
Abstract
Purpose:
To evaluate the clinical role, durability, anatomical response, and safety for suprachoroidal triamcinolone acetonide (SCTA) (Xipere) in routine clinical practice.
Methods:
Data were manually extracted from health records at a high-volume retina practice in Cleveland, Ohio. All patients with noninfectious inflammatory macular edema undergoing SCTA (≥1 billing code) between October 25, 2021, and July 17, 2025, were included. Patients with known systemic autoimmune or infectious associations were excluded. Unique eyes were defined by MRN + laterality, with “OU” entries split into OD/OS. Patient demographics, underlying diagnosis categorization, time between first and second injection (for eyes with ≥2 injections) were summarized. Pre- versus post-treatment central retinal thickness (CRT) and intraocular pressure (IOP) were compared via paired t-tests.
Results:
A total of 177 patients (195 eyes) received 340 SCTA injections for macular edema associated with an underlying diagnosis of intermediate uveitis (10%), pseudophakic cystoid macular edema (31%), and posterior uveitis (59%). The time between first and second injection was approximately 5 months [SD ± 72.5; median 144 (min 35, max 427)]. From baseline to follow-up, mean CRT decreased by 103 µm [95% CI: (−122,−83.2), P < 0.001], while IOP increased minimally [mean difference 0.7 mmHg, 95% CI: (−0.02, 1.43), P = 0.057]; and was medically managed when elevated.
Conclusions:
In this real-world cohort, findings suggest that SCTA achieves robust anatomical improvement, a favorable IOP profile, and prolonged durability across patients with inflammation-related macular edema.
Introduction
Corticosteroids are routinely administered for ocular inflammatory disease complicated by macular edema. 1 However, traditional intravitreal and periocular administration routes increase a patient’s risk for cataract formation and ocular hypertension by exposing the anterior segment to high corticosteroid levels.2,3 Fortunately, suprachoroidal triamcinolone acetonide (SCTA) (Xipere) offers an alternative delivery strategy. By injecting triamcinolone into the potential space between the sclera and choroid, SCTA delivers high drug levels in the chorioretina while limiting exposure to the anterior chamber. 4 This targeted approach is hypothesized to reduce the risks of cataract and steroid-induced glaucoma. 5 Difficulty in administering the injection in terms of accessing the suprachoroidal space and patient discomfort do contribute to making SCTA a secondary option, however.
Randomized clinical trials (RCTs) support both the efficacy and safety of SCTA.4,6 Indeed, as the PEACHTREE trial found, SCTA significantly reduced macular edema and improved visual acuity in patients with noninfectious uveitis. 6 It also lowered the incidence of cataract progression or sustained intraocular pressure (IOP) rise. 6 Subsequent preclinical pharmacokinetic studies confirmed SCTA produced higher posterior segment drug levels (∼12-fold increase) and minimized anterior segment exposure (460, 34, 22-fold decrease in lens, iris–ciliary body, and vitreous humor, respectively) when compared to intravitreal or periocular delivery methods. 5 Based on these findings, suprachoroidal triamcinolone acetonide was approved by the Food and Drug Administration (FDA) in October 2021 for suprachoroidal administration in uveitic macular edema.6,7
Despite its growing usage, real-world evidence describing SCTA’s performance remains limited, especially in large-scale, real-world clinical studies. High-volume retina practices, like the Retina Associates of Cleveland, provide fertile ground for valuable clinical data collection. This study is the largest report of SCTA usage and aggregates and analyzes all SCTA cases performed in a high-volume retinal practice in Cleveland, Ohio, over a 4-year period, focusing on durability, efficacy, and safety.
