
Abstract
Purpose:
This study aims to evaluate the effects of brimonidine eye drops and intravitreal administration in guinea pigs with form-deprivation myopia (FDM) and to analyze the ocular pharmacokinetics and irritation.
Methods:
The experimental guinea pigs were randomized to the normal control, FDM, FDM brimonidine topical eye drops, and FDM intravitreal injection groups. The experiment period was 13 days. Changes in ocular refraction and axial length were monitored regularly. The ocular pharmacokinetics of brimonidine and its metabolite brimonidine-2,3-dione were analyzed using ultra-performance liquid chromatography-tandem mass spectrometry. Ocular irritation was assessed by the Draize test, corneal fluorescein staining, and hematoxylin and eosin staining.
Results:
Two administration methods of brimonidine equally inhibited the increase in refraction and axial length in FDM guinea pigs (P < 0.05). Pharmacokinetic analysis revealed significant and sustained accumulation of brimonidine in the iris and choroid. Brimonidine was preferentially distributed to the cornea, conjunctiva, and sclera when administered topically, and preferentially to the retina and vitreous when administered intravitreally. The total area under the curve values for retinal and scleral tissues demonstrated that continuous topical administration was 1.95 times and 1.36 times that of intravitreal administration, respectively. The concentration of brimonidine-2,3-dione was significantly lower than that of brimonidine. Brimonidine topical eyedrops had less ocular irritation.
Conclusions:
At the drug concentrations in this study, both topical and intravitreal brimonidine achieved sufficient ocular exposure to exert similar myopia-suppressing effects. Continuous topical administration can maintain higher drug concentrations in the retinal and scleral tissues with less eye irritation.
Keywords
Introduction
The global prevalence of myopia has been steadily increasing in recent years, emerging as a significant public health concern. 1 In the year 2025, it is predicted that roughly five billion people worldwide will have myopia, with about one billion at high risk of progressing to high myopia. 2 Posterior staphyloma, choroidal neovascularization, and macular degeneration caused by high myopia can lead to irreversible visual impairment and bring a huge economic burden. 3
Currently, there is no definitive cure for myopia. Pharmacological therapy is an important strategy for myopia prevention and control. It has advantages such as early and efficient prevention and control, convenience, and high compliance. 4 Brimonidine, a highly selective alpha-2 adrenergic agonist, is utilized to lower intraocular pressure in the treatment of glaucoma and exhibits neuroprotective properties. 5 In different animal myopia models, brimonidine can suppress the progression of myopia. Liu et al. found that in lens-induced myopia (LIM) guinea pigs, brimonidine eye drops at concentrations of 0.1% and 0.2% effectively slowed the progression of myopia. 6 Carr et al. demonstrated that brimonidine intravitreal administration can inhibit axial length elongation in chicks with form-deprivation myopia (FDM). 7 Recent research indicated that brimonidine administered via local or intravitreal injection can mitigate myopic development in the FDM guinea pig model. 8
Brimonidine concentrations need to be in the effective range to slow myopia progression when administered topically or intravitreally.8,9 Insufficient concentrations of brimonidine may fail to adequately activate alpha-2 adrenergic receptors and G proteins to reach the threshold for effective treatment. Conversely, excessive concentrations of brimonidine may lead to receptor saturation or trigger G protein-mediated negative feedback regulation mechanisms, thus weakening the efficacy.9,10 Therefore, achieving effective therapeutic concentrations of brimonidine in ocular tissues is critical for its ability to inhibit myopia development. However, the concentration distribution and pharmacokinetic (PK) characteristics of brimonidine in ocular tissues remain unclear when brimonidine exerts its myopia-suppressive effect.
Brimonidine is an amphiphilic drug with both lipophilic and hydrophilic properties. Intraocular brimonidine can be oxidized and metabolized by aldehyde oxidase (AOX) to brimonidine-2,3-dione. 11 This study evaluated the effects of brimonidine eye drops and intravitreal injection on axial length and refractive power in FDM guinea pigs. When brimonidine is administered in two ways to produce an inhibitory effect on myopia, the PK of brimonidine and its metabolite brimonidine-2,3-dione, were analyzed using ultra-performance liquid chromatography-tandem mass spectrometry (UPLC-MS/MS). Furthermore, we also evaluated the ocular tissue irritation of two dosing regimens of brimonidine. This study provided experimental evidence and PK data to support the efficacy and safety of brimonidine for myopia control.
Methods
Animals
Three-colored guinea pigs (n = 120) were purchased from Xi’an Yifengda Biotechnology Co., Ltd. (Xi’an, China). Selection criteria were the age of three weeks, male sex, and body weight of 100–150 g. Before the experiment began, guinea pigs with eye diseases such as congenital myopia, lens opacity, keratitis, and corneal leukoma were excluded. All guinea pigs were maintained under constant temperature conditions (24 ± 1°C) and 300 lux illumination with a light-dark cycle of 12/12 h. Animals were provided with ample food, water, and fresh vegetables. All experimental procedures involving animals strictly adhere to the Association for Research in Vision and Ophthalmology statement on the use of animals in ophthalmic and vision research.
Experimental design
Animals were randomly divided into four groups: normal control group (NC, n = 30), FDM group (FDM, n = 30), FDM brimonidine topical eye drops group (FDM + Topical eye drops, n = 30), and FDM brimonidine intravitreal injection group (FDM+IVI, n = 30). The NC group received no treatment, while the remaining three groups underwent form deprivation in the right eye using an opaque balloon mask. Guinea pigs in the FDM + Topical eye drops group received 5 μL of brimonidine (80 μg/μL) in the right eye twice daily. Animals in the FDM+IVI group received a single intravitreal injection of 5 μL brimonidine (4 μg/μL) in the right eye every 96 h. Refraction and axial length were monitored in all groups. The Draize test and corneal fluorescein staining (CFS) were performed regularly to evaluate the ocular surface status. Following 13 days of continuous treatment, ocular samples were collected for PK analysis and hematoxylin and eosin (H&E) staining.
