
Abstract
Purpose:
Dry eye disease affects quality of life and generates significant health care costs. Severe forms, refractory to conventional treatments, are responsible for visual impairment and disability. Autologous serum eye drops (ASEDs) are proven to be a therapeutic alternative. We carried out a national inventory of ASEDs preparation practices that highlights low supply (13 producer centers in France) and preparation heterogeneity. The general objective was to develop a national consensus-based protocol for ASEDs preparation in French university hospitals using a Delphi method, with the goal of improving ASEDs quality, safety, and supply.
Methods:
Method for consensus reaching is Delphi method. Four protocol parts are covered: blood sampling and controls, preparing and packaging the eye drops, postproduction controls, and storage and conservation. Expert panel are hospital pharmacists. Steps were as follows: questionnaire construction, mailing with link access to Google Forms®, response analyses, consensus rate calculation, result synthesis, and anonymous referral to experts.
Results:
With 12 answering experts, after 4 rounds: out of 39 proposals initially submitted, the work resulted in a 26 validated item protocol at the final. In sampling and controls: 15 items were validated, 5 dropped. Preparation: 5 were validated, 1 dropped. Postcompounding Control: 3 were validated, 4 dropped. Storage and Conservation: 3 were validated. The four rounds took 86 days.
Conclusions:
A standardized protocol for ASEDs preparation was proposed. This could improve the supply of care across the country. Method strengths are a consultation of dedicated experts on the draft questionnaire of the Delphi survey and qualified experts on the topic, anonymity avoiding opinion leader.
Introduction
Dry eye disease is a multifactorial pathology affecting the tear film and ocular surface. 1 It results in symptoms, of varying intensity, of discomfort, visual disturbance, and instability of the tear film, with potential damage and inflammation of the ocular surface.
It is one of the most frequent causes of consultation in ophthalmology. This condition affects millions of people throughout the world, particularly in South-East Asia and concerns 6% to 34% of the world’s population.2,3 In France, a 34.5% prevalence of dry eye, characterized by the presence of at least 2 clinical signs, is found in patients aged 82 years on average. In 33.3% of cases, patients had moderate grade dryness and in 1.2% of cases severe grade dryness.4,5
This high prevalence, its significant impact on quality of vision and life, and its financial cost make it a massive public health issue.
While the treatment of minimal-to-moderate forms is generally simple and effective, that of severe forms is often more challenging. The use of autologous serum eye drops (ASEDs) therefore represents a potentially interesting therapeutic alternative in the management of patients suffering from severe forms that are refractory to conventional treatments (artificial tears, topical immunosuppressants, contact lenses, punctual occlusion, systemic diseases appropriate management).
ASEDs contain growth factors (epidermal growth factor, nerve growth factor, transforming growth factor beta (TGFβ), insulin-growth factor 1 (IGF1), vitamins and fibronectin that can promote regeneration and proliferation of epithelial cells in the cornea and conjunctiva. 6 Controlled studies are still lacking, to assess the role of this therapeutic option.7–9 Variability in the preparation process for this eye drop could also lead to variations in the qualitative and quantitative composition of the eye drop, and there is no standardized production method. 10
In France, ASEDs preparation practices are very heterogeneous. 11 Their preparation is complex to implement, and the number of French establishments producing this treatment is limited: 13 out of 30 university hospital centers. This situation can lead to variations in the quality of eye drops between establishments, with a risk of loss of opportunity for patients for whom this may be a treatment of last resort.
The introduction of a standardized protocol throughout France could improve the range of treatment available by encouraging more centers to manufacture these eye drops, which are still too difficult to access.
The lack of regulations governing the production of eye drops, combined with varying levels of equipment and organization, does not facilitate the rollout of this preparation in France. The use of the Delphi method with pharmacists in university hospital centers in France who prepare such eye drops could help to define the outlines of a consensus protocol,12,13 to improve the quality, safety of use, and supply of ASEDs.
In this context, the primary objective is to develop a national consensus-based protocol for ASEDs preparation in French university hospitals using a Delphi method. Secondary objectives were to describe current heterogeneity into practices and to generate a practical stepwise protocol.
Methods
Delphi method applied to the survey
Composition and recruitment of the panel of experts
To understand the practices for preparing ASEDs in France and the capacity to standardize the preparation, we sought to involve pharmacists from centers performing these preparations.
We chose not to include other health care professionals involved in the care of patients using ASEDs because we focused on the preparation phase, which can impact the composition, quality, and safety of use. Furthermore, France has a dedicated regulation framework applicable to any hospital pharmacists. 14
We therefore wanted to recruit pharmacists implicated in production of ASEDs in French university hospitals.
The inclusion criteria for being recruited as experts were: pharmacists in French hospitals directly involved in the preparation of ASEDs, who agreed to participate throughout the Delphi survey, at each stage.
The exclusion criteria were as follows:
pharmacists involved in dispensing without preparation (through subcontracting with hospital pharmacies that perform this preparation). pharmacists who did not agree to participate and complete the questionnaires at each stage. pharmacists involved exclusively in the preparation of autologous plasma eye drops rich in growth factors (ie, using the Endoret® medical device technology). Other health care professionals (ophthalmologists, biologists, etc.) not directly involved in the preparation phase of ASEDs; in this case, they were asked to indicate the resource pharmacist involved in the production of ASEDs within their institution.
Pharmacists were recruited in September 2020 by email, on the basis of a previous review of practices, carried out in 2019, among those who reported compounding ASEDs. 11 The pharmacist heads of compounding units in centers that have not already prepared ASEDs at the time of the 2019 survey were also informed of the heterogeneity of practices and were invited to contact us if they had been asked to prepare them in the meantime.
