
Abstract
Purpose:
To compare the efficacy, safety, and patient satisfaction of bepotastine besilate 1.5% versus sodium cromoglycate 4% eye drops in the management of chronic allergic conjunctivitis.
Methods:
In this prospective, double-masked comparative study, 100 adult patients with chronic allergic conjunctivitis were assigned to receive either bepotastine twice daily (n = 50) or cromolyn 4 times daily (n = 50) for 6 months. The primary outcome was the change in ocular itching severity on a standardized 0–3 scale. Secondary outcomes included changes in redness, tearing, swelling, discomfort, treatment compliance, adverse events, and patient satisfaction. Assessments were conducted at baseline, 2 weeks, 6 weeks, 3 months, and 6 months.
Results:
Both treatments significantly improved symptoms from baseline after 6 months. Bepotastine showed superior reduction in ocular itching severity (74.4% improvement) compared to cromolyn (63.8%, P < 0.01). Cromolyn was more effective in reducing conjunctival redness (70.0% vs. 59.3%). Bepotastine also showed numerical advantages in tearing, swelling, and discomfort relief. Adverse events were mild and comparable, with slightly more burning sensation reported in the cromolyn group. Compliance and patient satisfaction were higher in the bepotastine group, attributed to its convenient twice-daily dosing.
Conclusions:
Both bepotastine besilate and sodium cromoglycate are effective and safe for chronic allergic conjunctivitis. Bepotastine offers faster relief of itching and greater convenience, whereas cromolyn provides better control of conjunctival redness. Treatment choice should be individualized based on symptom profile and patient preferences.
Introduction
Allergic conjunctivitis represents one of the most prevalent ocular conditions encountered in clinical practice in India (19.1%–29.2% prevalence among children), particularly in high-humidity coastal regions like Kerala (study site), and significantly impacts quality of life. 1 Environmental factors contribute substantially to allergic conjunctivitis prevalence. In Kerala, the dominant airborne pollens include Poaceae (grasses), Cocos (Coconut), Artocarpus (Jackfruit), Amaranthus/Chenopodium, and Tridax, along with tropical species such as Areca catechu and Casuarina equisetifolia. These allergens are abundant in the coastal environment and contribute to persistent year-round symptoms. Allergic conjunctivitis represents one of the most prevalent ocular conditions encountered in clinical practice, affecting between 15% and 40% of the global population and significantly impacting quality of life. The condition manifests as a bilateral inflammatory response of the conjunctiva triggered by allergen exposure, with chronic forms presenting particular management challenges. Although seasonal and perennial allergic conjunctivitis constitute the majority of cases, chronic variants such as vernal keratoconjunctivitis and atopic keratoconjunctivitis often require sustained therapeutic intervention due to their persistent and recurrent nature.2,3
The pathophysiology of chronic allergic conjunctivitis involves complex immunological cascades, primarily mediated through immunoglobulin E-dependent mast cell degranulation and the subsequent release of inflammatory mediators including histamine, leukotrienes, and prostaglandins. This immediate hypersensitivity reaction is often followed by a late-phase response characterized by eosinophil infiltration and chronic inflammation, particularly in severe cases. The result is a constellation of debilitating symptoms including intense ocular itching, conjunctival hyperemia, chemosis, tearing, and photophobia that can persist for months or years without appropriate treatment. 4
Current therapeutic strategies for chronic allergic conjunctivitis rely heavily on topical antihistamines and mast cell stabilizers, either as monotherapy or in combination formulations. These agents work through complementary mechanisms—antihistamines provide rapid symptomatic relief by blocking histamine H1 receptors, whereas mast cell stabilizers offer preventive effects by inhibiting mediator release from mast cells. 5 However, the optimal choice between different therapeutic options remains a subject of clinical debate, particularly in chronic cases where both immediate symptom control and long-term disease management are essential. 6
Bepotastine besilate 1.5% has emerged as a promising dual-action therapeutic agent, combining potent histamine H1-receptor antagonism with mast cell stabilizing properties. Beyond its antihistaminic effects, bepotastine demonstrates anti-inflammatory actions through inhibition of leukotriene B4 synthesis and suppression of eosinophil migration, potentially offering superior efficacy in chronic inflammatory conditions. Clinical studies have demonstrated rapid onset of action within 15 min of instillation, with sustained effectiveness lasting 8–16 h.
