
Abstract
Introduction
Scorpion sting-induced Kounis syndrome (Ks) is a rare and underrecognized form of allergic acute coronary syndrome. Although scorpion envenomation is a significant cause of morbidity in endemic regions, its association with Ks has been infrequently reported. This study aimed to describe the clinical characteristics, management, and outcomes of venom-induced Ks.
Methods
Following institutional ethical approval, medical records of 175 patients admitted with scorpion envenomation between January 2014 and March 2024 were retrospectively reviewed. Of these patients, 34 met predefined inclusion criteria. Demographic data, clinical features, cardiac investigations, treatments, intensive care unit course, and short-term outcomes were analyzed. Group comparisons and odds ratios with 95% confidence intervals were calculated using appropriate statistical methods.
Results
The cohort comprised 21 children and 13 adults, with a median age of 9 y (interquartile range 4–52). Chest pain (88.2%) and generalized erythema or urticaria (94.1%) were the most frequent presenting features. Pediatric patients exhibited significantly higher rates of cardiac involvement, including left ventricular ejection fraction reduction, hyperlactatemia, clinical need for prazosin, and need for inotropic support. Severe cardiac involvement occurred more frequently in children than in adults (90 vs 23%; odds ratio 31.7, 95% CI 4.52–221.73, P<0.001). Coronary angiography, performed selectively, revealed no significant obstructive lesions in most patients. No 30-d mortality was observed.
Conclusions
Pediatric patients demonstrated a more severe pattern of cardiac involvement than adults, suggesting an age-dependent clinical phenotype following scorpion envenomation. Given the limited sample size, these findings should be interpreted with caution and warrant validation in larger multicenter cohorts.
Keywords
Introduction
Kounis syndrome (Ks) represents a critical intersection between systemic hypersensitivity reactions and acute coronary syndromes, reflecting a complex interplay between allergic mediators and cardiovascular dysfunction. Ks is classified into 4 variants. Type 1 involves allergic coronary vasospasm in patients with angiographically normal coronary arteries and may present as myocardial infarction with nonobstructive coronary arteries. Type 2 occurs in patients with preexisting atherosclerotic disease, in whom an allergic trigger may cause vasospasm or plaque rupture leading to acute myocardial infarction. Type 3 is related to coronary stents and manifests as allergic stent thrombosis (3a) or restenosis (3b). Type 4, a recently proposed variant, refers to allergic thrombosis of coronary artery bypass grafts. Although uncommon, Ks presents considerable diagnostic and therapeutic challenges, particularly when precipitated by unconventional triggers such as venomous envenomation.1–4
Among venom-induced hypersensitivity reactions, scorpion sting-associated Ks is exceptionally rare yet of pathophysiologic significant. Scorpion species endemic to the Middle East and North Africa produce α-toxins that induce prolonged neuronal depolarization, resulting in a catecholamine surge and a systemic inflammatory response. This dual mechanism can precipitate coronary vasospasm, myocardial ischemia, and myocarditis, often mimicking acute coronary syndromes. Despite these mechanistic insights, clinical data on scorpion envenomation-related Ks remain limited, increasing the risk of misdiagnosis and suboptimal management in endemic regions.5,6 In particular, Androctonus crassicauda is recognized as one of the most medically significant scorpion species in this region.
Given this paucity of data, we present a case series of patients with Ks following scorpion envenomation. Assessment was based on clinical symptoms, electrocardiography, and cardiac biomarkers, whereas advanced cardiac imaging was performed in selected patients to support the diagnosis and enable type differentiation.
Methods
Study Design and Setting
This retrospective study was conducted at a tertiary care referral center between January 2014 and March 2024. During the study period, 175 patients with scorpion envenomation were admitted, most of whom were referred from peripheral hospitals due to severe systemic manifestations. Among these, 34 patients fulfilled the diagnostic criteria for scorpion sting-associated Ks and were included in the final analysis. Given the institution's role as a tertiary referral center, a higher proportion of complicated envenomation cases was observed compared with primary healthcare settings.
Diagnostic Criteria, Classification, and Evaluation
Ks was established based on a confirmed history of scorpion sting accompanied by venom-induced allergic manifestations (ie, erythema, urticaria, and pruritus), together with the presence of at least 2 of the following 3 myocardial infarction-related criteria: 1) clinical ischemic symptoms (eg, chest pain or dyspnea), 2) newly developed electrocardiographic (ECG) abnormalities (eg, ST-segment elevation or depression or T-wave inversion), and 3) elevated cardiac biomarkers (eg, troponin) and/or evidence of ischemic or transient functional cardiac impairment on imaging modalities, including echocardiography, computed tomography angiography, or magnetic resonance angiography.