The expert pharmacists from the participating centers agreed to collaborate after being informed of the objectives of the research work, the course of the study, and their role by a second email explaining the Delphi method.
Process of the method
Elaboration and completion of questionnaires
A steering committee formed the organizational team for the Delphi study. As defined in the article previously, their main tasks were to identify and recruit experts, draft and distribute successive versions of the questionnaires, analyze the results obtained, provide feedback to the experts after each round, and finally, write the final report.
The steering committee for the Delphi method was composed of the following professionals from the University Hospital of Limoges:
the pharmacy resident in charge of the study; the pharmacist responsible for the pharmaceutical preparations unit; a methodologist from the university hospital.
The steering committee drafted the questionnaire for the first round, taking care to choose targeted, precise, and, where possible, quantifiable questions. The questionnaire for the first round was developed using data from the March 2019 assessment of preparation practices conducted with 9 hospital pharmacists 11 and updated data through a literature review in the MEDLINE® database.
The 9 pharmacists who participated in the 2019 assessment evaluated the relevance of each of the 26 proposed items (to retain, remove, or modify) and were also asked to suggest new items for inclusion before launching the first round of the Delphi study.
This allowed us to identify all the steps to be addressed in standardizing preparation practices.
The items were broken down into the 5 parts of the standard preparation circuit, reworded to take account of the specific nature of ASEDs with the raw material “serum”: “Sampling and controls,” “Process of preparation and packaging,” “Controls after preparation,” “Storage and conservation,” “Dispensing and use by the patient.”
Following the responses received from the 9 pharmacists, the steering committee was able to draw up the first version of the Delphi questionnaire, comprising 39 items, divided into 4 parts as follows: sampling and controls, pharmaceutical operations of preparation and packaging, postproduction controls, and storage and conservation of the preparation. The “Dispensing and use by the patient” section was dropped because we felt it was inappropriate for standardizing preparation protocols and difficult to harmonize because it is the step following preparation, and it depended on all the parameters of the preparation protocol. We purpose to defer the question of the relevance of standardizing dispensing to a possible future project.
Each of the proposed items corresponded to a stage in the ASEDs compounding process. Consulted experts had to answer to any item by indicating: agree or not agree and adding, if justified, a comment or a reason (« called a reasoned response »). A positive convergence was defined when experts agree the item above the consensus threshold.
The questionnaires were distributed using Google Forms® software, a survey administration program offered free of charge by Google®. The questionnaires were accessible online via a link that the experts received in an invitation e-mail. Reminders were sent by e-mail in the event of a nonresponse, to maintain the same panel of experts for all the rounds.
The different versions of the questionnaire were drawn up by reformulating the items, after analyzing the responses from the previous round, which had not obtained a consensus or which had obtained a consensus but with discordant comments that were not supported or argued either scientifically or with regard to the Good Preparation Practices reference framework. 14 For each item reformulated and resubmitted in the next round, all the answers and comments obtained in the previous round were presented anonymously to the experts. This enabled them to reassess their degree of agreement for each item by comparing it with the group’s opinions and arguments.
Determining the consensus threshold
The panel of experts were asked about the consensus threshold to be chosen between 80% and 85%. These two thresholds, proposed by the steering committee, are among those commonly found in reviews evaluating the methodology to be adopted for establishing a Delphi methodology.15,16
Analysis of responses received
The results and any comments were exported to Excel for analysis. Responses and comments were analyzed after each round to allow for an iterative approach, with the following round being used to clarify, develop, and refine emerging perspectives. If necessary, clarifications were requested on certain responses between rounds, to limit the number of rounds and carry out a well-founded analysis of all the responses obtained, with as much accuracy as possible.
The items were analyzed by the steering committee, one by one, according to the answers obtained in each round. Three situations could be observed as follows:
Validated item: item having obtained a positive convergence, that is, a number of responses in agreement with the proposed item equal to or greater than the consensus threshold. Nonvalidated item:
Item which obtained a number of responses in agreement equal to or greater than the threshold but for which one or more participants made comments in opposition to the opinion of the group. This item was then reassessed and could be resubmitted to the experts in the next round, reworded or not (depending on the comments), with all the arguments presented; An item that did not obtain a number of responses in line with the threshold: after analyzing the comments and arguments, the item could be reworded to take account of the reasoning presented and then resubmitted in the next round, or if the majority of comments disagreed with the item, it could be proposed for abandonment in the next round. Any dropped item followed the same procedure as the validation of an item; it was submitted to the panel of experts with a favorable opinion having reached the consensus threshold.
The reformulated item in the next round was always accompanied by the elements of the reasoning that led to the reformulation and the bibliographic references systematically provided to the experts to help them make their decision.
All validated or abandoned items in each round were communicated to the experts.
Results
Experts on the panel
Following the review carried out in 2019 and the responses obtained after the pharmacists in charge of the ASEDs who were contacted by email, a list of 14 expert pharmacists was drawn up based on the French university hospital centers that are manufacturers. Of these 14 experts, 13 responded favorably and agreed to take part in our project.
These 13 participants were recruited from the following university hospitals across France: Angers, Bordeaux, Brest, Caen, Lille, Marseille, Nantes, Nice, Poitiers, Rennes, Rouen, Strasbourg, and Toulouse.
All 13 participants completed the first questionnaire. One of the participants mentioned compounding eye drops exclusively from plasma enriched with growth factors. As the criterion of the pharmacist in charge of ASEDs was not met, his establishment was excluded a posteriori from the second round and his responses from the first round were not considered. The panel was therefore reduced to 12 experts, all of whom responded in rounds 2 and 3. Only 10 of them responded to the fourth round.