Induction of form-deprivation myopia
Monocular form deprivation was induced in guinea pigs by covering the right eye with a 10-cm opaque latex balloon, ensuring no pressure was exerted on the eyelid or cornea. The left eye, ears, nose, and mouth remained fully exposed to allow for normal activity and feeding. We checked the balloon multiple times a day to ensure it covered the right eye and cleaned it promptly.
Drug preparation and administration
Brimonidine tartrate (MedChemExpress, Shanghai, China) was dissolved in phosphate buffer saline (Wuhan Pricella Biotechnology Co., Ltd., Wuhan, China)to prepare the corresponding concentration. In the FDM + Topical eye drops group, 5 μL of brimonidine solution (80 μg/μL) was instilled into the conjunctival sac of the guinea pigs at 8 am and 8 pm daily. Using the Hamilton microsyringe, 5 μL of brimonidine solution (4 μg/μL) was injected into the vitreous body at a location approximately 2 mm posterior to the superior temporal corneal limbus.
Diopter and axial length measurements
Refraction diopters were measured in dark environments with a hand-held streak retinoscopy (YZ24B, 66 Vision-Tech, China). The same experienced optometrist conducted all measurements. Before examination, cycloplegia and full pupillary dilation were achieved through the topical administration of 0.5% tropicamide eye drops. The mean spherical equivalent was calculated based on three repeated measurements per eye. Following local anesthesia with 0.4% oxybuprocaine hydrochloride eye drops, axial length was measured using A-scan ultrasonography (AXIS II, Quantel Medical, France). The A-scan probe was gently placed in a vertical position on the central cornea to avoid depressing the cornea. The measurements of both eyes were repeated five times to record the average value of the axial length.
Sample preparation
Guinea pigs were sacrificed with an overdose of sodium pentobarbital (100 mg/kg). Guinea pigs were sampled before and 0.5, 1, 2, 4, 8, 12, 24, or 96 h after the last administration. Each group randomly selected the right eyeball of three guinea pigs at each time point. In pre-cooled phosphate buffer saline, the cornea, conjunctiva, aqueous humor, iris, lens, and vitreous body were removed in sequence. The transparent retina, dark brown choroid, and white sclera were gently and bluntly separated using microscopic instruments. All tissue samples were immediately immersed in liquid nitrogen for 10 min and then transferred to a −80°C refrigerator for subsequent experiments.
UPLC-MS/MS
About 0.13 M hydrochloric acid was added to the eye tissue sample, followed by the addition of 50 µL of the internal standard working solution (10 µg/mL). Brimonidine standard (purity >98%) and brimonidine-2,3-dione standard (purity >98%) were purchased from Shanghai Yuanye Biotechnology Co., Ltd. (Shanghai, China). Tissue homogenate was obtained using a Precellys® Evolution homogenizer (Bertin Technologies, France). By adding 5 mL of acetonitrile to the tissue homogenate, followed by vortexing and centrifugation, the supernatant can be obtained. The supernatant evaporated to dryness under nitrogen at 40°C. The sample solution was reconstituted with acetonitrile solution and filtered through a 0.22 μm microporous filter membrane for analysis.
The analysis was performed using an ultra-high performance liquid chromatography triple quadrupole mass spectrometry (Triple Quad 6500+) and a Waters Acquity UPLC BEH C18 column (2.1 × 100 mm, 1.7 μm). Mass spectrometry data were analyzed using Analyst® (version 1.7.3, AB Sciex, USA).
Pharmacokinetics analysis
The PK parameters of drugs were calculated using the non-compartmental model analysis tool of Phoenix WinNonlin software (version 8.0). PK parameters include the maximum observed concentration (Cmax), the time of observed maximum concentration (Tmax), the area under the curve from time zero until the last sampling point (AUC0-t), the area under the curve from time zero to infinity (AUC0-∞), the elimination half-life (T1/2), and the elimination rate constant (Ke). For aqueous humor, the concentration was measured as ng/mL. For other ocular tissues, the concentrations were measured as ng/mg.
Ocular irritation assessment
The Draize test was used to assess the degree of ocular irritation. 12 The cornea, conjunctiva, and iris of guinea pigs were monitored daily before drug administration using a slit lamp (YZ 2, Suzhou, China) for 13 consecutive days. CFS was performed using ocular surface corneal and conjunctival staining test strips (Liaoning Meizilin Pharmaceutical Co., Ltd., Liaoning, China) at baseline and on the second, sixth, and tenth days after administration. Staining results were scored using the Oxford scoring method. 13 After the final administration, all guinea pigs were euthanized with an overdose of pentobarbital sodium. The right eyes were then enucleated and processed into frozen sections at a thickness of 8 μm. The frozen sections were fixed with 4% paraformaldehyde (Servicebio, Wuhan, China) for 15 min and then stained with H&E (Beyotime, Shanghai, China). The Nikon Eclipse E800 microscope (Nikon Corp, Tokyo, Japan) was employed to capture the images.
Statistical analysis
Statistical analysis was performed using SPSS 26.0 software, and the values were recorded as mean ± standard deviation. Two-way repeated measures (ANOVA) and Bonferroni multiple comparisons were used to analyze differences between groups. A P value of <0.05 was defined as statistically significant.
Results
Effects of topical eye drops and intravitreal injection of brimonidine on FDM in Guinea pigs
The experimental workflow is outlined (Fig. 1A). Before form deprivation-induced myopia, there was no significant statistical difference in baseline refraction and axial length between the groups (P > 0.05). Following the induction of FDM, the interocular differences in refraction (P < 0.05) and axial length (P < 0.01) in the FDM group were greater than those in the NC group at day 7. On day 13, the difference between the FDM and NC groups was more significant. The changes in refractive power and axial length between eyes in the brimonidine topical eye drops and intravitreal injection groups were lower than the FDM group (all P < 0.01, Fig. 1B, C). The interocular differences in refraction and axial length at different time points and the pairwise comparison between the groups are shown in Supplementary Table S1. Monitoring the changes in axial length and refractive power in each group revealed that topical eye drops and intravitreal administration of brimonidine for 13 days effectively suppressed myopia development in FDM guinea pigs.
