
Abstract
Tick-borne disease (TBD) poses a significant threat to human health due to increasing incidence, a broad range of symptoms, and potential severity.1,2 Prevention behaviors are essential for reducing the risk of TBD and include strategies to avoid tick bites as well as steps to minimize the likelihood of infection after a bite. The US Centers for Disease Control and Prevention (CDC) recommends prevention behaviors for the general population, outlining steps to take both before going outdoors and after returning indoors after outdoor exposure. 3 These behaviors include treating clothing and gear with products containing 0.5% permethrin, minimizing exposure to tick habitats, using insect repellent sprays/creams/lotions, and conducting tick checks of clothing and the body shortly after outdoor activity. 3
The Appalachian Trail (AT) is a continuous footpath spanning across 14 states in the eastern United States and attracts over 3 million visitors annually. 4 While many visitors hike short sections (1–2 days), others undertake longer excursions lasting a week or more. Long-distance hiking involves spending extended time periods on the trail, covering significant distances, and living primarily in the wilderness for 5–7 days at a time before spending a night in a town at a hostel or hotel. 5 One form of long-distance hiking, known as thru-hiking, consists of completing the entire AT within a year, which typically requires 5–7 months outdoors. Long-distance hiking exposes individuals to a range of health risks, including poor sanitation, blisters, giardia, and norovirus. 6 However, the AT Conservancy (ATC) highlights TBD as the most serious concern hikers face while hiking on the AT. 6 Additionally, the main hiking season, from spring through early fall, coincides with peak tick activity, further increasing TBD risk. 7 While several tick species are found along the AT, the blacklegged tick (Ixodes scapularis) is of primary concern due to carrying Lyme disease as well as several other TBDs that are increasing in prevalence on the AT, such as babesiosis and anaplasmosis. Other notable tick species are the American dog tick (Dermacentor variabilis), carrier of Rocky Mountain spotted fever, and the lone star tick (Amblyomma americanum), carrier of ehrlichiosis and causative agent of alpha-gal syndrome. 7
The ATC reinforces the CDC's recommended prevention behaviors and offers additional guidelines specific to hikers, such as avoiding sitting directly on the ground or on logs and selecting lower-risk times and areas for hiking. 6 Many of these recommended prevention behaviors are feasible for both the general population and for individuals hiking short sections of the trail. However, long-distance hiking presents unique challenges. For example, showering after outdoor exposure, recommended by both the CDC and ATC, may be impossible for long-distance hikers who spend extended periods camping in remote areas without access to facilities. Additionally, long-distance hikers may struggle to limit their exposure to high-risk tick habitats, as it typically requires covering many miles each day in outdoor environments. 5 Consequently, the combination of high tick prevalence along the AT and the practical limitations of long-distance hiking places these hikers at a particularly elevated risk of contracting TBD. 8
Despite the unique challenges that long-distance AT hikers face in implementing prevention behaviors against TBD, most existing research focuses on the general population or on individuals engaging in outdoor recreation more broadly, rather than on extended, long-distance hiking.9-12 Research has found that knowledge about TBD is poor among the general population, and adoption of prevention behaviors varies significantly across groups. 13 Studies of people who engage in outdoor recreation are more mixed, suggesting that patterns of knowledge, risk perception, and prevention behavior may differ between the general population and hikers.12,14 The knowledge, attitudes, and preventive behaviors of long-distance hikers remain unknown. Understanding the specific behaviors of long-distance AT hikers is therefore essential, as their prolonged exposure to wilderness environments may place them at a uniquely elevated risk.