Methods
Data source and cohort eligibility
The described research adhered to the tenets of the Declaration of Helsinki. The Ethics Committee ruled that IRB approval was not required for this study. As this was a retrospective chart review, the requirement for informed consent was waived, but all patient data were handled in compliance with HIPAA regulations to ensure privacy and confidentiality. Data was manually extracted in August 2025 from injection billing records, clinical notes, procedure reports, and imaging records across two Health Information Technology systems, the Physician Office Drug Inventory System (PODIS) (a retina inventory and payment management system) and Nextech [electronic health record (EHR)]. We used string searches in PODIS to identify SCTA patients and matched them to their respective EHR records. Data abstraction followed a standardized protocol and was reviewed for accuracy by practicing ophthalmologists. All patients with noninfectious inflammatory macular edema who received at least one SCTA injection (0.1 mL with a concentration of 40 mg of triamcinolone acetonide per milliliter utilizing a 1100 μm needle tip) between October 25, 2021 (FDA approval date) and July 17, 2025 at Retina Associates of Cleveland, Inc. were included. Patients with infectious or known systemic autoimmune diagnosis were excluded.
Variables and outcomes
All variables and outcomes were measured and documented in the EHR by trained ophthalmological technicians within the practice. We then organized (and analyzed) the data per eye (defined by MRN + laterality with “OU” entries split into OD/OS). Variables included age, sex, number of injections, each injection date, and