
Abstract
Introduction:
This retrospective study aims to assess the efficacy of infliximab by intravenous infusion in treating pediatric non-infectious uveitis, including as a second-line anti-tumor necrosis factor (TNF) for patients with insufficient control from adalimumab.
Introduction
Pediatric uveitis makes up approximately 5–15% of all uveitis seen in hospital eye services1,2 and has an overall prevalence of 25–30/100,000 population, 3 it can cause substantial visual morbidity through cystoid macular edema and sequalae of chronic ocular inflammation such as band keratopathy, cataract, and uveitic glaucoma (Fig. 1). The causes of uveitis in children are diverse; in the developing world, infectious agents and trauma are common, whereas in the developed world Juvenile Idiopathic Arthritis (JIA)-associated uveitis is the leading diagnosis. 4 JIA is the most common inflammatory arthritis of childhood and adolescence, with a prevalence of 16–150/100 000 population. 5 Approximately 1 in 5 patients with JIA develop uveitis, 6 which is predominantly of the anterior uveitis phenotype and follows a chronic relapsing course. It is frequently asymptomatic in the early stages, or the child is unable to express the symptoms, in contrast to adult anterior uveitis. Therefore, screening of children with JIA for uveitis in mandatory. 7 The lack of symptoms can make it difficult to convince children and parents of the importance of treatment, which initially involves topical corticosteroids. Due to the well-documented side effects of corticosteroids such as cataract formation and raised intraocular pressure, treatment is usually quickly escalated to steroid-sparing Disease Modifying Anti-Rheumatic Drugs (DMARDS) if control of inflammation cannot be established with, and maintained on, a very low dose of, corticosteroids. 8 Methotrexate is the steroid-sparing agent of choice.7,9
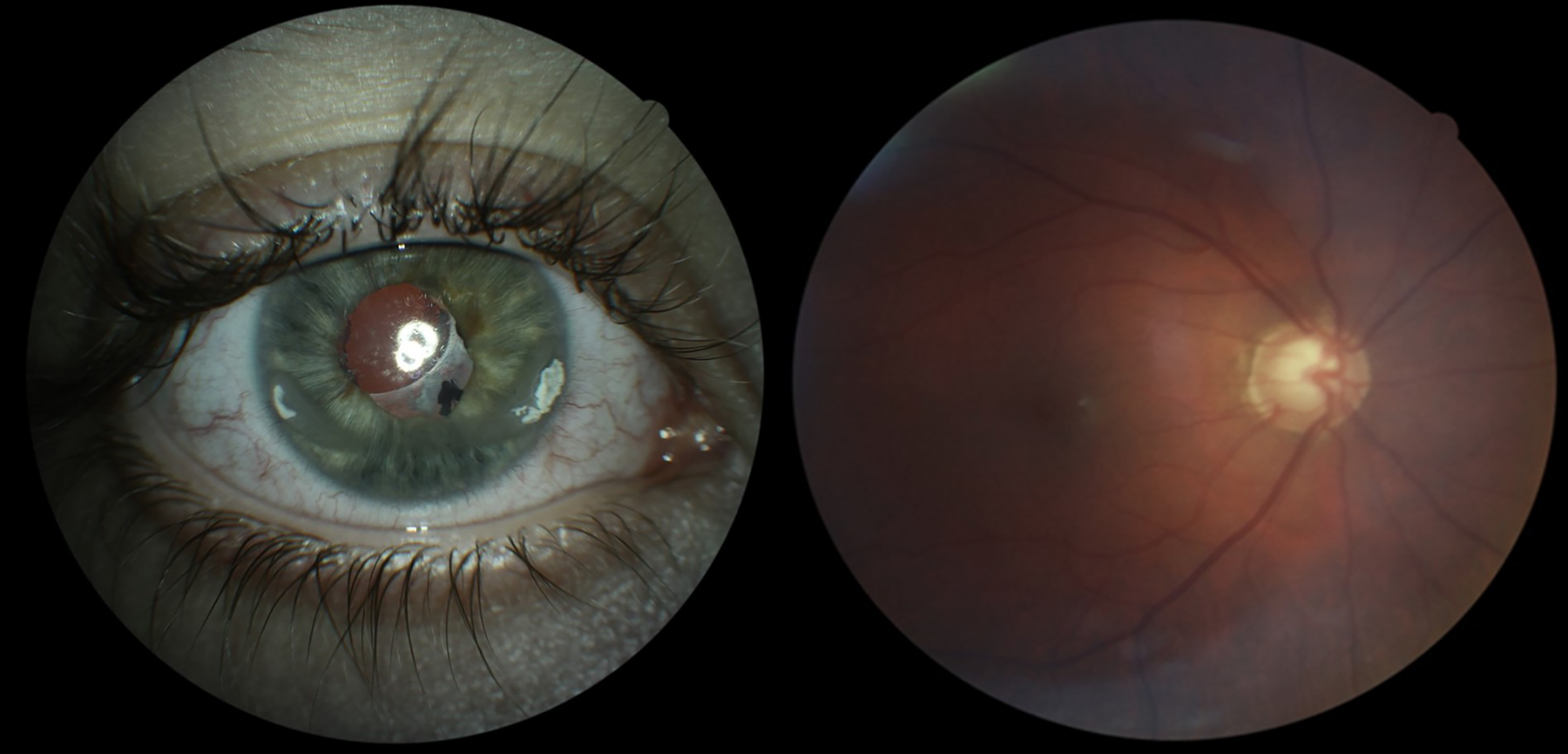
Left—image of a right eye with calcific band shaped keratopathy and pseudophakia following cataract surgery for uveitic cataract. Right—marked glaucomatous optic disc cupping due to chronic uveitic glaucoma.