Scorpion envenomation was confirmed based on a detailed history obtained at admission, in which the sting event was directly reported by the patient or accompanying individual and supported by clinical findings consistent with envenomation. Due to the study's retrospective design, precise species-level identification was not possible. However, epidemiologic data indicate that A crassicauda is the most prevalent medically significant scorpion species in the region and is responsible for most of the severe envenomation cases.
To ensure diagnostic accuracy, all cases were reviewed and confirmed through a multidisciplinary assessment involving at least 2 specialist physicians. Pediatric cases were jointly evaluated by a pediatric intensive care specialist and a pediatric cardiologist, whereas adult cases were assessed by an anesthesiology and reanimation specialist in collaboration with a cardiologist.
Patients with a history of anaphylaxis or a preexisting active systemic allergic disease prior to the scorpion sting, those with concomitant systemic conditions potentially leading to secondary elevations in cardiac biomarkers, and those with insufficient medical records precluding diagnostic confirmation were excluded from the study. Disease severity and clinical course were classified using the Isbister-Bawaskar grading system for scorpion envenomation and the Ks classification for cardiac involvement.
All patients underwent transthoracic echocardiography to evaluate left ventricular function and regional wall motion abnormalities. In line with a diagnostic strategy prioritizing noninvasive approaches, coronary angiography was not considered mandatory; instead, it was performed selectively to aid Ks subtype differentiation and to assess underlying coronary anatomy when clinically indicated, particularly in adult patients with increased atherosclerotic risk.
Treatment Protocol
All patients received scorpion antivenom supplied by the Turkish Ministry of Health (Public Health General Directorate). Each 1 mL of the antivenom contains F(ab′)2 immunoglobulin fragments capable of neutralizing >100 LD50 of A crassicauda venom. The formulation includes a total protein content of <100 mg·mL-1, 3-methylphenol (m-Cresol) <3.5 mg·mL-1, and sodium chloride 85 to 95 mg·mL-1.
The standard administered dose was 1 ampoule (10 mL), independent of patient weight or age, in accordance with national treatment protocols. In addition to antivenom, patients received supportive therapy including antihistamines, corticosteroids, vasopressors, inotropes, and antihypertensive agents such as prazosin when clinically indicated.
Ethical Considerations
Ethical approval for this retrospective study was obtained from the local ethics committee (Approval No. 2024/06-5443). Informed consent was waived due to the retrospective design and anonymized nature of the data. The study was conducted in accordance with the principles of the Declaration of Helsinki.
Statistical Analyses
Categorical variables were expressed as counts and percentages and compared using the χ2 or Fisher's exact test as appropriate. Continuous variables were expressed as mean±SD or median (ie, interquartile range) depending on distribution and compared using the Mann-Whitney U test. A composite endpoint termed severe cardiac involvement was predefined as the presence of at least 1 of the following: 1) new-onset left ventricular ejection fraction reduction, 2) requirement for inotropic support, 3) hyperlactatemia (>4 mmol·L-1), or 4) administration of prazosin therapy. Odds ratios (ORs) with 95% confidence intervals (CIs) were calculated to estimate the strength of association between age group and outcomes. A 2-sided P value of <0.05 was considered statistically significant. Categorical variables were compared using Fisher's exact test due to small sample size and expected cell counts.
Results
The cohort of 34 patients demonstrated a wide age distribution, with a median age of 9 y (IQR 4–52; range 1–81). The study population included 21 children and 13 adults, with a slight female predominance (20 females vs 14 males). Chest pain was present in 30 of 34 patients (88.2%). Additional symptoms included generalized erythema or urticaria (94.1%), dyspnea (41.1%), abdominal discomfort including nausea or vomiting (58.8%), mild convulsion (8.8%), and priapism (8.8%). A localized hematoma at the sting site was observed in 1 patient. Detailed clinical, ECG, echocardiographic, and laboratory findings are summarized in Tables 1 and 2.
Demographic, Clinical, and Outcome Characteristics of the Study Population Patients (N=34).