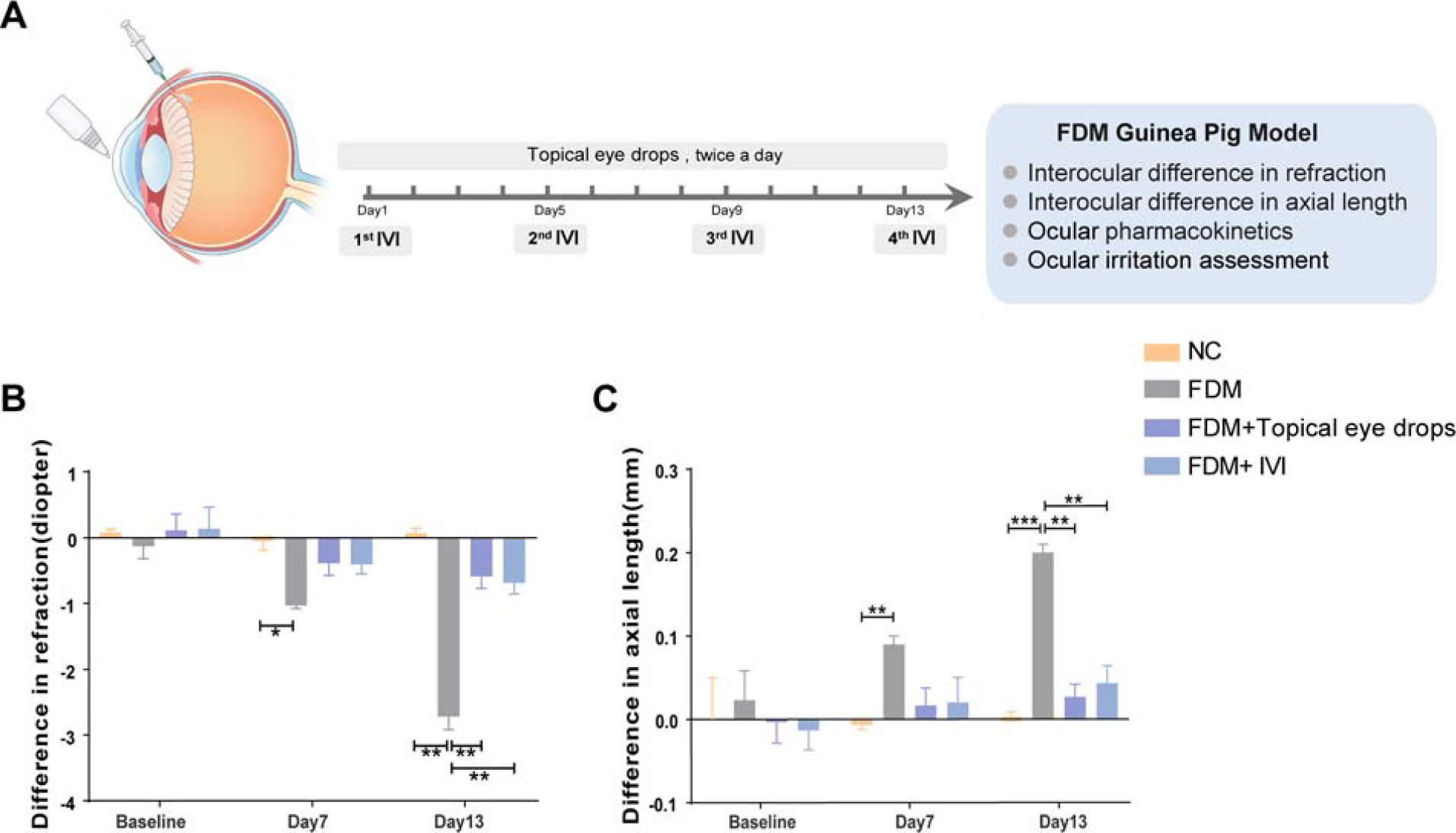
The effects of brimonidine topical eye drops and intravitreal injection on the FDM guinea pig.
Ocular Pharmacokinetics Study of Brimonidine and Its Metabolites
After administering brimonidine using two dosing regimens for 13 days, we measured the concentrations of brimonidine and its metabolite brimonidine-2,3-dione at 0 h (before the last dose) and within 96 h after the last dose.
Following administration of brimonidine topical eye drops, significant brimonidine enrichment was observed in the melanin tissues of the iris (2258 ng/mg) and choroid (161.1 ng/mg) (Fig. 2D, H). The peak concentration of brimonidine in the cornea (22.82 ng/mg) and conjunctiva (31.17 ng/mg) was higher than the levels in the vitreous (0.57 ng/mg), retina (6.75 ng/mg), and sclera (11.96 ng/mg) (Fig. 2A, B, C, F, G, I). Interestingly, brimonidine reached its maximum concentration in the sclera 0.5 h after the last dose, but the drug concentration increased significantly again at 4 h (Fig. 2I).
