
Abstract
Introduction
Trauma patients often require intravenous (IV) access for analgesia. Alternatively, analgesia can be administered intranasally (IN). This open-label crossover randomized, controlled trial aimed to determine the time required for IV and IN analgesia administration by military nurses in simulated prehospital trauma scenarios.
Methods
Military nurses completed 2 simulated prehospital trauma scenarios using a high-fidelity mannequin. Each scenario included patient assessment and administration of a simulated analgesic (water for injection). Military nurses administered the simulated analgesic intravenously in the first scenario and intranasally in the second scenario (sequence IV/IN) or vice versa (sequence IN/IV). Primary outcome was the time required for administration of the simulated analgesic. Secondary outcomes included on-scene time and user satisfaction with the route of administration employed.
Results
Of the 16 participants, 8 were allocated to sequence IV/IN and 8 to sequence IN/IV. Median age was 29 y, and 69% were female. IV administration required significantly more time than IN administration: mean difference 2.9 min (95% CI 2.4–3.4, p<0.0001). On-scene time also was significantly longer for IV administration: mean difference 3.3 min (95% CI 2.5–4.1, p < 0.0001). Median satisfaction scores were 6 (interquartile range 5–7) for IV administration and 9 (interquartile range 8–9) for IN administration. Satisfaction scores were lower for IV administration (p<0.0001).
Conclusions
Administration of a simulated analgesic required 2.9 min longer for IV compared with IN administration when performed by military nurses in simulated prehospital trauma care scenarios.
Keywords
Introduction
Pain management is a crucial aspect of prehospital trauma care. 1 The incidence of pain in prehospital trauma patients is high and often requires administration of analgesics, traditionally via intravenous (IV) access. 2 While seriously injured patients might require immediate IV access for other reasons, most notably administration of blood products in case of hemorrhage, many patients are not in immediate need of volume resuscitation but do require administration of analgesics. For these patients, obtaining IV access for the purpose of delivering analgesia might delay treatment. Research has shown that obtaining IV access is not always easy and increases on-scene time of Emergency Medical Services (EMS).3–5 Obtaining IV access might be even more challenging for providers who work in austere and environmentally challenging environments, such as military healthcare personnel. Other drug administration routes may provide suitable alternatives.
Intranasal (IN) administration has long been recognized as an easy and noninvasive alternative administration route for analgesia in emergency care. Although analgesia has a delayed onset of action after IN compared with IV administration, this might be compensated in part by easier and therefore earlier administration. A classroom-based study in advanced paramedic trainees found that IN administration required a mean 91 s less time than IV administration. 6 IN administration also was perceived to be easy and safe. Research evaluating the times required for IN and IV administration in simulated prehospital scenarios is lacking. Therefore, this trial aimed to determine the times required for IV and IN analgesia administration by military nurses in simulated prehospital trauma care scenarios. We hypothesized that the time required for analgesia administration would be longer for IV compared with IN administration.
Methods
Trial Design
This was an open-label randomized controlled trial with 2×2 crossover design. Because within-participant variation of the primary outcome was expected to be less than between-participant variation, using a crossover design required fewer participants. There was no patient or public involvement in the design of this trial.
The trial was performed by researchers from the Amsterdam university Medical Center (UMC) at the Netherlands Ministry of Defence. The Institutional Review Board of the Amsterdam UMC confirmed that the Medical Research Involving Human Subjects Act did not apply to this study (Waiver No. 2023.0492, July 20, 2023) because participants were not subject to procedures or required to follow rules of behavior, as documented in the Medical Research Involving Human Subjects Act. The study was registered prospectively at ClinicalTrials.gov (Registration No. NCT06351137). No significant changes were made to the trial protocol after the trial commenced. Study results were reported according to the CONSORT (Consolidated Standards of Reporting Trials) guidelines for randomized crossover trials, including the extension for healthcare simulation research.7–9
Participants
Eligible as participants were Dutch military nurses attending simulation training on prehospital trauma care. Military nurses are certified to provide prehospital military trauma care and trained according to the Dutch military guidelines based on guidelines by the Committee on Tactical Combat Casualty Care. 10 Written informed consent was obtained from all participants.