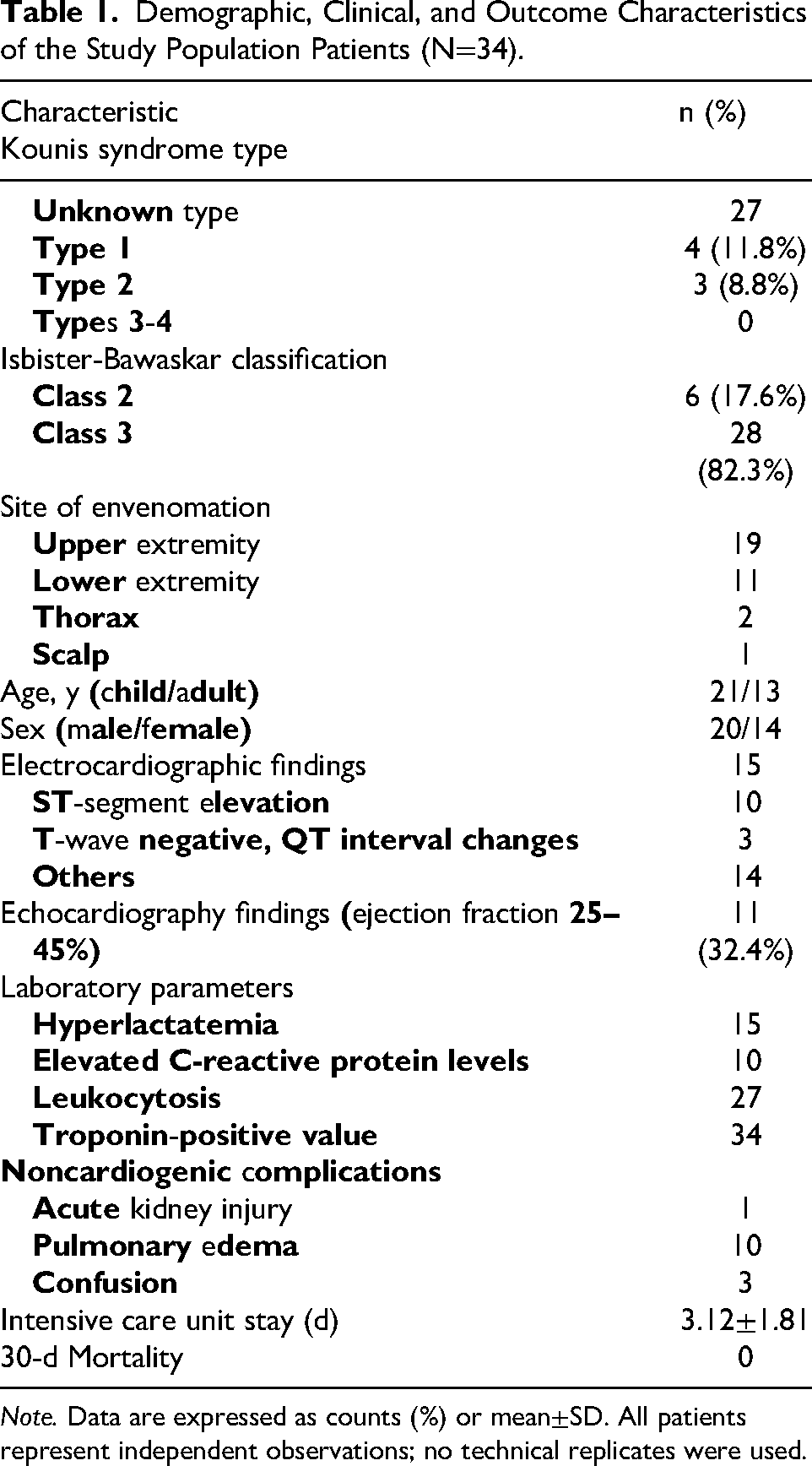
Note. Data are expressed as counts (%) or mean±SD. All patients represent independent observations; no technical replicates were used.
Age-Based Comparison of Clinical and Cardiac Findings (N=34).
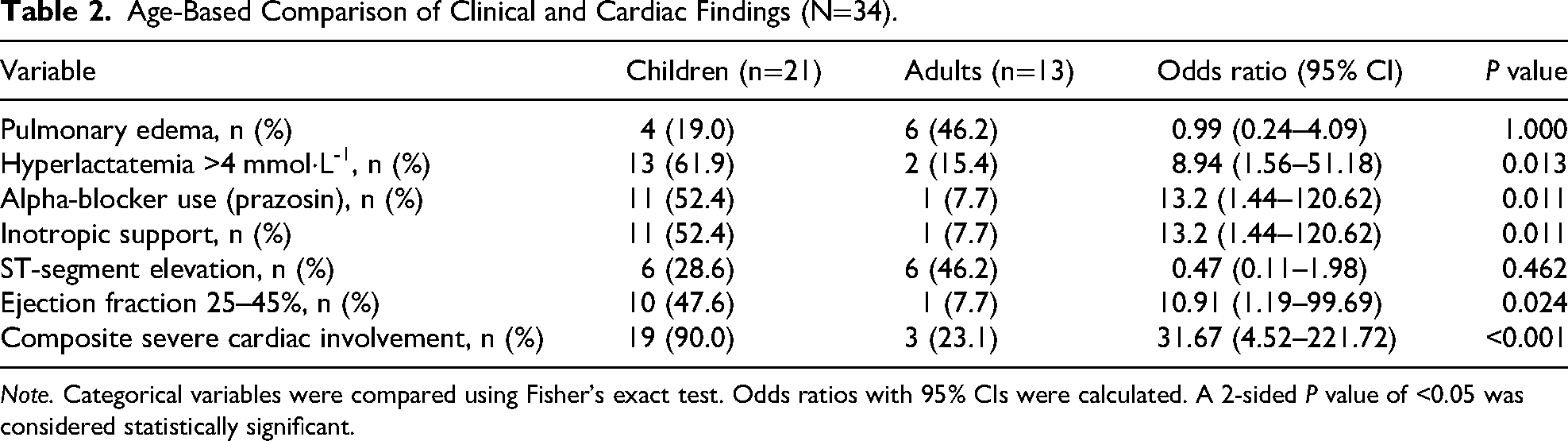
Note. Categorical variables were compared using Fisher's exact test. Odds ratios with 95% CIs were calculated. A 2-sided P value of <0.05 was considered statistically significant.