Results related to the consensus threshold
To the question of the threshold (80% or 85%): a total of 5 experts out of 13 (38.5%) answered 80%, 4 (30.8%) chose the 85% threshold, one expert (7.7%) “voted” for both values, and 3 experts (23%) did not express an opinion. A consensus threshold of 80% was thus set, to be applied from the first round.
First round of the Delphi survey
The first round of questionnaires took place between September 02, 2021 and October 15, 2021 (43 days).
Out of 39 proposals submitted in the first round:
10 proposals obtained positive convergence (answers in agreement ≥ 80%): 8 proposals obtained positive convergence without disagreement or discordant comments and were therefore validated; 2 proposals obtained positive convergence, but also reasoned responses. They were also reformulated for their submission in the second round. 29 proposals did not obtain a positive convergence of responses (≤80%): 22 proposals were reformulated to be proposed again to the second round; 2 items were merged twice, leading 20 items to the second round; 6 proposals obtained argumentative responses in disagreement; the choice was therefore made to propose their abandonment in the 2nd round; 2 proposals were deleted by elimination and not proposed to the second round.
Figure 1 and Table 1 summarize the results of the first round of the Delphi survey.
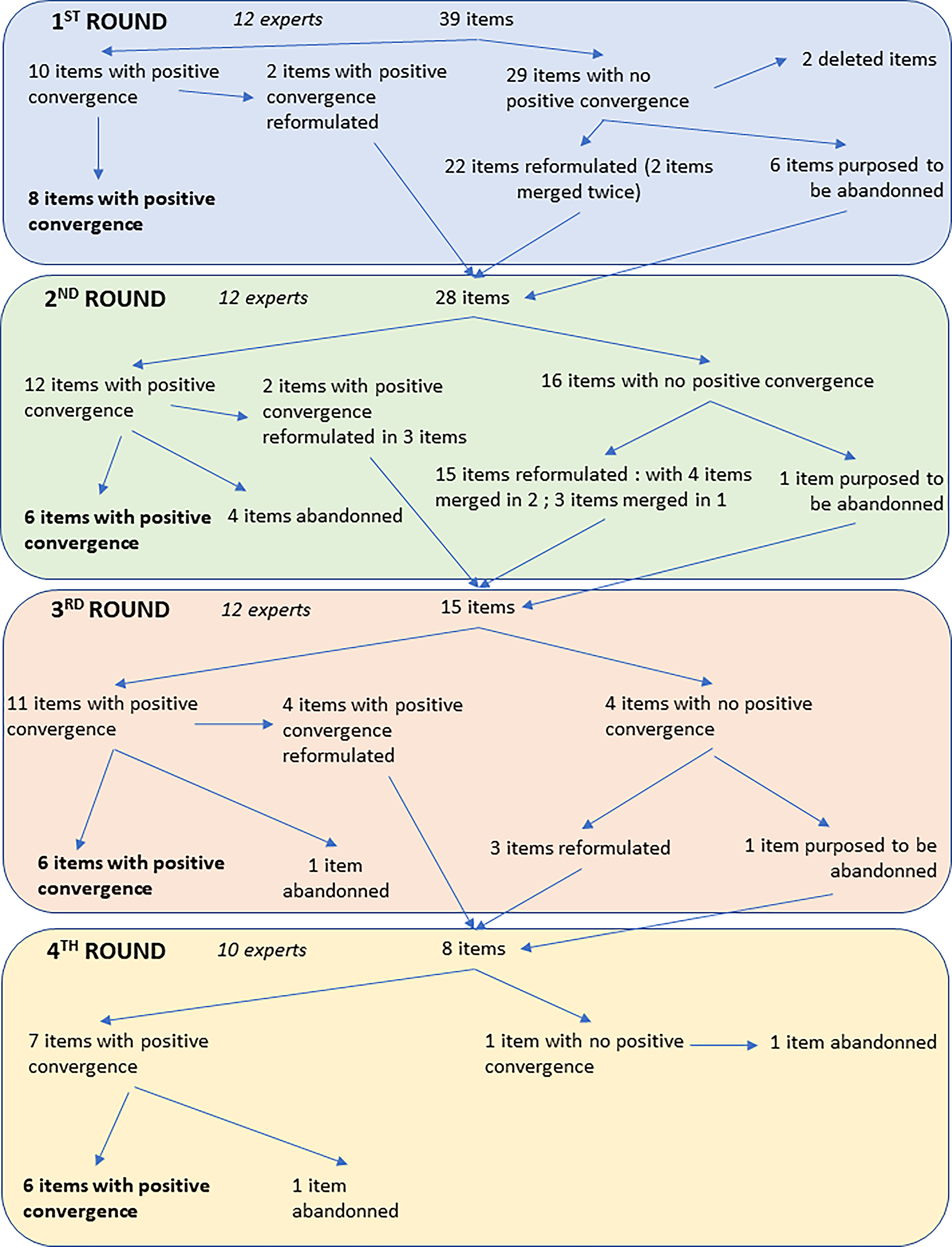
Flow chart summarizing the 4 rounds.
