
Abstract
Artificial intelligence (AI) is transforming wilderness Search and Rescue (SAR), where time constraints, austere conditions, and limited personnel have historically defined outcomes. This narrative review synthesizes the current evidence for AI applications in SAR, drawing on parallel developments in prehospital Emergency Medical Services (EMS) to illuminate the field's trajectory. This article is the result of searching PubMed, IEEE Xplore, Scopus, and Google Scholar from 2018 through March 2026 using combinations of “artificial intelligence,” “machine learning,” “search and rescue,” “unmanned aerial vehicle,” “wilderness medicine,” and “prehospital care.” Operational reports and trade publications were included when peer-reviewed sources were unavailable for deployed SAR technologies. Findings were organized under 3 temporal frameworks: operationally deployed, demonstrated capability approaching scale, and credible near-to-medium-term projection. AI-enabled unmanned aerial vehicles with thermal imaging and computer vision are operationally deployed in wilderness SAR, with field-validated rescues demonstrating detection through canopy, darkness, and adverse weather. Deep reinforcement learning algorithms for autonomous search-path optimization achieve more than 160% improvement over conventional coverage methods. However, the prehospital EMS literature provides an essential cautionary lesson: The Blomberg randomized, controlled trial showed that even technically superior AI may fail to improve outcomes without careful attention to human-AI interaction design and workflow integration. AI appears to be contributing to successful SAR outcomes and has been associated with several documented live rescues. Near-term priorities include prospective outcome validation, swarm-drone coordination, large language model-assisted wilderness medical protocols, and sustainable funding models for volunteer SAR organizations.
Keywords
Introduction
