
Abstract
Purpose:
Demodex blepharitis is caused by Demodex mite infestation of the eyelash follicles and associated sebaceous glands (the glands of Zeis) and is often associated with tear film instability and dry eye disease (DED). Information on the role of Zeis glands is limited. This study used surrogate Zeis gland secretions in healthy volunteers to evaluate whether Zeis gland secretions could potentially contribute to the tear film lipid layer.
Methods:
The blinking status of each eye (partial or complete blinker) was assessed with interferometry. A surrogate Zeis gland secretion was applied with a moistened ophthalmic fluorescein strip across the center of the lower eyelid near the eyelash base. The presence of fluorescent dye in the tear film was evaluated at 2 and 5 min using a fluorescein angiography image acquisition system.
Results:
Forty eyes (20 subjects) were enrolled; 31 (77.5%) partial blinkers, 4 (10.0%) complete blinkers, and 5 (12.5%) nonblinkers that did not blink during the interferometry assessment. Fluorescent dye was detected in the tear film of 18 (45.0%) eyes at 2 min and 24 (60.0%) eyes at 5 min, with similar proportions of partial blinker, complete blinker, and nonblinker eyes demonstrating a fluorescent signal.
Conclusion:
A surrogate Zeis gland secretion accessed the tear film in most eyes, suggesting that Zeis gland secretions may contribute to the tear film. In Demodex blepharitis, abnormal or reduced lipid production from the Zeis and/or meibomian glands may contribute to DED. Further research is needed to clarify the underlying mechanisms of DED in patients with Demodex blepharitis.
Introduction
The eyelid margin contains three distinct types of glandular structures: the meibomian glands, glands of Zeis, and glands of Moll. 1 Meibomian glands are elongated, modified sebaceous glands that form the structural basis of the tarsal plates of the eyelid. 1 These glands secrete a lipid-rich substance called meibum, the main source of the lipids that form the tear film lipid layer, 2 which is essential for tear film stability and the prevention of evaporative dry eye disease (DED). 3 The functions of the Zeis glands and glands of Moll are less understood, but they may also contribute to the integrity of the tear film, albeit to a lesser extent than the meibomian glands. 4