Summary of the Results of the 4 Rounds of the Delphi Process, with the Evolution of the Items Submitted to the Experts
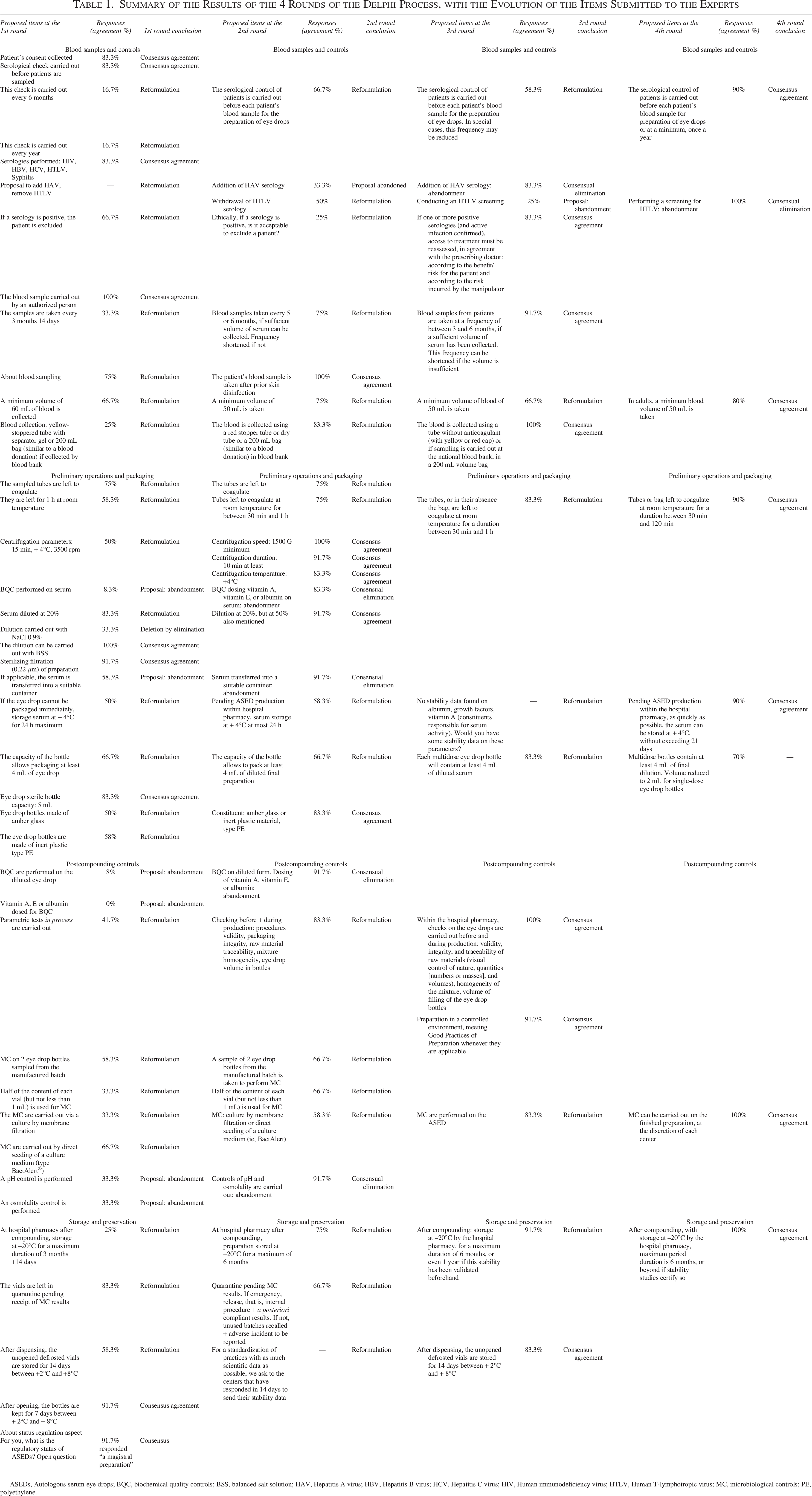
ASEDs, Autologous serum eye drops; BQC, biochemical quality controls; BSS, balanced salt solution; HAV, Hepatitis A virus; HBV, Hepatitis B virus; HCV, Hepatitis C virus; HIV, Human immunodeficiency virus; HTLV, Human T-lymphotropic virus; MC, microbiological controls; PE, polyethylene.
Furthermore, concerning the items on the constituent material of the eye drop bottles, amber glass or inert plastic, the participants’ responses were very heterogeneous, and without scientific data on the stability in contact with these materials. Also, participants were asked if they can provide bibliographic data and/or internal stability data.
Second round of the Delphi survey
The second round took place between February 1, 2022 and February 24, 2022 (23 days).
Out of 28 proposals submitted in the second round:
12 proposals obtained positive convergence (responses in agreement ≥ 80%): 6 proposals obtained positive convergence without disagreement or discordant comments and were therefore validated; 4 proposals were abandoned after obtaining positive convergence without disagreement or discordant comments following the proposal to abandon them; 2 proposals obtained positive convergence but also reasoned responses. They were also reformulated in 3 items for their submission to the third round. 16 proposals did not obtain a positive convergence of responses (≤80%): 15 proposals were reformulated, whose 2 items merged twice (leading to 2 items), and 3 items were merged in 1 item, leading to 11 items being proposed again in the third round; 1 proposal obtained reasoned responses in disagreement, and the choice was therefore made to propose its abandonment in the third round.
Figure 1 and Table 1 summarize the results of the second round of the Delphi survey.
Third round of the Delphi survey
The third round took place between June 1, 2022 and June 15, 2022 (14 days). Out of 15 proposals submitted in the third round:
11 proposals obtained positive convergence (responses in agreement ≥ 80%): 6 proposals obtained positive convergence without disagreement or discordant comments and were therefore validated; 1 proposal was abandoned after obtaining positive convergence without disagreement or discordant comments following the proposal to abandon it; 4 proposals obtained positive convergence but also reasoned responses. They were also reformulated for their submission to the fourth round; 4 proposals did not obtain a positive convergence of responses (≤80%): 3 proposals were reformulated to be proposed again in the fourth round; 1 proposal obtained reasoned responses in disagreement, and the choice was therefore made to propose its abandonment in the fourth round.