Should DMARDS prove insufficient to control inflammation, the biological anti-tumor necrosis factor (TNF) agents are the next-line agents of choice. Since the first anti-TNF drugs were successfully deployed for the treatment of rheumatoid arthritis in 1993, 10 they have become a cornerstone of treatment for several inflammatory diseases. The SYCAMORE study provided strong evidence of the efficacy of adalimumab in addition to methotrexate for the control of JIA-associated uveitis. 11 Adalimumab is the first-line anti-TNF agent for JIA-associated pediatric uveitis, 9 and is the only anti-TNF agent funded by the National Health Service in England for the treatment of pediatric uveitis. 12 However, a proportion of patients do not respond to adalimumab, or initially respond before control of inflammation is then lost again. This cohort is particularly difficult to treat. Causes of treatment failure include noncompliance with treatment, intolerance to the drug, primary inefficacy, and the development of antidrug antibodies. These form as part of an immune reaction against the drug in around 37% of patients taking adalimumab for non-infectious uveitis 13 and can directly neutralize the action of the monoclonal antibody or increase the clearance of the drug. Lack of concomitant methotrexate therapy is associated with a higher risk of anti-drug antibody formation. 14 With regards to non-compliance with treatment, the requirement for infliximab to be administered via intravenous infusion means that treatment is supervised by health care professionals. This can improve compliance with infliximab therapy over that of adalimumab. Infliximab is an alternative to adalimumab with a similar mechanism of action, and a previous meta-analysis of studies comparing etanercept, adalimumab, and infliximab found similar efficacy of infliximab and adalimumab for childhood autoimmune uveitis. Both infliximab and adalimumab were superior to etanercept. 15 If control of inflammation is lost on adalimumab it can prove difficult to restore control without the use of other biological agents. Therefore, this study was initiated to examine the efficacy of off-licence use of infliximab in adalimumab non-responders. This is a retrospective study of all pediatric patients with uveitis at a single tertiary center who started infliximab between 2014 and 2023. Our aim is to demonstrate that infliximab is an effective therapy for pediatric non-infectious uveitis and an effective second-line anti-TNF medication.
Methods
The hospital electronic database (DAWN, 4S Information Systems Ltd., UK) was searched for patients taking infliximab between 2014 and 2023. All patients with a diagnosis of uveitis who were treated with infliximab (Remicade, Janssen Biotech, Inc.) were included. Infliximab intravenous infusion was at a dose of 5–6 mg/kg for a loading regime of 3 doses given at 0, 2, and 4 weeks, followed by a maintenance regime of 4–8 weekly. The initial loading regime reflects that commonly used for pediatric inflammatory bowel disease (licensed indication). Patient records were then examined manually to extract clinical data, including grade of anterior chamber (AC) inflammation based on clinical examination, best corrected visual acuity (BCVA), intra-ocular pressure (IOP), and concurrent medications used. Demographic data and diagnosis were recorded. Grade of AC inflammation was recorded as per the SUN classification 16 for cells in the AC. Visual acuity was reported in LogMAR where recordable. For low Visual Acuity (VA), counting fingers, hand movements, perception of light, and no perception of light were substituted with 2.10, 2.40, 2.70, and 3.00 LogMAR, respectively, in keeping with previous publications.17,18 Data were extracted at baseline, taken to be the visit at which the decision to initiate infliximab was made, and at 6 weeks, 6 months, 1 year, and 2 years post-initiation of infliximab therapy.
Analysis of the inflammatory activity was undertaken by assessing the AC inflammatory activity of the worse eye and by taking the mean of the AC inflammation scores of the 2 eyes at each time point. IOP in each eye was assessed at each timepoint. BCVA was assessed in each eye independently and in the worse eye at each timepoint. The frequency of topical corticosteroid eye drops was averaged between eyes at each timepoint. Statistical analysis was performed using GraphPad Prism version 10.1.2 (GraphPad Software, USA). Mean inflammatory activity score, BCVA, IOP, and topical corticosteroid burden were compared between time points using a one-way analysis of variance, with Dunnett’s correction for multiple comparisons. This work was undertaken adhering to the tenets of the Declaration of Helsinki.
Results
Fifteen patients were identified from the database as having been on infliximab in the timeframe of interest. Of these, 1 had been counselled for infliximab therapy but never started it. Another was transferred to our unit’s care while on infliximab, and no information was available regarding the grade of inflammation, vision, or IOP when treatment was started. These patients were both excluded.