Wilderness Search and Rescue (SAR) operates under constraints that make it one of the most challenging domains in emergency response: limited personnel, communication degradation, terrain inaccessibility, weather extremes, and a relentlessly narrowing survival window. In the United States alone, the National Park Service logs >4000 SAR incidents annually, 1 and based on the author's experience as a member of the volunteer Southern Arizona Rescue Association (personal observations, 1982–2008), such volunteer teams conduct dozens of missions annually in desert terrain where daytime temperatures can exceed 43°C. 2 Such heat sharply compresses the narrowing survival window noted above: Dehydration, exertional heat illness, and heatstroke can convert a survivable exposure into a fatal one within hours, so the time available to reach a lost subject is often far shorter than terrain and distance alone would suggest.
Artificial intelligence (AI)—which encompasses machine learning (ML), deep learning, computer vision, natural language processing, and reinforcement learning—is rapidly reshaping SAR, with autonomous drones, machine-vision detection, and decision-support tools moving from research demonstrations into routine field operations within the past several years (Table 1). This review synthesizes the current evidence base, near-term operational capabilities, and projected trajectories for AI in wilderness SAR. Because SAR shares operational characteristics with prehospital Emergency Medical Services (EMS)—including time-critical intervention, austere conditions, and resource scarcity—key developments in prehospital AI are used to illuminate translational opportunities and cautionary lessons.
Selected Technical Terms Related to Search and Rescue Use of Artificial Intelligence.
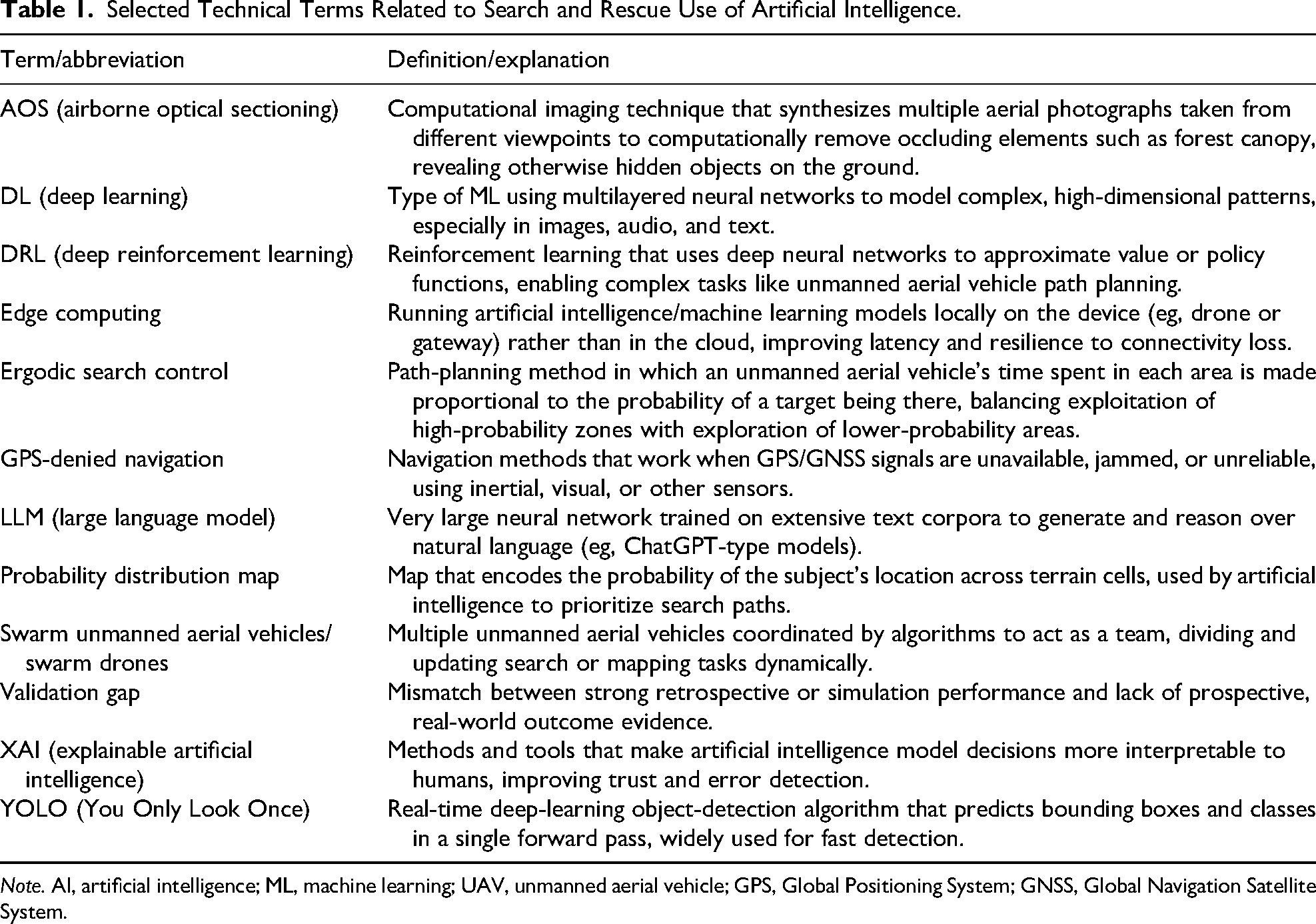
Note. AI, artificial intelligence; ML, machine learning; UAV, unmanned aerial vehicle; GPS, Global Positioning System; GNSS, Global Navigation Satellite System.
This review is organized under 3 temporal frameworks: operationally deployed (ie, current evidence-based deployment), demonstrated capability (ie, capability approaching operational scale), and near-term projections (ie, credible near-to-medium-term projection) (Figure 1).
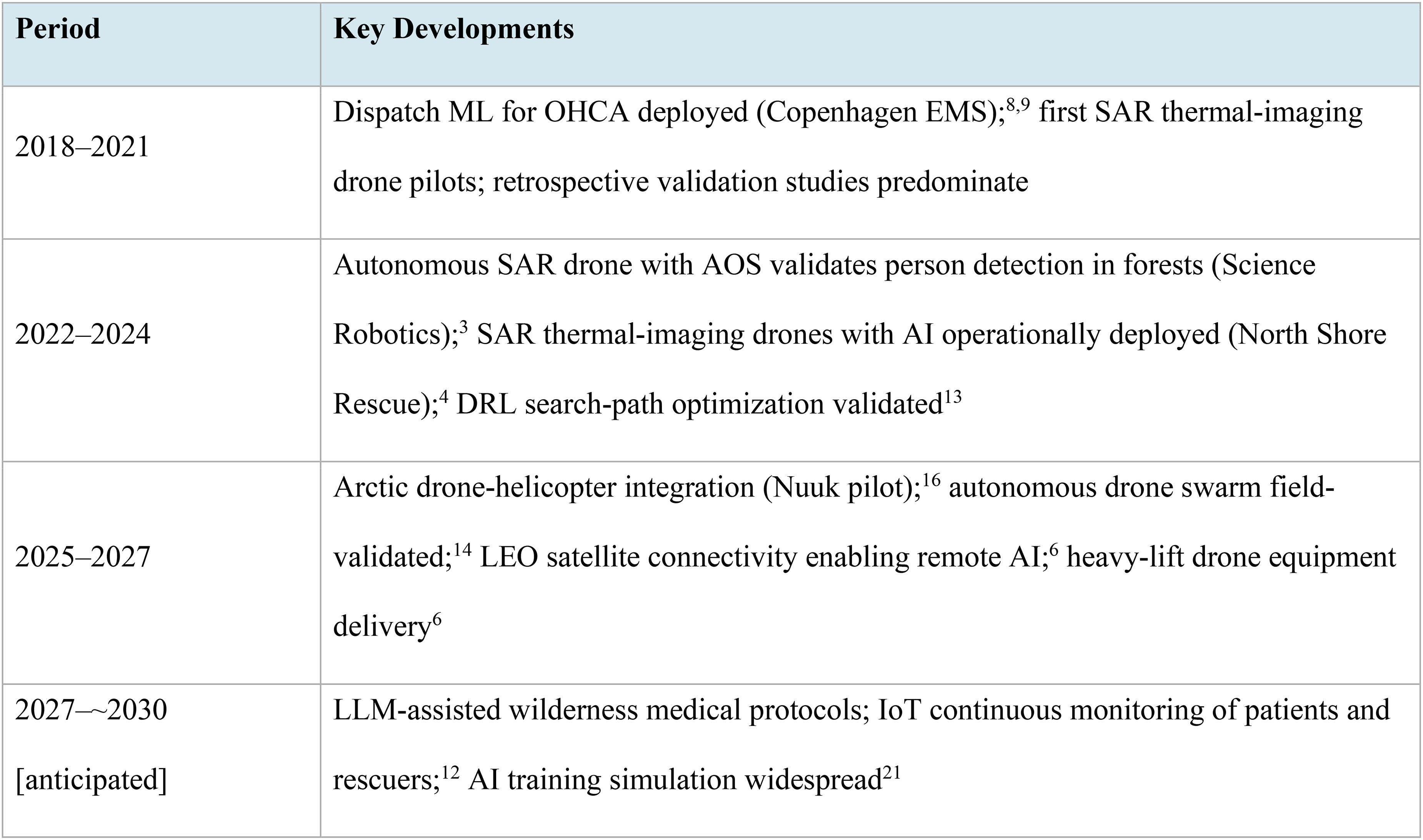
Development timeline: Artificial intelligence in wilderness Search and Rescue (2018 to ∼2030 [anticipated]).
