
Abstract
Historical medical texts occasionally preserve therapeutics of unexpected modern relevance. This hypothesis-generating review presents a new translation and interpretation of human milk-based ophthalmic remedies in the Ebers papyrus (∼1550 BC) and evaluates their potential applicability to contemporary dry eye disease. Growth factors abundant in human milk parallel those delivered by autologous serum tears, and emerging evidence, including animal models and limited clinical studies, demonstrates that both human milk and bovine colostrum can promote corneal epithelial healing and reduce ocular surface inflammation. Given the high cost of current therapies and the ethical constraints surrounding donor human milk, bovine colostrum represents a low-cost, scalable alternative warranting further investigation. This historical-biomedical synthesis illustrates how ancient medical practices may inform modern strategies for managing refractory ocular surface disease.
Introduction
The search for novel, cost-effective therapies often leads modern practitioners to look toward the past, seeking inspiration in medical texts composed long before mass-produced pharmaceuticals. Perhaps the most celebrated recent example is the discovery of artemisinin, an anti-malarial derived from a traditional Chinese remedy, which earned Tu Youyou the Nobel Prize in 2015. A similar historical approach may offer insights for ophthalmology.
This article presents a new translation and interpretation of an ancient Egyptian ophthalmic remedy found in the Ebers Papyrus (∼1550 BC), the most comprehensive surviving medical text of the era. By tracing the historical transmission of this remedy and correlating it with a narrative review of contemporary medical literature, we propose a cost-effective alternative for a prevalent, often refractory condition: severe (Oxford grade > 4) aqueous-deficient dry eye disease (DED).
The Challenge of Dry Eye Disease
DED is one of the most frequently encountered ophthalmic pathologies, with population-based studies estimating prevalences ranging from 5% to 17%. 1 While numerous risk factors and associated diseases influence its course, the general management paradigm remains largely consistent across etiologies.
As detailed in the DEWS III report, 2 first-line management typically includes patient education, eyelid hygiene, ocular lubricants, with adjunctive measures such as punctal plugs in selected cases. Refractory cases may require oral macrolides or tetracyclines, followed by topical immunomodulators such as steroids or cyclosporine. For patients unresponsive to these therapies, autologous serum tears may be used. Surgical interventions, including amniotic membrane transplantation or tarsorrhaphy, are sometimes necessary.
The financial burden associated with advanced therapies for DED represents a significant barrier to access across healthcare systems. In publicly funded settings, topical immunomodulators and autologous serum tears incur substantial institutional costs, with the latter requiring specialized phlebotomy, laboratory processing, and storage infrastructure. In the United Kingdom, the NHSBT provides autologous and allogenic serum eye drops at a cost of approximately £1,100 for 3–5 months’ supply delivered. Cost and availability range and depend on country, compounding concentration, insurance, allogenic or autologous supply. 3 In the United States, where these treatments are often not routinely covered by insurance, patients frequently bear direct out-of-pocket expenses. This can limit long-term affordability and adherence, pointing to a need for alternative cost-effective therapies.
Historical precedent suggests that one possible solution is the adaptation of human milk (HM). Since we now know that HM contains growth factors and immune proteins analogous to serum, HM-derived products might therefore be explored as low-cost biological tear substitutes. We find the first reference to HM as an ophthalmic remedy in ancient Egyptian medical literature.
Human Milk in Ancient Egyptian Ophthalmology
The Ebers papyrus contains four ophthalmic remedies requiring HM. There is #368 for an unknown blindness condition, #384 for removing ‘blood in the eyes’, #408 for removing ‘red inflammation in the eyes’, and #414 for ‘opening the vision.’ Taken together, the most plausible unifying context for these conditions is ocular surface disease. Interpretation is complicated, however, by the obscurity of the underlying ailment in #368 and by an unidentified grain ingredient in #384. Fortunately, the latter two remedies, both on page 62 of the papyrus, present fewer uncertainties (Fig. 1).