Figure 1 and Table 1 summarize the results of the third round of the Delphi survey.
Fourth round of the Delphi survey
The fourth round took place between August 11, 2022 and August 17, 2022 (6 days). Out of 8 proposals submitted in the fourth round:
7 proposals obtained positive convergence (responses in agreement ≥ 80%): 6 proposals obtained positive convergence without disagreement or discordant comments and were therefore validated; 1 proposal was abandoned after obtaining positive convergence without disagreement or discordant comments following the proposal to abandon it; 1 proposal did not obtain a positive convergence of responses (≤80%): “Each multidose eye drop bottle contains at least 4mL of final preparation, diluted. This volume is reduced to 2mL for single-dose eye drop bottles,” and was abandoned.
Figure 1 and Table 1 summarize of the results of the fourth round of the Delphi survey.
Summary of recommendations
To obtain a consensus, 4 rounds of Delphi were conducted between September 2, 2021 and August 17, 2022, over a total effective period of 86 days.
At the end of the 4 rounds of questionnaires, a total of 43 different items were submitted to the entire panel of experts.
Out of 39 proposals initially submitted, in the fourth round and after reformulation and merging of certain items, 26 items obtained a consensus rate of responses in agreement for their validation and 6 for their abandonment.
Table 2 lists all the initial proposals, reformulated or merged at the end of the 4 rounds of the Delphi, and therefore constitutes the complete standardized preparation protocol obtained.
Standardized Protocol Proposal
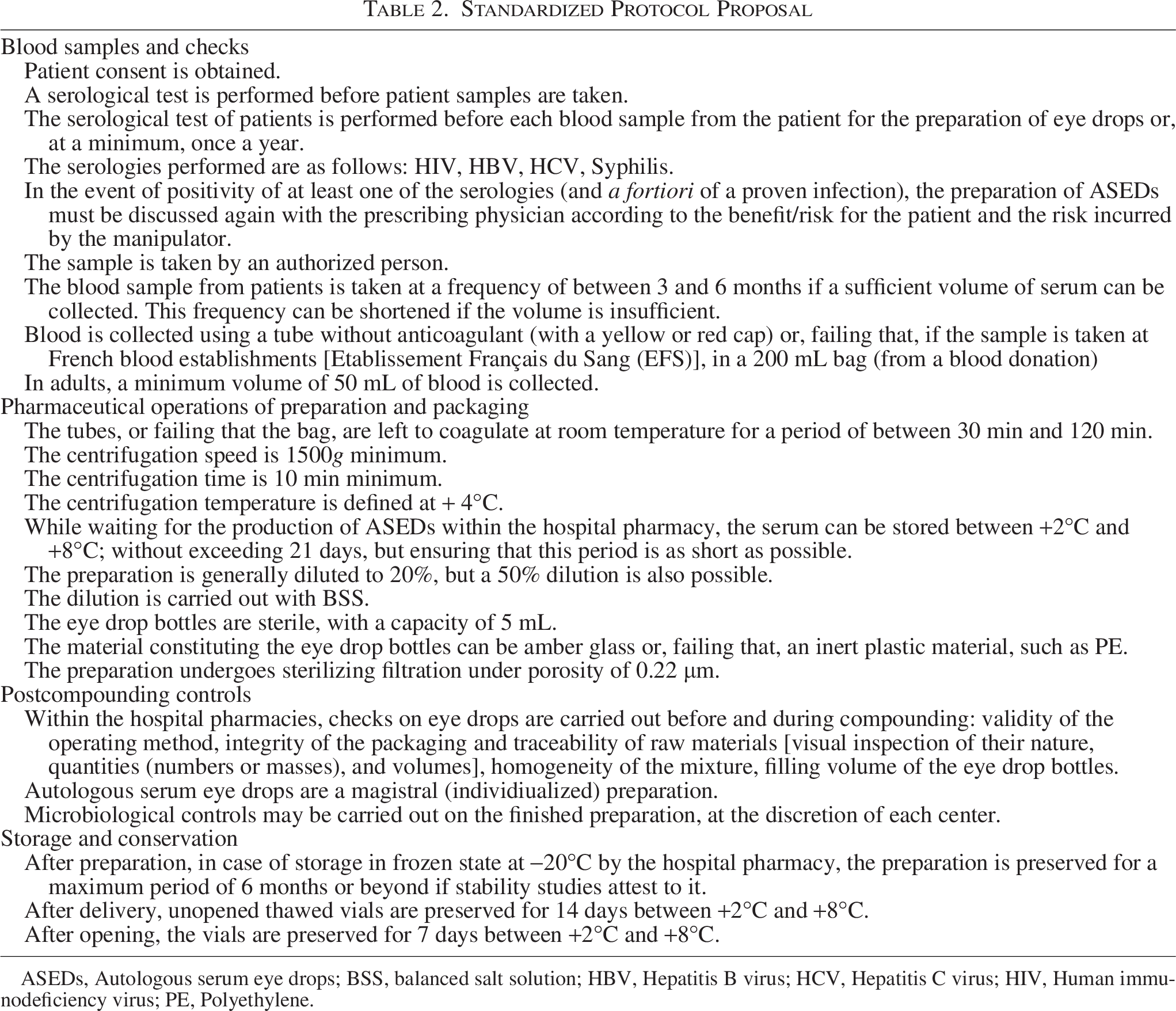
ASEDs, Autologous serum eye drops; BSS, balanced salt solution; HBV, Hepatitis B virus; HCV, Hepatitis C virus; HIV, Human immunodeficiency virus; PE, Polyethylene.
