-10.1177_10806032261447193 - Supplemental material for Sport-Specific Expertise Drives Provider Choice Among Injured Rock Climbers
Supplemental material, sj-docx-4-wem-10.1177_10806032261447193 for Sport-Specific Expertise Drives Provider Choice Among Injured Rock Climbers by Daniel C. Santana, MD, MS, Taylor Rakauskas, MS, Jack Kornfeld, MD, and Zachary C. Lum, DO in Wilderness & Environmental Medicine
Footnotes
Ethical Considerations
The study was deemed exempt by the University of California, Davis Institutional Review Board (Approval No. 2237056).
Consent to Participate
Participants were provided with a letter of information prior to the survey and consented to participate by proceeding to complete the survey.
Financial/Material Support
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Contribution(s)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.