The Zeis glands are sebaceous glands located at the base of the eyelashes within the eyelid margin that open into the eyelash follicles in close proximity to the glands of Moll and the meibomian glands (Fig. 1). 5 We have observed that Zeis glands can be expressed by applying light pressure to the eyelid margin (Fig. 2). Oily secretions from sebaceous glands (sebum) are believed to help maintain a healthy skin barrier, promote skin hydration, and deliver antioxidants and antimicrobial lipids. 6 Therefore, Zeis gland secretions likely help lubricate the eyelash follicles and eyelashes while protecting against irritation and microbial invasion. The glands of Moll (also known as ciliary glands) are apocrine sweat glands located on the eyelid at the base of each eyelash. It is unclear if the glands of Moll open into the cilia of the eyelash or open directly onto the lid margin. 7 Moll gland secretions include antimicrobial peptides and have been postulated to play a role in self-protection and immune defense, maintaining ocular surface homeostasis, and maintaining the integrity of the tear film. 7
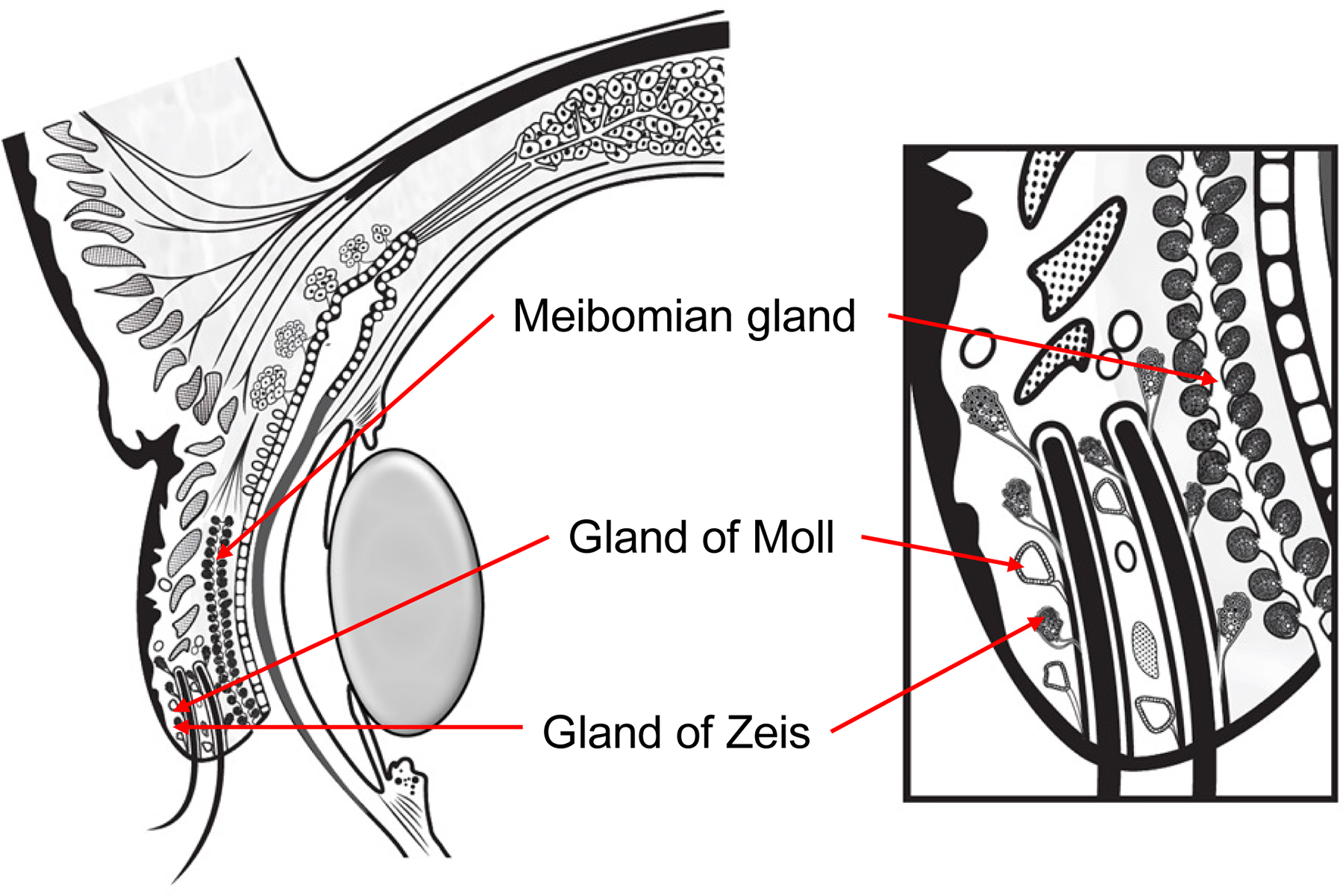
Schematic of glands in the eyelid margin.
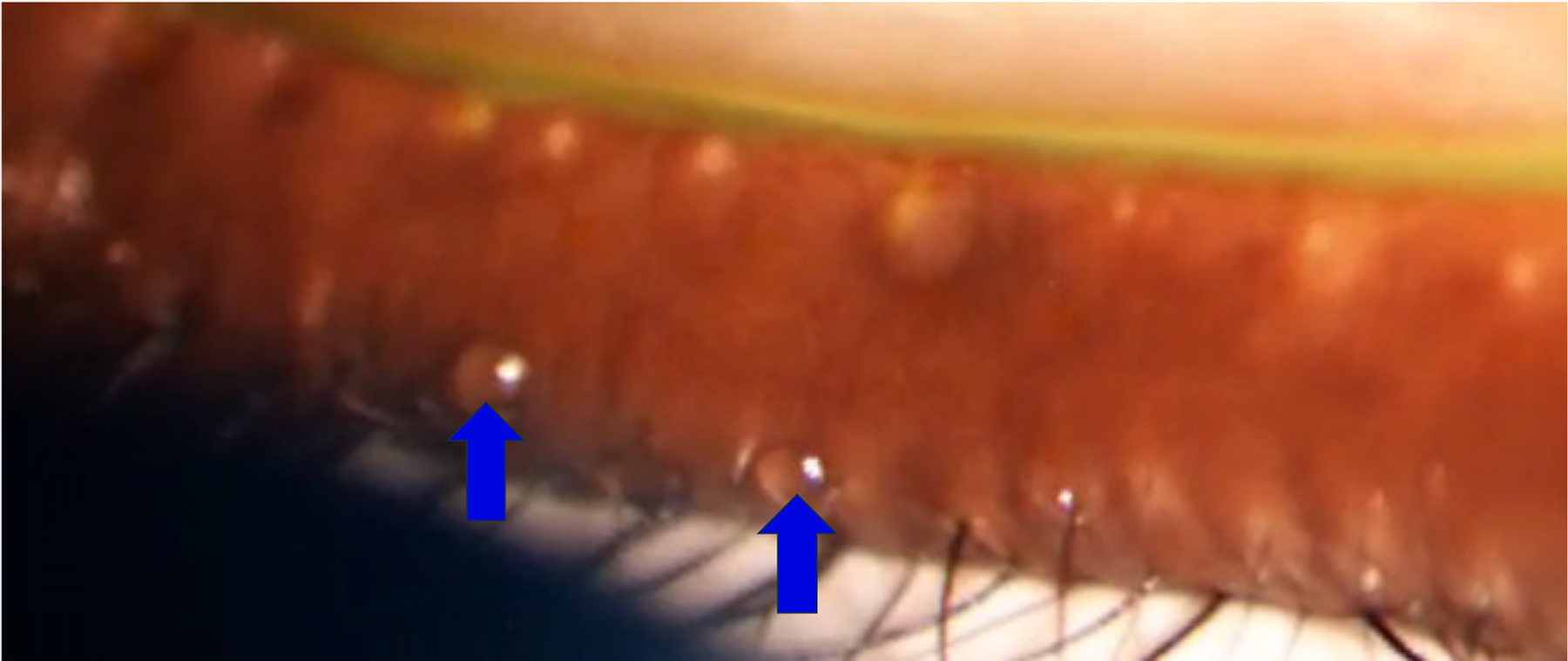
Zeis gland secretions (blue arrows). A Meibomian Gland Evaluator was used to apply uniform pressure and express glands on the lower eyelid.
Demodex blepharitis is caused by Demodex mite infestation of the eyelash follicles and associated sebaceous glands (i.e., the Zeis glands), leading to chronic inflammation of the eyelid margin. Collarettes (waxy, cylindrical, tube-shaped deposits of mite debris that form at the base of the eyelashes) are the hallmark sign of the disease. 8 Demodex blepharitis is commonly associated with ocular symptoms including itching, dryness, discharge, redness, burning, foreign body sensation, pain, and blurry vision, 8 and it is frequently accompanied by DED. In a large retrospective study of patients seen at U.S. eye care clinics, 59.7% of patients with Demodex blepharitis also presented with DED, and 58.9% of patients with DED also presented with Demodex blepharitis. 9
The mechanism linking Demodex mite infestation to dry eye is not fully understood. Although the glands of Zeis are further from the tear meniscus than the meibomian glands, it is possible that Zeis gland secretions contribute to the tear film and are involved in the maintenance of tear film homeostasis. Thus, in Demodex blepharitis, inflammation secondary to the mite infestation could