The health belief model (HBM) is a theoretical framework used to predict and understand why individuals choose to take action to prevent illness.15,16 According to the constructs of the HBM in terms of TBD, individuals are more likely to engage in prevention behaviors if they perceive themselves as at risk of TBD (perceived susceptibility), believe TBD would have serious consequences (perceived seriousness), believe that a given prevention behavior is effective in reducing the risk or severity of TBD (perceived benefits), believe that any barriers or costs to the prevention behavior (perceived barriers) are outweighed by the benefits, and believe they have the ability to accomplish the prevention behavior (self-efficacy). While previous studies have found HBM constructs effective in predicting prevention behavior against TBD in various populations, their applicability has not yet been examined within long-distance hiker populations.17-19
The purpose of the present study is to examine the prevention behaviors that long-distance hikers on the AT employ to protect against TBD, as well as the perceptions and beliefs that shape these behaviors. Guided by the HBM, this study investigates hikers’ preventive behaviors and perceptions of these behaviors and TBD. The study seeks to answer the following questions: 1) What strategies are long-distance AT hikers employing to prevent TBD, and 2) Do the constructs of the HBM predict whether long-distance AT hikers engage in behaviors to prevent TBD? By addressing these questions, the study aims to provide a better understanding of the factors influencing TBD prevention among long-distance hikers. Given the considerable challenges that the long-distance hiking environment presents for practicing prevention behaviors, we hypothesize that long-distance AT hikers tend to have low adherence to prevention behaviors for TBD and that perceived barriers are strongly associated with hikers’ prevention behaviors.
Methods
It was determined by Appalachian State University's Institutional Review Board (IRB) that this study constitutes research with human subjects, but that, in accordance with federal regulations and university policy and procedures, the research activities are exempt from IRB review (IRB study #HS-25-72). Participants were eligible if they were 18 years old or older and had any prior experience hiking on the AT. Exclusion criteria were being under 18 years old and having no experience hiking on the AT.
Survey Development and Data Collection
A self-administered questionnaire using Qualtrics (https://www.qualtrics.com) obtained demographic information and assessed participants’ TBD exposure, prevention practices, and constructs of the HBM. The survey was pilot-tested with 12 individuals, including those with and without hiking experience, to assess comprehension and estimate completion time. No major revisions were required following the pilot test. The survey took approximately 10 min to complete and was adapted to hardcopy to provide an alternative way for participants to complete the survey.
Demographic Characteristics and Hiking Experience
Survey items included questions on gender, age, race/ethnicity, highest level of education, and total annual household income. One item classified respondents’ previous hiking experience on the AT at any time point as either a thru-hiker (completed the AT in a calendar year or less), a section-hiker (hiked a section or sections of the AT), or a casual hiker (day-hiker or weekend hiker on the AT).
TBD Exposure and Prevention Behaviors
Survey items assessed whether participants had ever received a diagnosis of a TBD from a licensed healthcare provider and, if so, whether the disease was attributed to a tick bite sustained while hiking on the AT.
Preventive behaviors were classified according to the CDC and ATC guidelines as: 1) avoiding sitting directly on the ground or logs; 2) avoiding tick-prone areas and staying on marked trails; 3) carrying and, if needed, using tick removal devices such as tweezers; 4) performing daily full-body tick checks; 5) showering or bathing after hiking; 6) using clothing and gear correctly treated with permethrin; 7) wearing insect repellent; 8) wearing light-colored clothing; and 9) wearing protective clothing (long pants/long socks). The frequency that participants engaged in each prevention behavior while hiking on the AT was measured using items on a 5-point scale from “never” to “always.” A mean prevention behavior score was computed for each participant by averaging their Likert-scale ratings across all 9 prevention behaviors. This yielded a single variable reflecting overall prevention frequency.
Constructs of the HBM
Perceived seriousness, susceptibility, and self-efficacy were assessed on 5-point Likert scales from “strongly disagree” to “strongly agree.” Perceived seriousness and susceptibility were each measured by one statement (“If I contracted a tick-borne illness, it would be a serious health concern” and “I thought it was likely that I would contract a tick-borne illness while hiking on the AT,” respectively). Self-efficacy was measured through 2 statements (“I feel confident in my ability to prevent tick bites while hiking on the AT” and “I feel confident in my ability to identify and manage tick bites while hiking on the AT”), and a variable was created as the mean of these two items.