Of the 13 patients included, there were 2 males and 11 females; the median age at initiation of infliximab was 9 years (range 6–16 years). Twelve patients had JIA-associated uveitis, of whom 7 had the polyarticular subtype of JIA, 3 had extended oligoarticular JIA, 1 had oligoarticular JIA, and 1 had psoriatic JIA. One patient had idiopathic panuveitis without underlying JIA. Demographic details are given in Table 1. Seven out of 13 (53.8%) of patients had structural uveitic complications, indicating the severity of disease in this cohort.
Demographic Information
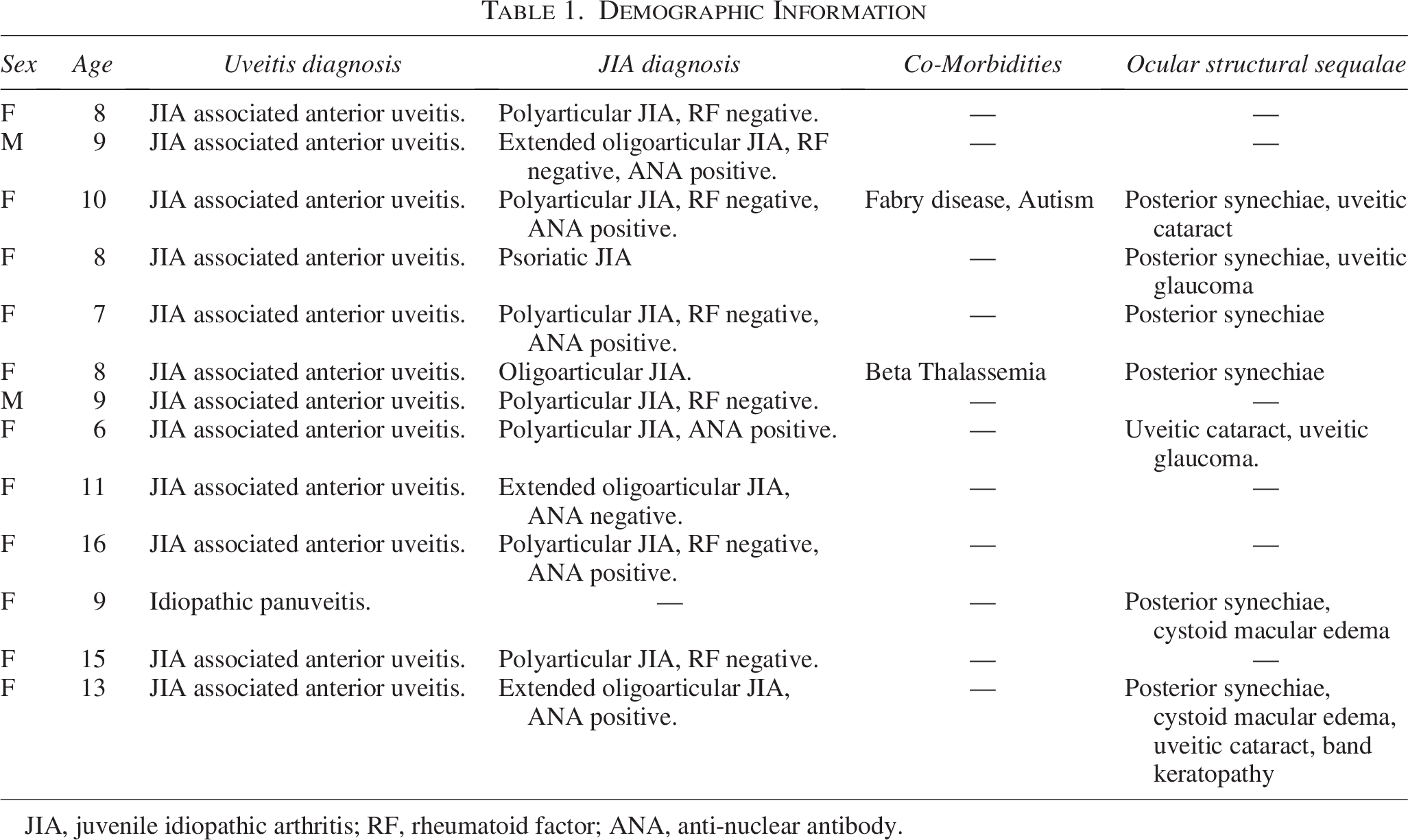
JIA, juvenile idiopathic arthritis; RF, rheumatoid factor; ANA, anti-nuclear antibody.