interfere with secretions from the Zeis glands as well as the meibomian glands, resulting in changes in the tear film lipid layer that contribute to tear film instability and DED. 8 This study using a surrogate for Zeis gland secretions was conducted to further our understanding of the underlying mechanism of DED in Demodex blepharitis by determining whether lipid secretions from the Zeis glands could potentially contribute to the tear film lipid layer.
Methods
Ethical conduct
The study adhered to the tenets of the Declaration of Helsinki, and the Advarra institutional review board approved the study protocol at the study site (approval number MOD02455600). All participants provided written informed consent.
Study design
The study was conducted at the
Subjects were enrolled at the screening visit (day 1). Following enrollment, blink dynamics in both eyes were evaluated with the LipiView II Ocular Surface Interferometer (Johnson & Johnson Vision, Irvine, CA). This device measures the completeness of each blink that occurs during the assessment. Based on the findings, each eye was categorized as a complete blinker (no partial blinks) or a partial blinker (any partial blinks) during the assessment.
Transfer of a surrogate Zeis gland secretion (a fluorescent dye placed near the base of eyelashes on the lower eyelid margin) to the tear film was evaluated at a second study visit, which could be combined with the screening visit. With the subject seated at a slit lamp, a BioGlo ophthalmic fluorescein strip (HUB Pharmaceuticals, Scottsdale, AZ) was moistened with an ophthalmic balanced salt solution (BSS) and lightly spread across ∼1 cm of the central lower eyelid margin, near the eyelash base, of the right eye. The subject was asked to blink normally following the fluorescein dye placement.
Fluorescent signal was imaged using the Optos Silverstone system (Dunfermline, UK) in fluorescein angiography image acquisition mode, with the participant’s eye positioned 1–2 inches away from the camera for anterior segment fluorescein imaging. Images were taken at baseline (before placement of the surrogate Zeis secretion on the eyelid) and at 2 min (±60 s) and 5 min (±90 s) after the dye placement. If fluorescein was not visualized in the tear film by the 5-min time point after normal blinking, the subject was asked to perform a hard eyelid squeeze/blink, and additional images were taken after the hard blink.