Emergency coronary angiography was performed in 20.5% of patients, and 57.1% of those examined showed no significant obstructive coronary lesions. Transthoracic echocardiography identified reduced left ventricular ejection fraction (LVEF 25–45%) in 11 patients (32.4%). Ten patients received prazosin therapy, and all patients required intensive care unit (ICU) admission. The mean time to antivenom administration was 3.87±3.50 h. No statistically significant association was observed between antivenom administration and the use of prazosin therapy (Spearman's ρ=−0.015, P=0.932). Similarly, antivenom dose did not differ significantly between patients who received prazosin and those who did not (P=0.953). During ICU follow-up, pulmonary edema was observed in 10 patients (29.4%), mild alterations in mental status in 3 (8.8%), and acute kidney injury in 1. No major bleeding, thromboembolic events, or mortality were recorded at 30 d.
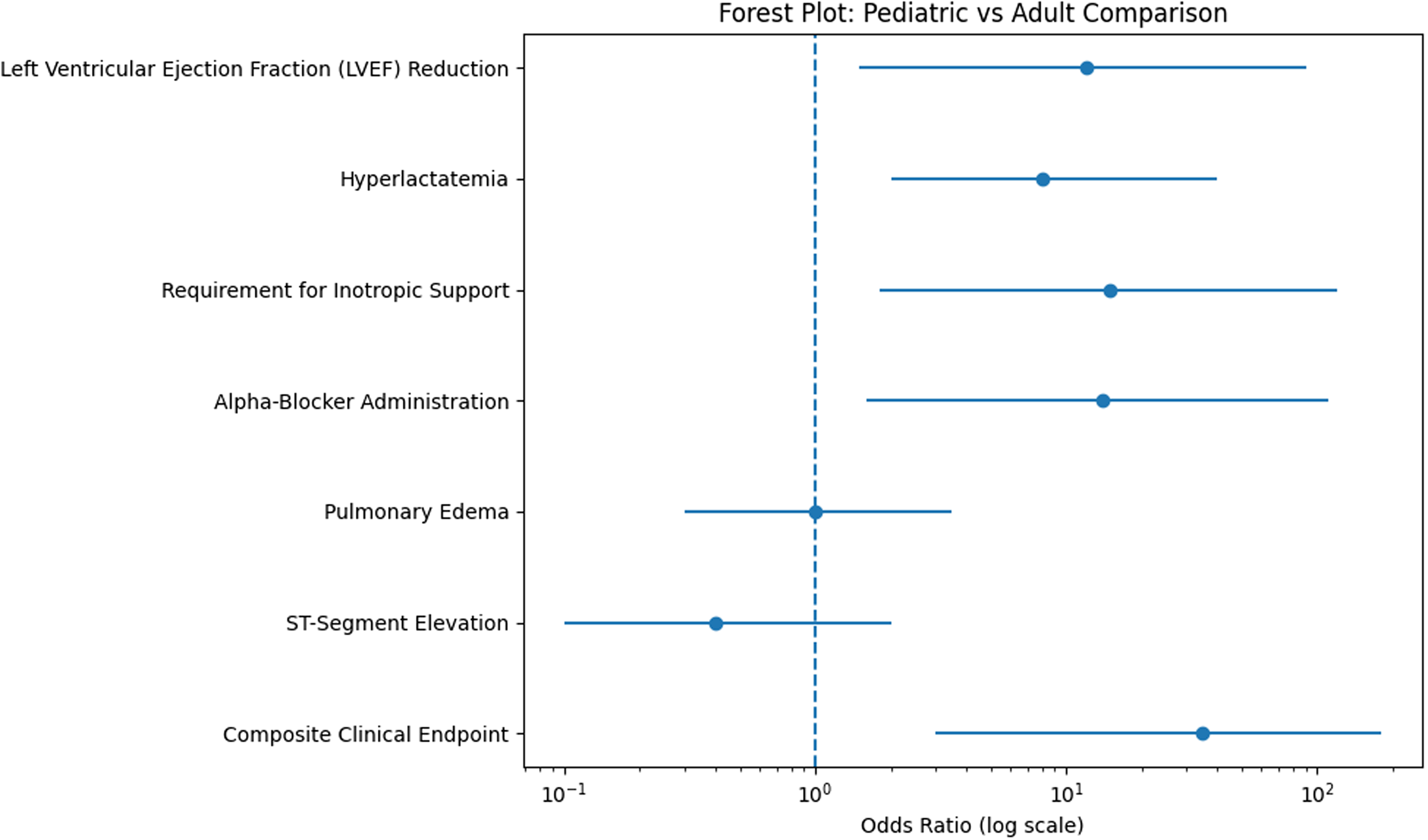
When pediatric and adult patients were compared, significant differences in cardiac involvement were observed. New-onset LVEF reduction was more frequent in pediatric patients (47.6 vs 7.7%, P=0.041). Hyperlactatemia (>4 mmol·L-1; 61.9 vs 15.4%, P=0.021) and administration of prazosin (52.4 vs 7.7%; P=0.022) also were significantly higher in children. Inotropic support was required more frequently in pediatric patients (52.4 vs 7.7%), and this difference was statistically significant (P=0.011). Time to antivenom administration did not differ significantly between the groups (Figure 1).
Forest plot of pediatric vs adult patients.
In univariable OR analysis, pediatric age was associated with increased odds of LVEF reduction (OR 10.9, 95% CI 1.19–99.69), hyperlactatemia (OR 8.94, 95% CI 1.56–51.19), administration of prazosin (OR 13.2, 95% CI 1.44–120.63), and inotropic support (OR 13.2, 95% CI 1.44–120.62). The predefined composite endpoint of severe cardiac involvement occurred more frequently in pediatric patients (90 vs 23%), with significantly increased odds compared with adults (OR 31.7, 95% CI 4.52–221.73, P<0.001).
Discussion