treatment indication diagnosis. We also recorded central retina thickness (CRT), measured by optical coherence tomography (OCT), and IOP prior to administering the first SCTA injection and again 4–6 weeks later. Additional SCTA doses were administered to patients with persistent or recurrent macular edema at follow-up. Clinical outcomes included average time in days between first and second injection (to explore treatment durability among those with ≥2 SCTA injections) and mean change (first follow-up—baseline) in CRT and IOP. Given previous literature on corticosteroids necessitating surgical management from raised IOP,8–10 we also documented whether any cases with increased IOP required surgical intervention.
Analysis
Descriptive statistics summarized patient demographic and clinical characteristics, including first to second reinjection interval. Paired student t-tests compared pre- and post-treatment OCT and IOP, with mean differences and corresponding 95% CIs reported. Eyes with missing paired OCT or IOP data were not included in their respective t-test calculations. We also categorized IOP change (<5 mmHg, 5–9 mmHg, 10–14 mmHg, ≥15 mmHg rise) to further explore IOP increase trends. A threshold of P < 0.05 defined statistical significance and all analyses were conducted in RStudio v 4.5.1. 11
Results
Patient and eye characteristics
All data were evaluated by our ophthalmology clinicians and epidemiologist co-authors. A total of 177 patients (195 eyes) received 340 SCTA injections during the study period (Table 1). The mean age was 72 years (SD ± 11), 53% were female, and about one-third (36%) underwent ≥2 injections. The underlying diagnosis of the noninfectious