
Abstract

In the selection of therapy for a patient, the doctor selects the appropriate therapy based upon a wealth of patient-specific considerations. We posit that there is an implicit assumption by the doctor that if a product is approved by the US Food and Drug Administration (FDA) for a given indication, the standards for efficacy are the same. Therefore, we believe it is worthwhile to evaluate whether the efficacy criteria at the FDA for drugs and devices for a given indication are the same. As reported previously, we found differences among drugs, among devices, and between drugs and devices for treatments for dry eye disease and glaucoma (elevated intraocular pressure, IOP). For glaucoma, we reported that all drugs approved for the treatment of glaucoma or ocular hypotension have very similar indication statements. By contrast, the approved and cleared glaucoma devices have a range of indication statements based upon the target patient population and nature of the surgical procedure in which the device is used. Herein, we present the details of the glaucoma products for 2003–2025. The 11 ophthalmic devices cleared/approved on the basis of premarket clinical data were manual instruments, lasers, and implants. The 17 ophthalmic drugs approved were new chemical entities, reformulations and drug delivery systems, and fixed-dose combinations of approved drugs. The disparities in the FDA premarket clinical evaluation of drugs vs. devices make it challenging for patients and caregivers to compare treatments, and for product developers to select the appropriate clinical study design for potential US regulatory approval.
When a doctor sees a patient, the first step is diagnosis. The next step is therapy—if applicable. The doctor selects the appropriate therapy based upon a wealth of considerations (e.g., history, comorbid conditions, concomitant medications, and patient preference).
We posit that there is an implicit assumption by the doctor that if a product is approved by the US Food and Drug Administration (FDA) for a given indication, the standards for efficacy are the same.
Recently, we investigated that assumption for treatments approved or cleared for ocular surface disease during the period 2003–2025. We reported that the measures for efficacy are very different among drugs, among devices, and between drugs and devices. 1
We also investigated this assumption for treatments for glaucoma. Note that all approvals or clearance for glaucoma therapy at present are for the lowering of elevated intraocular pressure (IOP), and none (yet) are for neuroprotection. 2
We reported that all drugs approved for the treatment of glaucoma or ocular hypotension have very similar indication statements (e.g., “…for the reduction of elevated intraocular pressure in patients with open-angle glaucoma or ocular hypertension”). By contrast, the approved and cleared devices have a range of indication statements based upon the target patient population and nature of the procedure in which the device is used. 2
We thought it might be useful for the readers of this journal to present the details of the glaucoma products. Provided in Table 1 is a detailed list of glaucoma devices authorized for marketing in the United States on the basis of premarket clinical data during the period of 2003–2025. Provided in Table 2 is a complementary detailed list of glaucoma drugs authorized in the same period. Note that there were no notable devices approved/cleared for use in glaucoma from January to November 2025.