Ks represents an uncommon etiology of scorpion sting-associated acute coronary syndromes in both pediatric and adult populations. Despite the observed increase in case reports, the number of published cases in the literature remains limited. We report 34 instances of rare scorpion venom-associated Ks in an endemic region, highlighting the spectrum of clinical presentations and hemodynamic compromise. To our knowledge, this represents one of the largest series focusing on toxin-induced allergic coronary vasospasm in children and adults.
Ks, traditionally conceptualized as an allergic acute coronary syndrome, exemplifies the complex interplay between immune-mediated hypersensitivity and cardiovascular pathophysiology. Triggered by mast cell degranulation, the release of inflammatory mediators contributes to coronary vasospasm and myocardial injury. 1 In scorpion-associated Ks, this immunologic cascade is compounded by direct venom-induced cardiotoxic effects, resulting in a dual-pathway mechanism involving both allergic mediators and neurocardiotoxicity. Importantly, this pathophysiologic spectrum extends beyond classic allergens to include envenomation syndromes, such as scorpion stings, which are particularly relevant in endemic regions. Although species-level identification was not feasible due to the retrospective nature of the study, epidemiologic data suggest that A crassicauda is the predominant species responsible for severe envenomation in the region. This contextual information supports the clinical relevance of the observed findings, although definitive species confirmation remains a limitation.
Scorpion venom α-toxins modulate voltage-gated sodium channels, prolonging depolarization, and a paradoxical “autonomic storm” characterized by simultaneous cholinergic and adrenergic hyperactivation.7,8 By inhibiting sodium channel inactivation, these toxins provoke sustained neuronal depolarization and a massive discharge of endogenous catecholamines, thereby promoting intense coronary vasospasm and myocardial oxygen supply-demand mismatch. In severe cases, this autonomic dysregulation may be accompanied by direct myocardial toxicity, manifesting as transient systolic dysfunction, arrhythmias, myocarditis-like injury, or cardiogenic shock.7,8 This convergence of venom-induced autonomic imbalance with classical Ks mechanisms provides a coherent framework for understanding the heterogeneous cardiovascular manifestations observed in this cohort.