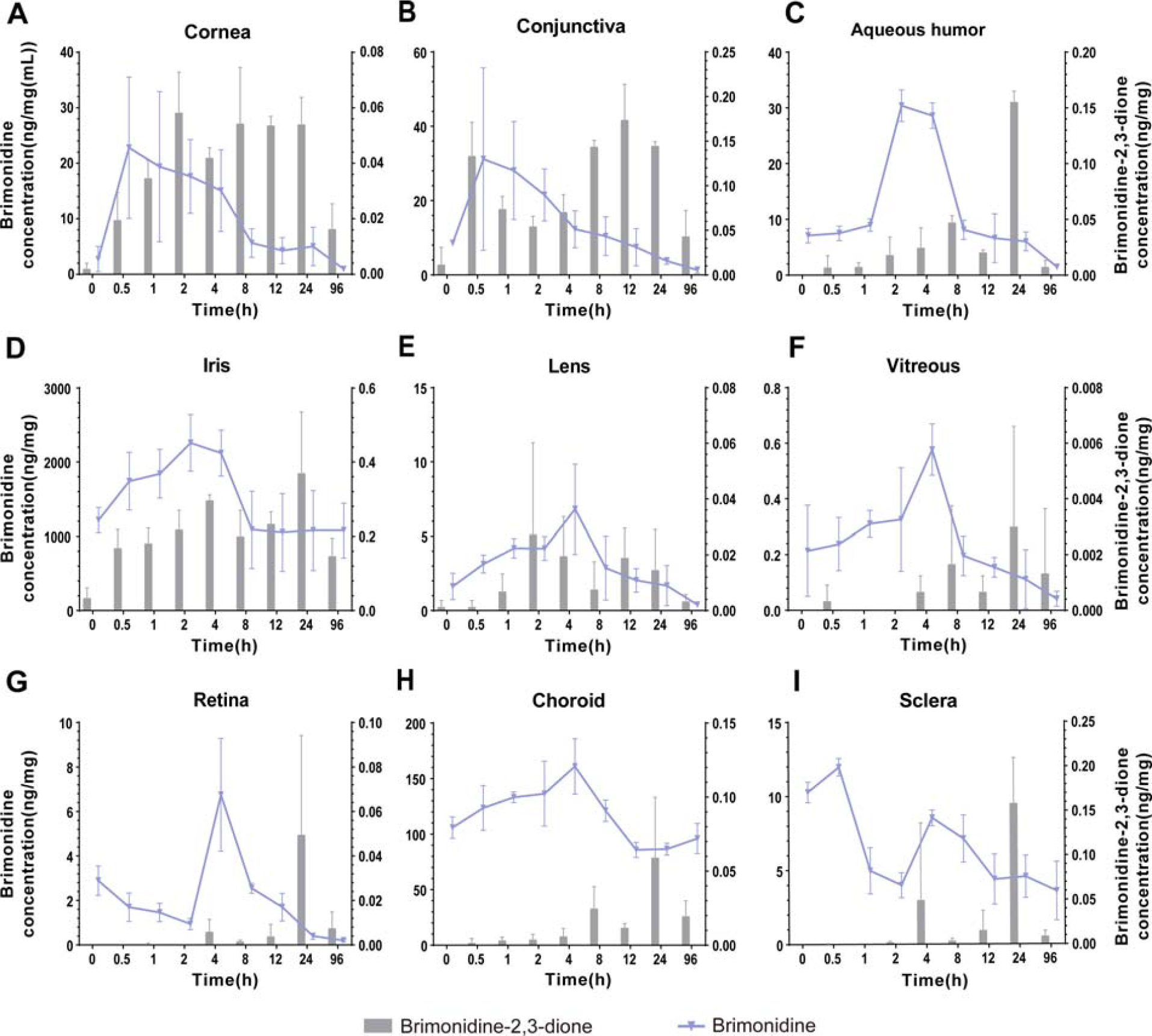
The concentration of brimonidine and brimonidine-2,3-dione at each time point after brimonidine topical eye drops (twice a day for 13 consecutive days). All values represent mean ± SD. Lines represent brimonidine concentrations, and bars represent brimonidine-2,3-dione concentrations. SD, standard deviation.
Following intravitreal administration of brimonidine, high concentrations of the drug were maintained in the iris (222.2 ng/mg) and choroid (266.2 ng/mg) (Fig. 3D, H). The maximum concentrations of brimonidine in the cornea (0.35 ng/mg) and conjunctiva (0.30 ng/mg) were lower compared to those in the vitreous (7.63 ng/mg), retina (8.38 ng/mg), and sclera (8.03 ng/mg) (Fig. 3A, B, C, F, G, I).
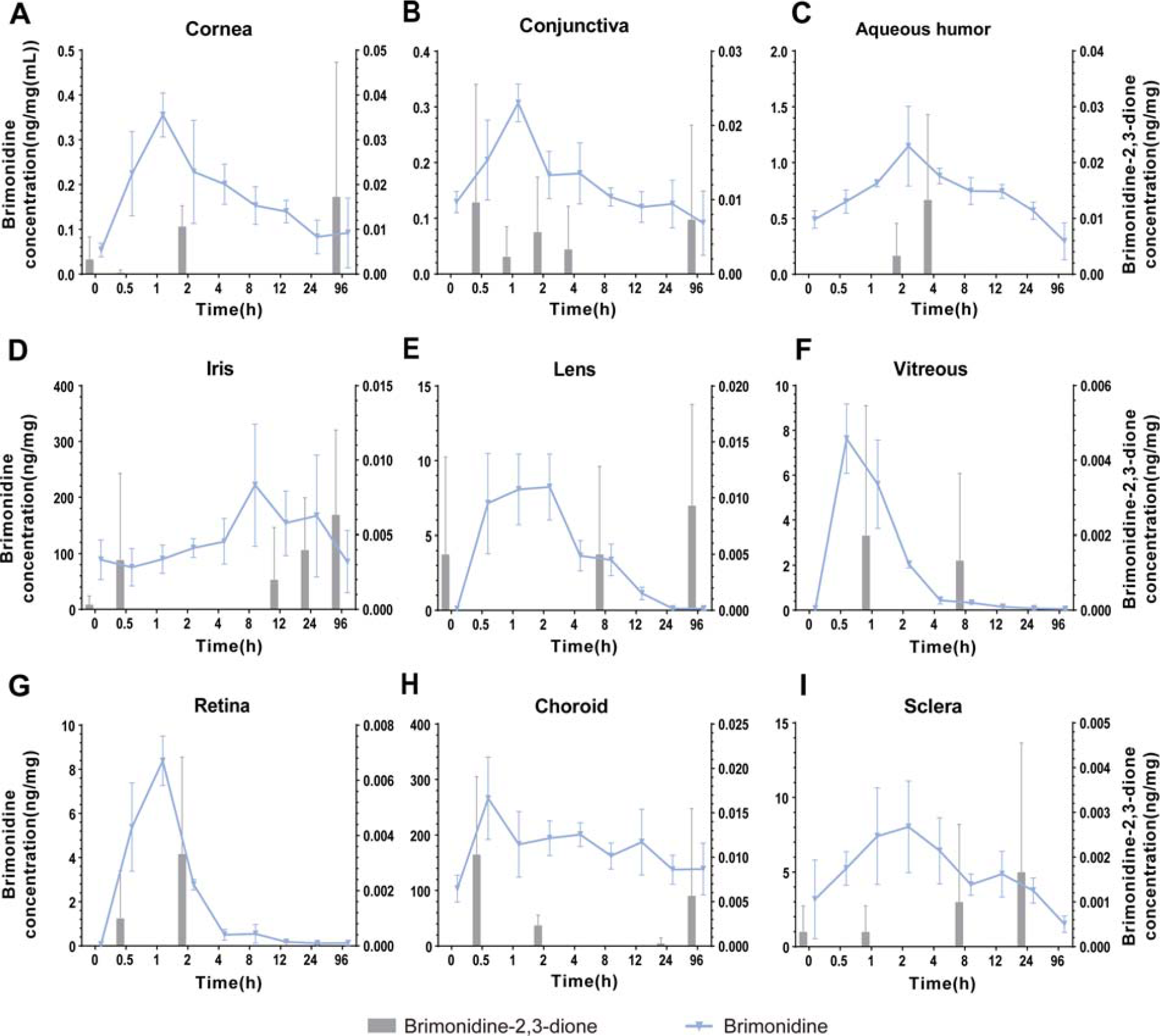
The concentration of brimonidine and brimonidine-2,3-dione at each time point after brimonidine intravitreal injection (Once every 96 h for 13 consecutive days). All values represent mean ± SD. Lines represent brimonidine concentrations, and bars represent brimonidine-2,3-dione concentrations.
Regardless of the route of administration, the concentration of brimonidine-2,3-dione in the tested tissues was markedly lower than that of brimonidine (Figs. 2 and 3).