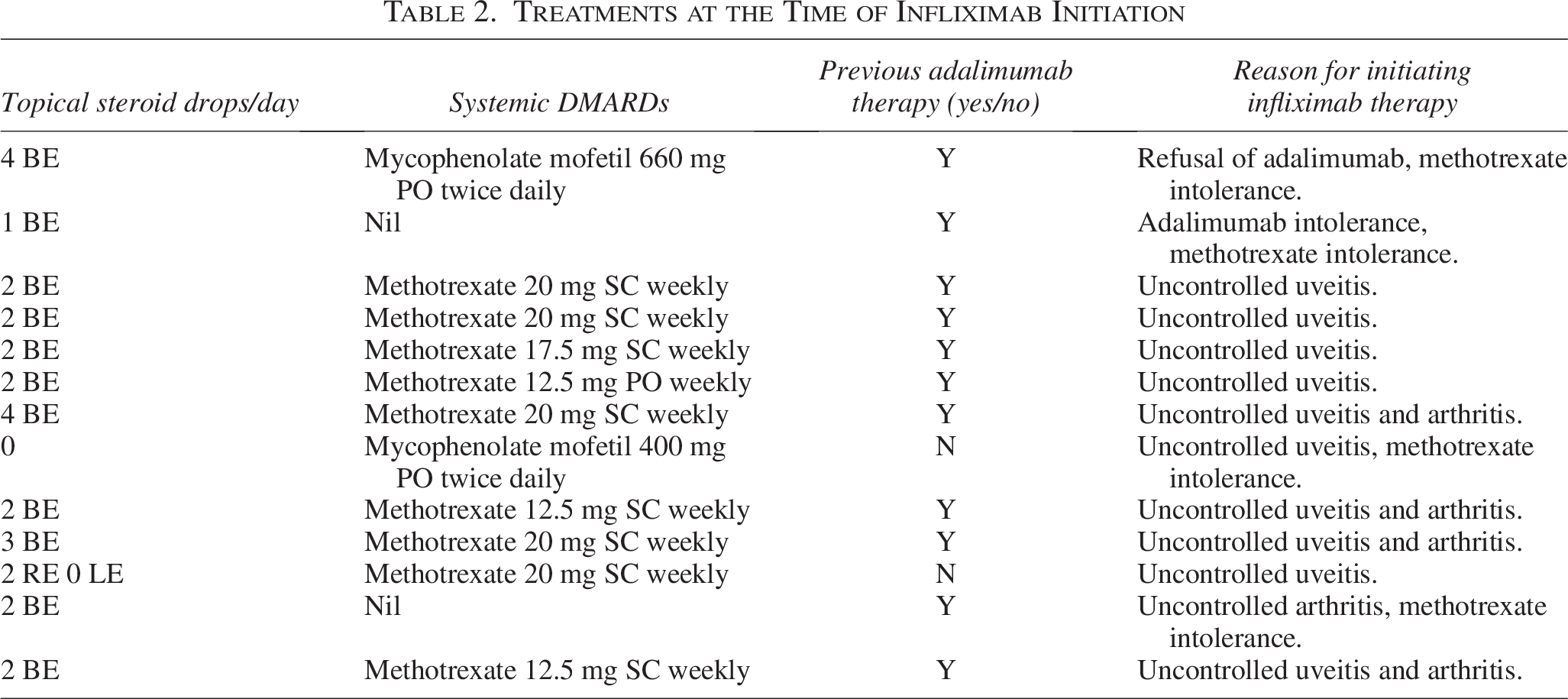
Of the 13 patients, all were already established on or had previously been on systemic immunomodulatory medications, either a DMARD or adalimumab, or more commonly both (Table 2). Eleven of 13 patients were on, or had previously been on, adalimumab therapy at the time of the decision to start infliximab. The decision to switch to infliximab was driven by inadequate disease control in terms of grade of inflammation within the anterior or posterior segments of the eye, as assessed by the treating clinician on clinical examination. The 2 patients who initiated infliximab prior to a trial of adalimumab did so before adalimumab became the standard first-line anti-TNF agent. Infliximab was given by intravenous infusion at a dose of 5–6 mg/kg in a loading regime of doses at 0, 2, and 4 weeks, followed by a maintenance regime of 4–8 weekly. Adalimumab standard dose was 20 mg Sub Cutaneous (SC) fortnightly for patients up to 30 kg body weight and 40 mg SC fortnightly for patients over 30 kg body weight.