Scenario
Participants individually performed 2 scripted simulated prehospital trauma care scenarios (see online Supplementary File 1). Both scenarios involved assessment of a patient suffering from severe traumatic pain and requiring analgesia. Patient assessment was performed according to the MARCH acronym (Massive Hemorrhage, Airway, Respiration, Circulation, Head Injury/Hypothermia Prevention). The scenarios were designed so that IV access was required only for the administration of analgesia and not for other reasons such as immediate fluid resuscitation. This design reflects clinical practice, in which IN administration of analgesia is intended primarily for stable patients who do not immediately require IV access for other indications. Participants received a short verbal introduction prior to each scenario and were given 2 min to organize the medical kit.
The study was performed at a simulation center, and the patient was simulated using a high-fidelity mannequin, the TraumaFX CRU-R Simulator (TraumaFX, now TacMed Simulation; Anderson, SC). This model allows assessment as required by the MARCH protocol, IN administration into both nostrils and IV administration in multiple veins accessible on the arms. All scenarios were facilitated by the same physician with relevant expertise in prehospital analgesia. Specific cues were delivered by the facilitator when asked by the participant (eg, reporting of a pain score). The simulation center was fitted with limited lighting, and the mannequin was positioned sitting up in the corner of the room with limited access to replicate some of the challenges for obtaining IV access in the prehospital environment. Participant orientation to the mannequin and environment was left to the discretion of the participant. Participants performed the scenarios in military uniform using the standard military medical kit. Pilot testing was performed on 2 military nurses prior to the recruitment period.
Interventions
This trial determined the times required for IV and IN analgesia administration by military nurses in simulated prehospital trauma care scenarios. Analgesia administration was performed using water for injection as simulated analgesic. IV administration required obtaining IV access, drawing up the “medication,” and administering the simulated analgesic into the vein. IN administration required drawing up the “medication,” attaching the nasal atomizer to the syringe, and administering the simulated analgesic into both nostrils.
Study Procedures
Prespecified events were registered in real time by 2 members of the research team independently using stopwatches:
Start of the scenario (participant entering the room) Participant grabs the first item required for administration of the simulated analgesic from the medical kit, either being an IV setup, nasal atomizer, glass drug vial, syringe or blunt fill needle. IV scenario: Participant grabs IV setup from medical kit (if not done at 2). IN scenario: Participant grabs nasal atomizer from medical kit (if not done at 2). IV scenario: IV access has been obtained and taped or flushed, whichever comes last. IN scenario: Nasal atomizer has been attached to the syringe. Administration of the simulated analgesic is completed. End of the scenario (remaining materials are disposed of).
Relevant time intervals are presented in Figure 1. Time intervals were calculated for each assessor and then averaged for further analysis.