Methods
This review is a narrative synthesis of the literature on AI applications in wilderness SAR and parallel prehospital EMS domains. It resulted from searching PubMed, IEEE Xplore, Scopus, and Google Scholar using combinations of the terms “artificial intelligence,” “machine learning,” “deep learning,” “search and rescue,” “unmanned aerial vehicle,” “wilderness medicine,” and “prehospital care.” Publication dates were limited to January 2018 through March 2026. The January 2018 start date was chosen because it follows the maturation of modern deep-learning frameworks (eg, TensorFlow [2015] and PyTorch [2016]) and corresponds with the first peer-reviewed publications applying these methods to unmanned aerial vehicles (UAV)-based SAR, after which the relevant literature expanded substantially. Reference lists of included studies were screened for additional relevant publications. No language restrictions were applied.
This review includes peer-reviewed original research, scoping reviews, systematic reviews, and randomized, controlled trials (RCTs). Because operational SAR AI deployment currently outpaces the peer-reviewed literature, the search was supplemented with operational reports and trade publications when peer-reviewed sources for deployed technologies were unavailable; these sources are explicitly identified as such throughout. Such non-peer-reviewed sources were included only when they 1) named the specific SAR organization, agency, or manufacturer involved, 2) provided first-hand operational detail—an identified official, a mission date, or a location—rather than secondary commentary, 3) could be corroborated by at least 1 independent report or were consistent with the peer-reviewed principles cited elsewhere in this review, and 4) carried an identifiable author or publisher and a publication date. Sources that did not meet these criteria were used, if at all, only to convey context and were not treated as evidence of effectiveness. A systematic review methodology was not feasible given the heterogeneity of the evidence, which spans clinical trials, simulation studies, field experiments, and operational case reports.
Operationally Deployed
AI-Enabled UAVs: Thermal Imaging and Computer Vision
AI-enabled UAVs represent the most consequential current technology in wilderness SAR (Table 2). Schedl, Kurmi, and Bimber demonstrated in a landmark Science Robotics study that an autonomous drone using airborne optical sectioning (AOS)—a synthetic-aperture imaging technique that combines many photographs taken from slightly different aerial vantage points so that occluding foreground elements such as forest canopy blur out while a target on the ground, which appears at consistent ground coordinates across all images, remains in focus—could, when combined with deep-learning-based classification, locate persons hidden beneath dense forest canopy in a predefined flight path with 86% precision across 17 field experiments, finding 38 of 42 hidden subjects. 3 (AOS does not literally “see through” canopy; rather, the canopy is averaged out across viewpoints while the still target reinforces.) This peer-reviewed experimental validation established the scientific foundation for the operational deployments that followed.
Current and Emerging Artificial Intelligence Applications in Wilderness Search and Rescue.