In contrast, cromolyn sodium 4% represents the archetypal mast cell stabilizer, preventing degranulation through calcium channel blockade and forming stabilizing complexes with mast cell membranes. Although highly effective for prophylactic treatment, cromolyn’s mechanism necessitates consistent use over days to weeks for optimal benefit, with its primary advantage being excellent long-term safety and minimal systemic absorption. Recent evidence suggests cromolyn may also act through GPR35 receptor activation, adding complexity to its therapeutic profile. 7
Despite their widespread clinical use, direct comparative data between bepotastine and cromolyn sodium in chronic allergic conjunctivitis remain limited. Most existing studies focus on individual agent efficacy or compare these medications against a placebo rather than head-to-head comparisons. This knowledge gap is particularly significant given the distinct pharmacological profiles, onset characteristics, and patient-specific factors that may influence treatment selection. Understanding the relative efficacy, safety, and patient-reported outcomes of these 2 therapeutic approaches is crucial for optimizing management strategies in chronic allergic conjunctivitis, where treatment decisions must balance rapid symptom relief with long-term disease control and tolerability considerations.
Methods
Study design and setting
This prospective, double-masked, comparative study was conducted at a tertiary eye care center at INHS Sanjivani, Kochi, Kerala, India. All patients resided within 50 km radius, ensuring uniform environmental exposure, between January 2025 and July 2025. The study protocol was approved by the Institutional Ethics Committee. All procedures adhered to the tenets of the Declaration of Helsinki, and written informed consent was obtained from all participants.
Participants
Inclusion criteria
Adults aged 18–65 years with chronic allergic conjunctivitis (duration ≥6 months) Baseline symptom severity score ≥2 on a 0–3 scale for ocular itching Positive history of allergic symptoms with identifiable triggers, with primary allergens being house dust mite, pollen, animal dander, or multiple Ability to comply with study visits and procedures
Exclusion criteria
Active ocular infection or nonallergic inflammatory conditions Use of topical or systemic anti-allergic medications within 2 weeks Contact lens wearers (unless discontinued for study duration) Pregnancy, lactation, or significant systemic illness Previous adverse reactions to study medications No use of systemic antihistamines, oral/topical corticosteroids, or other anti-allergic medications during the 6-month study period
Randomization and intervention
Eligible patients were randomized 1:1 using computer-generated randomization to receive either of the following:
Group A (n = 50): Bepotastine besilate 1.5% eye drops, 1 drop twice daily (BID) Group B (n = 50): Cromolyn sodium 4% eye drops, 1–2 drops 4 times daily (QID)
Both medications were provided in identical opaque bottles to maintain masking. Patients were instructed on proper instillation technique and compliance monitoring.
Masking protocol
Patients received identical opaque dropper bottles, preventing visual/volume identification. Investigators were masked to treatment allocation but aware of assigned dosing schedules (BID vs. QID) during compliance counseling and assessments. No unmasking events occurred. Primary efficacy endpoint (ocular itching) was the patient reported using standardized questionnaires completed independently prior to physician examination.
Outcome measures
Primary endpoint
The primary efficacy endpoint was the change in ocular itching severity score from baseline to 6 months (0–3 scale: 0 = none, 1 = mild, 2 = moderate, 3 = severe).
Secondary endpoints
Changes in redness, tearing, swelling, and discomfort scores Treatment compliance assessed by self-report and medication counts Adverse events and safety parameters Patient satisfaction scores (0–10 scale) Time to symptom improvement 0 = none (no symptom present) 1 = mild 2 = moderate 3 = severe
The symptom severity score used in this study refers to a standardized grading system for key symptoms of allergic conjunctivitis with average severity experienced over the prior 24 h, measured on a scale from 0 to 3 for each symptom. The specific scale is as follows:
For example, the ocular itching severity is rated by patients or investigators at each study visit using this scale. This same 0–3 scoring applies to other symptoms such as redness, tearing, swelling, and discomfort.
Data collection
Patients were evaluated at baseline, 2 weeks, 6 weeks, 3 months, and 6 months. At each visit, symptom severity was assessed using standardized questionnaires wherein patients independently completed validated questionnaires rating (average severity over the prior 24 h) for each symptom (ocular itching, redness, tearing, swelling, discomfort) using the standardized 0–3 scale (0 = none, 1 = mild, 2 = moderate, 3 = severe) immediately prior to physician examination. This 24-h recall period standardizes assessment across varying visit timing and captures therapeutic response to chronic therapy, and clinical examination was performed by masked investigators. Digital photography documented conjunctival changes when appropriate.