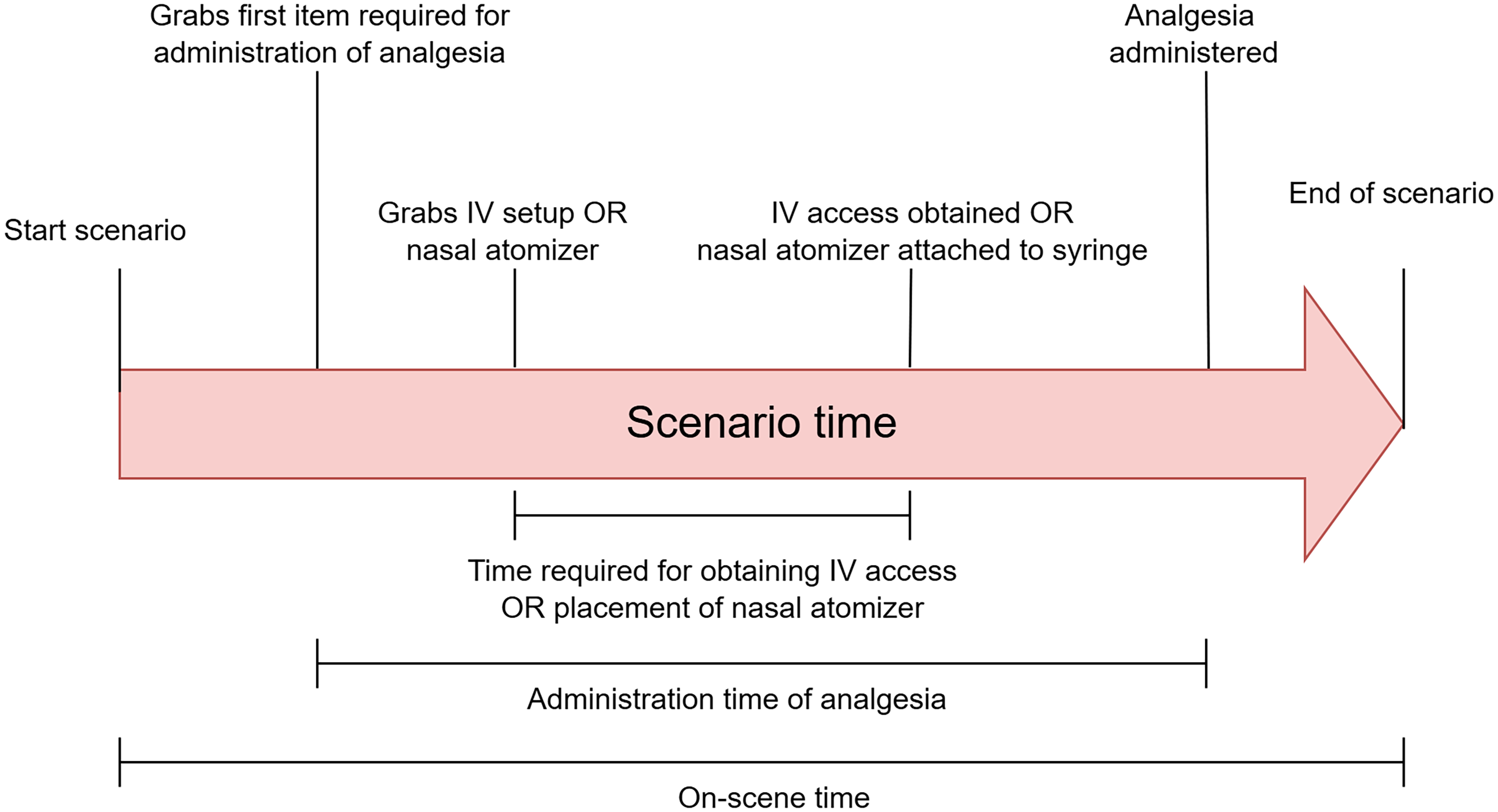
Events and intervals in the scenario. IV, intravenous.
Primary Outcome
Primary outcome was time required for administration of the simulated analgesic (Figure 1). The time interval started when the participant grabbed the first item required for administration of the simulated analgesic from the medical kit (eg, tourniquet, nasal atomizer, or drug vial). The time interval ended when administration of the simulated analgesic into the vein or nostrils was completed.
Secondary Outcomes
Secondary outcomes were on-scene time and time required for obtaining IV access or attaching the nasal atomizer (Figure 1). Participant satisfaction with the employed route of administration was measured on an 11-point Likert scale (0=extremely unsatisfactory; 10=extremely satisfactory) after each scenario.
Randomization
The randomization list was generated with R Statistical Software version 4.2.1 (R Core Team 2022, Vienna, Austria) before the start of the recruitment period using a randomization ratio of 1:1. Participants were randomized to sequence IV/IN or sequence IN/IV. Participants allocated to sequence IV/IN administered the simulated analgesic intravenously in the first scenario and intranasally in the second scenario. Participants allocated to sequence IN/IV administered the simulated analgesic intranasally in the first scenario and intravenously in the second scenario. A single member of the research group was responsible for generating the randomization list, enrolling participants, and assigning participants to the interventions.