Chronological List of Devices Approved/Cleared for the Reduction of Elevated Intraocular Pressure in the United States: 2007–2025
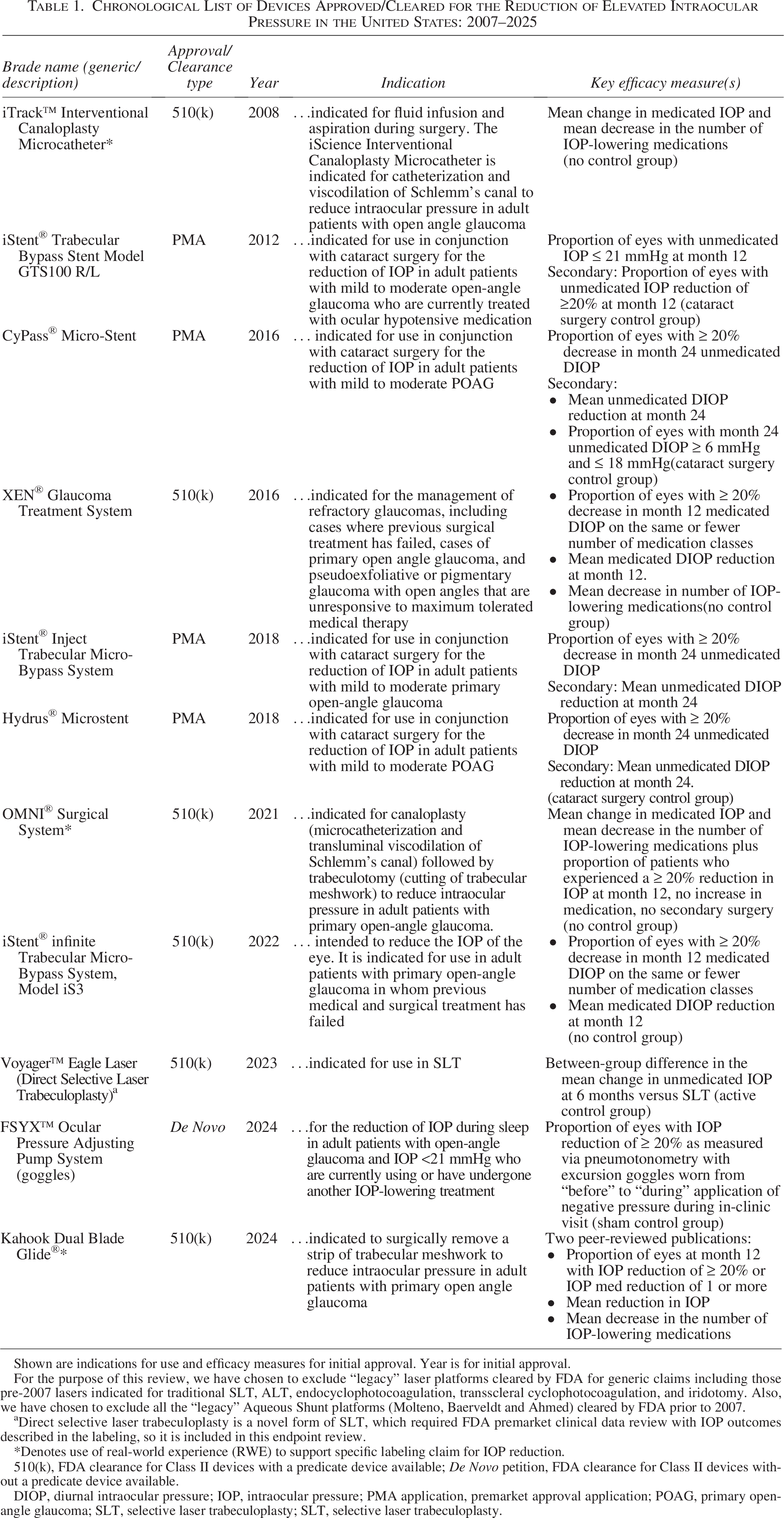
Shown are indications for use and efficacy measures for initial approval. Year is for initial approval.
For the purpose of this review, we have chosen to exclude “legacy” laser platforms cleared by FDA for generic claims including those pre-2007 lasers indicated for traditional SLT, ALT, endocyclophotocoagulation, transscleral cyclophotocoagulation, and iridotomy. Also, we have chosen to exclude all the “legacy” Aqueous Shunt platforms (Molteno, Baerveldt and Ahmed) cleared by FDA prior to 2007.
Direct selective laser trabeculoplasty is a novel form of SLT, which required FDA premarket clinical data review with IOP outcomes described in the labeling, so it is included in this endpoint review.
*Denotes use of real-world experience (RWE) to support specific labeling claim for IOP reduction.
510(k), FDA clearance for Class II devices with a predicate device available; De Novo petition, FDA clearance for Class II devices without a predicate device available.