Statistical analysis
The recorded data were analyzed using commercial software (SPSS Version 24.0; SPSS, Inc., Chicago, IL). Sample size calculation determined 50 patients per group would provide 80% power to detect a 0.5-point difference in symptom scores (α = 0.05). Continuous variables were analyzed using t-tests or Mann–Whitney U tests, and categorical variables were analyzed using chi-square or Fisher’s exact tests. Statistical significance was set at P < 0.05.
Results
Baseline characteristics
One hundred patients with chronic allergic conjunctivitis were enrolled and randomized (50 per group). Baseline demographics were similar between groups, with mean ages of 32.3 ± 10.3 years (bepotastine) and 37.2 ± 10.1 years (cromolyn) (Fig. 1). Females comprised 48% (24/50) of the bepotastine group and 58% (29/50) of the cromolyn group (P = 0.37). Average symptom duration was 29.9 ± 12.7 months (bepotastine) and 22.8 ± 11.8 months (cromolyn). All baseline characteristics were comparable, including primary allergen exposure. Study conducted during stable non-monsoon period (January to July 2025) with minimal pollen variation.
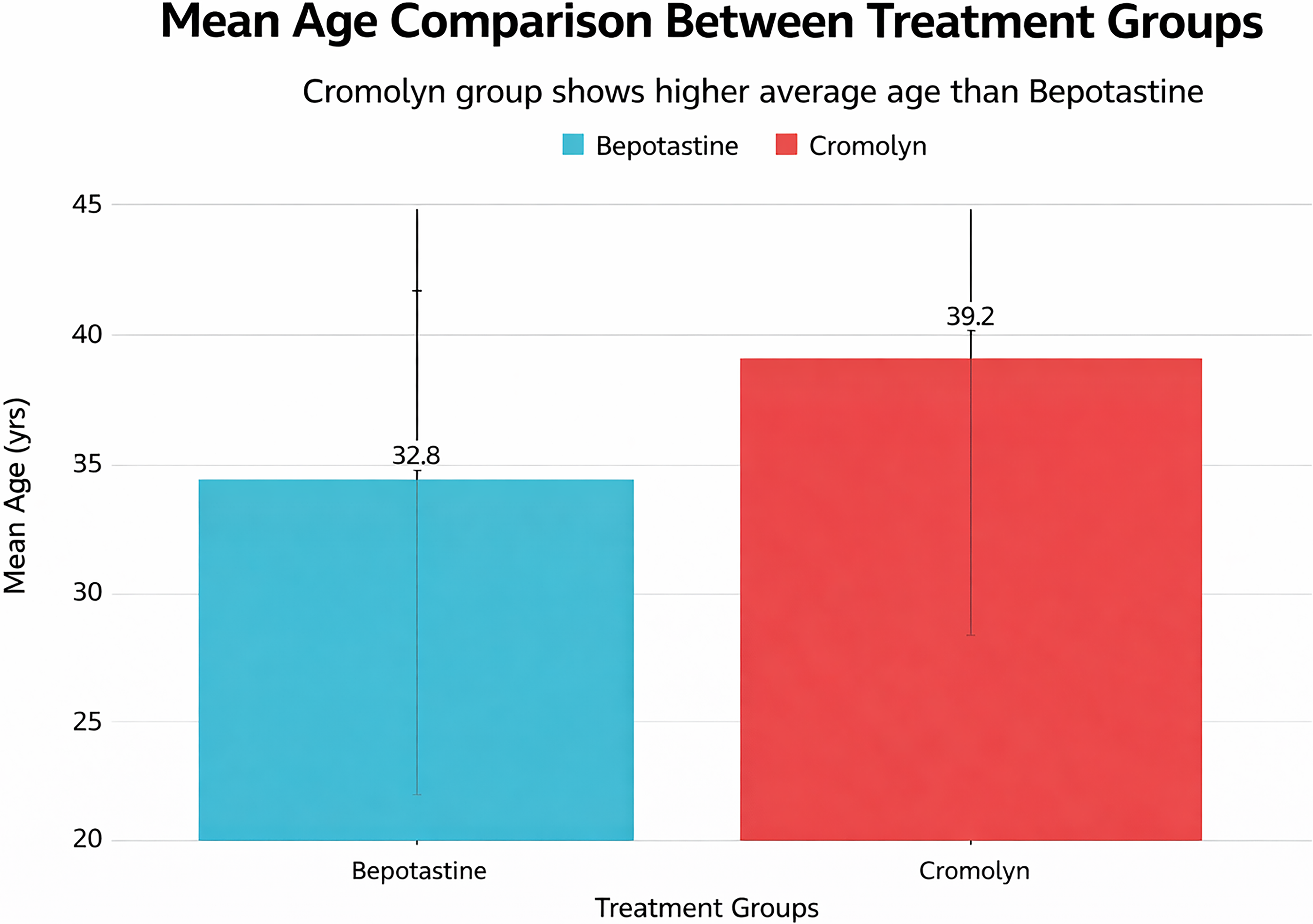
Mean age of study participants between the 2 groups treated with bepotastine and cromolyn.