Interlinear English translation of Ebers papyrus remedy #408, for ‘removing red inflammation in the eyes’, and #414, for ‘opening the vision’. Scan of the original papyrus in hieratic script (source: https://papyrusebers.de/en/) and transcription into hieroglyphs, followed by transliteration and translation.
These remedies all specify milk from a woman who has borne a son. Egyptologists typically interpret this as a form of sympathetic magic evoking the goddess, Isis, whose milk sustains her son, Horus, and restores the life of her slain husband, Osiris. 4 In several related narratives, the milk of Isis functions as a potent remedy applied to her son’s injuries, although some versions attribute the restorative act to the goddess Hathor, using the milk of a gazelle. 5 Such mythological associations likely contributed to the popularity of HM in ophthalmic prescriptions throughout several medical papyri. Over time, they also helped establish Isis as ‘the one who produces milk,’ an epithet reflected in the Isis lactans iconography (Fig. 2), which in turn influenced later depictions of Mary as Maria lactans in the Christian tradition. 6

The goddess, Isis, feeding Horus; wall relief from the temple at Edfu in Southern Upper Egypt. Photograph taken in 1989 by Carol Reeves. License: Attribution 4.0 International. Available: https://wellcomecollection.org/works/g8ed63dg.
Ancient Egyptian medicine was held in high regard by neighbouring cultures, facilitating the transmission of therapies that were perceived as effective. 7 Ophthalmic preparations employing HM are accordingly attested in Greek, Roman, and Byzantine medical literature. 8 The persistence of this remedy across cultures and centuries may reflect perceived benefit. Modern analyses of HM composition could now help to interrogate this idea.
Biomedical Correlates
Recent analyses of HM composition reveal potential sex-specific differences. Milk produced for male infants has been associated with a higher salt content and a lower percentage of fat. 9 Furthermore, male-infant-directed milk also exhibits an approximately 25% higher calorific content. 10
A proteomic analysis of 98 HM samples identified sex-specific differences for 42 of 146 proteins analyzed. 11 In this study, mothers of male infants produced milk with a greater abundance of proteins involved in energy metabolism, particularly during the mature lactation stage. Whether these sex-specific compositional differences translate into clinically meaningful effects when applied topically to the ocular surface remains unknown, and such an analysis is therefore exploratory.
Regardless of any sex specificity, HM is a rich source of growth factors known to accelerate ocular surface healing. Epidermal growth factor (EGF) is at its highest concentration in HM in the days after parturition and gradually decreases over the first month. 12 Transforming growth factor alpha (TGF-α) is present in HM at lower levels. 13 Last, insulin-like growth factor 1 (IGF-1) and other metabolic growth hormones are also found in HM, in concentrations that correlate with infant weight. 14 This aligns somewhat with the Egyptian remedies, as male babies tend to have a higher birth weight. 15
A standard biological treatment for DED, autologous serum tears, is believed to exert its therapeutic effect by delivering these same growth factors (some of which are also present in natural human tears) to the ocular surface. 16 The existence of these potent growth factors within readily available HM (Table 1) points to a novel avenue of research in the management of recalcitrant DED. What is needed next is a more readily available biological treatment that is cheaper to process, sterile, and rich in these same growth factors, such that dosing is required less than every waking hour.