Nine items were used to assess participants’ perceived benefits of engaging in each behavior while hiking on the AT to prevent TBD on 5-point Likert scales from “not effective at all” to “extremely effective.” A combined variable for perceived benefits was created as the mean of all 9 items. Nine items were used to assess participants’ perceived barriers to engaging in each prevention behavior while hiking on the AT on 5-point Likert scales from “extremely difficult” to “extremely easy.” A combined variable for perceived barriers was created as the mean of all 9 items. Cues to action were assessed using 2 dichotomous items (yes/no) asking whether participants: 1) had personally been diagnosed with a TBD and 2) knew someone who had been diagnosed with a TBD. A combined dichotomous cues-to-action variable was created to indicate whether participants had personally been diagnosed with a TBD and/or knew someone who had been diagnosed with a TBD (yes) or had never been diagnosed and did not know someone who had been diagnosed with a TBD (no).
Data Collection
Three modes of survey data collection were employed: online forum posts, snowball sampling, and in-person recruitment, which included both online and paper-based surveys. The primary mode of data collection was in-person recruitment at the 2025 Trail Days Festival, held at the ATC's Damascus Trail Center in Damascus, Virginia. Trail Days is a 3-day annual festival of the AT and “hiker culture” that attracts past, current, and future hikers. 20 Multiple survey administration formats were offered, including paper surveys, iPads with the online survey, and QR codes linking to the online survey. Informational signage was displayed to provide a brief description of the study and invite potential participants to take part.
The survey link was also disseminated through online forums of hiking-related groups on Facebook, as well as in 2 of the largest Reddit communities of AT hikers. Posts included a brief description of the study, inclusion criteria, the estimated survey completion time, and a link to the survey.
Lastly, snowball sampling was used to expand recruitment by contacting AT hikers known to the research team who met eligibility criteria and inviting them to participate. These individuals were then asked to share the survey link with other AT hikers in their networks, extending the reach of data collection beyond the initial contacts.
Data Analysis
All analyses were performed using IBM SPSS Statistics (version 31). Respondents were only included in data analysis if they classified their hiking experience on the AT as either a thru-hiker or a section-hiker. Frequencies were calculated for demographic characteristics, hiking experience, TBD exposure, and TBD prevention behaviors. Multiple regression models assessed whether the HBM constructs predicted participants engaging in prevention behaviors. Nine regression models included each prevention behavior individually as the dependent variable, with the corresponding constructs as predictors, along with gender, age, education level, and total household income. A 10th regression model included the mean of all prevention behaviors as the dependent variable, with the corresponding constructs (combined perceived benefits and barriers variables) included as predictors, along with gender, age, education level, and total household income. The significance level was set at p ≤ .05 for all analyses.
Results
A total of 247 respondents completed the survey. After excluding 23 respondents who identified as casual hikers and 22 with missing data on the key variables for data analysis, a total of 202 responses were included. Table 1 provides all the demographic characteristics of the sample. Over one-fifth (20.8%) of respondents reported having been diagnosed by a licensed healthcare professional with 1 or more TBDs. Lyme disease was the most reported diagnosis, accounting for 78.6% of all TBD diagnoses reported by respondents. This represents 16.3% of the total sample. Alpha-Gal syndrome accounted for 14.3% of all TBD cases. Babesiosis, anaplasmosis, ehrlichiosis, and Rocky Mountain spotted fever each accounted for 4.8% of reported TBD cases.
Demographic Characteristics of Respondents.