Following imaging, the eye was rinsed with ophthalmic BSS, and the fluorescent dye application and imaging procedures were repeated on the left eye. For each eye, if the procedures were unsuccessful because of difficulty with dye placement, they could be repeated after 30 min or at an additional study visit.
Images obtained after normal blinking and hard blinks were assessed for the presence of fluorescent signal in the tear film. The main outcome measures were the proportion of eyes with fluorescence signal in the tear film, the proportion of blinks in each eye that were partial blinks, and the proportion of partial-blinker eyes and complete-blinker eyes with fluorescent signal in the tear film.
The analysis used descriptive statistics and was based on observed values. The sample size was not based on a power analysis for hypothesis testing. If a fluorescence rate of 80% were observed in 20 subjects (40 eyes), the 95% confidence interval of the fluorescence rate would have a half-width of 13.3%.
Results
Twenty individuals were screened and enrolled. The mean age of the study participants was 46.0 years (range, 24–63). Most of the subjects were White (50%) or Asian (40%); 11 subjects (55%) were female and 9 (45%) were male. All 20 subjects completed the study. No adverse events were reported during the study, and no safety concerns were noted.
Blink dynamics in each study eye (n = 40) were evaluated with interferometry at screening. The mean number of blinks during the evaluation was 6.6, the mean number of partial blinks during the evaluation was 3.0, and, on average, 44% of blinks in each eye were partial blinks (Table 1). Most eyes (77.5%) had at least one partial blink during the evaluation and were categorized as partial blinkers. All blinks were complete in 4 (10%) eyes, which were categorized as complete blinkers. Five (12.5%) eyes did not blink during the evaluation and were categorized as nonblinkers.
Blink Dynamics and Blinker Status
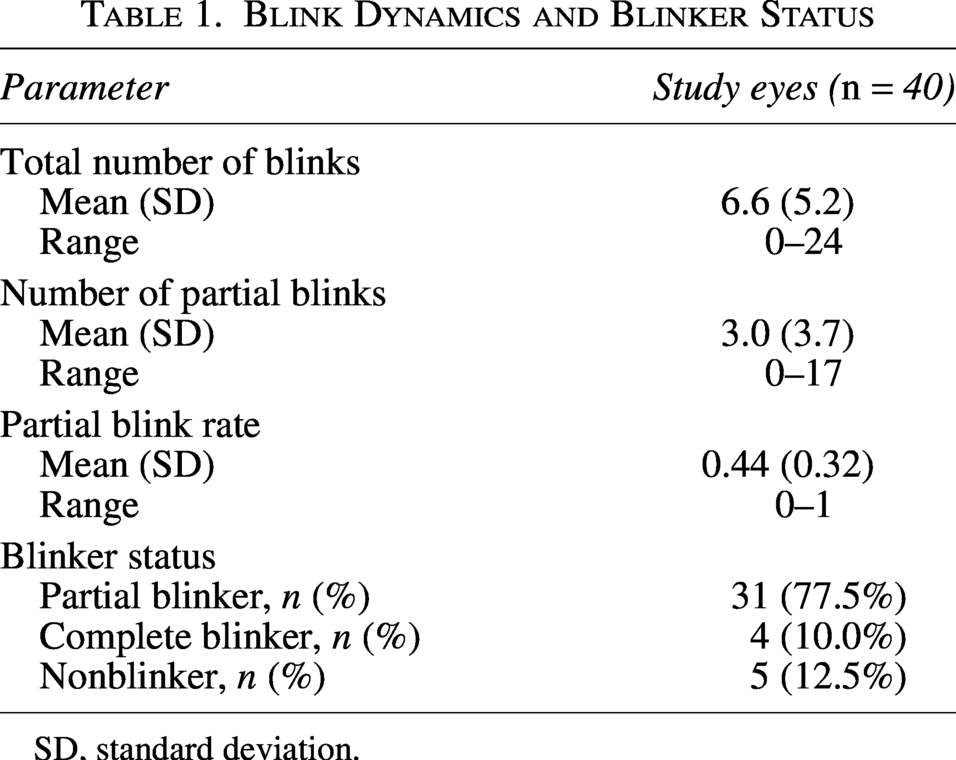
SD, standard deviation.