inflammatory macular edema was charted by the treating physician as: 20 cases of intermediate uveitis (10%), 60 cases of pseudophakic cystoid macular edema (CME) (31%), and 115 cases of posterior uveitis (59%). No cases of injection-related complications were noted, including inadvertent intraocular injection or infection.
Patient and Eye Characteristics Among Those Receiving at Least 1 SCTA Injection Between October 25, 2021, and July 17, 2025 at Retina Associates of Cleveland, Inc
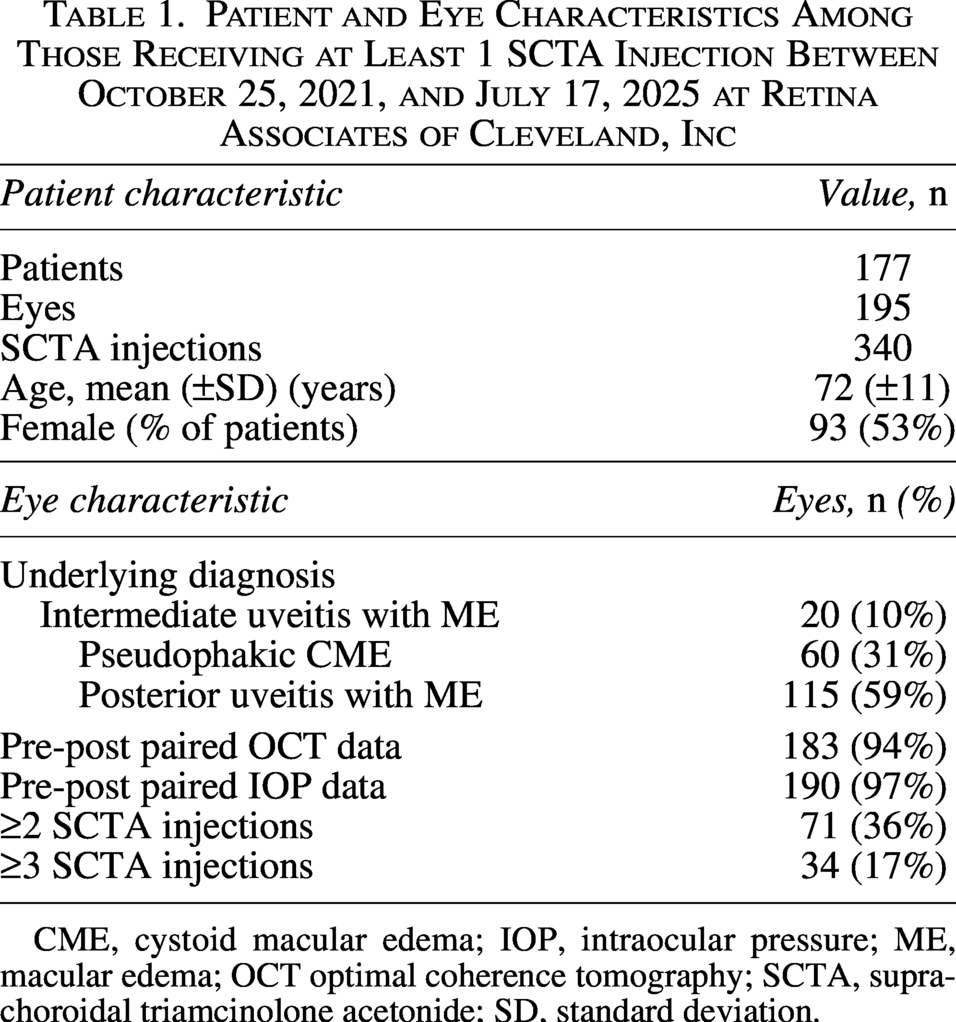
CME, cystoid macular edema; IOP, intraocular pressure; ME, macular edema; OCT optimal coherence tomography; SCTA, suprachoroidal triamcinolone acetonide; SD, standard deviation.
Reinjection interval between 1st and 2nd injections
For eyes treated with at least two injections, the mean time in days between the first and second injections was 156 [SD ± 72.5; median 144 (min 35, max 427)], or approximately 5 months (Fig. 1).
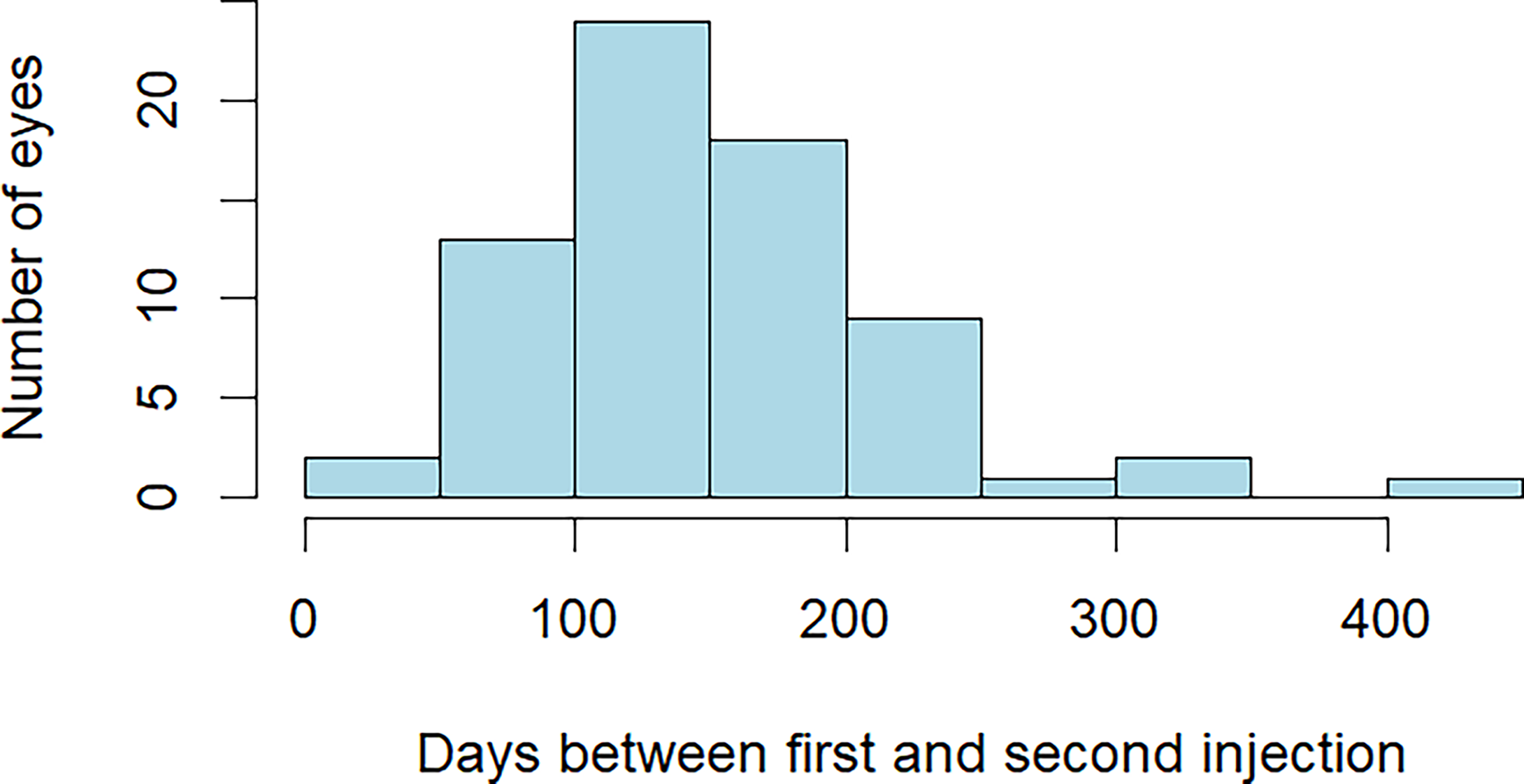
Reinjection interval between 1st and 2nd injections. Histogram of reinjection intervals (per eye) among eyes with ≥2 injections; typical spacing ∼5 months.
Change in CRT and IOP
Among eyes with paired OCT data, average CRT decreased from 440 µm (SD ± 126) at baseline to 337 µm (SD ± 114) post-treatment, representing a mean reduction of 103 µm [95% CI: (−122,−83.2), P < 0.001] (Fig. 2).
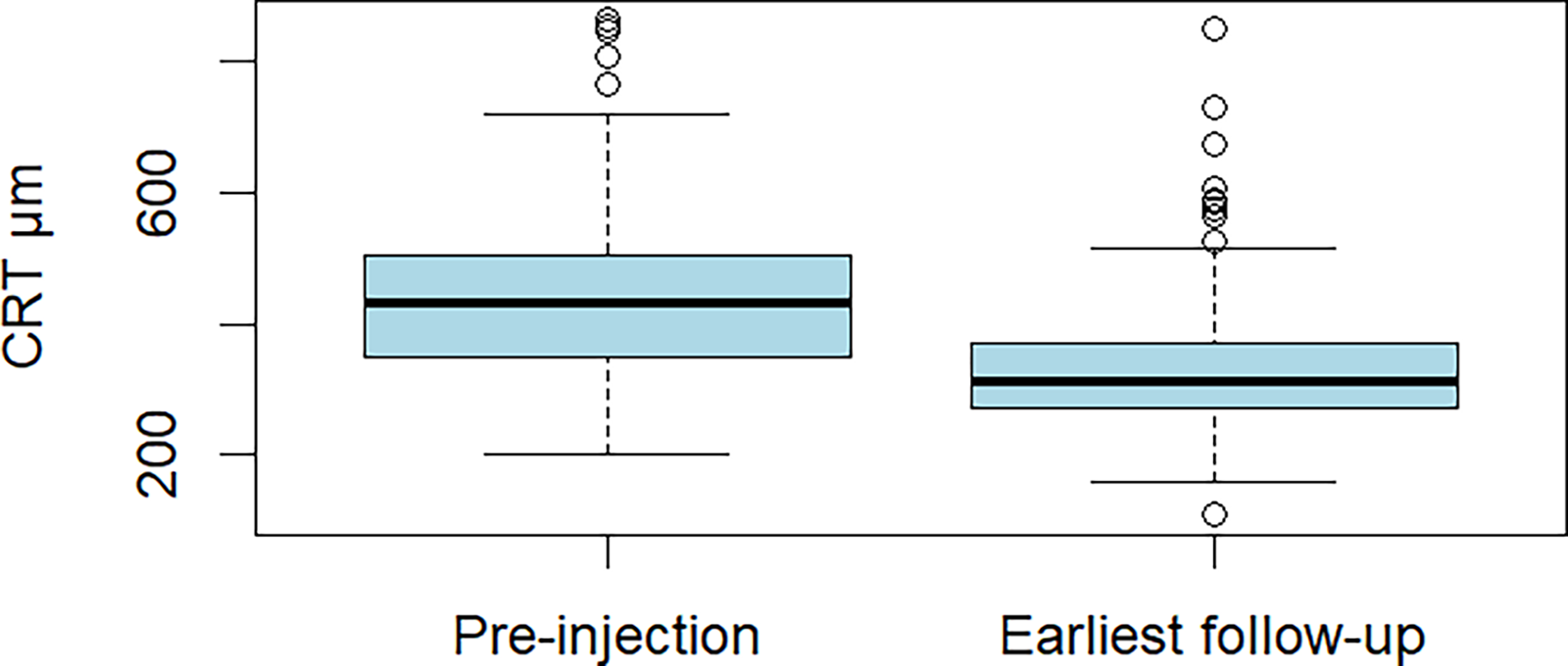
Central retinal thickness at baseline and earliest follow-up. Box-and-whisker plot across unique eyes; paired distribution shows left-shift consistent with edema resolution.