Table 3 is a short, high-level schematic checklist/box summarizing the key steps from this complete protocol.
Schematic Checklist/Box Summarizing the Key Steps from the Complete Protocol
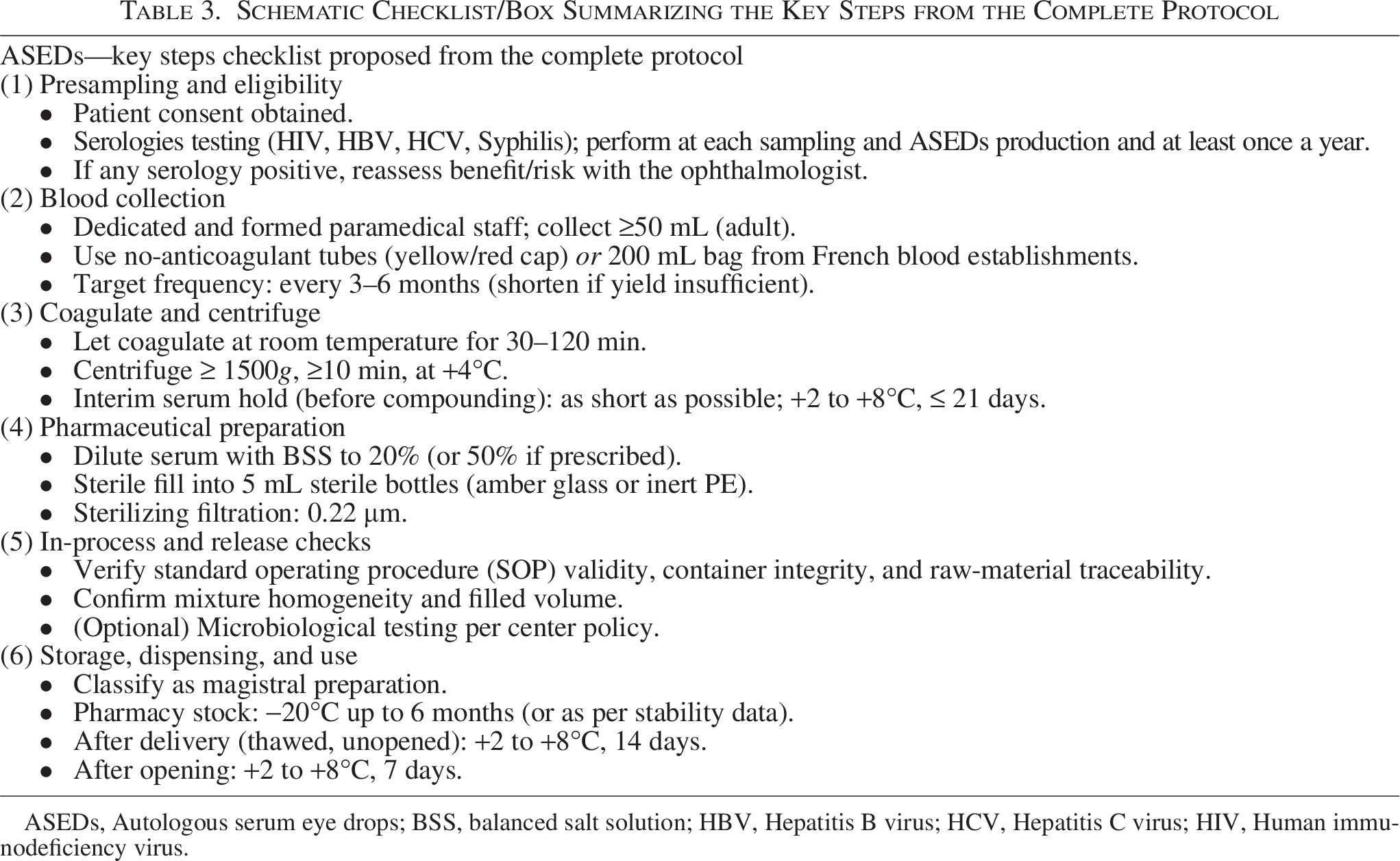
ASEDs, Autologous serum eye drops; BSS, balanced salt solution; HBV, Hepatitis B virus; HCV, Hepatitis C virus; HIV, Human immunodeficiency virus.
Discussion
The implementation of the Delphi method with pharmacists who have an experience in the preparation of eye drops has enabled the development of a feasible and secure protocol to facilitate the provision of these treatments to patients who require them. The objective of this theoretical work was to propose realistic guidelines for a protocol, with a view to its subsequent practical application. This constraint was respected throughout the work thanks to the selection of experts who regularly prepare ASEDs and led to the definition of a validated 26-items protocol covering all aspects related to preparation.
The Delphi method allows at the same time the pooling of data and knowledge. On the one hand, this survey allowed everyone to share their knowledge and scientific data on ASEDs. On the other hand, our consultations allowed the expression of knowledge not shared or available in the form of an official manner (poster, oral communication, publication) and therefore difficult to access. This is also the case for user knowledge. Thus, thanks to this Delphi questionnaire, we were able to obtain important additional stability data on the conservation of ASEDs at −20°C after preparation.