Treatments at the Time of Infliximab Initiation
Control of inflammation
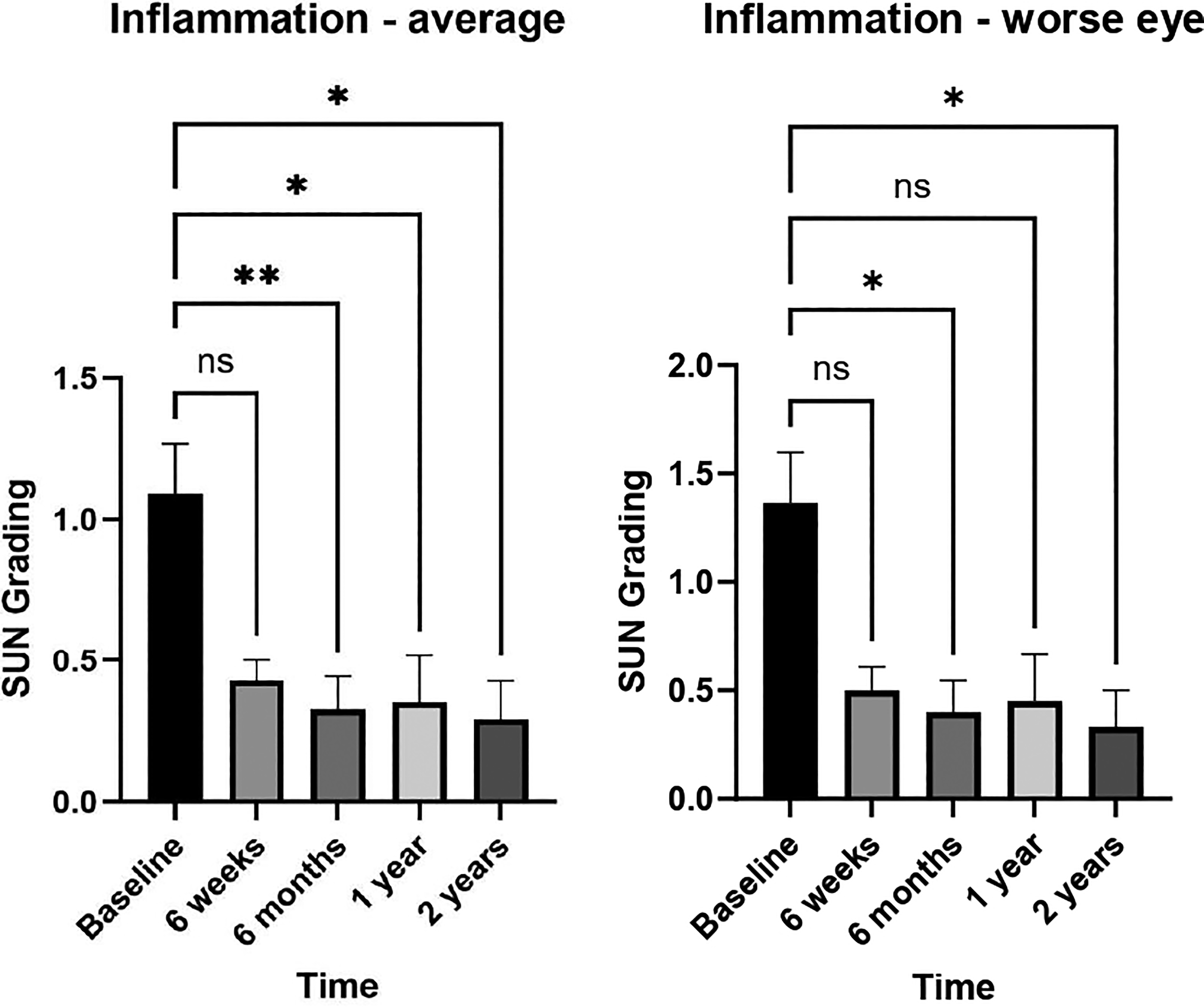
The mean grade of inflammation across both eyes at baseline (point of decision to initiate infliximab) was 1.08 (standard deviation [SD] 0.67, 95% confidence interval [CI] ± 0.36). There was a statistically significant improvement in the grade of AC inflammation at 6 weeks to 0.39 (SD 0.22, 95% CI ± 0.14, P = 0.02), 6 months to 0.27 (SD 0.36, 95% CI ± 0.20, P = 0.003), 1 year to 0.29 (SD 0.50, 95% CI ± 0.28, P = 0.013), and 2 years to 0.22 (SD 0.31, 95% CI ± 0.22, P = 0.02) after starting infliximab. These results are supported by the change in grade of inflammation in the worse eye, taken to be whichever eye had the higher grade of inflammation at the time of assessment. This is a more clinically relevant measure of treatment success, as decisions to modify treatment are driven by the control of inflammation in whichever eye is worse. There was a statistically significant improvement in the grade of AC inflammation in the worse eye from 1.31 (SD 0.83, 95% CI ± 0.49) at baseline to 0.33 (SD 0.44, 95% CI ± 0.25, P = 0.004) at 6 months, 0.38 (SD 0.64, 95% CI ± 0.36, P = 0.028) at 1 year, and 0.25 (SD 0.38, 95% CI ± 0.26, P = 0.015) at 2 years after starting infliximab. Improvement at 6 weeks just missed statistical signifcance at mean 0.50 (SD 0.35, 95% CI ± 0.23, P = 0.065) (Fig. 2).