There was a nonsignificant mean increase from 15 mmHg (SD ± 4.6) to 15.7 mmHg (SD ± 4.83) [mean difference 0.7 mmHg, 95% CI: (−0.02, 1.43), P = 0.057] in eyes with paired IOP data. No eyes developed IOP rises ≥ 15 mmHg or required surgical intervention (Fig. 3).
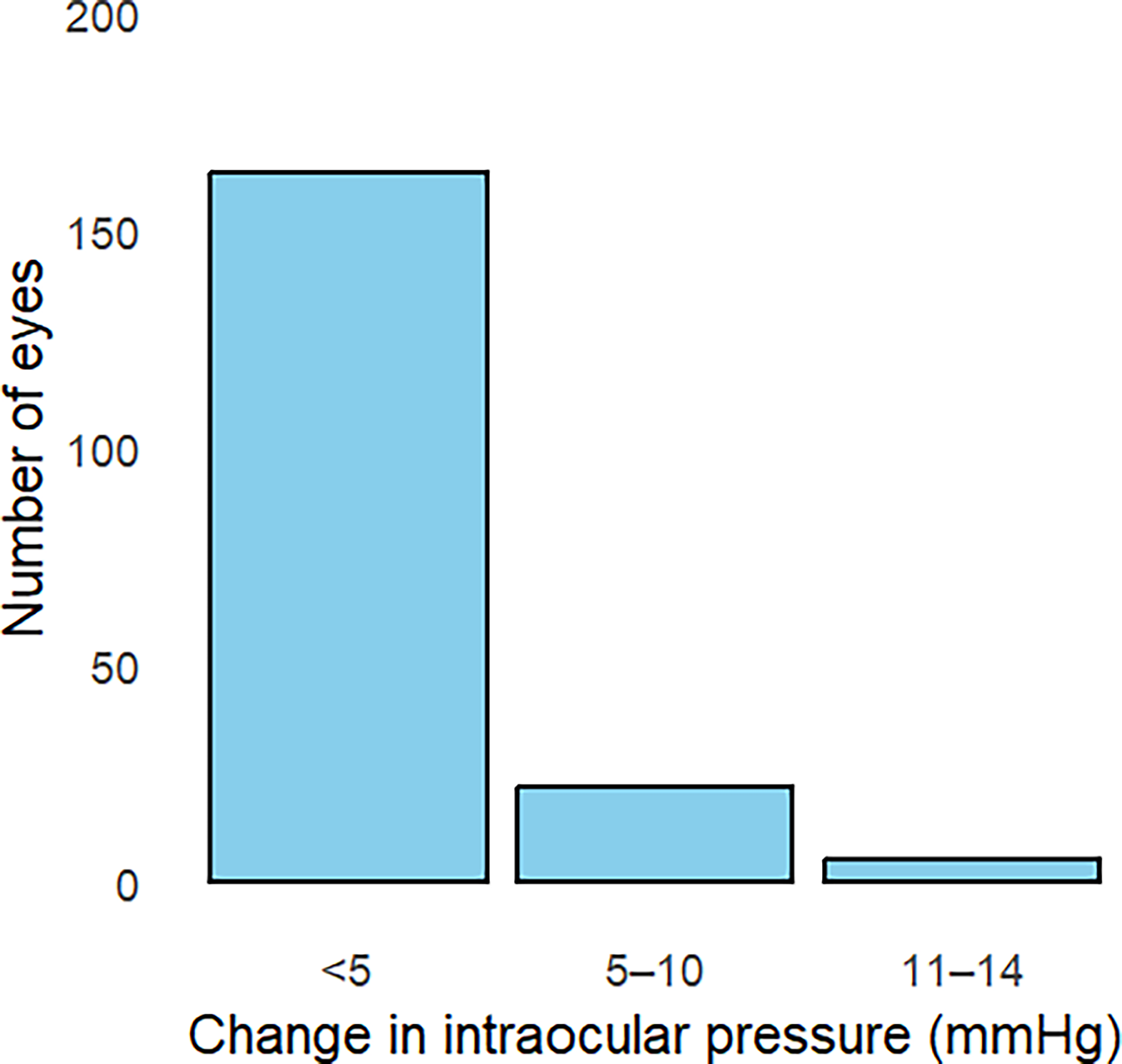
Rise in intraocular pressure after SCTA. Bar chart showing frequencies of <5, 5–9, 10–14, and ≥15 mmHg increases; no eyes required glaucoma surgery.
Discussion
We conducted a real-world study within a high-volume retina practice to describe and evaluate SCTA’s performance. Our findings suggest that SCTA provides robust anatomical efficiency, durability, and a favorable safety profile among those with noninfectious inflammatory macular edema.
By targeting the posterior segment and mitigating anterior segment exposure, suprachoroidal therapy is hypothesized to achieve high local drug concentrations at the site of inflammation and edema while limiting trabecular meshwork exposure, thereby reducing the likelihood of steroid-induced ocular hypertension and cataract formation.12–14 Here, we observed that both the magnitude of macular edema decrease and the modest, but nonsignificant IOP increase parallel findings from previous clinical trials and real-world cohorts.6,14–16 Although all of the patients in this study were categorized as having uveitic macular edema, the treating physician’s distinction between intermediate, posterior, or postsurgical CME can be nuanced, and could not be reliably parsed in this review. Therefore, among the limitations of this paper is the broad label of non-infectious inflammatory macular edema, but this is a practical approach in the real-world clinic. In addition, no known autoimmune or infectious cases were included. Another weakness to