Primary efficacy outcomes
At 6 months, both treatments demonstrated significant symptom improvement from baseline. Bepotastine showed superior efficacy for ocular itching, with mean scores decreasing from 2.28 ± 0.39 to 0.58 ± 0.11 (74.4% improvement), compared to cromolyn’s reduction from 2.09 ± 0.34 to 0.76 ± 0.17 (63.8% improvement, P < 0.01) (Fig. 2).
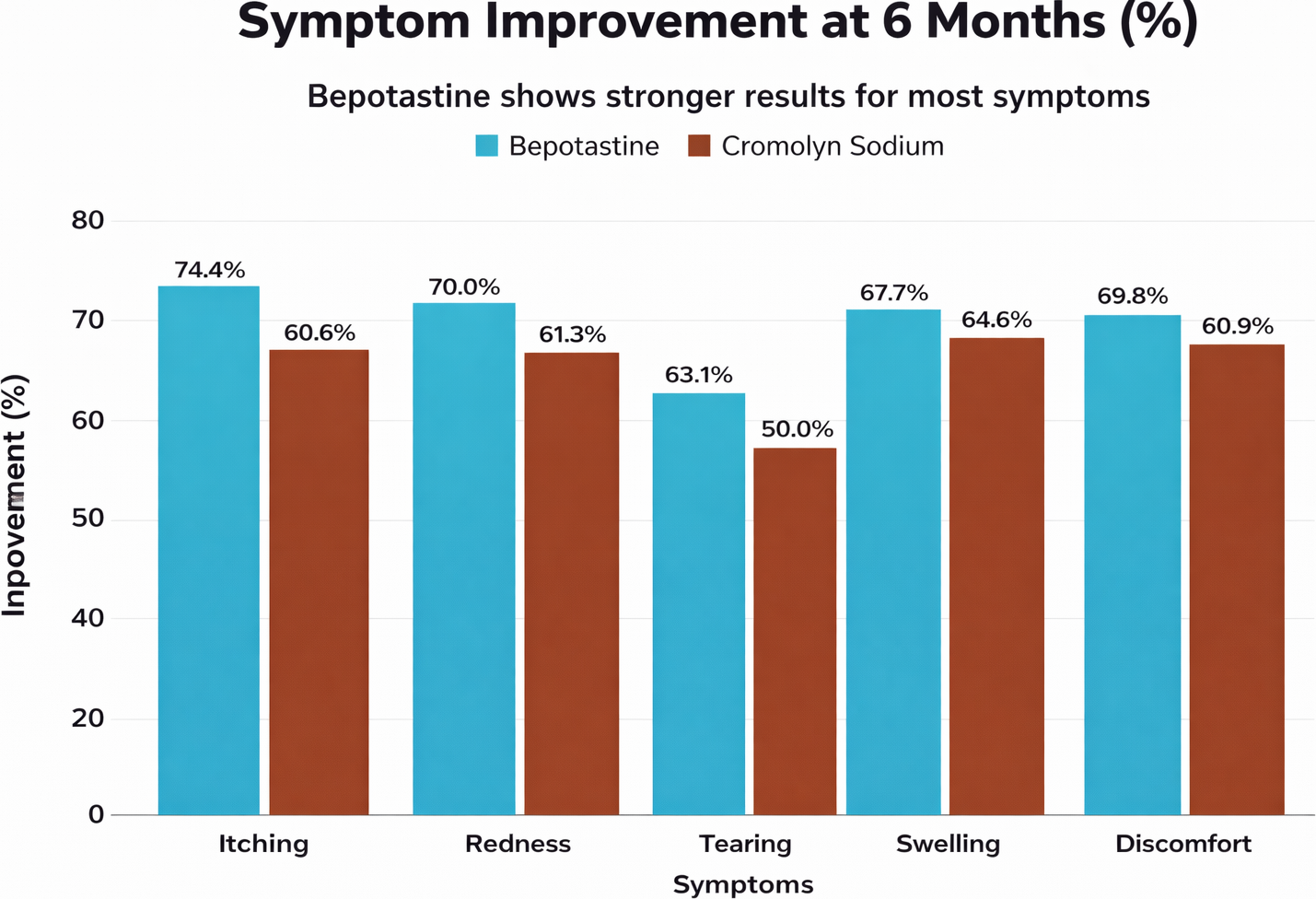
Comparison between improvement in symptoms at 6 months with the use of bepotastine versus cromolyn.