DIOP, diurnal intraocular pressure; IOP, intraocular pressure; PMA application, premarket approval application; POAG, primary open-angle glaucoma; SLT, selective laser trabeculoplasty; SLT, selective laser trabeculoplasty.
Chronological List of Drugs Approved/Cleared for the Reduction of Elevated Intraocular Pressure in the United States: 2007–2025
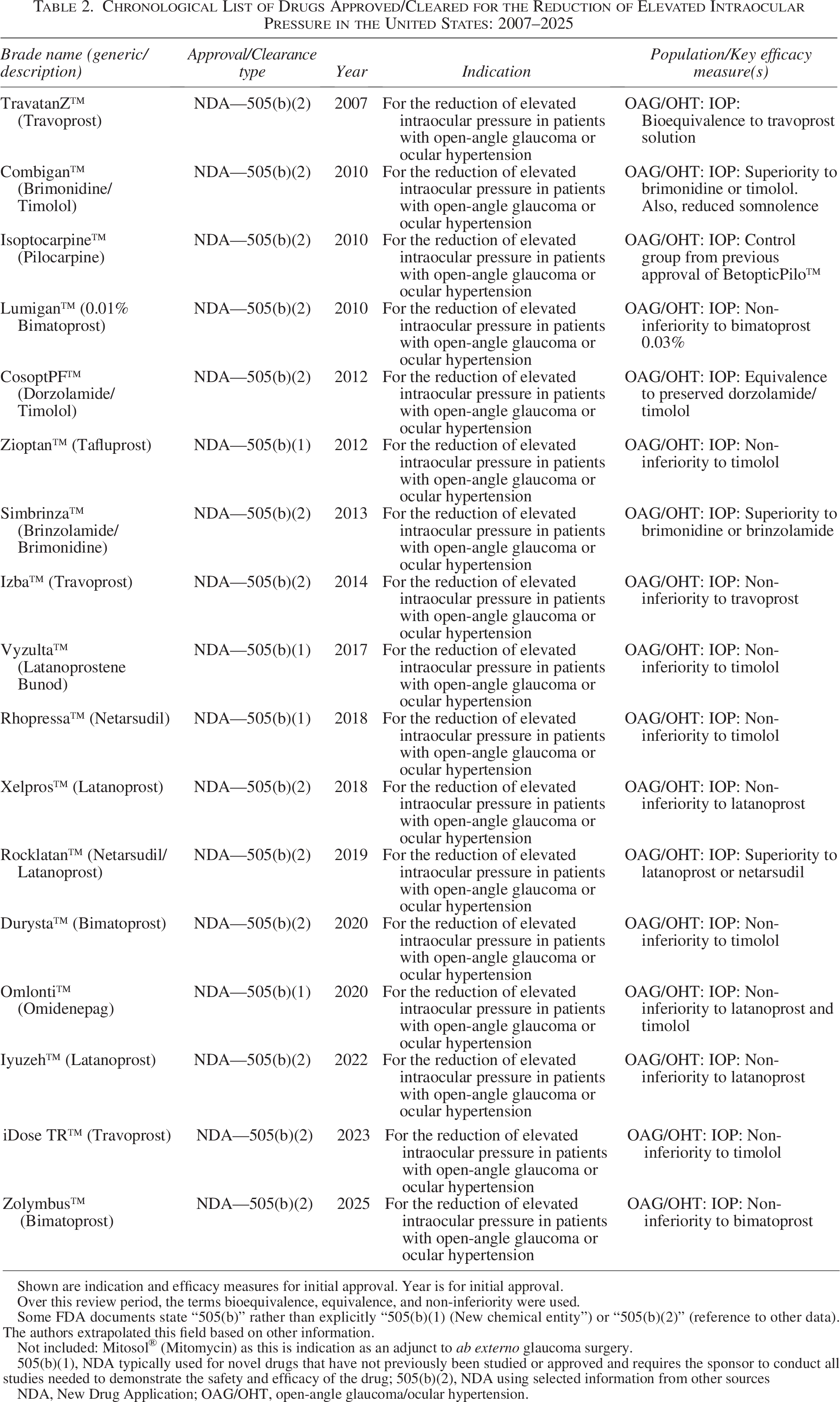
Shown are indication and efficacy measures for initial approval. Year is for initial approval.