Ocular Surface Focussed Comparison of the Composition of Human Milk, Human Serum, and Human Tears (Basal Secretion)
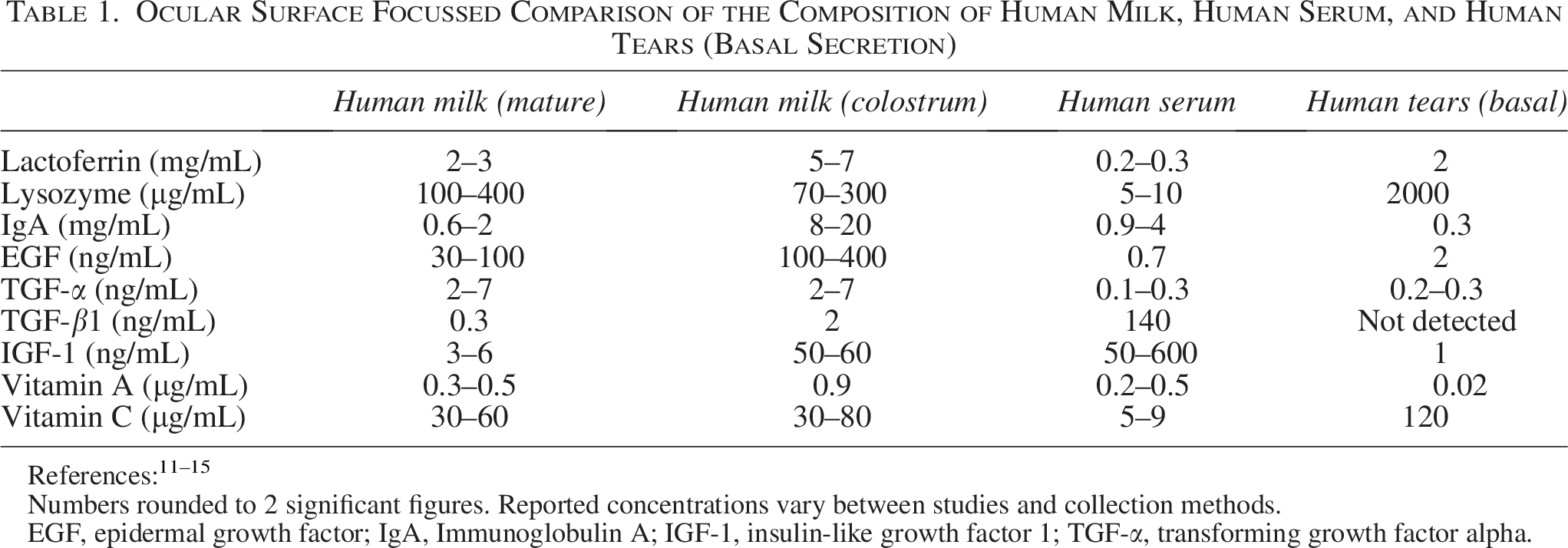
Numbers rounded to 2 significant figures. Reported concentrations vary between studies and collection methods.
EGF, epidermal growth factor; IgA, Immunoglobulin A; IGF-1, insulin-like growth factor 1; TGF-α, transforming growth factor alpha.
Evidence for Topical Human Milk in Ophthalmic Disease