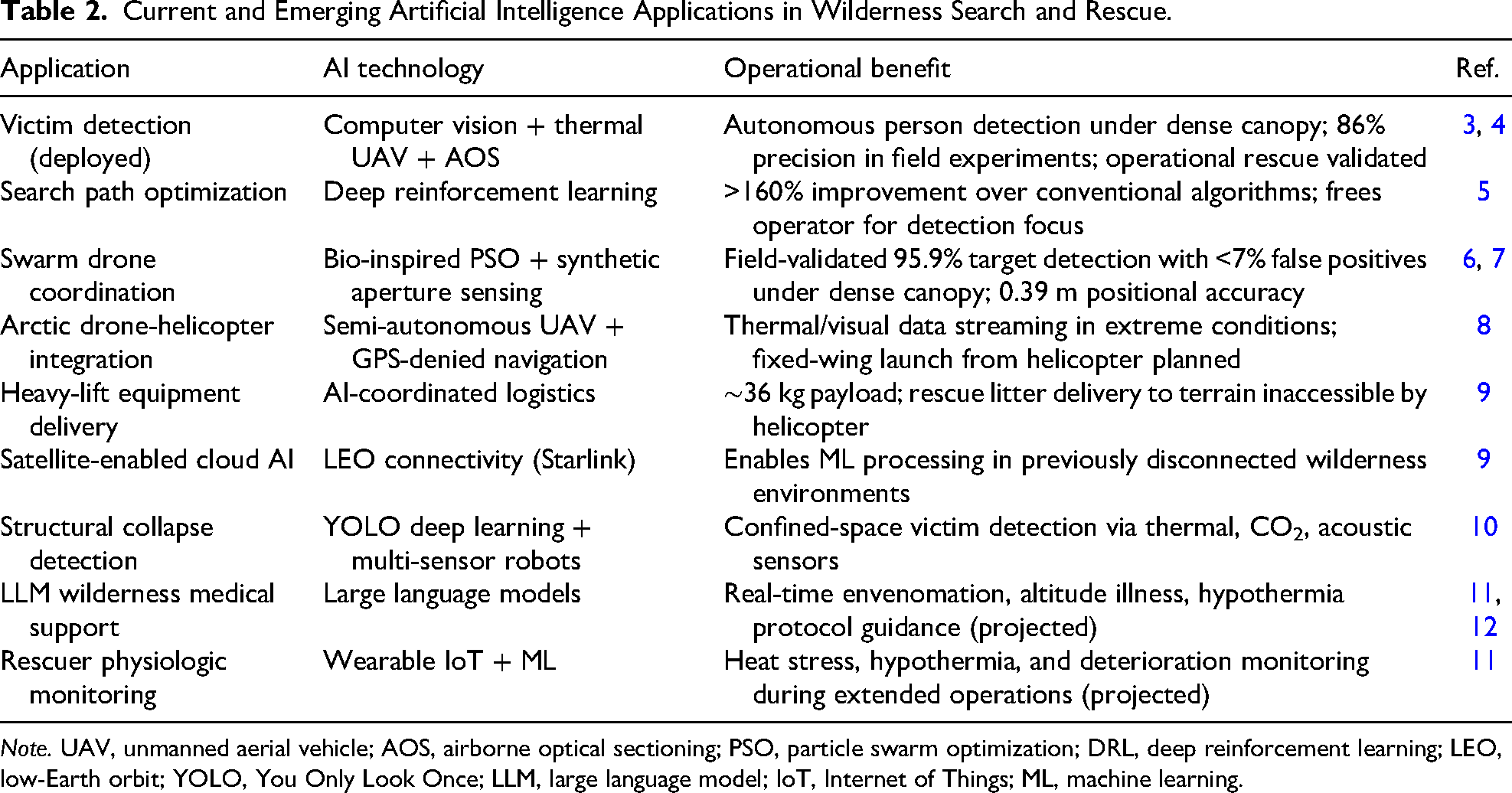
Note. UAV, unmanned aerial vehicle; AOS, airborne optical sectioning; PSO, particle swarm optimization; DRL, deep reinforcement learning; LEO, low-Earth orbit; YOLO, You Only Look Once; LLM, large language model; IoT, Internet of Things; ML, machine learning.
North Shore Rescue (NSR, North Vancouver, British Columbia), one of North America's busiest volunteer SAR teams, has deployed drones equipped with thermal cameras and computer vision software that analyzes each pixel in real time, detecting heat signatures, movement, and bright clothing even through partial canopy cover. In December 2024, the NSR team rescued a hypothermic hiker on Mount Seymour in −6°C conditions with dense rainforest canopy on the drone's last battery charge. According to the team leader, without the technology, the outcome would have been a body recovery rather than a live rescue. 4
AI eliminates a critical human limitation. Unlike a human observer, who must focus on one region at a time and whose attention degrades with fatigue, the AI system scans every pixel of every frame continuously across the full field of view without degradation. 13 Additional operationally documented deployments include Deschutes County SAR (Oregon) confirming human remains recovery from AI-generated coordinates; Weber County SAR (Utah) operating a 12-drone fleet for ∼$90,000 acquisition cost, compared with $7.2 million for a single rescue helicopter (and helicopter operating costs of $2000–$5000 per flight hour vs a few dollars per drone mission for batteries and routine maintenance); and an Italian rescue team locating a missing climber by flagging red pixels from the victim's helmet after nearly a year of searching. 9
Dumenčić et al provided experimental validation of a UAV search and detection system in a real Mediterranean wilderness environment using 78 volunteer subjects, demonstrating that integrated sensor-AI platforms using ergodic search control—a path-planning method in which the drone's time spent in each area is proportional to the probability of a target being there—can achieve reliable detection rates under field conditions rather than only in simulation. 14
Lessons from Prehospital EMS: The Validation Gap
Although wilderness SAR and prehospital EMS appear superficially distinct, the 2 fields share the operational features that determine whether an AI deployment ultimately helps or harms. Both must function in time-compressed, information-poor settings; both rely on a small number of human decision makers operating under high cognitive load; both involve a continuous chain of decisions in which an early classification error can propagate through the entire response; and both depend on AI outputs that must be interpreted and acted on in real time rather than reviewed later. For these reasons, prehospital EMS AI—where prospective trials and large implementation cohorts are more mature—provides the most relevant experiential analogue for what SAR teams should expect when they integrate AI into operations. The errors and absent statistical effects observed in prehospital EMS validation studies are therefore not peripheral curiosities but a direct warning about how SAR-AI tools may behave when they leave the simulator and enter the field.