Pharmacokinetic parameters showed that in retinal tissue, the FDM + Topical eye drops group (Cmax: 6.752 ng/mg; AUC0–∞: 72.81 ng·h/mg) and the FDM+IVI group (Cmax: 8.387 ng/mg; AUC0–∞: 37.26 ng·h/mg) reached the maximum concentration level at 4 and 1 h, respectively. The AUC0-t of brimonidine in the choroid was 9144 ng·h/mg for the topical eye drop group and 14120 ng·h/mg for the intravitreal injection group. The corresponding elimination half-life (T1/2) was significantly prolonged, measuring 238.6 h and 228.8 h, respectively. In scleral tissue, the FDM + Topical eye drops group (Tmax: 0.5 h) reached peak brimonidine concentrations faster than the FDM+IVI group (Tmax: 2 h). The Cmax and AUC0–∞ values of the FDM + Topical eye drops group were 1.48-fold and 1.35-fold higher than those in the FDM+IVI group, respectively (Table 1).
Pharmacokinetic Parameters for Brimonidine and Metabolites After Topical Eye Drops and IVI Administration from NCA
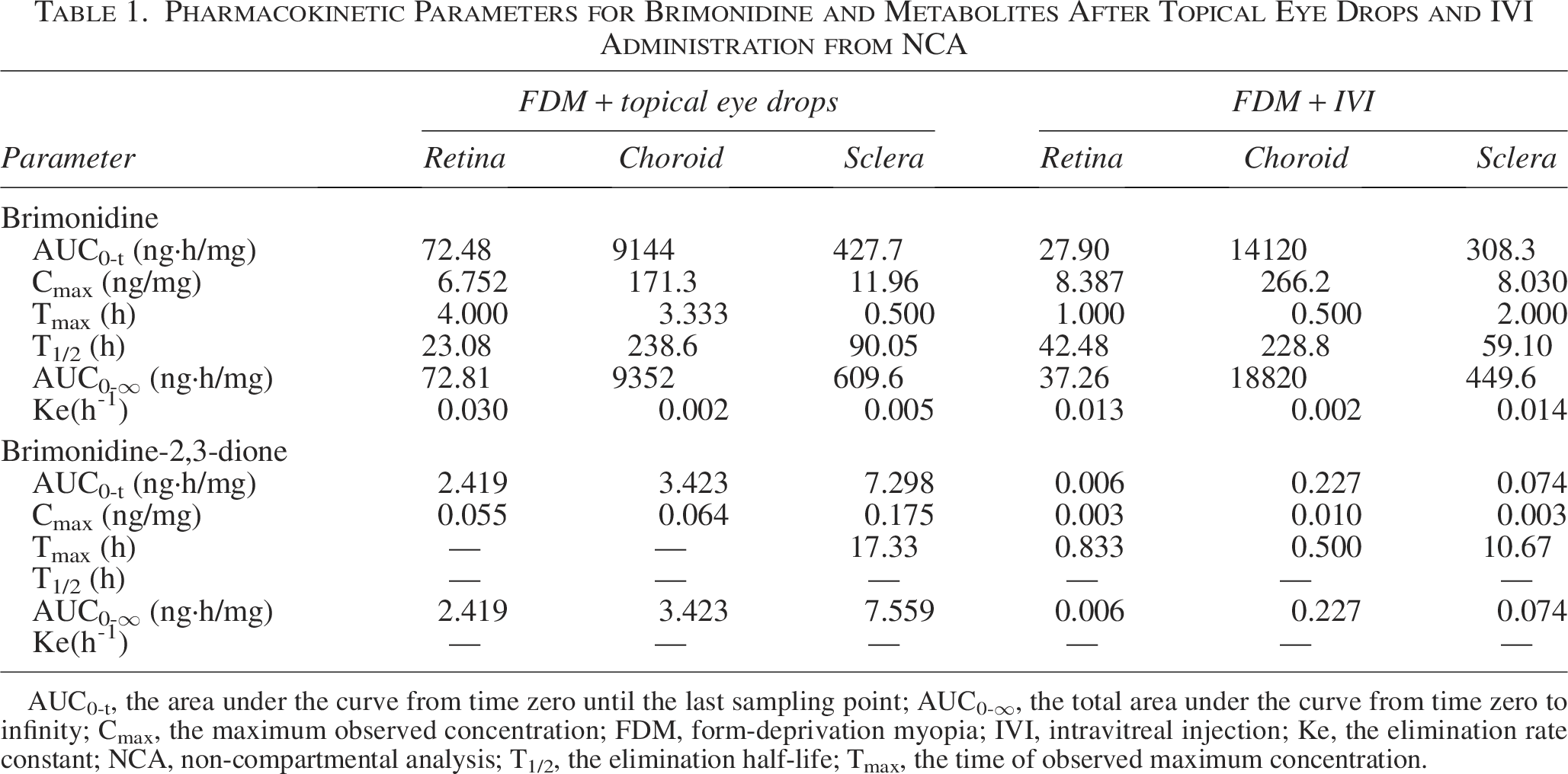
AUC0-t, the area under the curve from time zero until the last sampling point; AUC0-∞, the total area under the curve from time zero to infinity; Cmax, the maximum observed concentration; FDM, form-deprivation myopia; IVI, intravitreal injection; Ke, the elimination rate constant; NCA, non-compartmental analysis; T1/2, the elimination half-life; Tmax, the time of observed maximum concentration.