The severity of events in all cases was assessed using both the Ks classification and the Isbister-Bawaskar criteria. Analysis revealed that Isbister-Bawaskar Class 3 (n=28) and Ks Type 1 (n=4) were the most frequently observed, followed by Ks Type 2 (n=3) and Isbister-Bawaskar Class 2 (n=6). Although Ks Type 1 and Isbister-Bawaskar Class 1 cases are reported to be more prevalent in the literature, Ks Type 2 and Isbister-Bawaskar Class 2 and 3 cases were associated with more severe clinical outcomes. These findings further underscore the clinical importance of early phenotypic differentiation in guiding therapeutic decision making.1–3
Review of published case series and systematic analyses demonstrates that Ks encompasses a broad spectrum of clinical manifestations and triggers. In the largest compilation by Yakushin et al, involving 235 patients, the most frequent precipitants were antibiotics (32.3%) and nonsteroidal anti-inflammatory drugs (24.3%), whereas insect stings were less commonly implicated. The predominant clinical features included hypotension (74.2%), chest pain (59.1%), pruritus (30.6%), and dyspnea (30.6%), with ST-segment elevation reported in 42.9% of patients. Coronary angiography was performed in 80.4% of patients, half of whom (50.3%) demonstrated angiographically normal coronary arteries. Similarly, Rachel-Perez et al analyzed 155 cases and reported that Ks Type 2 and Type 3 variants accounted for 24.38 and 14.11% of presentations, respectively. In this cohort, ECG abnormalities were observed in 94.1% of patients, with ST-segment elevation in 59.09%. 9
In a pediatric review of 11 patients, all demonstrated ECG abnormalities, most commonly ST-segment changes (63.6%) and T-wave alterations (18.2%), with less frequent ST elevation followed by depression (9.1%) and T-wave inversion (9.1%). Coronary angiography was unavailable in 27.3% of patients. Echocardiography performed in 9 patients was normal in 6. Cardiovascular pharmacotherapy was administered in 25% of patients, including vasodilators, angiotensin-converting enzyme inhibitors, beta-blockers, calcium channel blockers, diuretics, and aspirin. 10 Most patients underwent coronary angiography to assess coronary anatomy, whereas only 1 patient underwent computed tomography angiography. Although both imaging modalities reliably depict coronary anatomy, initial use of computed tomography angiography may be advantageous by avoiding invasive procedures.
In pediatric series, ECG abnormalities are frequent, with ST-segment changes predominating. 10 In our cohort, coronary angiography was performed less frequently (20.5%) than reported in the literature. This selective approach was guided by clinical, laboratory, and imaging findings suggesting predominantly functional or vasospastic mechanisms rather than fixed obstructive coronary disease.
ECG findings, particularly ST-segment elevation, were observed in 29.4% of patients, but no statistically significant difference was found between pediatric and adult groups (P=0.462). While ST-segment elevation may reflect coronary vasospasm or myocardial injury, the spiked-helmet sign should be considered a differential diagnosis in hyperadrenergic states. Recognition of the spiked-helmet sign is clinically important because it may prevent unnecessary invasive reperfusion strategies in patients whose presentation is driven by autonomic dysregulation.