While no studies have yet assessed the use of topical HM for DED in human subjects, robust preclinical and clinical data from related ophthalmic conditions provide grounds for investigation (Table 2).
Review of Studies Assessing Topical Milk-Based Treatments for Ophthalmic Conditions, Summarising Clinical and Preclinical Evidence
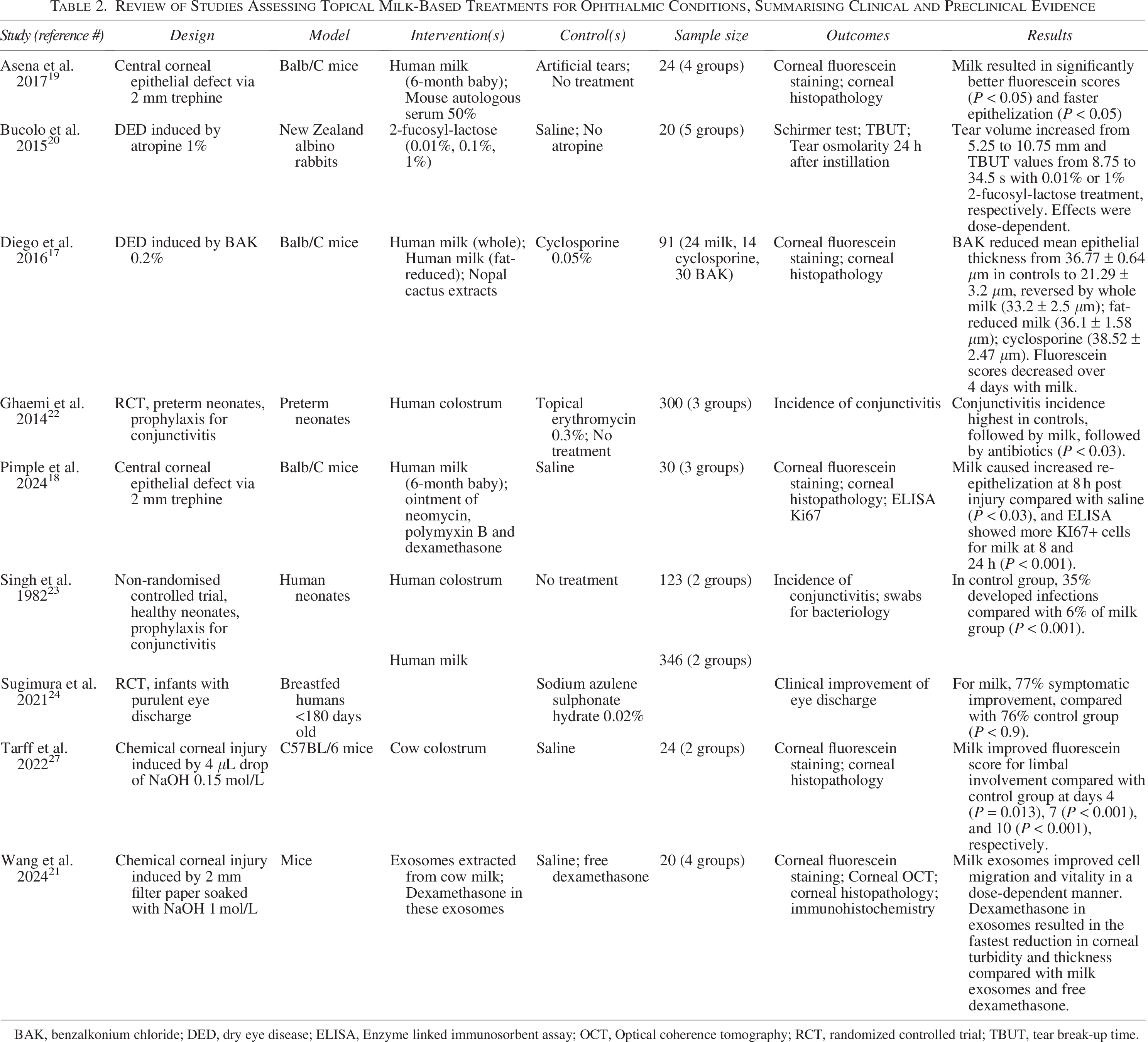
BAK, benzalkonium chloride; DED, dry eye disease; ELISA, Enzyme linked immunosorbent assay; OCT, Optical coherence tomography; RCT, randomized controlled trial; TBUT, tear break-up time.