Secondary efficacy outcomes
Cromolyn demonstrated superior efficacy for conjunctival redness, with 70.0% improvement versus bepotastine’s 59.3% improvement. For other symptoms, bepotastine showed numerical advantages: tearing (63.1% vs. 58.9%), swelling (69.7% vs. 64.8%), and discomfort (69.8% vs. 60.0%).
Safety and tolerability
Both treatments were well tolerated. Side effects occurred in 5 patients (10.0%) in the bepotastine group and 7 patients (14.0%) in the cromolyn group. The most common adverse events were mild burning/stinging upon instillation, more frequent with cromolyn (8.0% vs. 4.0%). No taste disturbances (bitter taste, unpleasant aftertaste) were reported in either group despite bepotastine’s known mild nasolacrimal drainage effect in product labeling. This may be attributable to careful patient instruction on nasolacrimal occlusion, which reduces systemic absorption and minimizes drainage into the oropharynx. The absence of taste complaints in our cohort also reflects the relatively small sample size and possible underreporting of minor sensations. All reported adverse events were ocular (burning/stinging) with no systemic taste complaints. No serious adverse events were attributed to study medications.
Compliance and patient satisfaction
Compliance was excellent in both groups, with 74.0% of bepotastine patients and 70.0% of cromolyn patients reporting “always” compliant behavior. Patient satisfaction scores favored bepotastine (7.8 ± 1.2 vs. 7.2 ± 1.4), although the difference was not statistically significant (P = 0.08). The study was successfully completed with no dropouts, demonstrating the feasibility and acceptance of both treatment regimens in chronic allergic conjunctivitis management over a 6-month period.
Discussion
The results of this 6-month comparative study provide valuable insights into the differential efficacy profiles of bepotastine besilate 1.5% and cromolyn sodium 4% in chronic allergic conjunctivitis management. Our findings demonstrate that both agents offer significant therapeutic benefits, but with distinct patterns of symptom improvement that reflect their underlying pharmacological mechanisms and clinical positioning.
Primary efficacy findings
The superior performance of bepotastine in controlling ocular itching (74.4% improvement vs. 63.8% for cromolyn) aligns with established literature demonstrating the rapid antihistaminic effects of dual-action agents. This finding corroborates previous conjunctival allergen challenge studies where bepotastine demonstrated statistically significant reduction in ocular itching within minutes of application, with sustained effectiveness for up to 8 h. The magnitude of improvement observed in our study (74.4%) is consistent with real-world clinical data showing that approximately 80% of patients achieve complete resolution of primary allergic symptoms after 60 days of bepotastine therapy. 4
The mechanism underlying bepotastine’s superior antipruritic efficacy involves its dual pharmacological action as both an H1-receptor antagonist and mast cell stabilizer. Unlike traditional antihistamines that solely block histamine receptors after mediator release, bepotastine’s mast cell stabilizing properties prevent the initial degranulation cascade, thereby addressing both the immediate and late-phase allergic responses. This dual mechanism is particularly advantageous in chronic allergic conjunctivitis, where sustained inflammation perpetuates symptom severity and requires comprehensive mediator control.
Conversely, cromolyn’s superior performance in reducing conjunctival redness (70.0% vs. 59.3% for bepotastine) reflects its established efficacy as a pure mast cell stabilizer with potent anti-inflammatory properties. This finding is consistent with the drug’s mechanism of action, which primarily focuses on preventing inflammatory mediator release rather than blocking histamine receptors. 8 Clinical studies have consistently demonstrated cromolyn’s effectiveness in reducing conjunctival hyperemia, limbal edema, and other inflammatory signs, particularly with sustained use over weeks to months. 3
Clinical significance and treatment selection
The differential efficacy patterns observed in our study have important implications for personalized treatment selection in chronic allergic conjunctivitis. Bepotastine appears optimal for patients prioritizing rapid symptom relief, particularly those with severe ocular itching as the predominant complaint. The drug’s twice-daily dosing regimen (compared to cromolyn’s 4-times-daily requirement) may also enhance patient compliance and convenience, factors crucial for long-term management of chronic conditions.