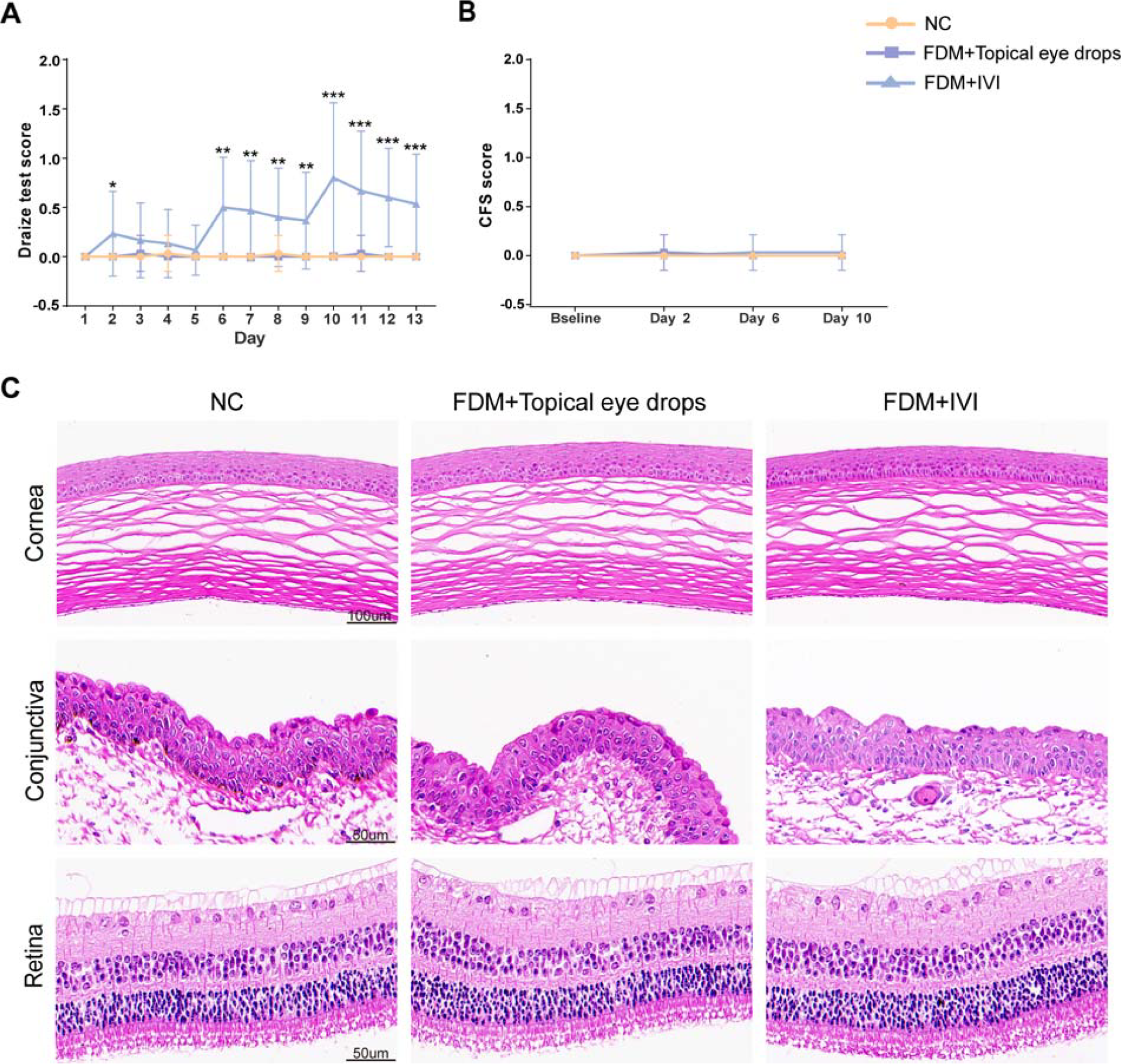
Ocular irritation assessment
Based on the Draize irritation rating scale, no significant differences in ocular irritation scores were observed between the NC group and the FDM + Topical eye drops group. Intravitreal injections were prone to subconjunctival hemorrhage, congestion, and edema, so the Draize irritation score gradually rose with an increasing number of injections (Fig. 4A). Slit lamp images of the anterior segment and CFS are shown in Supplementary Figures S1–S3. No statistically significant differences in CFS scores were observed among the three groups at any time point (P > 0.05, Fig. 4B). Histological analysis revealed the absence of inflammation or morphological changes in the cornea, conjunctiva, and retina of guinea pigs following 13 days of continuous treatment (Fig. 4C). Overall, administration of brimonidine eye drops exhibited minimal irritation to ocular tissues.