Mechanistic studies in animal models support HM as an ocular surface healing agent. An animal study investigating HM’s effect on an ocular surface disease model (induced by benzalkonium chloride) demonstrated significantly reduced fluorescein staining and increased epithelial thickness in the treated mouse group. 17 Further research using a mouse model of epithelial debridement showed faster corneal epithelization and enhanced cellular proliferation in eyes treated with HM. 18 This effect is hypothesized to be due to HM’s abundance of growth factors, which is the same mechanism of action proposed for autologous serum tears. Supporting this hypothesis, one mouse study directly compared HM to mouse autologous serum 50%, finding that central epithelial defects healed faster in the HM group. 19 However, other HM components may also be instrumental in epithelial healing. Notably, topical instillation of the milk oligosaccharide, 2-fucosyl-lactose, was shown to reverse atropine-induced DED in rabbits in a dose-dependent manner, specifically decreasing osmolarity while increasing tear break-up time and tear volume. 20 Another promising component is the milk exosome as a nanocarrier, which can be loaded with dexamethasone via ultrasound. Bovine milk exosomes alone were found to increase corneal epithelial cell vitality and migration rate, and when loaded with dexamethasone, resulted in faster corneal healing after alkaline injury than free dexamethasone alone. 21
The use of HM has also been evaluated in human clinical trials for other ophthalmic conditions. Most notably, a randomized controlled trial investigated the use of colostrum for the prevention of neonatal conjunctivitis in preterm babies. 22 The lowest incidence of conjunctivitis was observed in the group treated with topical erythromycin, followed closely by the HM group, with the highest incidence in the control group. This substantiated the findings of a 1982 non-randomized controlled trial comparing HM to no treatment for conjunctivitis prophylaxis. 23 The antimicrobial effects of colostrum have been attributed to its high content of immunoglobulins and lysozymes. Accordingly, another randomized controlled trial found HM non-inferior to sodium azulene sulfonate in infants with eye discharge. 24 More speculatively, HM has also reportedly been used for the management of congenital nasolacrimal duct obstruction, though the supporting evidence remains preliminary and requires further confirmation. 25
Cost-Effectiveness
In the USA, in 2015, the average cost of donor HM from milk banks was $100–$170 per liter. 26 It is difficult to ascertain the cost per treatment course if this was used for DED, as research on dosage is required. However, this has the potential to be considerably less expensive than standard immunosuppressants or autologous serum tears used in the management of DED. Nonetheless, alternative mammalian sources may be cheaper, with the most economically viable option likely derived from the most commonly farmed species.
Bovine colostrum has demonstrated efficacy in facilitating corneal healing in murine models of acute ocular alkali burns, 27 and small-scale clinical studies suggest potential benefit in patients with severe ocular surface disease.28,29 As a by-product of the dairy industry, raw bovine colostrum is relatively inexpensive, with some Irish products retailing for as little as £10 (∼$13) per liter. However, raw ingredient pricing would differ from that of a regulated ophthalmic product. Bovine colostrum’s diverse applications as a nutraceutical have contributed to steadily increasing interest, especially in North America, 30 but bioactive properties vary considerably across brands, 31 highlighting the need for a pharmaceutical-grade product specifically formulated for ophthalmic use. None currently exists. As is the case with serum-derived drops, formulation of milk-based treatment would require donor/batch screening, microbiological testing, sterile processing, validated stability, unit-dose packaging, and cold-chain distribution. Each of these would inevitably add to the total product cost.
Challenges and Considerations for Ophthalmic Translation
The principal translational challenges for milk-derived ophthalmic therapy are microbiological safety and pharmaceutical standardization.
Contamination of multidose ophthalmic bottles during use is well documented in clinical settings, and contamination risk increases with duration of use. 32 Ocular milk-derived preparations would require controlled aseptic manufacture and an ophthalmic-grade sterility assurance strategy, rather than repurposing raw or consumer-grade products.
Several processing routes are theoretically feasible, but each involves trade-offs between sterility assurance and preserved bioactivity. Holder pasteurization is widely used in donor milk banking and reduces infectious risk, but it can alter concentrations of biologically active components. 33 For example, EGF levels remain stable, 34 whereas IGF-1 levels can reduce by as much as 39%. 35 Early translational work should prioritize preservative-free preparations because preservatives can worsen ocular surface disease. 36 A practical initial clinical format could be single-use (unit-dose) vials compounded aseptically, analogous to established handling approaches used for autologous serum eye drops. 37
To reduce contamination risk in real-world administration, early-phase studies could specify single-use containers, limited use time after opening, refrigerated storage, and explicit patient-handling instructions.32,38 These measures are motivated by demonstrated contamination pathways involving dropper tips, caps, and residual bottle contents.32,38
Tear film homeostasis, including osmolarity, is central to DED pathophysiology and management.39,40 Consequently, a clinically viable milk-derived ophthalmic product would also require standardization of osmolarity and pH. Standardization would likely require dilution and/or reformulation in a buffered vehicle. However, this would risk reducing concentration and stability of putative bioactive factors, hence necessitating empirical dose–response evaluation.