Cromolyn remains valuable for patients requiring sustained anti-inflammatory control, especially those with prominent conjunctival hyperemia and inflammatory signs. 9 Its excellent long-term safety profile, minimal systemic absorption, and lack of tachyphylaxis make it particularly suitable for pediatric populations and patients requiring extended therapy. The drug’s prophylactic nature also makes it ideal for patients who can anticipate allergen exposure and prefer preventive treatment strategies.
Safety and tolerability considerations
Both treatments demonstrated excellent safety profiles in our study, with adverse events occurring in 10.0% (bepotastine) and 14.0% (cromolyn) of patients. These rates are consistent with published literature, where the most common side effects include mild burning/stinging upon instillation, particularly with cromolyn. The slightly higher adverse event rate with cromolyn likely reflects the increased frequency of instillation (QID vs. BID), leading to more frequent exposure to potential irritants.
The absence of serious adverse events in our study supports the favorable safety profiles established in larger clinical trials. Bepotastine’s safety database includes over 1,000 patients with no significant systemic absorption or drug-related serious adverse events. Similarly, cromolyn’s safety record spans decades of use across multiple formulations and patient populations, with minimal systemic exposure (<0.07% absorption from ophthalmic solutions). 10
Compliance and patient-reported outcomes
The high compliance rates observed in both groups (74.0% for bepotastine and 70.0% for cromolyn) likely reflect the chronic nature of symptoms and patients’ motivation for sustained treatment. However, the numerical advantage for bepotastine may relate to its more convenient twice-daily dosing schedule compared to cromolyn’s 4-times-daily requirement (Fig. 3). Previous studies have demonstrated that dosing frequency inversely correlates with long-term adherence in chronic ophthalmic conditions. 11
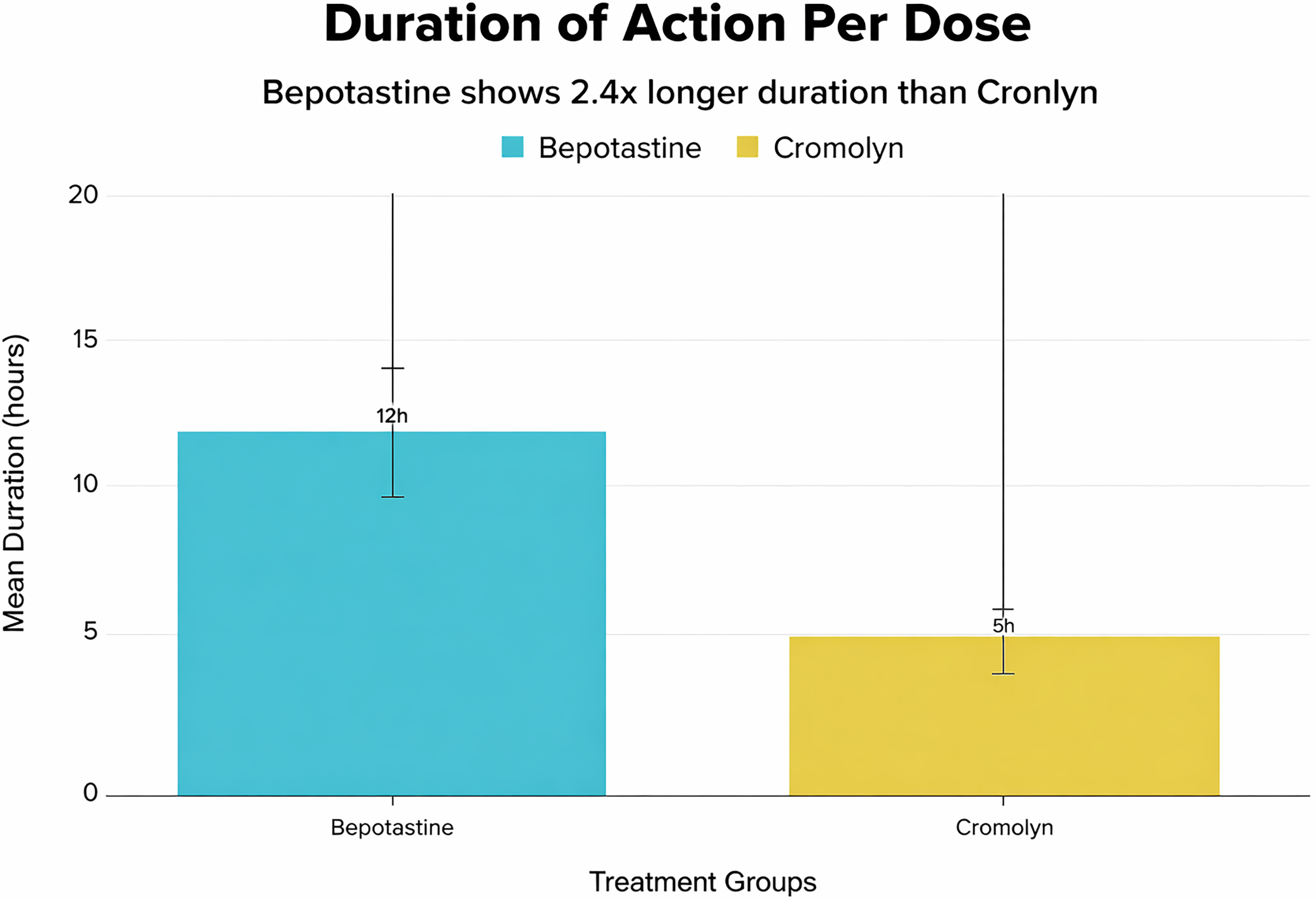
Comparison of the drug duration per dose between bepotastine and cromolyn.