Also 10 items were abandoned using the same methods, within the framework of a consensus (agreement of at least 80% of the experts of the panel to abandon the item). In the majority of cases, the abandonment of items was due to a lack of scientific objectification, such as the choice of material constituting the eye drop bottles, or for the biochemical controls carried out on the undiluted serum (consensus rate of 8.3%).
To our knowledge, this work is the first on this topic in Europe, with a preparation provided in a pharmaceutical environment. Various protocols were carried out in various countries (United Kingdom, 17 United States, 18 Australia, 19 Japan 20 ) in nonpharmaceutical environments, such as blood services, tissue banks environment, or productions made in clinical ophthalmology services.
However, as proposed in our protocol, body evidence collected from systematic reviews has shown that sterile preparations in a pharmaceutical environment improve the microbiological quality of the preparation made and ensure the robustness of the preparation process.21,22
An experts’ feedback from South Korea is reported, 23 with authors that carried out an inventory of ASEDs preparation and control practices in their country, through a national survey, and assessment of preparation protocols published in other countries. They deducted standardized guidelines applicable for laboratories, in South Korea.
Compared with the standardized protocol finally obtained, the proposed guidelines in South Korea
23
provide following additional elements:
Human T-lymphotropic virus (HTLV) screening; a blood volume of 120 mL collected after eliminating the first 30–45 mL, that is, a collection volume closer to those carried out at the Etablissement Français du Sang in France; an item mentioning the transfer of the collected blood into “sterile 50 mL conical tubes,” a step not mentioned in our work, by any expert; a coagulation time of 120 min at room temperature, compared with a duration of between 30 min and 120 min at room temperature in our protocol; centrifugation at 3000g for 15 min (without any mention for temperature), compared with 1500g for 10 min at +4°C for our protocol; an item mentioning the following step, “The separated serum is transferred into a sterile conical tube using a sterile pipette or syringe.” We had proposed a similar item “If necessary, the serum is transferred into a suitable container,” which was abandoned by the majority in the second round; the possibility of diluting (or not) the serum, and in the event of dilution, the choice is left between Balanced Salt Solution (BSS) and 0.9% NaCl. A dilution of 20%, or even 50%, is carried out with our protocol using only BSS; microbiological controls are carried out by distributing “5 mL of undiluted or diluted serum in aerobic and anaerobic culture bottles,” controls that our consensus leaves to the discretion of each manufacturing center; an item mentioning a unit volume of “2 mL of undiluted or diluted serum poured into each sterile dropper bottle,” the only item that has not managed to be standardized in our work; an item concerning the labeling of the final preparation, a step not described in our protocol because labeling is uniform due to dedicated national regulation. the eye drops are then stored at −80°C until the results of the microbiological controls are obtained, an item not mentioned in our protocol because these controls are not mandatory for individualized « magistral » preparations. It should also be noted that in French hospital pharmacies, ASEDs are stocked at −20°C.
The choice of the Delphi method in our case and the respect of strict methodological quality criteria bring strengths to the protocol we propose. By recruiting qualified experts on the topic addressed, with a low number of follow-up, it gave access to the expertise and experience relating to the preparation of the ASEDs of each establishment concerned, while ensuring the diversity of points of view through their different practices. Anonymity of individual responses guarantees free expression of the experts, while limiting conflicts of interest and avoiding the possible influence of an « opinion leader ».
The method we performed allows consideration of extreme opinions. One of the main limitations of the Delphi method is that it usually does not retain extreme opinions. This bias was taken into account in our case by choosing to resubmit proposals that had obtained consensus but for which an expert expressed a contrary opinion. This gave all participants the opportunity to revise their opinion in the next round, in light of the contrary opinions.
The suggestibility bias (ie, the emergence of new ideas after the process had been launched, with the associated risk of overbidding) has been limited by encouraging experts to participate in creating the initial questionnaire. Thus, 5 new items were added and proposed during the first round: “The bottles are left in quarantine while awaiting receipt of the microbiological results,” “Biochemical quality controls are carried out on the patient’s serum,” “Biochemical quality controls are carried out on the diluted eye drops,” and “The molecules measured for this biochemical control are vitamin A, vitamin E, or albumin” (2 items).
The development of this protocol, even if limited to the critical preparation stage, through improved control of key steps (centrifugation, packaging, storage, and duration of use), is likely to reduce variability in the quality of ASEDs and potentially improve patient safety.
The development of this standard protocol is the essential first step and allows for minimizing the bias of pharmaceutical variability, enabling a prospective clinical evaluation in patients who have received ASEDs to assess potential clinical benefits in terms of efficacy and safety.
Consensus could not be reached on certain items, which therefore had to be dropped. This applies to the items concerning biochemical controls carried out on undiluted serum. The submission of these items to the panel should however be reiterated because, in the current state of knowledge, molecules as growth factors, vitamins, and albumin could be at the origin of the effectiveness of the ASEDs. But, more than the search for consensus on them, the most relevant work would be to evaluate their exact contribution in the action of the ASEDs. And, if their implication in the effectiveness is demonstrated, then it would be interesting, for a standardization of preparation protocol, to establish a range of concentrations to target for each molecule involved.
Some limitations of the procedure should however be noted.
Certain are due to the panel composition.
A possible bias is the selection of experts, by choosing to recruit only pharmacists involved in the preparation of ASEDs, without ophthalmologists, biologists, patients, or scientists. Such participants would probably have contributed their knowledge on certain specific points: ophthalmologists, on the relevance or not of treating patients contaminated (regarding human immunodeficiency virus (HIV), hepatitis B virus (HBV), hepatitis C virus (HCV), Treponema pallidum) or carrying a proven blood-borne infection. In the absence of a defined status for autologous blood in France regarding its handling and the biological validation of the sample’s use, to ensure the safe use of these eye drops, the biologist may use their expertise to select an optimized and appropriate strategy for blood collection and the detection of biological markers and to take into account the specific characteristics of patients who may be diabetic, cancerous, or on anticoagulants.