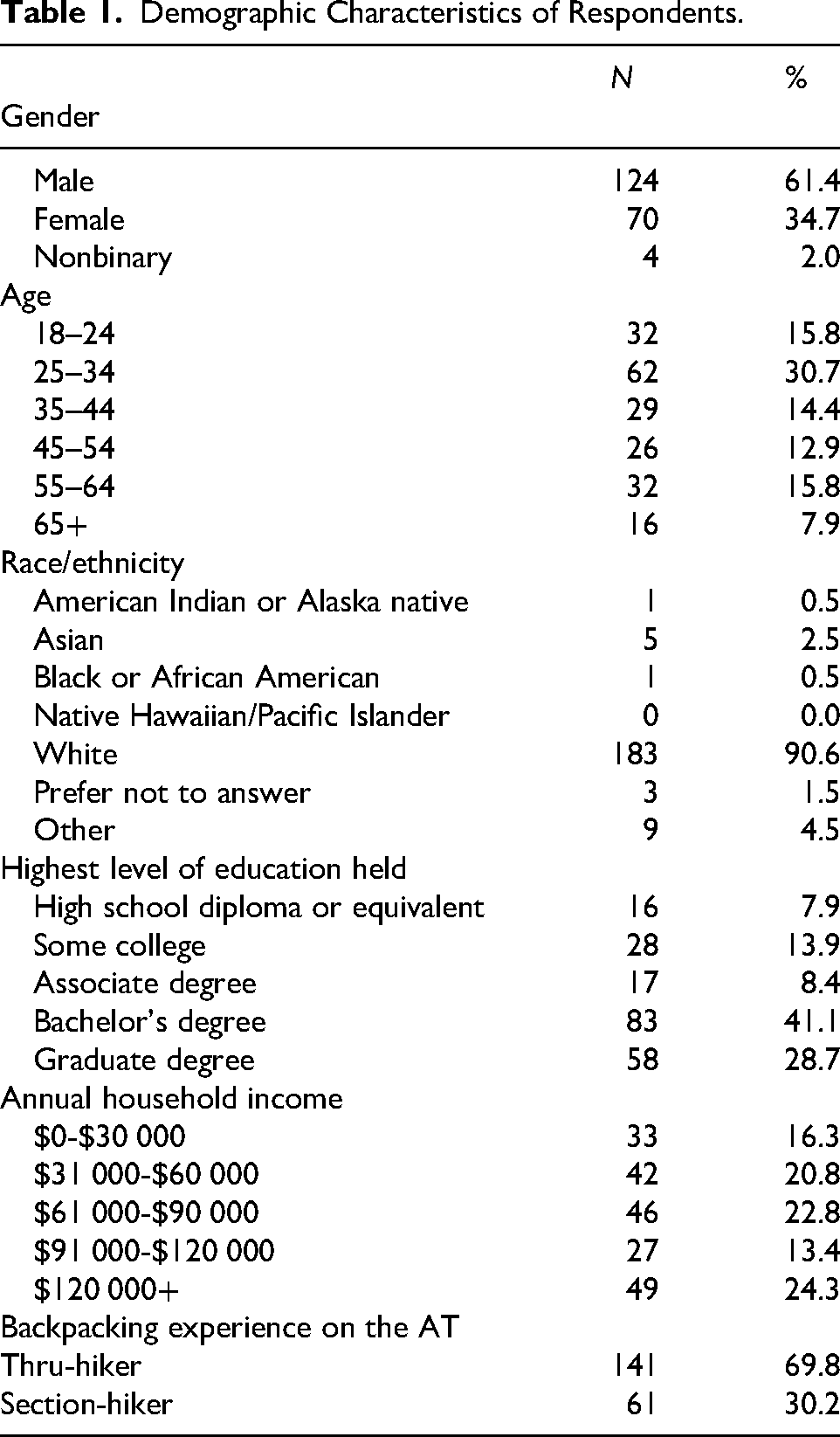
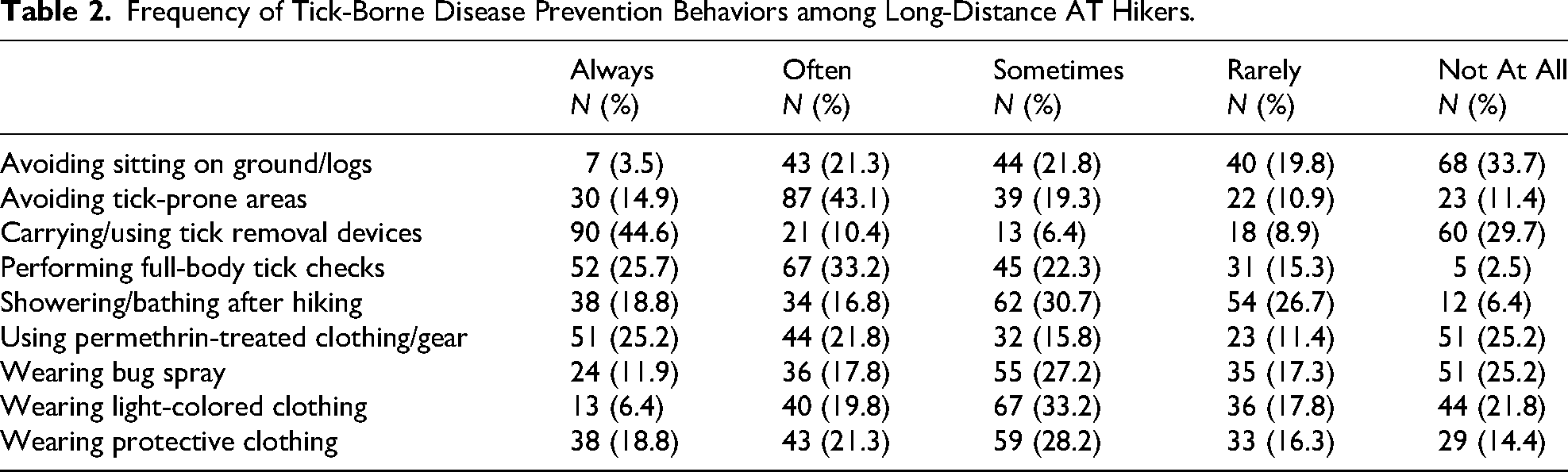
Table 2 provides the reported frequencies of all prevention behaviors. Almost three-quarters (72.8%) of the sample reported always performing at least 1 prevention measure. The prevention behaviors most frequently reported as “always” performed were carrying and using tick removal devices if needed (44.6%), performing daily full-body tick checks (25.7%), and using clothing and gear correctly treated with permethrin (25.2%). The prevention behaviors least frequently reported as “always” performed were avoiding sitting directly on the ground or logs (3.5%), wearing light-colored clothing (6.4%), and wearing bug spray (11.9%). The prevention behaviors most frequently reported as “not at all” performed were avoiding sitting directly on the ground or on logs (33.7%), carrying and using tick removal devices if needed (29.7%), using clothing and gear correctly treated with permethrin (25.2%), and wearing bug spray (25.2%).
Frequency of Tick-Borne Disease Prevention Behaviors among Long-Distance AT Hikers.
The multiple regression models statistically significantly predicted avoiding sitting on the ground/logs, F(10, 168) = 14.535, p < .001, adj. R2 = .432; avoiding tick-prone areas, F(10, 166) = 6.385, p < .001, adj. R2 = .234; carrying and using tick removal devices, F(10, 168) = 