After placement of the fluorescein-containing surrogate Zeis gland secretion on the lower eyelid margin, fluorescent signal was detected in the tear film of 45% (18/40) of eyes after 2 min and 60% (24/40) of eyes after 5 min of normal blinking. Figure 3 shows a representative eye with fluorescein dye applied at the eyelash base, the site of Zeis gland secretion, and serving as a surrogate marker for Zeis gland secretions. A fluorescent signal is visible in the tear film. At both 2 and 5 min, the proportion of eyes with fluorescent signal in the tear film was comparable among the subgroups of eyes by blinker status (partial blinkers, complete blinkers, and non-blinkers) (Table 2).
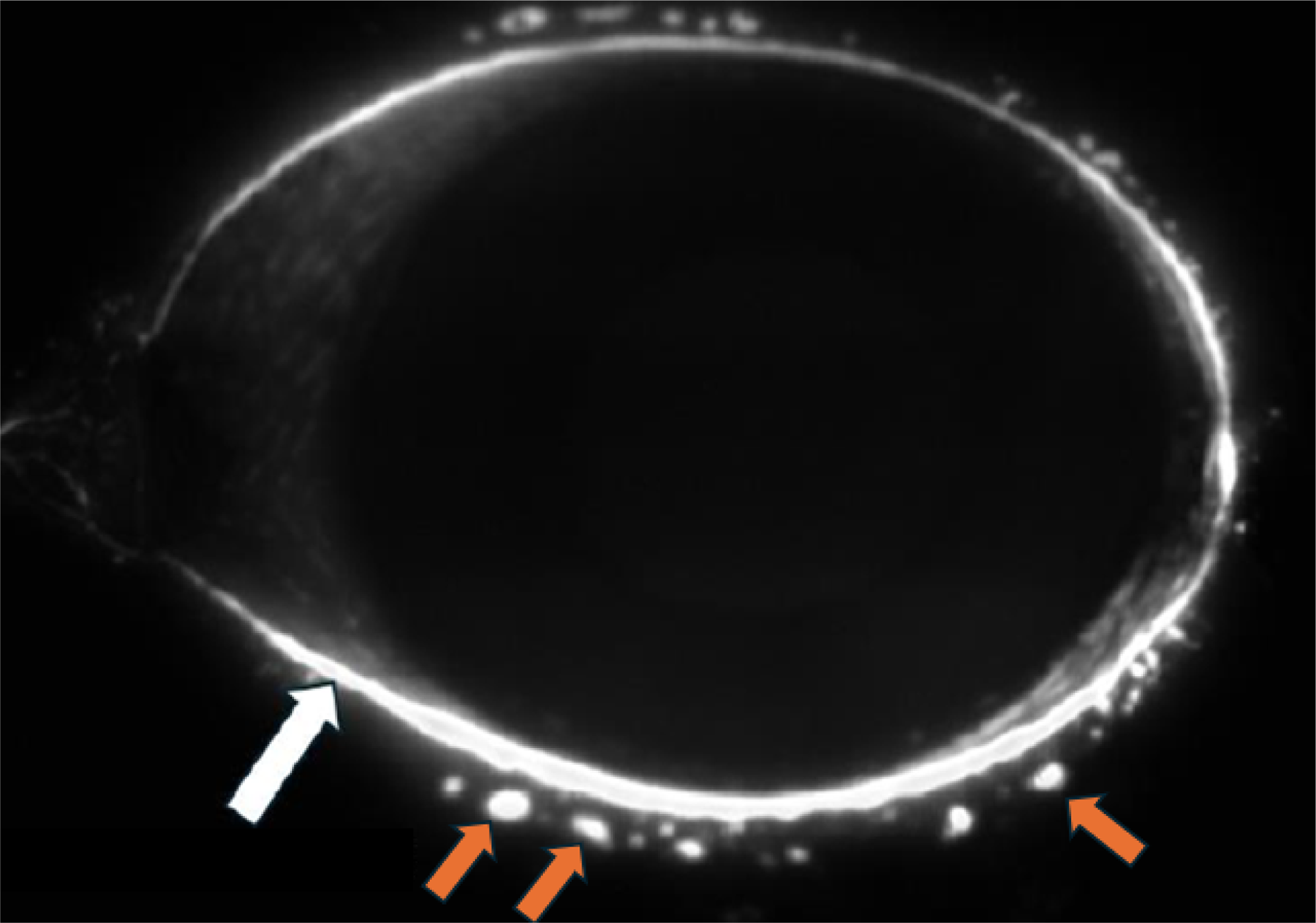
Fluorescence image of an eye after placement of fluorescein dye at the base of the eyelashes where the Zeis glands secrete (orange arrows). The fluorescein is acting as a surrogate for Zeis gland secretions. Fluorescent signal is present in the tear film and tear meniscus (white arrow). Punctate signal on the upper lid results from touch to the lower lid during blinking.