Regarding the dispensing of these eye drops, given that they are pharmaceutical preparations, the formalized guidelines associated with this pharmaceutical act would be best developed jointly with all health care professionals involved in patient care as well as with the patients themselves.
Furthermore, the nonparticipation of the National Hospital of Ophthalmology (CHNO) may have introduced another bias, since these were colleagues with the greatest experience in the field of producing eye drops in France. The consensus obtained therefore reflects the opinion of the pharmacist experts who responded favorably to our requests for participation.
Another point of limitation are the methodological constraints.
The average response time of the experts between each round is another limit. On average, it took 21 days to obtain responses from the entire panel of participants. This response time decreased as the rounds progressed, as if there was a virtual learning curve, and also less items to analyze. Nevertheless, reminders were necessary for each round to maintain responses from the entire panel of participants. It was after the sending of the questionnaire for the first round that the maximum number of reminders had to be ensured to obtain exhaustiveness in the responses.
For recurring discussion points, a bias in the processing of divergent judgments by the steering team cannot be also excluded.
Even though this approach was conducted in France, with specificities, particularly related to national legislation dedicated to preparation, this protocol provides key elements that are useful to any professional, wherever they may be, likely to implement ASEDs in their health care organization by indicating the key points of preparation: in particular, the importance of eligibility and biological screening, the methods of blood collection and treatment by coagulation, the key elements related to aseptic preparation, and the methods of storage and use of these ASEDs.
Conclusion
The Delphi process was an important step toward reaching a consensus on the proposal of a national protocol for the preparation of ASEDs. Through indirect consultation of manufacturing establishments, an exhaustive standardization of recommendations for preparation practices was proposed.
Indeed, the pooling, through the Delphi method, of the experiences, reflections, and questions of each party allowed a questioning of each person’s practices and the highlighting of points requiring clarification. The data and information sources used by each participant were also shared to argue any comments opposing the consensus opinion and therefore indirectly allowing a structured and enriching exchange for everyone. The discussion and pooling thus allowed certain stages of the preparation protocol to evolve and to move closer to a standardization of practices, to ensure the safest possible care for patients requiring this type of treatment. Furthermore, the provision of a standardized protocol can facilitate the development of ASEDs preparation in hospitals for which the absence of recommendations concerning this preparation constitutes a hindrance. The objective of this project was to obtain a final consensus and to propose an exhaustive framework for an ASEDs preparation protocol. The definition of these guidelines should make it possible to optimize the quality and therefore the therapeutic effects of ASEDs. However, there is a lack about controls (due to status consideration of these preparations by French manufacturers) and particularly biochemical ones (which will probably highlight knowledge about effectiveness of these eye drops). It is necessary for national and European authorities to take a greater interest in this subject and in particular in the regulation of ASEDs, in particular to define the status of this preparation.
Authors’ Contributions
L.C., D.L., M.C., J.J., P.-Y.R., M.R., and V.R.: Contributors. L.C., D.L., P.-Y.R., M.R., and V.R.: Conceptualization. L.C. and V.R.: Data curation. L.C., D.L., and V.R.: Formal analysis. J.J. and V.R.: Funding acquisition. L.C.: Investigation. L.C. and V.R.: Methodology. D.L., J.J., and V.R.: Project administration. J.J. and V.R.: Resources. L.C.: Software. D.L., M.C., J.J., P.-Y.R., M.R., and V.R.: Supervision. V.R.: Validation. L.C., D.L., and V.R.: Visualization. D.L.: Writing—original draft. M.C., J.J., P.-Y.R., M.R., and V.R.: Writing—review and editing.
Footnotes
Acknowledgments
Colleagues, from 14 university hospitals (CHU), formed the panel of experts or provided us useful information. In alphabetic order:
Binson Guillaume, CHU Poitiers Boivin Pierre-Nicolas, CHU Rennes Delmotte Nicolas, Assistance Publique—Hôpitaux de Marseille Deloison Emilie, CHU Caen Dory Anne, CHU Starsbourg Dugor Cathy, CHU Rennes Epinette de Bois Grollier Anne-Caroline, CHU Poitiers Hervouet Charles, CHU Rouen Hugerot Hélène, CHU Brest Lannoy Damien, CHU Lille Laurent Marion, CHNO des Quinze-Vingt Lester Marie-Antoinette, CHU Rennes Magalon Jeremy, Assistance Publique—Hôpitaux de Marseille Molignier Sara, CHU Poitiers Olivier Emmanuelle, CHU Nantes Ramjaun Zoubeir, CHU Toulouse Riutort Sandra, CHU Nice Saint-Lorant Guillaume, CHU Caen Tapon Amandine, CHU Brest Venet Arnaud, CHU Bordeaux Vrignaud Sandy, CHU Angers
Maillan Gaëlle, for proofreading Lucille’s thesis and for having judging thesis.
The « Epidémiologie des Maladies Chroniques en zone Tropicale » EpiMaCT Unit (Inserm U1094 IRD UMR270) for funding our first feasibility studies on the dosage of an active molecule in ASEDs.
Léo Pignol, pharmacy resident of our Galenic Pharmacy Unit, who helped to advance work on ASEDs, but was unable to promote them due to lack of time.
Author Disclosure Statement
No disclosure to declare from any of the contributors.
Funding Information
No funding was received for this article.