Blinding
This was an open-label trial because blinding of route of administration was impossible both for participants and for outcome assessors.
Data Collection and Management
All data were collected on paper case report forms during a single visit and subsequently entered into Castor EDC (Ciwit B.V., Amsterdam, Netherlands). Data were collected and processed in accordance with General Data Protection Regulation (EU) 2016/679, good clinical practice, and other relevant regulations. Subject data were coded and stored for 5 y according to local regulations.
Statistical Methods
Statistical analysis was conducted using R version 4.3.3 (R Core Team 2025). Assessment of normality was performed using visual inspection of histograms and Q–Q plots, normality tests, and calculation of skewness and kurtosis.
Categorical variables were presented as counts with percentages. Continuous variables were presented as mean with 95% confidence intervals (CIs) when normally distributed and median with interquartile range (IQR) and minimum-maximum when nonnormally distributed. All outcomes were continuous and paired. When paired differences in outcome were normally distributed, the paired t test was used. When paired differences in outcome were nonnormally distributed, either the Wilcoxon signed-rank test or the sign test was used depending on symmetry of the distribution. A p value of <0.05 was considered statistically significant. Analyses were performed based on the intention-to-treat principle, including all randomized subjects. Missing data for the primary outcome were handled by multiple imputation.
Crossover trials have a concern for carry-over and period effects. Although carry-over effects were not applicable for this study, there could have been a learning effect, with time required for administration of analgesia decreasing with repetition of scenarios. In a 2×2 crossover design with equal numbers of participants allocated to each sequence, on average, the period effect will not bias the estimate of the treatment effect. 7 Therefore, we have not adjusted for period effects.
Sample Size Calculation
Sample size was calculated using nQuery version 8.5.1 (Statsols, Cork, Ireland) for a 2×2 crossover design to detect a minimum mean difference in time required for administration of 3.0 min using an expected standard deviation of the differences of 2.8 min, significance level of 0.05, and power of 90%. 11 This resulted in a required sample size of 6 subjects per sequence (12 subjects in total). To account for possible nonnormality of the distribution of our primary outcome and loss of statistical power with nonparametric statistical testing, we increased our sample size by 30%, which resulted in 8 subjects per sequence (16 subjects in total).
Onset of pain relief is slower after IN administration than after IV administration. For IN administration to be clinically useful, this delay should be at least compensated in part by the possibility of earlier administration. For fentanyl, which is standard of care in civilian and military prehospital care, onset of patient-reported meaningful pain relief was 5 min slower after IN administration than after IV administration. 12 A minimum mean difference in time required for administration of 3 min in favor of IN administration would compensate a substantial part of the delay in onset after administration.
Results
Participants were recruited between March 2024 and September 2024. Sixteen participants were included and randomized. Eight participants were allocated to sequence IN/IV and 8 participants to sequence IV/IN. All participants completed the study and were included in the analysis. Baseline characteristics are presented in Table 1.
Baseline Characteristics.