Ocular irritation assessment. (
Discussion
This study found that continuous topical and intravitreal administration of brimonidine for 13 days can inhibit axial lengthening and refractive increase in FDM guinea pigs. The distribution and metabolism of brimonidine in target tissues when exerting its myopia-suppressive effect were clarified by analyzing the ocular pharmacokinetics of two administration schemes. Topical administration reduces the risk of subconjunctival hemorrhage caused by frequent intravitreal injections and has less ocular irritation.
Brimonidine has been confirmed to effectively inhibit the progression of myopia through eye drops, subconjunctival injections, and intravitreal injections in LIM guinea pigs, FDM guinea pigs, and FDM chick models.6,7,9 This study discovered that brimonidine topical eye drops (80 μg/μL) or intravitreal injection (4 μg/μL) slowed myopia progression in FDM guinea pigs following 13 days of continuous administration. Topical administration requires higher brimonidine concentrations and more frequent dosing than intravitreal administration to achieve similar myopic suppression effects. In our previous study, topical administration of low-concentration brimonidine eye drops (40 μg/μL) resulted in insufficient intraocular drug levels to reach the therapeutic threshold. 14 High-concentration brimonidine eye drops (80 μg/μL) may enable saturated binding of the drug to its target receptors in ocular tissues, thereby exerting a biological effect in inhibiting myopia progression. Further research is needed to develop innovative ocular drug delivery systems that minimize the potential toxicity and adverse effects associated with high concentration brimonidine, which would improve its safety profile and facilitate its clinical translation. In the same administration method, equally excessively high or low concentrations of brimonidine may lead to a reduction in its inhibitory effect. 8 This phenomenon implies that brimonidine could have a concentration-independent mechanism of action. 9 Topical or intravitreal administration needs to ensure that brimonidine attains an effective concentration profile in ocular tissues to exert its pharmacological effect.
We employed UPLC-MS/MS to analyze the ocular pharmacokinetics to further clarify the tissue drug distribution of brimonidine when it exerts myopia-suppressing effects via two administration methods. When administered topically, brimonidine reached peak concentrations first in the cornea, conjunctiva, and sclera, with higher concentrations in the anterior segment tissues. Conversely, intravitreal administration led to initial drug exposure in the vitreous, with elevated concentrations in posterior segment tissues. Different administration methods have different drug penetration pathways. The concentration gradient between tissues drives the drug to passively diffuse from high-concentration tissues to low-concentration tissues.15,16 Topical administration facilitates the diffusion of the drug from highly concentrated corneal and conjunctival tissues to the posterior segment of the eye.17,18 Intravitreal administration promotes drug diffusion into the retinal tissue. Due to the low permeability of the lens and the reverse clearance of the aqueous humor circulation, it is difficult for drugs to diffuse from the vitreous body to the ocular anterior segment.19,20
The mechanism of brimonidine suppression of myopia remains incompletely understood. After intravitreal injection of brimonidine in FDM guinea pigs, it was found that the expression levels of the genes Col1a1 and Mmp2, which are closely related to myopia, were upregulated in the retina. 9 On the other hand, brimonidine may inhibit myopia development by modulating retinal dopamine release through activation of the alpha-2 adrenergic receptor.21–23 Brimonidine effectively increased choroidal blood flow in FDM guinea pigs, which may be associated with the vasodilatory response induced by nitric oxide.8,24 Liu et al. demonstrated that brimonidine suppressed myopia progression in LIM guinea pigs and significantly reduced intraocular pressure. 6 They speculated that brimonidine can delay the scleral creep phenomenon caused by myopia by lowering intraocular pressure. Additionally, brimonidine may regulate scleral remodeling by affecting the expression of basic fibroblast growth factor and transforming growth factor beta.24–28 Previous studies suggest that the posterior segment of the eyeball may be the target tissue for brimonidine in inhibiting myopia. The retinal/choroidal/scleral signaling cascade is a key pathological mechanism for the occurrence of myopia. 29 Brimonidine needs to achieve sufficient drug exposure in the ocular posterior segment to intervene in this signaling cascade and achieve efficacy.
This study analyzed the pharmacokinetic parameters of posterior segment ocular tissues when brimonidine exerts its myopia-suppressing effect through two different administration routes. In the retina, the AUC0–∞ value of brimonidine administered intravitreally was 0.51 times that of topical administration. This difference may be attributed to the higher frequency and concentration of topical administration in the dosing regimen of this study. This could lead to a greater accumulation of brimonidine in retinal tissue. We detected that at 0.5 h after brimonidine eye drops, the drug concentrations in the conjunctiva and cornea were comparable. In the sclera, topical brimonidine administration reached peak drug concentration faster and had higher Cmax and AUC0–∞ values than intravitreal administration. Intravitreal drugs need to cross the blood–retinal barrier to penetrate the choroid and sclera. However, when brimonidine is administered locally, the loose tight junctions of the conjunctival epithelium and the larger absorption surface area of the sclera together facilitate the rapid absorption of drugs by the sclera.30,31 In previous similar studies, Khopade et al. confirmed that brimonidine eye drops can be rapidly absorbed through the conjunctiva and distributed to the scleral tissue. 32 The hydrophilic and lipophilic characteristics of the small-molecule compound brimonidine are critical for promoting its penetration into posterior ocular segment tissues.32–35 When administered topically, the drug’s lipophilicity facilitates passage through conjunctival paracellular pores.36,37 The hydrophilic characteristics make it easy to penetrate the sclera and spread to the retina and choroid.18,38,39 Conversely, intravitreal administration allows hydrophilic molecules to readily diffuse within the vitreous and retinal tissues. Lipophilic molecules can traverse the blood–retinal barrier towards the posterior segment.40,41 In conclusion, brimonidine can be distributed to the posterior segment tissues via different permeation pathways. Topical application through the conjunctival route can more efficiently deliver the drug to the sclera.