Fluorescent Dye Transfer to the Tear Film at 2 and 5 Minutes
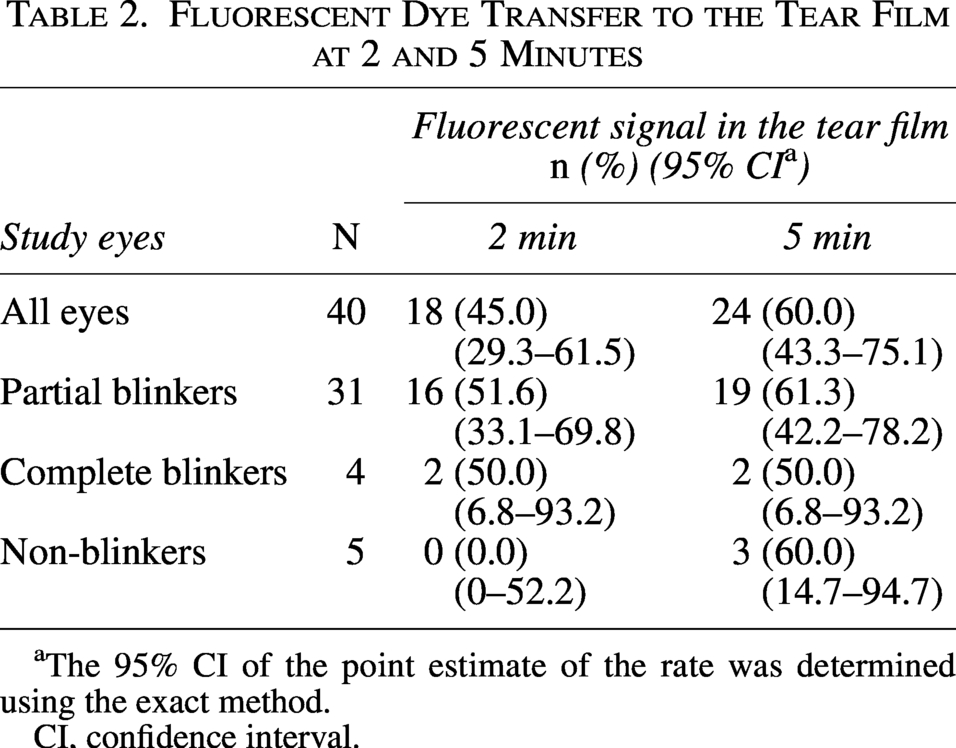
The 95% CI of the point estimate of the rate was determined using the exact method.
CI, confidence interval.
Of the 16 eyes with no detectable fluorescent signal in the tear film at 5 min, 9 demonstrated fluorescence in the tear film after a hard blink/squeeze. Overall, some portion of the surrogate Zeis secretion transferred to the tear film during normal blinking or after a hard blink in 82.5% of the study eyes (33/40). Among the 5 nonblinker eyes (those that did not blink during the interferometer assessment at screening), none were observed to have fluorescent signal in the tear film at 2 min, but 3 had fluorescent signal in the tear film at 5 min, and the remaining 2 eyes had fluorescent signal in the tear film after a hard blink.
Discussion
In this study using a fluorescent surrogate Zeis gland secretion in healthy eyes, 60% of eyes had fluorescent dye in the tear film after 5 min of normal blinking. The proportion of eyes with a fluorescent signal in the tear film was similar among the subgroups of eyes by blinker status (partial blinkers, complete blinkers, and nonblinkers). These results suggest that Zeis gland secretions may contribute to the tear film and that Zeis glands could potentially be involved in DED associated with eyelid pathologies.
Zeis glands are often regarded as rudimentary appendages of the eyelid margin without a significant function. Physiological Zeis gland expression of sebum is likely to involve compression of the glands via muscle activity at the lid margin during blinking. Histologically, Zeis glands are identical to meibomian glands. The meibomian glands are specialized sebaceous glands that secrete meibum, which is biochemically distinct from the sebum found in the skin in other areas of the body. The role of meibomian glands in tear film function is well established, as the tear film lipid layer is primarily composed of meibum, and meibomian gland dysfunction (MGD), the leading cause of evaporative DED, is characterized by changes in the quantity and quality of the meibum produced by the meibomian glands.