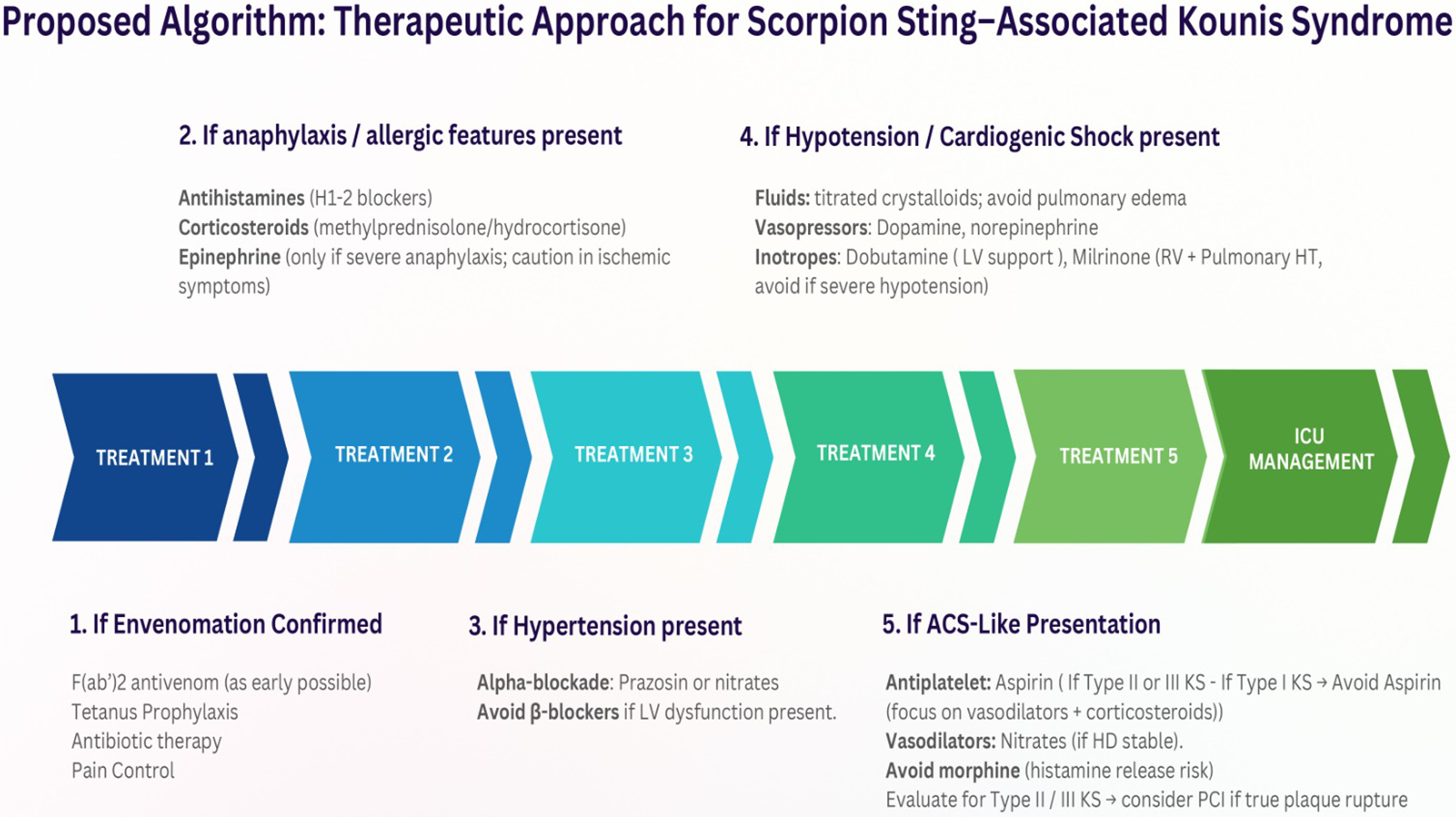
In this study, cases of Ks triggered by scorpion envenomation were managed following algorithms that incorporate acute interventions and supportive care despite the lack of a universally accepted treatment consensus. The frequency of administered therapies—including antihistamines, corticosteroids, antihypertensives (eg, prazosin and nitrates), vasopressors, inotropes, antivenom, tetanus prophylaxis, antibiotics, and diuretics—is summarized in Figure 2. This systematic documentation facilitates a comprehensive evaluation of treatment strategies and may inform clinical decision making, potentially guiding optimized management approaches in scorpion sting-induced Ks. 11
Stepwise management of scorpion sting-induced Kounis syndrome.
Management of scorpion sting-associated Ks requires simultaneous control of the allergic response, venom-induced cardiotoxicity, and acute coronary manifestations. Early administration of antivenom and cardiovascular stabilization with vasopressors, inotropes, and antihypertensives (eg, prazosin or nitrates) are essential. Adjunctive therapies, including systemic corticosteroids and antihistamines, are recommended despite variability in clinical studies, given their potential role in mitigating hypersensitivity-mediated cardiovascular inflammation.12,13 Antihistamines may further stabilize mast cell membranes and modulate endothelial activation, although robust evidence for independent clinical efficacy remains limited.6,12
In the early vascular phase of scorpion envenomation, heightened catecholamine release leads to systemic hypertension, increased myocardial contractility, and tachyarrhythmias. Management strategies frequently include alpha-adrenergic blockade with prazosin or nitrates to reduce coronary ischemia and peripheral vascular resistance, whereas antithrombotic therapy supports coronary perfusion. Prazosin administration enables rapid hemodynamic stabilization, controlling myocardial oxygen consumption without increasing preload or afterload.14,15 Although β-blockers may suppress sympathetic overactivity, their use is limited in patients with reduced cardiac reserve due to risks of bradycardia and negative inotropy. 16
In patients developing myocardial dysfunction, hemodynamic support was prioritized. In patients with concomitant heart failure, hypotension, or acute pulmonary edema, dopamine and dobutamine were administered to enhance cardiac output and organ perfusion, leveraging their inotropic effects alongside mild vasodilatory properties. In patients with elevated pulmonary artery pressures, milrinone was selectively used due to its ability to reduce pulmonary vascular resistance and right ventricular afterload. In patients with acute coronary syndrome, the primary goal was medical stabilization, with coronary angiography and percutaneous interventions performed when clinically indicated.