this review is the lack of lens status or cataract progression, which was not collected. Given the brevity of the follow-up in the article, we would not have seen adequate passage of time to fairly assess for cataract progression, but a longer follow-up is warranted and could help investigate such concerns as steroids are a known contributor to worsening cataract. Collectively, the results reinforce the concept that compartmentalized delivery through the suprachoroidal space optimizes treatment efficacy for macular edema while reducing side effect risks of elevated IOP.
Unlike the PEACHTREE Trial protocol, in which all participants received a second injection at 12 weeks, 6 real-world administration of a second SCTA injection is generally made at the physician’s discretion and is guided by the ongoing presence of macular edema. Indeed, as our findings showed, only 36% of patients required a second dose. Among those who received multiple injections, the average reinjection interval was nearly twice that of the 12-week protocol. These results align with a recent real-world physician survey, which found that only 17% of patients required an additional injection within 3–6 months. 17 Consequently, the 5-month reinjection interval, longer than the typical 2–4 months dosing cycles of intravitreal triamcinolone or dexamethasone implants,18,19 may help reduce treatment burden and improve adherence, particularly in chronic inflammatory or edematous diseases. Additionally, a greater understanding of the breakdown of specific subsets of non-infectious uveitic macular edema such as pseudophakic macular edema could better inform the efficacy of SCTA for specific disease pathologies.