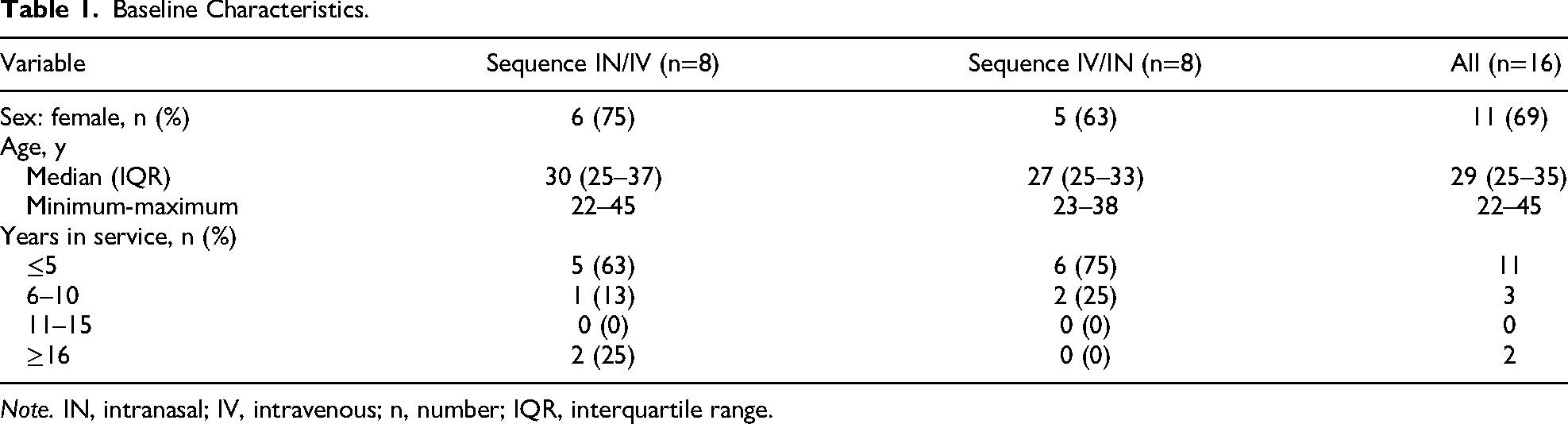
Note. IN, intranasal; IV, intravenous; n, number; IQR, interquartile range.
Primary Outcome
Mean time required from preparation until completed administration of the simulated analgesic was 4.8 min (95% CI 4.2–5.5) for IV administration and 1.9 min (95% CI 1.6–2.3) for IN administration (Table 2, Figure 2). IV administration required significantly longer than IN administration: mean difference 2.9 min (95% CI 2.4–3.4, p<0.0001).