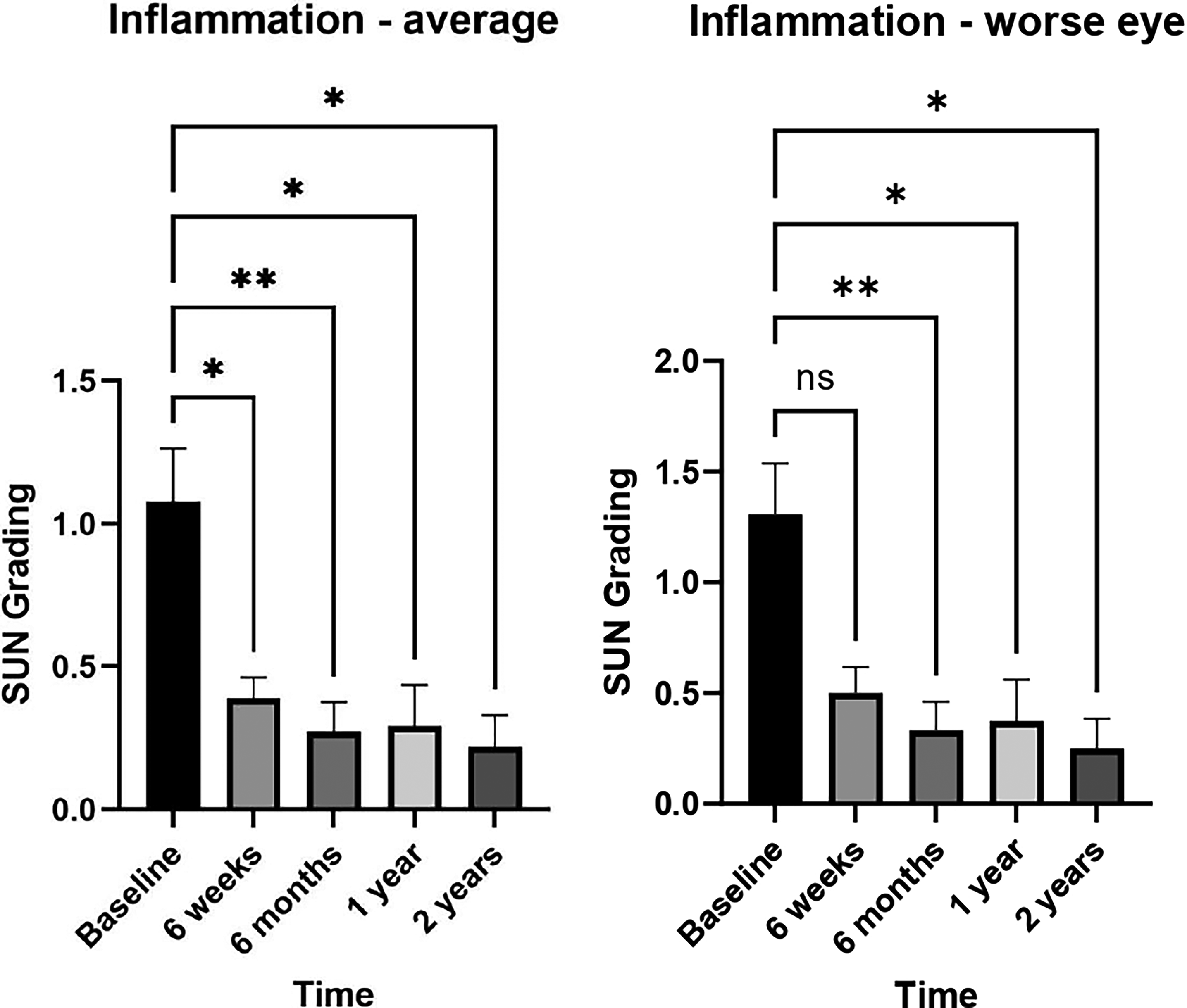
Infliximab therapy produces a significant improvement in both the average grade of inflammation between 2 eyes at all time points assessed (left), and in the grade of inflammation in the worse eye (right). *P < 0.05, **P < 0.01, error bars show SEM.
Visual acuity and IOP
Mean BCVA (LogMAR notation) did not significantly change from a mean of 0.19 (SD 0.27, 95% CI ± 0.16) in the right eye and 0.32 (SD 0.80, 95% CI ± 0.47) in the left eye at baseline. The BCVA in the worse eye did not significantly change from 0.41 (SD 0.80, 95% CI ± 0.47). Likewise, the mean IOP in mmHg did not significantly change from 15.2 (SD 4.0, 95% CI ± 2.40) in the right eye and 16.7 (SD 4.80, 95% CI ± 2.84) in the left eye (Fig. 3). One patient underwent cataract surgery during the course of follow-up for this study at 5 months following Infliximab initiation.
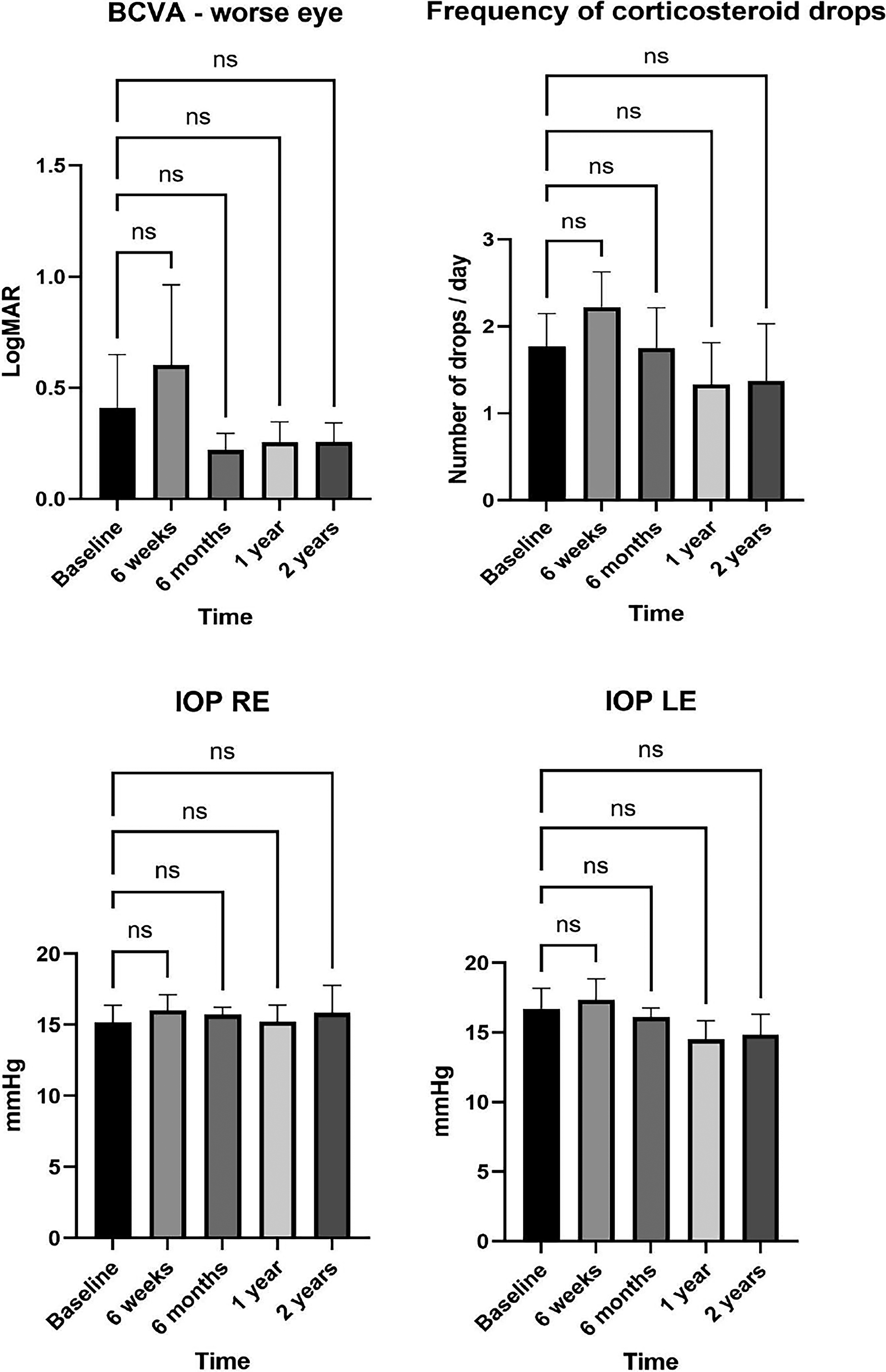
No significant difference is seen in IOP, visual acuity, or frequency of corticosteroid drops between baseline and any assessed time point. Error bars show Standard Error of the Mean (SEM). IOP, intra-ocular pressure.
Topical corticosteroid frequency
The mean frequency of topical corticosteroid drops at baseline was 1.77 applications per day (SD 1.36, 95% CI ± 0.74). This did not significantly change over the follow up period (Fig. 3).
Control of inflammation in adalimumab nonresponders