18.130, p < .001, adj. R2 = .490; performing full-body tick checks, F(10, 166) = 9.459, p < .001, adj. R2 = .325; showering or bathing after hiking, F(10, 166) = 10.045, p < .001, adj. R2 = .339; using clothing and gear treated with permethrin, F(10, 165) = 9.308, p < .001, adj. R2 = .322; wearing bug spray, F(10 165) = 7.662, p < .001, adj. R2 = .276; wearing light-colored clothing, F(10, 166) = 7.889, p < .001, adj. R2 = .281; wearing protective clothing, F(10, 168) = 7.910, p < .001, adj. R2 = .280; and combined prevention behaviors, F(10, 170) = 11.320, p < .001, adj. R2 = .364. The inclusion of perceived barriers was the only variable that resulted in a statistically significant improvement in all of the models. The inclusion of perceived benefits resulted in a statistically significant improvement to all of the models except for the model predicting showering/bathing after hiking. The inclusion of perceived susceptibility resulted in a statistically significant improvement to the models predicting avoiding sitting on the ground/logs, performing full-body tick checks, showering/bathing after hiking, and performing any prevention strategy. The inclusion of cues to action resulted in a statistically significant improvement in the model predicting performing any prevention strategy. Regression coefficients and standard errors are found in Table 3.