Patient satisfaction scores favored bepotastine (7.8 ± 1.2 vs. 7.2 ± 1.4), although the difference did not reach statistical significance. This trend may reflect patients’ preference for rapid symptom relief and dosing convenience, factors that significantly influence treatment satisfaction in chronic allergic conditions.
Study limitations and clinical context
Several limitations warrant consideration when interpreting our results. The study design did not include a placebo control group, precluding assessment of absolute treatment effects. Additionally, the 6-month duration, although adequate for chronic condition evaluation, may not capture seasonal variations in symptom severity or long-term safety profiles. Environmental allergen monitoring (pollen counts/aeroallergens) was not performed during the study period (January to July 2025), consistent with standard methodology for chronic/perennial allergic conjunctivitis trials where symptoms demonstrate year-round persistence independent of seasonal exposure peaks. Due to Kerala’s tropical monsoon climate, the region experiences a hot pre-monsoon season (March to May), heavy rainfall during the southwest monsoon (June to September), lighter rains during the northeast monsoon (October to November), and a relatively mild winter (December to February). These weather patterns, combined with the prevalence of grass, Coconut, Jackfruit, and Amaranthus pollens, result in continuous allergen exposure with peaks during the late rainy and dry seasons. This background may explain the chronic nature of allergic conjunctivitis observed in our study population. The absence of objective measurement tools such as conjunctival allergen challenge or standardized hyperemia grading scales limits the precision of efficacy assessments.
Furthermore, our patient population represents a specific demographic (adults aged 18–65 years) and may not be generalizable to pediatric or geriatric populations, where safety and efficacy profiles may differ. The exclusion of contact lens wearers also limits applicability to this significant patient subgroup.
Investigator blinding was partial due to differing dosing frequencies (BID vs. QID), potentially introducing assessment bias. However, the primary outcome (ocular itching) remained patient reported and unaffected. This pragmatic design mirrors real-world clinical practice where medication regimens differ by indication.
Future research directions
Our findings highlight the need for head-to-head comparative studies with standardized outcome measures and longer follow-up periods. Future research should incorporate objective assessment tools, quality-of-life measures, and health economic analyses to provide comprehensive treatment comparisons. Additionally, studies evaluating combination therapy approaches and personalized treatment algorithms based on symptom patterns and patient characteristics would enhance clinical decision making.
The emergence of newer dual-action agents and novel delivery systems also warrants comparative evaluation against established therapies like bepotastine and cromolyn. Understanding the optimal sequencing of treatments and the role of combination therapy in refractory cases represents another important research priority.
Future research should establish a comprehensive efficacy ranking through 3-way RCTs comparing modern dual-action agents—bepotastine besilate 1.5% (BID), alcaftadine 0.25% (BID), olopatadine hydrochloride 0.2% (QD)—using identical endpoints (ocular itching as primary; composite symptom scores secondary) over 6–12 months. Such head-to-head data, absent from current literature, would enable evidence-based treatment algorithms balancing rapid onset, symptom spectrum coverage, dosing convenience, and long-term tolerability.