Of the 13 patients described here, 11 had been treated with adalimumab previously but had inadequate control of inflammation and so were switched to infliximab. The mean grade of AC inflammation for these patients at the time of decision to start infliximab was 1.09 (SD 0.58, 95% CI ± 0.34). There was a statistically significant improvement in the average grade of AC inflammation between the eyes at 6 weeks to 0.43 (SD 0.19, 95% CI ± 0.14, P = 0.037), 6 months to 0.33 (SD 0.37, 95% CI ± 0.23, P = 0.003), 1 year to 0.35 (SD 0.53, 95% CI ± 0.33, P = 0.021), and 2 years to 0.29 (SD 0.33, 95% CI ± 0.26, P = 0.027) after starting infliximab. In the worse eye, there was a statistically significant improvement in the grade of AC inflammation from 1.36 (SD 0.78, 95% CI ± 0.46) at baseline to 0.40 (SD 0.46, 95% CI ± 0.29, P = 0.008) at 6 months and to 0.33 (SD 0.41, 95% CI ± 0.33, P = 0.033) at 2 years after starting infliximab (Fig. 4). The trends towards better control in the worse eye at 6 weeks and 1 year did not reach statistical significance.
Switching to infliximab if control of intraocular inflammation is lost on adalimumab gives statistically significant improvements in anterior chamber inflammation in the worse eye at 6 months and 2 years (right) and in average anterior chamber inflammatory activity between two eyes after 6 weeks (left). *P < 0.05, ** P < 0.01, error bars show SEM.
Adverse events
One patient developed anaphylactic reactions to infliximab, which required that treatment be stopped. One patient developed neutralizing anti-drug antibodies to infliximab, as assessed by enzyme linked immunosorbent assay (ELISA). One patient’s parents refused to continue systemic therapies following a staphylococcal infection. Two patients were changed from infliximab to tocilizumab by their treating rheumatologist because of insufficiently controlled joint inflammation.