Multiple Regression Analysis Results for HBM Predictors of Prevention Behaviors.
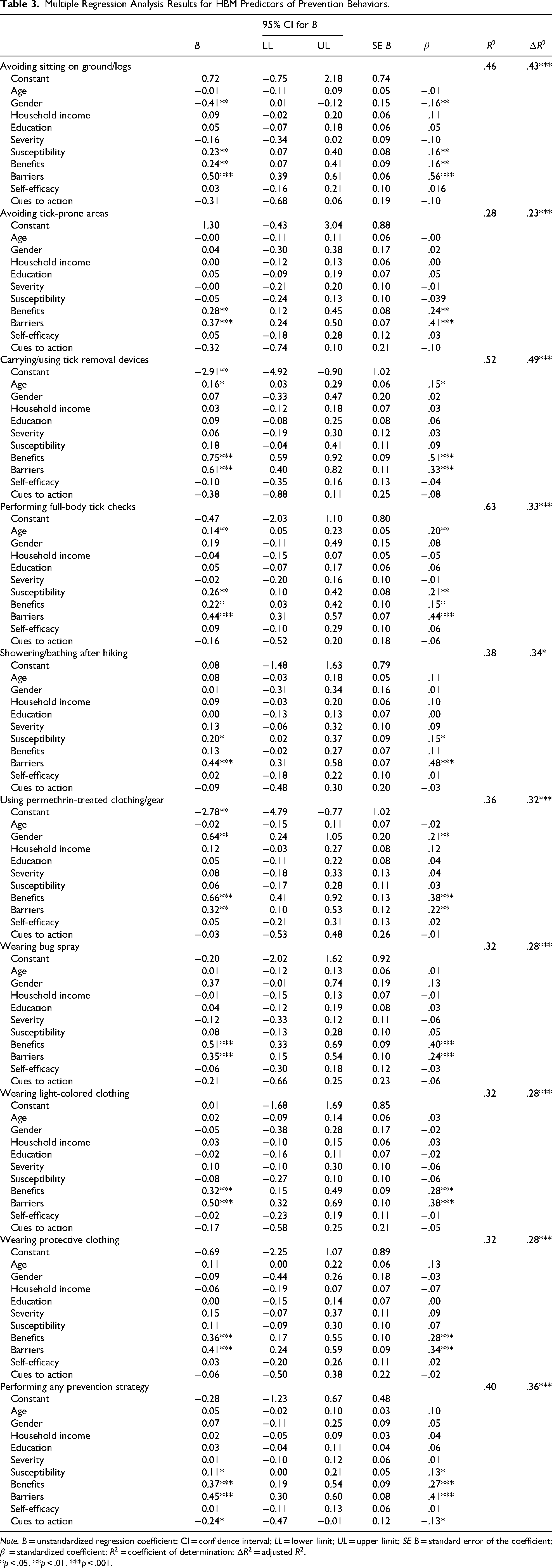
Note. B = unstandardized regression coefficient; CI = confidence interval; LL = lower limit; UL = upper limit; SE B = standard error of the coefficient;
*p < .05. **p < .01. ***p < .001.