Beyond the coronary arteries, scorpion envenomation can involve cerebral and mesenteric vessels, contributing to systemic complications such as acute kidney injury and altered mental status. Noncardiac complications are common, with acute kidney injury observed in 1 patient (2,9%), mild confusion in 3 patients (8.8%), and pulmonary edema in 10 patients (29,4%), reflecting the widespread vascular impact of envenomation. Venom-induced hypoperfusion, systemic inflammatory activation, and direct nephrotoxic effects likely underlie renal injury, whereas cerebral involvement may account for the observed confusion. Pulmonary edema, often accompanied by dyspnea, reflects cholinergic overstimulation and impaired left ventricular function, frequently necessitating noninvasive mechanical ventilation.
Reported mortality rates for Ks in the literature range from 7.47 to 22%.14–17 In contrast, all patients in our series survived and were discharged in stable condition, with no mortality observed within 30 d. These favorable outcomes may be associated with timely antivenom administration and comprehensive intensive care support. All patients received F(ab′)2 antivenom within a mean of 3.87±3.50 h after envenomation. Early antivenom therapy has been associated with a reduced incidence of severe systemic complications.18,19 Notably, no anaphylactic reactions to antivenom were observed, consistent with the established safety profile of F(ab′)2 fragments. 20 The critical importance of early recognition of Ks, prompt and appropriate antivenom administration, and the provision of individualized, multidisciplinary supportive care in the ICU setting is emphasized.
In this study, no significant association was identified between antivenom administration and subsequent prazosin use. However, this finding should be interpreted with caution because antivenom dosing showed limited variability and the sample size was relatively small, potentially limiting statistical power.
A notable observation was the predominance of pediatric patients in this cohort (n=21; 61.7%). Age-stratified analysis demonstrated significantly higher rates of LVEF reduction, hyperlactatemia, and administration of prazosin in children compared with adults despite similar antivenom administration times. These findings suggest a potentially age-dependent cardiovascular response to scorpion envenomation.
Physiologic differences in body surface area, distribution volume, and myocardial reserve may contribute to this pattern. A relatively greater effective venom burden per body mass may amplify catecholamine-mediated myocardial stunning, resulting in transient systolic dysfunction and hemodynamic instability.
In contrast, adults demonstrated lower rates of LVEF reduction, indicating a potentially different physiologic response pattern. The absence of differences in treatment delay between groups supports the hypothesis that intrinsic age-related factors, rather than timing of antivenom administration, may contribute to these disparities.
The composite endpoint of severe cardiac involvement further reinforced this age-related pattern, occurring more frequently in children. Although the observed odds ratio was substantial, the wide confidence interval reflects the limited sample size and warrants cautious interpretation.
In our pediatric cohort (n=21), coronary angiography was deliberately avoided owing to the low likelihood of preexisting atherosclerotic disease and the high probability that ECG abnormalities reflected functional or nonischemic mechanisms, such as autonomic dysregulation or the spiked-helmet sign. To mitigate the venom-induced autonomic storm and associated hypertension, prazosin was administered to 9 pediatric patients in the emergency department, enabling rapid hemodynamic stabilization by reducing afterload and optimizing myocardial oxygen balance.
This predominantly noninvasive diagnostic and therapeutic strategy, combined with early antivenom administration (mean time 3.87±3.50 h), was associated with excellent clinical outcomes. These findings suggest that in carefully selected pediatric patients with scorpion-associated Ks, invasive procedures may be avoidable in carefully selected cases when prompt pharmacologic treatment and multidisciplinary supportive care are implemented.
Limitations
This study has several limitations. First, the retrospective design limits causal inference and relies on the accuracy of medical records. Second, the relatively small sample size and single-center setting restrict the generalizability of the findings. Third, precise species-level identification of the scorpion was not possible, which may limit the interpretation of envenomation severity and toxin-specific effects. Finally, treatment parameters, particularly antivenom dosing, showed limited variability, which may have reduced the ability to detect potential associations between treatment interventions and clinical outcomes.
Conclusions
Scorpion sting-associated Ks is a rare but clinically significant condition. Unlike in allergen-triggered variants, the availability of a specific antivenom targeting scorpion venom may have contributed to the absence of mortality in this cohort. In our experience, early recognition, close monitoring, and timely supportive management were generally associated with favorable short-term outcomes. However, larger prospective studies are needed to better characterize this underreported manifestation and to establish standardized diagnostic and therapeutic approaches.
Footnotes
Ethical Considerations
Ethical approval was granted by the local ethics committee (Approval No. 2024/06-5443).
Financial/Material Support
The authors received no financial support for the research, authorship, and/or publication of this article.
Author Contribution(s)
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.