Conclusion
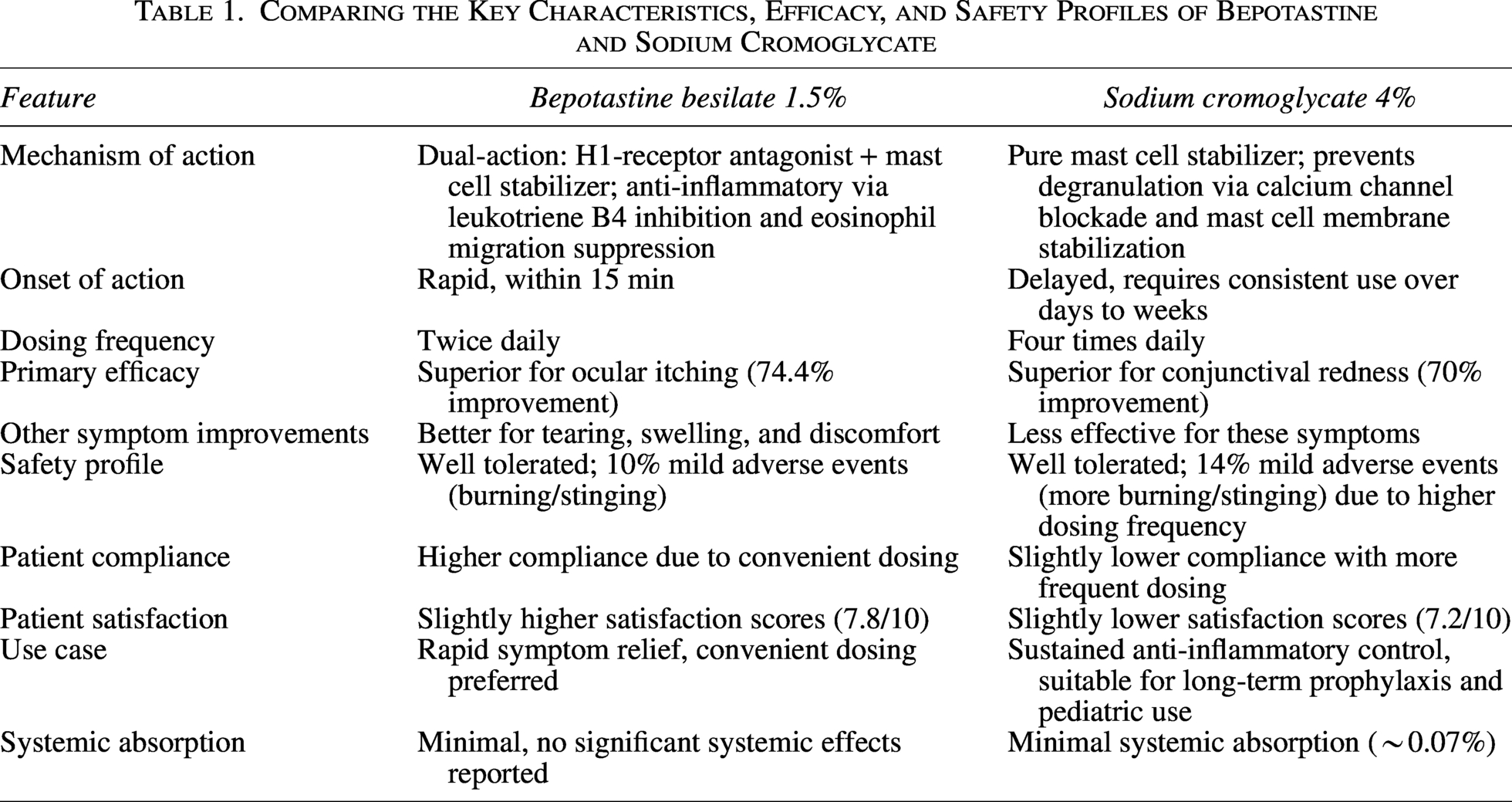
Based on our study results, both bepotastine besilate 1.5% and cromolyn sodium 4% represent effective therapeutic options for chronic allergic conjunctivitis, with complementary efficacy profiles that support individualized treatment selection. Clinicians should consider bepotastine for patients prioritizing rapid symptomatic relief and dosing convenience, whereas cromolyn remains optimal for those requiring sustained anti-inflammatory control and long-term safety assurance (Table 1). The excellent safety profiles of both agents support their continued use as first-line therapies in chronic allergic conjunctivitis management.
Comparing the Key Characteristics, Efficacy, and Safety Profiles of Bepotastine and Sodium Cromoglycate
Authors’ Contributions
All authors contributed to the study conception and design. Material preparation and data collection were done by M.J., and analysis was performed by A.N. The first draft of the article was written by S.G., and all authors commented on previous versions of the article. All authors read and approved the final article. The requirements for authorship as stated earlier in this document have been met, and each author believes that the article represents honest work.
Footnotes
Author Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
The authors received no financial support for the research, authorship, and/or publication of this article.