In an observational study that we conducted to investigate signs and symptoms associated with the presence and severity of MGD, the meibomian glands in the central lower eyelid of the study eye in the non-MGD, mild/moderate MGD, and severe MGD cohorts were expressed manually at the slit lamp by applying a Meibomian Gland Evaluator (Johnson & Johnson Vision) to the eyelash base, and the investigator graded the quality of the meibomian gland secretions from the 6 central meibomian glands in the lower eyelid. 10 Video recordings of the lower lid compression and glandular secretions were made with a video camera mounted on the slit lamp. 11 Although only the evaluation of meibomian glands and meibum was preplanned in the study, when reviewing the meibography video recordings, we observed that application of the Meibomian Gland Evaluator also resulted in oily secretions emanating from Zeis glands. Although the glands of Moll are in close proximity to the Zeis glands, we attributed the expressed secretions near the base of eyelashes to Zeis glands because manual expressibility is more consistently associated with sebaceous glands than apocrine sweat glands.
The video recordings were used to assess the number of expressible Zeis glands and the quality of the Zeis gland secretions in the central lower eyelid. Lower lid compression resulted in Zeis gland secretions in 67.2% of the gradable study eyes [79.2% (19/24) in the non-MGD cohort, 40.9% (9/22) in the mild/moderate MGD cohort, and 81.0% (17/21) in the severe MGD cohort]. 12 Importantly, in all cohorts, all secretions from Zeis glands were graded as grade 0 (clear with normal viscosity) at each study visit (Fig. 4). In marked contrast, the quality of meibomian gland secretions decreased with increased severity of MGD.10,11 These observations indicate that Zeis glands continue to function normally in the presence of MGD.
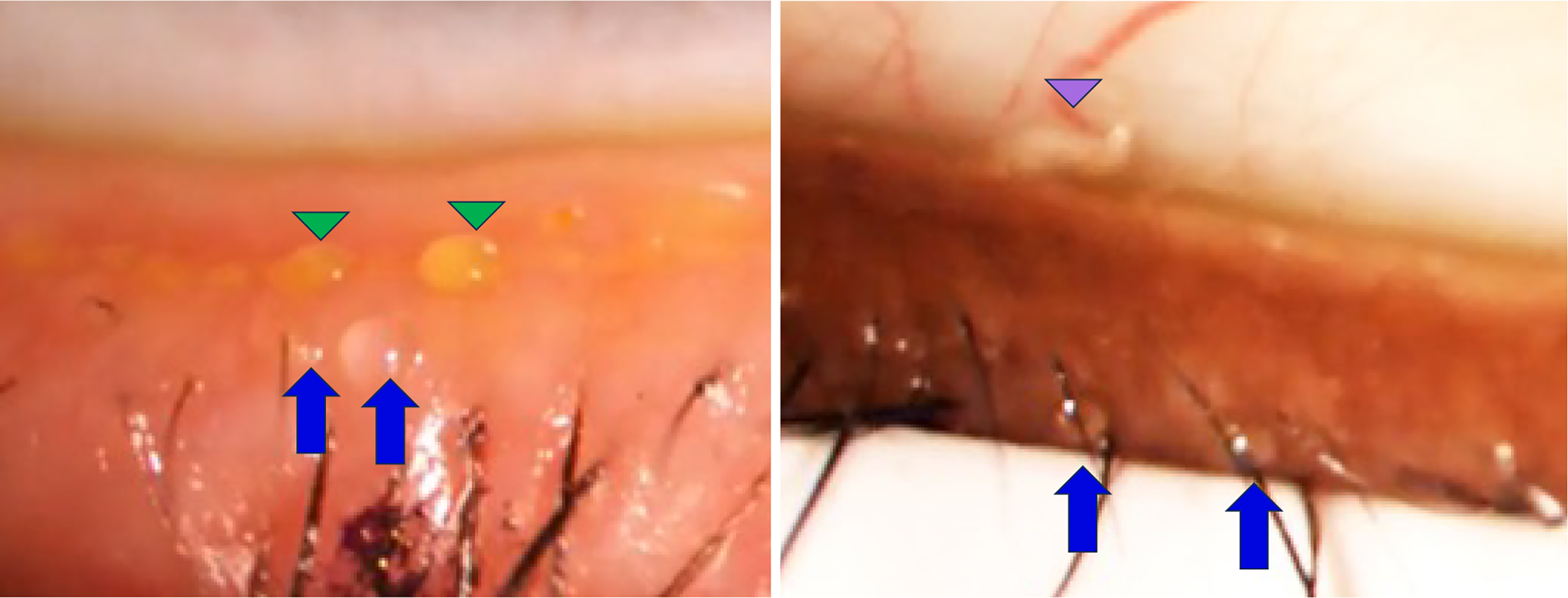
Zeis gland and meibomian gland secretion quality in two patients with MGD-related DED. A Meibomian gland evaluator was used to apply uniform pressure and express glands on the lower eyelid. The quality of the Zeis and meibomian gland secretions was graded with Mather’s scale. Left panel: Blue arrows: grade 0 (normal) Zeis gland secretion; green arrowheads: grade 1 meibomian gland secretion. Right panel: Blue arrows: grade 0 (normal) Zeis gland secretion; purple arrowhead: grade 3 meibomian gland secretion. DED, dry eye disease; MGD, meibomian gland dysfunction.