The prehospital EMS literature provides essential context for evaluating SAR AI claims. The most mature prehospital AI application, ML-assisted dispatcher recognition of out-of-hospital cardiac arrest (OHCA), illustrates both the promise and the central challenge. Byrsell et al demonstrated that in retrospective analysis of >100,000 emergency calls in Stockholm, ML recognized 36% of OHCA cases within the first minute vs 25% for human dispatchers, with a mean 28-s speed advantage and improved sensitivity without an unacceptable rise in false positives. 15 However, the landmark Blomberg et al double-masked RCT (169,049 calls, Copenhagen EMS) found no statistically significant improvement in dispatcher OHCA recognition when ML alerts were provided vs suppressed, despite the same algorithm performing well retrospectively. 16
This pattern—in which AI demonstrated superior accuracy in retrospective analysis yet failed to improve patient outcomes when deployed prospectively in real time—represents the central cautionary finding for all prehospital and SAR AI technologies. The most widely cited example outside EMS is the Epic Sepsis Model, a proprietary prediction tool implemented at hundreds of US hospitals. When externally validated by Wong et al across nearly 40,000 hospital admissions, the model achieved an area under the curve of only 0.63 with 33% sensitivity at the manufacturer's recommended threshold and generated alerts on 18% of all hospitalized patients—performing far worse than the developer's retrospective results had suggested and contributing to substantial alert burden. 17 Several explanations have been proposed for this class of discrepancy. Alert fatigue may cause clinicians to discount or ignore frequent AI-generated notifications, particularly when work complexity is high and repeated alerts erode their informational value. 18 Cognitive friction—the added mental effort of interpreting and acting on AI recommendations during time-pressured tasks—may slow rather than aid decision making. Finally, high algorithmic sensitivity does not ensure workflow integration; a model that detects findings accurately in isolation may fail to improve outcomes if its outputs do not align with existing clinical or operational processes. A scoping review of 106 prehospital AI studies by Chee et al confirmed that most remain internally validated and retrospective, with rigorous prospective validation as the critical unmet need. 11 The same validation gap applies to SAR: While operational case reports and simulation studies are accumulating, prospective outcome data—find time, false-positive rates, and survival to definitive care—remain sparse, and SAR teams should treat retrospective performance as a hypothesis to be tested in the field rather than a guarantee.
Demonstrated Capability
Deep Reinforcement Learning for Search Path Optimization.
Ewers, Anderson, and Thomson (University of Glasgow) published a deep reinforcement learning (DRL) algorithm that generates optimized UAV search paths. The algorithm uses probability distribution maps—which encode the likelihood of a missing person's location across terrain cells based on their likely behavior—to guide the drone's flight path. The DRL approach outperformed conventional coverage planning algorithms—specifically the boustrophedon (“lawnmower”) sweep, spiral search, and local hill-climbing greedy-window methods that have long been standard in SAR doctrine—by >160% in search efficiency. 5 The operational context is Scottish Mountain Rescue and Police Scotland Air Support Unit, which are positioning drone fleets across Scotland for rapid deployment. Critically, the DRL system addresses the cognitive-load bottleneck: By automating the search path, it frees the drone operator to focus entirely on detection rather than simultaneously flying and analyzing the video feed.
Autonomous Drone Swarm Coordination
Amala Arokia Nathan et al, publishing in Communications Engineering (Nature), demonstrated a fully autonomous drone swarm capable of detecting and tracking targets occluded—that is, visually obstructed—by dense forest vegetation. The 6-drone swarm used a coordination algorithm modeled on collective animal behavior (decentralized rules in which each drone adjusts its position based on the behavior of its neighbors, analogous to bird flocking) and combined imagery from multiple drone positions using the same synthetic-aperture principle as AOS to reveal subjects hidden under canopy. In field experiments, the system correctly identified 95.9% of targets present, with a false-positive rate of <7% and positional accuracy within 0.39 m. 6 An earlier companion study established the simulation framework for swarm-based detection of these occluded targets in forested environments, demonstrating that adaptive swarm strategies—in which the drones dynamically redistribute themselves toward the most informative viewpoints—achieved maximum target visibility of 72% within 14 s, compared with 51% after 75 s for conventional fixed-pattern sampling. 7 These peer-reviewed results move swarm SAR from theoretical projection to demonstrated, field-validated capability.
Arctic Drone-Helicopter Integration
A September 2025 pilot study in Nuuk, Greenland, conducted by the University of Southern Denmark, the Alexandra Institute, and the Joint Arctic Command tested semi-autonomous drone integration with helicopter crews, streaming live thermal and visual data to guide aerial searches in areas with extreme cold, wind, and limited GPS coverage. 8 The next development phase aims for a fixed-wing SAR drone that is launchable and recoverable from a helicopter in midflight. Systems proven in Arctic conditions—such as navigation when GPS signals are unavailable, long-range data streaming, and extreme weather resilience—are directly applicable to mountain rescue, earthquake zones, wildfires, and collapsed-infrastructure scenarios.
Heavy-Lift Drones and Satellite Connectivity
Two enabling technologies are approaching operational maturity. Heavy-lift drone platforms (eg, DJI Flycart 30, a 16-blade, ∼36-kg payload capacity) have demonstrated remote delivery of rescue litters and medical equipment, a capability that could transform response in terrain inaccessible to helicopters. 9 Low-Earth orbit satellite internet (eg, Starlink Mini and equivalents) is closing the connectivity gap that has prevented cloud-based ML from operating in wilderness environments. This infrastructure development unlocks AI-enhanced SAR in precisely the remote environments where it is most needed. 9
AI-Enabled Snake Robots for Structural Collapse
AI-enabled snake (serpentine) robots are slender, multisegmented mobile robots whose articulated bodies allow them to enter rubble voids, pipes, and partially collapsed spaces that wheeled or legged robots cannot (Figure 2). They typically carry forward-looking infrared, a microphone, and carbon dioxide and video sensors and are paired with You Only Look Once (YOLO)-based deep-learning object-detection models—a family of algorithms that locate and classify objects in an image in a single rapid forward pass, fast enough to run on the limited compute available on a small mobile robot. A 2024 study found that YOLO-based models provide the best balance of speed and accuracy for real-time confined-space victim detection. 10 Although more relevant to urban SAR than wilderness SAR, this technology extends the AI rescue frontier into environments where neither drones nor humans can safely operate.