Discussion
TBD Prevalence
One-fifth of the sample reported having been diagnosed with one or more TBDs, with Lyme disease having the highest reported prevalence rate (16.2%), making up 78.6% of all TBD cases. This aligns with existing research, which shows that Lyme disease is the most frequently diagnosed zoonotic TBD worldwide and the most common TBD in the United States, with case numbers continuing to rise. 21 Previous studies have also found that outdoor workers and recreationists have an elevated risk of Lyme disease, supporting our finding that long-distance hikers, who often spend comparatively greater time outdoors, also experience high rates of Lyme disease. 22
TBD Prevention Measure Frequency
Almost three-fourths (72.8%) of the respondents reported “always” performing at least 1 prevention behavior. This rate is higher than what has been reported in most previous studies of the general population and those visiting and recreating in outdoor areas, which generally suggest that personal prevention behaviors are not widely or consistently practiced. 23 Specifically, studies find that only about half or fewer individuals engage in such behaviors.9,11,24-26 Notably, our elevated finding is consistent with, though lower than, a study of British Columbia hikers, in which 92% reported taking at least one preventive measure against TBD. 12 This may indicate that hikers, especially those who spend extended time in outdoor environments in tick-prone regions such as the eastern United States, may adopt prevention behaviors more often than general recreationists or the general public.
Carrying tick removal devices was the most commonly reported behavior, with 44.6% of respondents indicating that they “always” carry and, when needed, use these devices. This contrasts with the 29.7% of respondents who reported “not at all” carrying these devices, representing the second-highest rate of non-use among the behaviors surveyed. These contrasting findings suggest that hikers are either consistently carrying tick removal devices or are never carrying these devices. Commercial devices specifically designed for tick removal have been shown to be effective for removing both nymphs and adult ticks and are a beginner-friendly tool, though most studies have focused on their use with animals, and research on their efficacy for humans remains limited.27-29 Carrying a tick removal device may be effective for hikers due to it being a simple and easy prevention behavior. Because carrying tick removal devices has rarely been categorized as a prevention behavior in prior research, our finding that it was the most commonly used strategy broadens understanding of the prevention approaches preferred by hikers.
The second most frequently reported behavior performed “always” was conducting daily full-body tick checks, reported by 25.7% of respondents. Although this represents the second most common behavior, the rate is relatively low and falls below adherence levels reported in previous studies, which range from 30% to 70%.9,17,18,30 Nonetheless, the prominence of tick checks aligns with prior research identifying them as one of the most commonly practiced prevention behaviors among outdoor recreationalists, outdoor workers, and the general population.9,17,18,30
About a quarter (25.2%) reported “always” using permethrin-treated clothing and gear. In contrast, fewer than 15% of the general population in high-incidence US states use permethrin-treated clothing, and willingness to do so was found to be the lowest out of any prevention measure.30,31 This low willingness may be due to largely unfounded concerns about chemical safety. Evidence supports the safety of permethrin for humans, even with prolonged daily use by military personnel, a scenario comparable to the extended use of treated gear by long-distance hikers.32,33 The differences in permethrin use between our sample and the general population may indicate that hikers hold different beliefs about permethrin use.
HBM Constructs
Perceived barriers (how easy/difficult the behavior is) were the most consistently significant construct, being associated with all of the prevention behaviors. The consistent significance of perceived barriers in our models suggests that, for long-distance AT hikers, these barriers strongly influence the likelihood of performing prevention behaviors. Previous research has identified barriers to TBD prevention behaviors and indicates that they significantly predict behavior.17,30,34,35 However, barriers are not consistently included in studies of TBD prevention behavior, including studies using the HBM. 18
Perceived benefits (how effective the behavior is) were the next most frequently significant construct after barriers, significantly associated with all of the prevention behaviors, with the exception of showering/bathing after hiking. Compared to the other behaviors, showering/bathing has numerous potential benefits aside from tick prevention (ie, basic hygiene) that could have limited the perception of effectiveness solely for tick prevention. Perceived benefits are generally identified as significant predictors, with behaviors perceived as more effective being more likely to be practiced.9,10,36-38 This aligns with our study findings.
Perceived susceptibility was a significant predictor of avoiding sitting on the ground/logs, performing full-body tick checks, showering/bathing, and the combined prevention behaviors. Evidence for perceived risk is mixed: among outdoor recreationalists, risk perception has a weak effect on preventive behavior, whereas studies of the general population and outdoor workers generally report a significant positive association between perceived risk and preventive behaviors.9,25,30,37,38 These mixed results may be partly explained by differences in how perceived susceptibility is measured. Many studies assess perceived susceptibility specifically for Lyme disease, whereas in the current study, the focus was on contracting any TBD.25,30,37,38 This distinction could contribute to inconsistent findings, as Lyme disease is the most common and therefore likely most recognizable TBD among AT hikers in our sample. Hikers may perceive their risk of TBD as lower or less tangible than their risk of Lyme disease specifically.