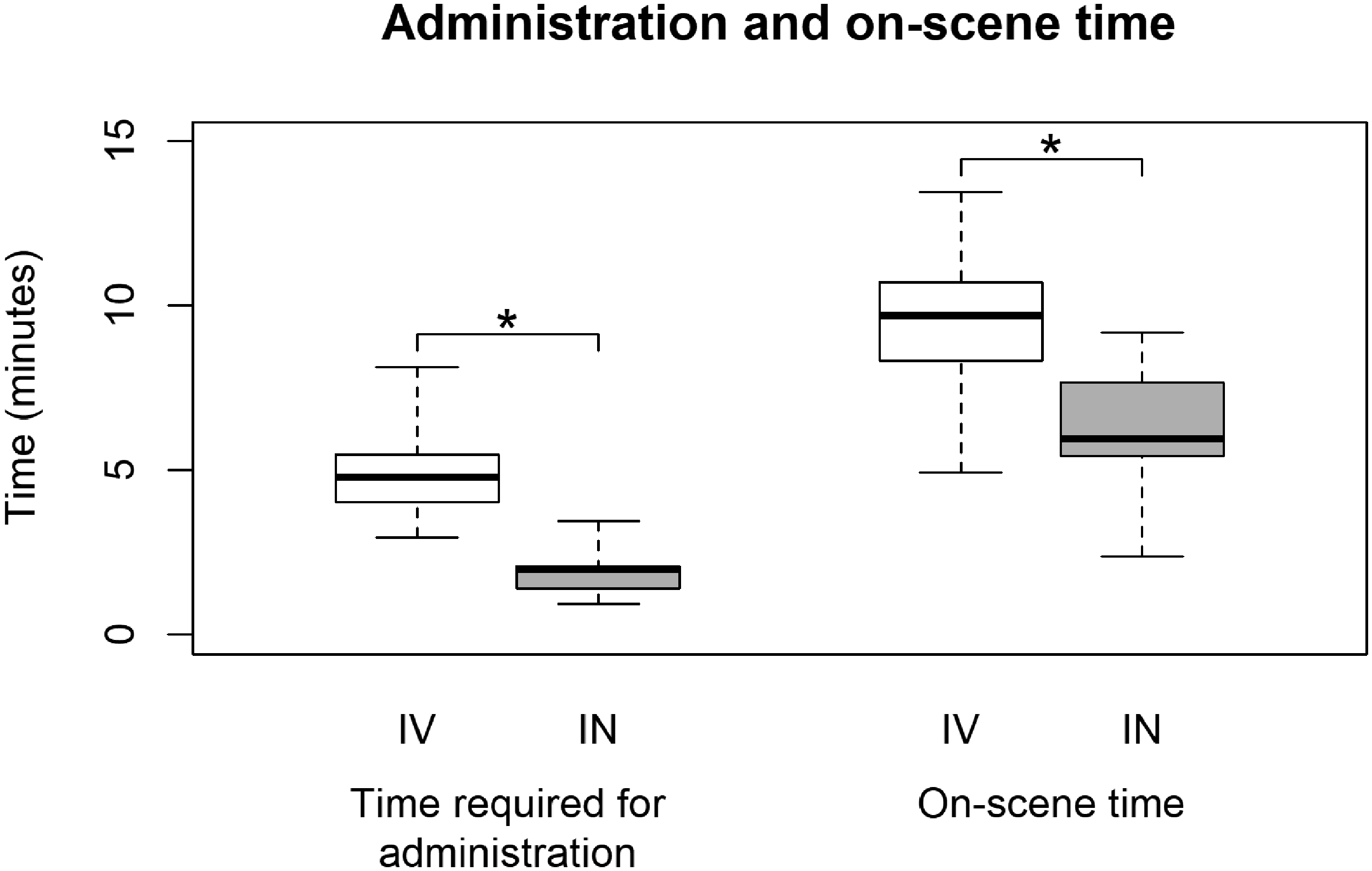
Boxplots of administration and on-scene time for IV and IN administration. Boxes represent the interquartile range (Q1–Q3), with the median indicated by a horizontal line. Whiskers extend to the minimum and maximum observed values IN, intranasal; IV, intravenous. *p<0.0001.
Primary and Secondary Outcomes.
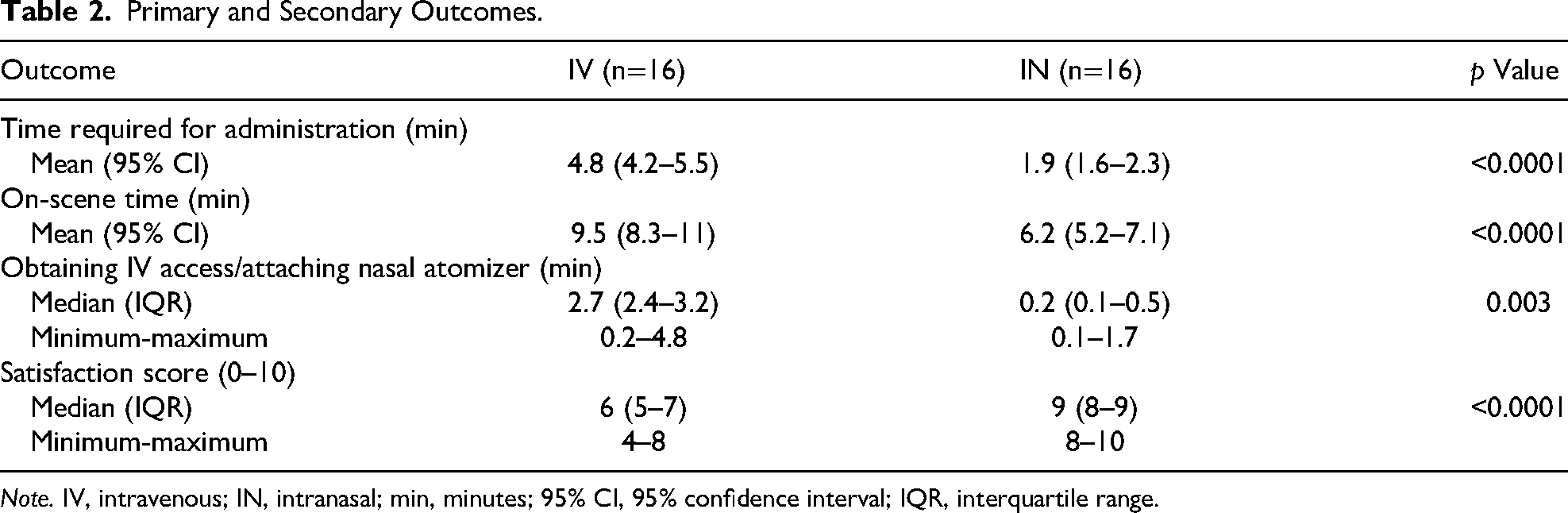
Note. IV, intravenous; IN, intranasal; min, minutes; 95% CI, 95% confidence interval; IQR, interquartile range.