Both Zeis glands and meibomian glands express urea transporter B, which promotes the influx of urea into the tear film. 13 Urea homeostasis within the tear fluid is believed to be essential for tear film stability because urea affects the surface tension of the tear film and may serve as a natural moisturizer and humectant for the ocular surface. 13 The concentration of urea in tears has been shown to be significantly reduced in patients with DED compared with normal controls. 14 This finding supports a potential role of Zeis glands with respect to promoting tear film stability and suggests that Zeis glands could be a therapeutic target in the treatment of DED, particularly where there is involvement of the eyelash follicle such as in Demodex blepharitis.
This was an exploratory study, and the sample sizes for eyes that were complete blinkers and non-blinkers were too small to allow statistical comparison with the results in eyes that were partial blinkers. Another study limitation was that differences in chemical composition between the surrogate secretion used and actual lipid-rich Zeis gland secretions could have affected the likelihood of transfer to the tear film. Fluorescein is a hydrophilic molecule, whereas Zeis gland secretions are lipid-rich and hydrophobic in nature. Therefore, it is uncertain whether the transfer behavior of fluorescein accurately reflects the physiological transfer dynamics of native Zeis gland lipids to the tear film. Finally, no fluorescent dye was detected in the tear film in 17.5% of eyes, even after a hard blink, for reasons that remain unexplained.
Conclusions
These study results suggest that oil secretions at the lash base from Zeis glands have the potential to contribute to the lipid layer of the tear film. This may help explain why interferometry assessments have not reliably shown a decrease in tear film lipid layer thickness in patients with severe MGD. 15 Because Demodex blepharitis affects the Zeis glands and also the meibomian glands in some patients, abnormal or reduced lipid production from these glands may contribute to DED in affected patients. Our study participants had no clinically significant DED. Moreover, it remains unknown how well the transfer of the surrogate Zeis gland secretion reflects the physiological transfer of native Zeis gland lipid secretions to the tear film. Further studies are needed to elucidate the potential contribution of Zeis gland secretions to the tear film and the potential role of these secretions in DED associated with eyelid margin disorders such as Demodex blepharitis and MGD. We recommend that one such future study exploring the transfer of Zeis gland secretions to the tear film use a lipophilic dye, which may replicate the localized physiological environment more closely, as a surrogate Zeis gland secretion.
Authors’ Contributions
A.N.: Study design, data collection, data analysis, data interpretation, and critical review, revisions, and approval of the article. M.M.S.: Study design, data collection, data interpretation, and critical review, revisions, and approval of the article. J.P.: Data collection, data interpretation, and critical review, revisions, and approval of the article. L.N.: Data collection, data interpretation, and critical review, revisions, and approval of the article. P.L.: Data analysis, data interpretation, and critical review, revisions, and approval of the article. M.R.R.: Study design, data analysis, data interpretation, and critical review, revisions, and approval of the article.
Data Sharing Statement
AbbVie is committed to responsible data sharing regarding the clinical studies we sponsor. This includes access to anonymized, individual, and study-level data (analysis data sets), as well as other information (e.g., protocols, clinical study reports, or analysis plans), as long as the studies are not part of an ongoing or planned regulatory submission. This includes requests for clinical study data for unlicensed products and indications. These clinical study data can be requested by any qualified researchers who engage in rigorous, independent, scientific research, and will be provided following review and approval of a research proposal, Statistical Analysis Plan, and execution of a Data Sharing Agreement. Data requests can be submitted at any time after approval in the US and Europe and after acceptance of this article for publication. The data will be accessible for 12 months, with possible extensions considered. For more information on the process or to submit a request, visit the following link: https://www.abbvieclinicaltrials.com/hcp/data-sharing/.
Footnotes
Acknowledgment
Medical writing assistance was provided to the authors by Evidence Scientific Solutions, Inc. (Raleigh, NC) and funded by AbbVie. All authors had access to relevant data and participated in the drafting, review, and approval of this publication.
Author Disclosure Statement
All authors are employees of AbbVie and may hold AbbVie stock.