Cues to action, defined in the current study as either having a history of a TBD diagnosis or knowing someone who has, were only a significant predictor in the combined model. Existing literature suggests that cues to action can influence preventive behavior, but their effects may vary by type. For example, knowing someone with a TBD has been found to be a significant predictor in some studies, whereas personal experience with a TBD was not consistently significant.24,25 The influence of cues to action is challenging to establish, likely due to the complexity and difficulty of measurement.39,40
Perceived severity was not a significant predictor of behavior in any of our models, which is notable given that the ATC identifies contracting a TBD as the greatest threat to health for AT hikers. 41 While some previous studies assessing perceived severity of Lyme disease found this construct to be insignificant, others reported that perceived severity of Lyme disease was positively associated with preventive behaviors.24,30,37 These distinctions between our results and existing literature may also be due to our measurement approach, assessing perceived severity of TBD rather than of specifically Lyme disease. Additionally, self-efficacy was not a significant predictor in any models. This finding contrasts with previous research, which generally finds self-efficacy to be a significant predictor of behavior.9,18,37,42 The lack of significance for self-efficacy is likely due to the measurement approach. We assessed self-efficacy using only 2 broad questions about confidence in preventing tick bites and TBD. Measuring self-efficacy separately for each prevention behavior may have more accurately captured its impact on confidence in taking specific preventive actions by allowing respondents to assess their confidence for each behavior separately. Separate measurement would also aid in the targeting of education toward those behaviors that show the lowest self-efficacy.
Limitations
Because this study utilized a cross-sectional design, the associations identified cannot be interpreted as causal. Longitudinal or experimental studies would be necessary to establish temporal relationships between HBM constructs and prevention behaviors. Additionally, the sample was generally homogeneous in race/ethnicity, although this is consistent with data on long-distance AT hikers. The annual AT thru-hiker survey by The Trek consistently finds that 94 to 96% of AT thru-hikers identify as white. 43 This study did not assess the specific sections of the AT that respondents hiked, which could influence HBM constructs due to the variation of TBD by geographic region. Additionally, the respondent pool may have been subject to self-selection bias, as participation was voluntary. Individuals with prior experience with TBD may have been more likely to participate, potentially inflating the proportion of respondents reporting a diagnosed TBD. Lastly, as the majority of data was collected at the Trail Days Festival, respondents may have been more likely to hike sections of the AT that are in the southern regions rather than the central and northern regions.
Conclusion
Overall, this study provides insight into TBD attitudes and prevention behaviors among AT long-distance hikers. A substantial proportion of participants reported a history of TBD, with Lyme disease expectedly comprising the vast majority of cases, underscoring the heightened vulnerability of this population. The most frequently practiced prevention behaviors, carrying tick removal devices, conducting daily full-body tick checks, and using permethrin-treated clothing and gear, may represent those with the most favorable balance between perceived benefits and barriers for hikers. Consistent with the HBM, perceived barriers and benefits emerged as the most consistently influential predictors of prevention behaviors, suggesting that future interventions should aim to enhance perceived benefits while reducing barriers to action.
Footnotes
Acknowledgements
We thank Dakota Jackson and Emily Mayo of the Appalachian Trail Conservancy (for allowing and facilitating data collection during the Trail Days Festival) and Dr Martie Thompson of Appalachian State University (for early statistical guidance).
Ethical Considerations
The Appalachian State University Institutional Review Board (IRB) determined that this study constitutes research with human subjects, but that, in accordance with federal regulations and University policy and procedures, the research activities are exempt from IRB review (IRB study #HS-25-72).
Consent to Participate
Passive consent was obtained on the first page of the survey.
Author Contribution(s)
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.