Secondary Outcomes
Secondary outcomes are presented in Table 2. On-scene time was significantly longer for IV administration than for IN administration: mean difference 3.3 min (95% CI 2.5–4.1, p<0.0001; Figure 2). Time required for obtaining IV access was longer than for attaching the nasal atomizer (p=0.003). Satisfaction scores were lower for IV administration than for IN administration (p<0.0001).
Discussion
This randomized controlled trial aimed to determine the time required for IV and IN analgesia administration by military nurses in simulated prehospital trauma care scenarios. The difference of 2.9 min in favor of IN administration confirms our hypothesis that IN administration is faster than IV administration. Satisfaction scores were lower for IV administration than for IN administration.
Although onset of action after IN administration is delayed compared with IV administration, our findings show that this is compensated in part by the possibility of earlier administration. For fentanyl, the difference of 2.9 min compensates a considerable part of the 5-min delay in onset after IN administration. This might be considered relevant for situations where obtaining IV access is challenging, such as in combat casualty care and wilderness medicine. An earlier classroom-based study comparing times required for administration of naloxone by advanced paramedic trainees between IV and IN administration found a mean difference of 91 s (95% CI 55–127) in favor of IN administration. 6 Assuming that civilian EMS personnel are more experienced and proficient in obtaining IV access than military nurses, the 2-fold greater time difference observed in our study is not surprising. Similarly, wilderness medicine can be provided by a variety of healthcare providers who may be less experienced and proficient in obtaining IV access than civilian EMS personnel. Therefore, our results are also relevant beyond the military prehospital healthcare provider and environment, although the limited sample warrants confirmation of our findings across a broader range of healthcare provider backgrounds.
It should be mentioned that the results of our simulation study may be a conservative estimate of the difference in times required for IV and IN administration. Austere prehospital environments present many challenges that were only partly replicated in our study. We did not assess the degree of physical, conceptual, and emotional realism as experienced by participants. Realistic scenarios improve participant engagement, leading to valid decision making and behavior. 13 It is likely that our scenarios did not fully capture the complexity, urgency, emotional stress, and chaos of the austere prehospital environment. Consequently, it is not unreasonable to assume that obtaining IV access may be more time consuming in reality. We believe that the time required for IN administration likely would be less affected. Therefore, the time difference of 2.9 min between IN and IV administration may be greater in actual austere prehospital settings, and the total time to analgesia with fentanyl intranasally may approach that of fentanyl intravenously in real-world austere environments.
Beyond improved speed of administration, satisfaction scores also were higher for IN administration. We did not investigate the underlying reasons for this difference. Satisfaction may represent a composite outcome influenced by factors such as ease and speed of administration, perceived efficacy, and logistical advantages. Future studies should further evaluate which factors contribute most to healthcare provider satisfaction with prehospital analgesia administration.