Example of a modular serpentine robot of the type adapted for confined-space Search and Rescue.
Near-Term Projections
LLM-Assisted Wilderness Medical Protocols
Large language models (LLMs)—AI systems trained on vast text collections to generate and reason over natural language—are well suited to the wilderness medicine context, where protocol ambiguity at the margins, rare presentations, toxic exposures requiring real-time toxicology consultation, multilingual patient interaction, and documentation burdens are common challenges. Consider a SAR team extracting a snakebite victim from a remote canyon. An LLM-based voice assistant could provide species-specific envenomation management updated to the latest evidence, support antivenom selection and dosing decisions for the receiving facility (recognizing that field SAR teams rarely carry antivenom themselves), assist with multilingual patient communication, and generate documentation, all while the team's hands are occupied with patient care. Similar applications for altitude illness, hypothermia rewarming, and marine envenomation represent credible near-term-use cases.11,12
These benefits must be weighed against well-documented risks. Contemporary general-purpose LLMs are prone to “hallucination”—the generation of plausible-sounding but factually incorrect output, including invented citations, fabricated drug doses, and confidently wrong clinical recommendations. In an adversarial assurance analysis of 6 leading LLMs across 300 physician-validated clinical vignettes, models repeated or elaborated on a single planted fabricated detail (eg, a nonexistent laboratory value or fictitious disease) in up to 83% of cases, with a simple corrective prompt only halving the error rate. 19 A clinician's guide published in the Interactive Journal of Medical Research catalogues additional failure modes, including stale training data, biased training corpora, and the model's tendency to favor confident, persuasive output over hedged uncertainty. 20 In the wilderness context—where the user is often a fatigued field provider with no Wi-Fi, no second opinion, and no time to verify—these failure modes are dangerous. Any LLM deployed in SAR therefore must be 1) restricted to validated reference content, ideally retrieval augmented from approved wilderness medicine protocols; 2) deployed with explicit hedging and source attribution; 3) audited for accuracy on a defined test set before each release; and 4) treated as a decision-support adjunct, not a replacement for trained clinical judgment.
Internet of Things Monitoring of Patients and Rescuers
Wearable sensor networks with ML analysis enable continuous physiologic monitoring in wilderness and disaster settings. For lost subjects, satellite-connected wearables (eg, heart rate, temperature, and GPS) can transmit data to the incident command post, enabling dynamic probability-of-survival mapping. For SAR team members, the same infrastructure monitors heat stress, hypothermia, and physiologic deterioration during extended operations—a significant occupational health advance for rescue teams operating in extreme environments such as the Sonoran Desert or alpine terrain. 11
AI in SAR Training and Simulation
A 2025 scoping review found that AI is already being used for EMS simulation, personalized learning, and disaster-preparedness training. 21 AI-generated scenarios can simulate wilderness injuries, cave rescues, avalanche incidents, and multicasualty events with endless variation and immediate performance feedback. An international Delphi consensus of EMS experts rated AI training applications among the highest anticipated changes by 2030. 22
Barriers to Implementation
Several barriers impede SAR's adoption of AI (Table 3). The most pressing for volunteer and municipal SAR teams is funding. AI-capable drone platforms range from $1000 to >$150,000 depending on specifications, yet most SAR organizations operate on minimal budgets. Regional shared-asset models, public-safety grant mechanisms, and manufacturer partnerships represent practical near-term pathways to acquire this technology. 9
Barriers to Artificial Intelligence Implementation in Wilderness Search and Rescue.