Strengths and Limitations
Our study leveraged data from a high-volume retina practice, providing a comparatively large cohort of patients treated with SCTA, and allowed for the evaluation of real-world treatment patterns and outcomes. This enhances the generalizability of findings to routine clinical practice, where patient profiles and treatment decisions are more heterogenic than clinical trials.
Despite our study’s strengths, we acknowledge its limitations. First, although our findings provide valuable real-world insights, the analyses were unadjusted and did not account for potential confounding factors such as prior steroid or anti-VEGF therapy. This is particularly relevant as prior steroid and anti-VEGF therapy likely biased our estimates toward the null, understating both anatomical response and durability while potentially exaggerating mean IOP increase in patients with cumulative steroid exposure.20–22 Second, because of the limited number of patients who received >2 injections, only the interval between first and second SCTA doses were evaluated. While subsequent injections were not assessed, few patients required rescue or emergency therapy after a second injection in clinical trials.6,23 Thus, understanding the durability between first and second injections, as well as the clinical predictors for reinjection, may offer more practical relevance for real-world decision-making. Although all IOP measurements were obtained between 8
In this large cohort, SCTA demonstrated meaningful anatomical efficacy, a favorable safety profile, and extended durability. These findings reinforce its role as a valuable therapeutic option in retinal practice and expanded the evidence base supporting its use beyond a controlled clinical trial setting. Further studies that account for potential confounding factors and include larger, more diverse populations are warranted to evaluate SCTA’s effectiveness across macular edema etiologies (such as pseudophakic macular edema), assess its safety in patients with glaucoma given its limited impact on IOP, and to identify clinical predictors of reinjection need. Further review is also needed regarding the ease of administration and patient discomfort as a factor in the decision-making among the choices to deliver ocular steroids.
Authors’ Contributions
Research design: C.W.M., C.A.S., M.L.J., H.D.S., D.G.M., and J.M.C. Data acquisition and/or research execution: C.W.M., C.A.S., M.J.H., J.A.U., C.D.G., and J.S.Z. Data analysis and/or interpretation: C.W.M., S.L.W., D.G.M., and J.M.C. Article preparation: All authors. Supervision: D.G.M. and J.M.C.
Ethical Considerations
The Ethics Committee ruled that IRB approval was not required for this study as it utilized fully de-identified data and does not meet the definition of human subjects research under the U.S. Department of Health and Human Services regulations (45 CFR 46.102). According to institutional policy, research activities that involve only the analysis of existing, de-identified data do not require Institutional Review Board (IRB) approval or exemption review. Therefore, formal IRB approval was not required for this study.
Footnotes
Acknowledgment
The authors would like to acknowledge all the ophthalmic technicians and staff at the Retina Associates of Cleveland, Inc.
Author Disclosure Statement
D.G.M. reports consulting fees, speaking honoraria, and travel support from Regeneron, Apellis, and Astellas. He also reports minor food and beverage payments from several ophthalmical companies. No other conflicts of interest. H.D.S. reports honoraria from Alimera Sciences and minor food and beverage payments from several ophthalmical companies. No other conflicts of interest. J.M.C. reports grants, consulting fees, honoraria, and travel support from multiple ophthalmical industry companies, including Alimera, Genentech/Roche, Regeneron, Apellis, Astellas, Ocular Therapeutix, and AbbVie. He also reports minor food and beverage payments from other industry sources. No other conflicts of interest. M.L.J. reports minor food and beverage payments from Dutch Ophthalmical and Regeneron. No other conflicts of interest. C.W.M., C.A.S., S.L.W., M.J.H., J.A.U., C.D.G., and J.S.Z. report no conflicts of interest.
Funding Information
The author(s) received no financial support for the research, authorship, and/or publication of this article.