It should be reiterated that the target population of this study is trauma patients without a need for immediate IV access for other reasons than analgesia, most importantly administration of fluids such as blood products. Our results should not be interpreted as a call to postpone obtaining IV access in patients who require fluid resuscitation for hemorrhage. Our findings do, however, have relevance for the subset of trauma patients who are in pain but in whom IV access can be delayed.
This study has some limitations. First, this is a simulation study that lacks the complexity and chaos of an actual prehospital environment. Second, participants were aware that the aim of the study was to compare the times required for IV and IN administration. We believe that this actually improves the validity of our results because participants’ awareness that administration time was being measured introduced some of the performance pressure and stress one normally experiences in prehospital trauma care. Third, our scenarios were designed to incorporate some of the challenges associated with obtaining IV access in the prehospital environment, such as suboptimal patient access and limited lighting. However, the prehospital environment similarly may present challenges for IN administration, including suboptimal patient positioning and limited patient cooperation. Future studies should include a broader range of environmental and patient-related factors to further evaluate the time difference between IV and IN administration. Finally, our study does not evaluate the clinical efficacy and safety of IN analgesia. Although IN fentanyl and (es)ketamine are already standard of care in civilian and military prehospital guidelines, there is limited high-quality evidence considering efficacy and safety endpoints.14,15 An earlier retrospective study in the prehospital environment has suggested that IN fentanyl may be effective as soon as 5 min after administration. 16 However, more high-quality evidence in this area is required.
This study has several strengths. Most important, the use of a crossover design allowed for within-participant comparison, reducing variability caused by differences between participants and thereby increasing statistical power. Second, using a high-fidelity mannequin allowed for realistic administration of medication (eg, enabling flashback of blood into the cannula chamber when obtaining IV access). Third, employing simulation and scripted scenarios resulted in standardization and enabled us to answer a question that cannot be answered in clinical practice in a feasible, safe, and timely fashion.
Conclusions
Administration of a simulated analgesic required 2.9 min longer for IV administration than for IN administration when performed by military nurses in simulated prehospital trauma care scenarios. On-scene times were longer and participant satisfaction scores were lower for IV than for IN administration. Healthcare providers working in the prehospital environment should be equipped with analgesics suited for IN administration.
Supplemental Material
sj-docx-1-wem-10.1177_10806032261460872 - Supplemental material for Time Required for Intranasal and Intravenous Analgesia Administration by Military Nurses in Simulated Trauma Care Scenarios: A Crossover Randomized, Controlled Trial
Supplemental material, sj-docx-1-wem-10.1177_10806032261460872 for Time Required for Intranasal and Intravenous Analgesia Administration by Military Nurses in Simulated Trauma Care Scenarios: A Crossover Randomized, Controlled Trial by Midas N. de Grunt, Nurseda Risvanoglu, Sterre Coenradie, Markus W. Hollmann, Milan L. Ridderikhof and Robert P. Weenink in Wilderness & Environmental Medicine
Footnotes
ORCID iDs
Ethical Considerations
The Institutional Review Board of the Amsterdam UMC confirmed that the Medical Research Involving Human Subjects Act did not apply to this study (Waiver No. 2023.0492, July 20, 2023) because participants were not subject to procedures or required to follow rules of behavior as documented in the Medical Research Involving Human Subjects Act.
Consent to Participate
Written informed consent was obtained from all participants.
Author Contributions
Financial/Material Support
This trial was funded by the Netherlands Military Healthcare Insurance Foundation (Stichting Ziektekosten Verzekering Krijgsmacht) under Grant No. 22-0024. The funder was not involved in the study design, data collection, analysis, interpretation, or writing of the report and did not participate in the decision to submit the manuscript for publication.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Anonymized participant data are available on reasonable request. Requests should be directed to the corresponding author and must be accompanied by a detailed research protocol. The corresponding author will evaluate the request and determine data availability based on the provided documentation and intended use.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.