Discussion
Pediatric uveitis is a cause of substantial visual morbidity from a young age. Though good control of inflammation can be achieved in most cases with methotrexate therapy and the addition of adalimumab where required, a proportion of patients do not respond to adalimumab. Despite evidence of infliximab’s efficacy for pediatric patients with disease uncontrolled on DMARDs, there is limited information on the utility of infliximab for patients who do not respond to adalimumab, with only a few previous reports supporting its use. 19 There is also some evidence supporting a switch to infliximab for pediatric uveitis patients with disease refractory to etanercept, another anti-TNF agent. 20 The rationale for switching anti-TNF medications in cases of treatment failure lies in their differing structures. Adalimumab is a fully humanized IgG monoclonal antibody to TNF, whereas Infliximab is a chimeric IgG monoclonal antibody, 21 and they bind to distinct areas of the TNF molecule. 22 Studies from other TNF-driven diseases support the practice of switching between anti-TNF medications, for example, in inflammatory bowel disease, though success from a second agent is more likely if the switch is made due to intolerance rather than loss of disease control (secondary failure) and better in cases of secondary failure than where disease control was not established at all on the first treatment (primary failure). 23
The results presented here demonstrate that infliximab provides good control of intraocular inflammation in pediatric uveitis. Additionally, control of intraocular inflammation can be established with infliximab in a cohort of patients who have already proved resistant to adalimumab. Control of inflammation is vital to preventing the destructive sequalae of uveitis, which lead to lifelong visual morbidity. This provides a rationale for switch to a different anti-TNF agent if disease control is sub-optimal with a first agent and shows that a class switch away from anti-TNF agents to other biological agents is not necessarily required to establish control.
Over 2 years of follow-up, infliximab provides control of intraocular inflammation and maintains visual acuity at a level comparable to baseline. The lack of an improvement in best corrected visual acuity may reflect irreversible structural damage caused by the intraocular inflammation prior to infliximab initiation. In our cohort, 53.8% of patients had some structural sequalae of chronic uveitis, which are not reversible by later control of inflammation. No significant effect is seen on intraocular pressure nor on the number of topical corticosteroid applications, though a trend toward an increase at 6 weeks after baseline followed by a decrease thereafter is noticeable in the data. This is expected, as a short-term increase in corticosteroid eyedrop frequency is usually prescribed at the time of initiation of biological therapies to bridge the gap between initiation and therapeutic effects being seen. The topical therapy is tapered once control is established. It should also be noted that this cohort of patients who are resistant to 1 anti-TNF agent represents a group who have inflammatory drive which is unusually difficult to control. The lack of a reduction in topical steroid burden may reflect this or be due to a reluctance of the treating clinician to risk a flare in disease by tapering topical corticosteroids too much.
Three of 13 patients in this cohort sustained adverse events on infliximab, one case of anaphylaxis, one of anti-drug antibody formation, and one of staphylococcal infection. Additionally, two patients were switched from infliximab due to poor response of their arthritis to the therapy. This adverse event rate of 23.1% is keeping with that found in the broader literature on the subject. Anti-drug antibodies are a common development in patients treated with biological therapies, and data suggest that pediatric patients are more likely to develop these antibodies and develop them earlier than adult patients. 24 The extent to which anti-TNF therapies, and infliximab in particular, increases the risk of infection is not clear, but most studies do indicate some increased risk. 25 Interestingly, the combination of biological anti-TNF therapy with another immunomodulatory agent seems to give no additional risk. 26 This is a small-scale retrospective study, and in the future, prospective study methods will be required to corroborate these findings. A prospective study design may also allow stratification of patients for inclusion on JIA subtype, whereas this study has included all disease subtypes, and it would also permit multiple clinicians to grade inflammation using the SUN grading scale. This would guard against inter-rater variability. A standardized follow-up protocol would be a further advantage of prospective study design, which could also integrate objective measures of inflammation, such as anterior segment Optical Coherence Tomography (OCT). Other limitations of this study are more difficult to alter; for example, the large imbalance in patient sex is reflective of the epidemiology of JIA and uveitis in children. Our cohort of patients overrepresent polyarticular JIA-associated uveitis compared to the overall population of JIA patients. It is not possible to determine from our sample whether these patients are more likely to fail adalimumab therapy overall or whether there are differences in the responsiveness of different uveitis subtypes to infliximab. These questions would be best examined by large-scale randomized trials.
In summary, switching to an alternative anti-TNF agent such as infliximab if uveitis control is lost with adalimumab can significantly improve control of inflammation, which can have long-term beneficial effects for maintaining vision. Clinicians should be aware that loss of disease control with adalimumab should not preclude use of a second anti-TNF agent. Infliximab may be an effective agent, particularly in recalcitrant cases failing adalimumab therapy. Policymakers should also be aware of this and consider routinely funding infliximab for pediatric patients who have active uveitis while on adalimumab therapy.
Authors’ Contributions
I.R.R.: Conceptualization, methodology, investigation, analysis, article writing, article review and editing. L.R.: Methodology, investigation, article review and editing. E.A.-A.: Conceptualization, methodology, article review and editing, supervision. S.P.G.: Conceptualization, methodology, article review and editing, supervision. J.W.: Conceptualization, methodology, article review and editing, supervision.
Ethics
The study was conducted as a retrospective study in accordance with the Declaration of Helsinki. The study was registered with and approved by the host institution, registration number—CARMS-31587.
Informed Consent/Patient Consent
Informed consent for publication of individual data was provided by a legally authorized representative of the patient.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
The authors received no funding for this work.