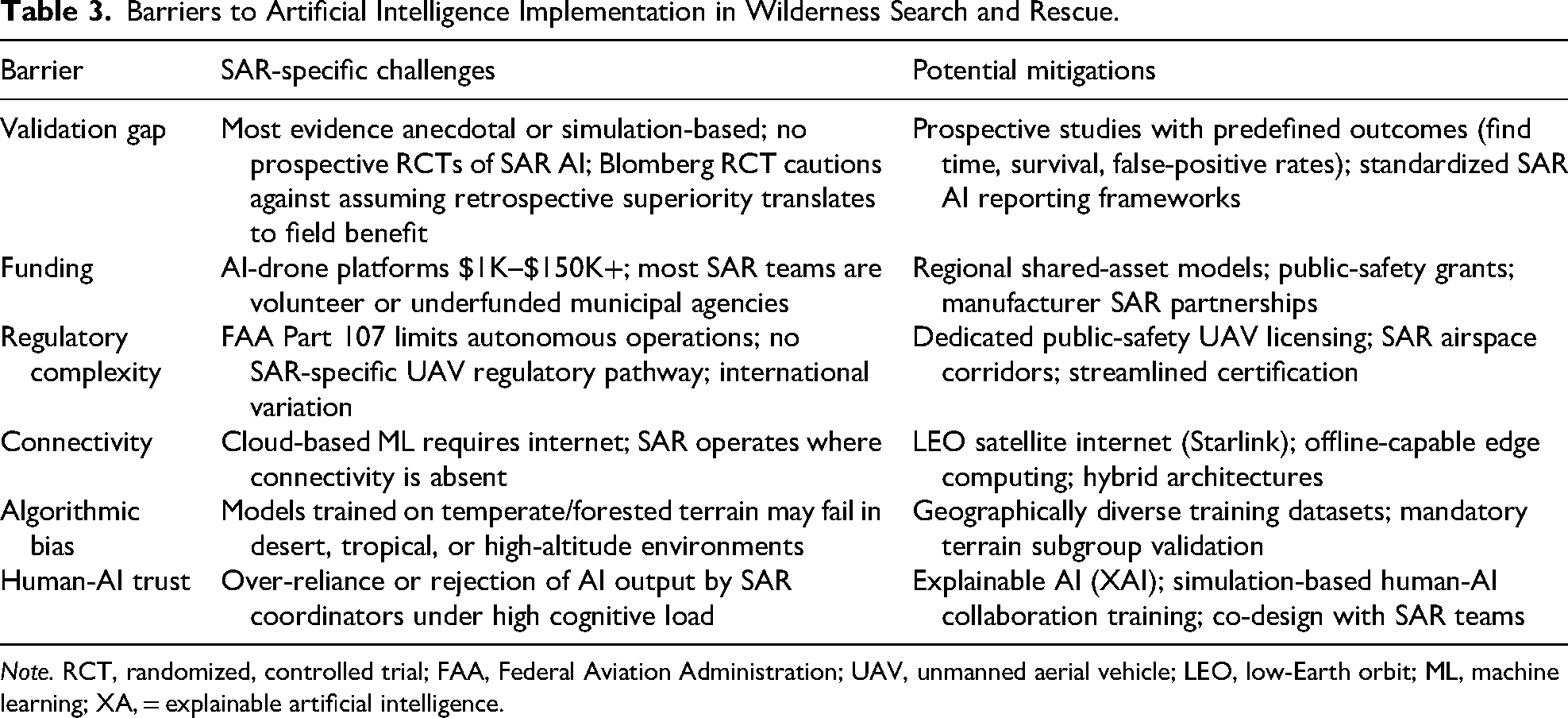
Note. RCT, randomized, controlled trial; FAA, Federal Aviation Administration; UAV, unmanned aerial vehicle; LEO, low-Earth orbit; ML, machine learning; XA, = explainable artificial intelligence.
The validation gap is equally critical. The Blomberg et al RCT—a double-masked trial of 169,049 emergency calls in Copenhagen in which dispatchers were randomized to receive or not receive a machine learning OHCA-recognition alert, with no statistically significant improvement in recognition observed—demonstrates that a technically superior AI system may fail to improve outcomes in the complex human context of emergency response. 16 Most SAR AI evidence is anecdotal or simulation based; prospective studies with predefined outcome measures (eg, find time, survival rates, and false-positive detection rates) are urgently needed.
Regulatory complexity further constrains operational flexibility. In the United States, Federal Aviation Administration (FAA) Part 107 certification limits autonomous operations and beyond-visual-line-of-sight (BVLOS) flight, both of which are central to long-range SAR work. The FAA published the Notice of Proposed Rulemaking for the new Part 108 BVLOS framework on August 7, 2025, with a final rule anticipated in 2026; if enacted as proposed, Part 108 will normalize routine BVLOS operations under a tiered permitting and certification structure, with expedited approvals for emergency response and public-safety operators.23,24 Dedicated public-safety UAV licensing pathways and SAR-specific airspace corridors would further accelerate deployment. Connectivity in austere environments—the defining operational challenge—is being addressed by low-Earth orbit satellite internet but remains incomplete. Finally, algorithmic bias is a concern: ML models trained on European or Pacific Northwest terrain and subject behavior data may underperform in desert, tropical, or high altitude environments.11,25
Ethical Dimensions
AI in SAR raises 3 primary ethical concerns: accountability, privacy, and trust. First is accountability. When SAR decisions are informed by AI—such as prioritizing 1 search sector over another or recommending mission suspension—and the outcome is adverse, the locus of responsibility (ie, algorithm developer, fleet operator, on-scene incident commander, or sponsoring agency) is unclear under current frameworks. Emergency medicine has been grappling with the same accountability gap as AI-driven decision support enters hospital practice, where comparable questions arise about clinician responsibility for following or overriding algorithmic advice, manufacturer liability for retrospective model performance not matching prospective field performance, and informed-consent obligations when AI shapes care.26,27
Second is surveillance and privacy. Thermal drones that detect lost subjects also may capture individuals in private settings adjacent to the search zone. Governance frameworks that translate generic civil-liberties principles into operational SAR rules are needed. At a minimum, these should specify data-minimization defaults (capture only the search corridor required for the mission), retention limits (purging nonevidentiary thermal and video footage within a defined postmission window), encryption of stored data, role-based access controls, an audit trail logging who viewed the footage and why, written use-of-force-style policies for the rare cases in which captured imagery may be shared with law enforcement, and clear public disclosure of agency practices28–30 Third is human-AI trust calibration. Overreliance on AI outputs is as dangerous as underreliance; both have been demonstrated in clinical decision-support studies. Kücking et al found that even when AI recommendations were deliberately incorrect, raters with higher perceived benefit of the AI agreed with the wrong recommendation at substantially higher rates, a phenomenon termed automation bias. 31 Dratsch et al showed the same pattern in mammography readers exposed to AI BI-RADS (Breast Imaging-Reporting and Data System) suggestions: Incorrect AI assessments significantly degraded reader performance. 32 The Blomberg RCT failure may partly reflect inadequately designed human-AI interaction. Explainable AI systems that reveal the reasoning behind recommendations, combined with simulation-based training for human-AI collaboration, are necessary to calibrate trust appropriately. 16
Results
Recommendations for SAR Organizations and Policy
Based on the evidence reviewed, the following priorities are suggested for SAR organizations, wilderness medicine societies, and policymakers.