Over this review period, the terms bioequivalence, equivalence, and non-inferiority were used.
Some FDA documents state “505(b)” rather than explicitly “505(b)(1) (New chemical entity”) or “505(b)(2)” (reference to other data). The authors extrapolated this field based on other information.
Not included: Mitosol® (Mitomycin) as this is indication as an adjunct to ab externo glaucoma surgery.
505(b)(1), NDA typically used for novel drugs that have not previously been studied or approved and requires the sponsor to conduct all studies needed to demonstrate the safety and efficacy of the drug; 505(b)(2), NDA using selected information from other sources
NDA, New Drug Application; OAG/OHT, open-angle glaucoma/ocular hypertension.
The 11 ophthalmic devices cleared/approved in this time period may be grouped into three main categories:a
The 17 ophthalmic drugs approved in this time period may be grouped in four main categories:
New chemical entities for which the efficacy data were non-inferiority to a positive control. Reformulations of approved drugs for which the efficacy was non-inferiority to a positive control—typically the same molecule in the innovator’s formulation. Fixed-dose combinations of approved drugs, which were superior to either agent used alone. Drug delivery systems. These unique products typically showed non-inferiority to a positive control. The safety of an intraocular implant is a concern with some of these products, leading to limited use.
The regulatory position on ocular hypotensive agents is that elevated IOP is associated with glaucomatous progression, and that lowering of elevated IOP is able to slow this progression. This position, which has been in place over 40 years, was validated by controlled, long-term studies. The studies include two negative-controlled studies of the progression from ocular hypertension to open-angle glaucoma,3,4 and several medication-controlled studies evaluating laser trabeculoplasty5,6 and filtering surgery. 7
As noted above, there are no approved/cleared products that have been labeled as being able to slow the progression of glaucomatous optic neuropathy. The regulatory requirements for a product which does not lower elevated IOP but has neuroprotective (or neuroenhancement) efficacy have been discussed for many years, most notably in a symposium held 2010. 8 There have been many potential products evaluated, including two Phase 3 studies on oral memantine. 9 In public presentations, both the Center for Devices and Radiological Health (CDRH) and the Center for Drug Evaluation and Research (CDER) have expressed interest in such a neuroprotective product and their openness to discussing regulatory requirements. With the increased use of non-invasive imaging technologies, some of these discussions center on whether benefit as described by a structural endpoint, which is presumed to precede benefit as described by functional endpoints, might be acceptable to FDA as the primary efficacy outcome within a Phase 3/pivotal study for an ophthalmic drug or device. In our opinion, it behooves the glaucoma community to provide appropriate data to support the use of shorter-term studies and surrogate endpoints to support a neuroprotective indication.
The disparities in the FDA premarket clinical evaluation of drugs vs. devices make it challenging for patients and caregivers to compare treatments. It also presents challenges to the firms developing novel products to select the appropriate clinical study design for potential US regulatory approval. Where appropriate and in conformance with FDA regulations and statutes, which differ for drugs and devices, we hope that the FDA will work to resolve these disparities and that innovative researchers and developers continue to develop novel pharmaceuticals and devices (as well as their combination in novel products) to substantially lower elevated IOP with an improved safety profile. We also hope that emerging treatments, which decrease glaucomatous progression independent of IOP effects, continue to be developed to better serve patients suffering from this ubiquitous and sight-threatening disease.
Authors’ Contributions
R.L.K. and G.D.N. both contributed to this commentary.
Footnotes
Author Disclosure Statement
The authors consult for numerous ophthalmic, pharmaceutical, and medical device firms.
Funding Information
No funding was received in support of this report.