Processing and storage conditions influence donor milk composition. Defined storage limits would be needed as controlled studies of refrigerated storage demonstrate changes in bacterial growth and selected components over time. 41 However, growth factor levels in frozen human colostrum remain stable for at least 6 months. 42
For ophthalmic translation, stability testing should be performed as for other biological ophthalmic preparations, including sterility and validated shelf-life. 37
Hypersensitivity reactions may limit use in some patients. Bovine milk allergy is most common in childhood and frequently resolves, although persistence occurs in a minority of individuals. 43 Food allergy in adults is also well documented, although prevalence and clinical phenotypes differ from pediatric disease. 44 Early-phase trials should therefore include screening for milk allergy or severe atopy and exclude known milk protein hypersensitivity.
In addition to safety considerations, ethical concerns regarding equitable access to donor HM must inform any translational ophthalmic application. Access to donor HM for its primary purpose of neonatal nutrition may already be insufficient and inequitable, even in resource-rich settings. 45 Ethical resource allocation could therefore prove challenging.
Last, regulatory oversight of donor HM varies substantially between jurisdictions, with important implications for any proposed ophthalmic application. In the United States, donor HM is not classified as a human tissue or pharmaceutical product at the federal level, and its collection, storage, and distribution are not regulated by the Food and Drug Administration. Instead, HM is treated primarily as a nutritional product, with milk banks operating under voluntary accreditation and safety guidelines issued by the Human Milk Banking Association of North America. 46
In contrast, while donor HM in the United Kingdom is similarly not classified as human tissue under the Human Tissue Act, milk banking operates within a more formalized clinical governance framework. UK milk banks must adhere to national guidance issued by the National Institute for Health and Care Excellence, which establishes criteria for donor selection, screening, processing, and quality assurance. 47 These regulatory differences highlight the need for jurisdiction-specific oversight should milk-derived products be investigated beyond their established nutritional role. What is needed next is a homogenization of regulatory differences in donor HM with criteria established for donor selection screening, processing, and quality assurance. This will allow multi center early phased trials to be designed across more than one country more easily.
Conclusion
In summary, the ophthalmic remedies in the Ebers Papyrus illustrate an intersection of ancient medical ingenuity, mythological symbolism, and biologically plausible therapeutics. HM offers a rich source of growth factors capable of promoting ocular surface healing, providing a potential parallel to modern autologous serum tears. This hypothesis-generating review hence details animal studies and related clinical studies demonstrating that HM and perhaps bovine colostrum offer a novel solution to DED worthy of further study. It also presents a pathway to the development of an ophthalmic pharmaceutical preparation based on these milk products, setting out the work that remains to be done.
Despite these encouraging observations, however, there is currently no direct evidence supporting the use of topical HM for the treatment of DED in human subjects. Consequently, until human studies are conducted, the use of milk-derived preparations for DED should be confined to experimental settings, with careful attention to safety, standardization, and regulatory oversight.
Literature Search
To collate the evidence of topical milk usage within ophthalmology, a literature search was performed via the PubMed database. We used the search string ‘eye’ AND (‘milk’ OR ‘colostrum’) on 1st February 2026. Included studies were all peer-reviewed original research articles investigating the use of topical milk or milk-derived products for any ophthalmic condition. Any studies not involving human or other animal participants were excluded. Of the 969 search results, only 9 met these criteria. One study was excluded as the abstract was only available in a book chapter. 28 Two were excluded because they only assessed the in vitro activity of HM against bacterial cultures derived from conjunctivitis cases.48,49 One study was excluded because it used only a rabbit corneal epithelial cellular model to test the effects of milk fractions on Acanthamoeba cytopathy. 50 Reference mining for each pertinent article was also performed, which did not reveal further pertinent studies. The nine reviewed studies were too heterogeneous in design for meta-analysis, so a narrative approach was chosen.
Authors’ Contributions
D.M.: Writing—review & editing, Writing—original draft, validation, formal analysis, conceptualization. R.M.B.: Writing—review & editing, writing—original draft, validation, formal analysis, conceptualization. A.O.: Writing—review & editing, validation, formal analysis.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.