For individual SAR teams: Organizations with limited budgets should prioritize thermal-imaging drones with AI-assisted detection software as the highest-impact, lowest-barrier current technology. A basic AI-capable drone platform can be acquired for <$10,000 in upfront cost; teams should budget separately for ongoing expenses, which typically include battery replacement and routine maintenance ($200–$500 per drone per year for a moderately used platform), Part 107 (and forthcoming Part 108) pilot training and recurrent testing (∼$150 for the initial knowledge test plus recurrent training every 24 months), AI detection software subscriptions where applicable (commonly $500–$2000 per year per organization), and an allowance for crew time. Emerging shared-asset models allow multiple teams to access advanced systems cooperatively. Teams also should invest in simulation-based training for human-AI collaboration to avoid the trust-calibration failures observed in the prehospital and broader clinical literature.31,32
For professional organizations (eg, Wilderness Medical Society, National Association for Search and Rescue, and Mountain Rescue Association), national organizations should advocate for dedicated public-safety UAV licensing pathways, SAR-specific airspace corridors, and federal grant mechanisms for AI-equipped SAR assets. Engagement with the FAA Part 108 rulemaking process is a near-term priority, particularly to secure favorable provisions for emergency-response operators. 23 Development of standardized SAR AI outcome-reporting frameworks analogous to the Utstein template for cardiac arrest research would accelerate the evidence base.
For researchers, prospective, outcome-driven studies with predefined endpoints (eg, time to find, survival rates, and false-positive detection rates) must replace retrospective simulation as the evidentiary standard. Geographically diverse validation datasets encompassing desert, tropical, alpine, and maritime environments are essential to address algorithmic bias. The wilderness medicine research community is well positioned to lead these efforts given its established multisite, multienvironment research infrastructure.
Limitations
This review has several limitations. As a narrative rather than systematic review, it is subject to selection bias in the literature included. Several key SAR AI deployments are documented only in trade publications and operational reports rather than peer-reviewed literature, reflecting the reality that field deployment is outpacing formal evaluation. The rapid pace of AI development means that specific technologies described here may evolve substantially between writing and publication. Finally, the prehospital EMS evidence used for translational context derives largely from high-income urban settings; its applicability to volunteer, rural, and international SAR contexts requires further study.
Conclusions
AI appears to be contributing to successful SAR outcomes and has been associated with several documented live rescues. Thermal-imaging drones with computer vision are operationally deployed and field validated, with peer-reviewed evidence demonstrating autonomous person detection through dense forest canopy. 3 DRL algorithms are optimizing search paths with dramatic efficiency gains, 5 autonomous drone swarms have achieved field-validated detection and tracking under canopy, 6 and enabling technologies such as satellite connectivity, heavy-lift drones, and Arctic integration platforms are closing operational gaps.
The prehospital EMS evidence provides both validation and caution. Integrated AI platforms demonstrate that real-time clinical decision support can reduce delays in austere, time-critical environments. 26 But the Blomberg RCT stands as the field's defining lesson: Even technically superior AI may fail to improve outcomes without careful attention to human-AI interaction design, workflow integration, and prospective validation. 16
For wilderness SAR organizations, AI simultaneously democratizes and differentiates capability. It multiplies the effectiveness of limited human teams but requires investment that many volunteer organizations cannot afford. Regional resource sharing, public-safety partnerships, and grant mechanisms represent policy priorities with direct life-safety implications. Prospective, outcome-driven research, rather than retrospective simulation, must be the evidentiary standard for the field.
In SAR, time is the irreversible currency. AI's singular contribution is compressing delays in detection, dispatch, routing, and clinical decision support. Every second recovered is survival probability regained.
Footnotes
Author Note
Kenneth V. Iserson, MD, MBA, FACEP, is Professor Emeritus of Emergency Medicine at the University of Arizona College of Medicine, Tucson. He has nearly 5 decades of clinical experience, has served as faculty at his university’s Level I trauma center and lead physician for the US Antarctic Program, and has practiced emergency medicine on all 7 continents. He is a 25+ y volunteer with the Southern Arizona Rescue Association and the author of nearly 400 peer-reviewed publications and >15 books on emergency medicine, medical education, bioethics, and wilderness medicine.
Author Contribution(s)
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Financial/Material Support
The author received no financial support for the research, authorship, and/or publication of this article.