Brimonidine is a highly melanin-binding drug that reversibly binds to ocular melanin with significant affinity.42–44 Brimonidine displays preferential distribution and slower elimination in melanin-rich ocular tissues. 33 This drug property enables brimonidine to bind easily to pigmented tissues to form a drug depot that gradually releases free drugs into surrounding tissues.45–48 In our study, we also observed a sustained and significant brimonidine accumulation in the pigmented tissues of the iris and choroid. Notably, the scleral drug concentration increased significantly at 0.5 and 4 h after the final administration of topical brimonidine, as indicated by the drug concentration-time curve. The initial concentration increase likely reflects rapid drug penetration into the sclera via the conjunctiva. The subsequent concentration increase may be attributed to the release of brimonidine from choroidal melanin into the sclera. The high affinity of brimonidine for the choroid facilitates the targeted transport of the drug to the ocular posterior segment and prolongs its efficacy. This property enhances brimonidine’s myopia-suppressing effects.
AOX is the key enzyme that dominates the metabolism of brimonidine in the eye and liver. In intraocular tissues, brimonidine is oxidized by AOX to the metabolite brimonidine-2,3-dione. 11 At present, there is a lack of comprehensive research on the intraocular distribution of this metabolite after brimonidine eye drops or intravitreal injection, which has important research value. AOX exhibits high activity in the iris, ciliary body, cornea, and conjunctiva. Brimonidine is primarily metabolized as brimonidine-2,3-dione in the ocular anterior segment, followed by clearance via the aqueous humor circulation.11,49 This study consistently detected relatively high concentrations of brimonidine-2,3-dione in anterior segment tissues, although its tissue content remained significantly lower than that of the parent drug. Del Amo et al. reported that in albino rabbit eyes, the AOX activity and brimonidine-2,3-dione content in the iris were higher after intracameral or intravitreal brimonidine administration. 11
In addition to the classical muscarinic acetylcholine receptor (mAChR) antagonism, alpha-2 adrenergic receptors may also play a significant role in the anti-myopia effect of atropine. Studies have shown that mAChR antagonists effective in suppressing myopia, such as atropine, can bind to and block alpha-2 adrenergic receptor signal transduction. Their efficacy in myopia suppression appears to correlate with their ability to block alpha-2 adrenergic receptors. 10 Injection of brimonidine in FDM chickens can inhibit myopia, and the required concentration is similar to that of atropine in effectively inhibiting myopia. 7 Therefore, alpha-2 adrenergic receptors may be an important target for atropine and brimonidine in inhibiting myopia. In the future, pharmacodynamic and pharmacokinetic studies comparing brimonidine and atropine can be conducted to further explore the advantages of alpha-2 adrenergic receptors in the control of axial myopia.
This study still has certain limitations. The 13-day experimental period was optimized to align pharmacokinetic sampling with the therapeutic effect window. However, this relatively short period may limit the comprehensive evaluation of the long-term pharmacodynamic effects of the drug. Differences in ocular physiology and anatomy between guinea pigs and humans result in species-specific pharmacokinetic and pharmacological activity studies. Compared with humans, guinea pigs have smaller eyeballs and a less vascularized retina, which may affect drug absorption and elimination within the ocular posterior segment. Future preclinical studies using primate models are needed to more accurately predict the clinical performance of drugs. During our research process, we strictly ensured that the mask did not touch the eyelids and the surface of the eyeball. Eye irritation mainly manifests as invasive damage caused by the vitreous injection procedure. Therefore, the interference of the mask had been effectively controlled, and the experimental results were not significantly affected. The concentration of brimonidine eye drops used in this study is higher than the concentration commonly used in clinical practice. 50 This may limit the ability of the ocular irritation results in guinea pigs to directly reflect the clinical safety of the drug concentrations used in this study.
In pediatric populations, especially in children under six years of age, brimonidine can penetrate the blood–brain barrier and activate central alpha-2 adrenergic receptors after ocular administration.51–53 This may lead to dose-dependent central nervous system depression and systemic toxicity. Such risks limit the clinical use of high concentration brimonidine for myopia control in young children. In the future, we can explore new targeted drug delivery technologies to precisely deliver brimonidine to the target tissues for myopia regulation. Targeted drug delivery technology can avoid the risk of systemic drug exposure and achieve safe and effective myopia intervention while significantly reducing the dosage concentration. This strategy could provide a potential translational pathway for the safe application of brimonidine in the pediatric population.
Conclusion
In summary, this investigation conducted a comprehensive examination of the ocular tissue distribution and pharmacokinetic characteristics of brimonidine in inhibiting myopia progression in FDM guinea pigs. At the concentrations of drug used in this study, both topical and intravitreal administration delivered sufficient amounts of brimonidine to ocular tissues, especially the posterior segment tissues, and produced similar myopia-suppressing effects. The high-affinity binding of brimonidine to choroidal melanin could prolong the pharmacological effect. Compared with intravitreal administration, continuous topical administration resulted in greater drug accumulation within the retina and sclera, while minimizing ocular irritation. These findings support the safety and therapeutic potential of brimonidine in the treatment of myopia and provide animal pharmacokinetic evidence to guide the optimization of future dosing regimens.
Authors’ Contributions
F.Z.: Methodology, data curation, investigation, and writing. H.H.: Methodology. S.H., J.Y., and Y.L.: Data curation and investigation. X.Z. and G.H.: Supervision, funding acquisition, and conceptualization. All authors reviewed and approved the article.
Footnotes
Acknowledgment
The authors are very grateful to researcher Xiuhuan Wang and the Institute of Tropical Biotechnology of the Chinese Academy of Tropical Agricultural Sciences for their technical support of this research.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This work was supported by grants from the National Natural Science Foundation of China (82271116), Hainan Province Clinical Medical Center, and the Science and Technology Planning Project of Hainan Province (ZDYF2022SHFZ326, LCYX2024-06).
Ethics Approval and Consent to Participate
Ethical review was provided by the Medical Ethics Review Committee of Hainan Eye Hospital (approval number: 2022-039-01).
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.