
Abstract
Purpose:
To evaluate whether bioimpedance-derived body composition parameters are associated with adalimumab exposure and immunogenicity in noninfectious uveitis (NIU) and whether they provide information complementary to body mass index (BMI).
Methods:
Forty-five patients with NIU receiving adalimumab monotherapy (40 mg every 2 weeks) for at least 12 months were enrolled in this single-center cross-sectional study. Body composition was assessed by use of multifrequency bioimpedance analysis (InBody 770). Serum adalimumab trough concentrations and anti-adalimumab antibodies (AAA) were measured. Associations were evaluated using Pearson correlations, multivariable linear regression, and receiver operating characteristic (ROC) analyses.
Results:
Adalimumab trough concentrations were moderately inversely correlated with BMI (r = −0.51, P = 0.0004), body fat mass (r = −0.51, P = 0.0004), percent body fat (r = −0.48, P = 0.001), and visceral fat area (r = −0.53, P = 0.0002), but not with lean-mass parameters. In separate multivariable models adjusted for age and sex, each adiposity measure was independently associated with trough concentrations (adjusted R2 0.18–0.25). ROC analysis showed comparable discrimination of low drug exposure for BMI (area under the curve [AUC] 0.69) and body composition metrics (AUC 0.70–0.74; DeLong P > 0.5). BMI showed the strongest correlation with AAA levels (r = 0.58, P < 0.0001).
Conclusions:
Bioimpedance-derived adiposity measures and BMI showed similar associations with adalimumab exposure in NIU. Body composition may offer complementary biological context for interpreting pharmacokinetic variability and immunogenicity. Future studies are warranted to determine whether body composition data improve therapeutic drug monitoring in uveitis.
Introduction
Adalimumab, a fully human monoclonal antibody targeting tumor necrosis factor-alpha (TNF-α), is the first biological agent approved for the treatment of noninfectious uveitis (NIU) and is the current standard of care for sight-threatening intermediate, posterior, and panuveitis.1,2 In the setting of standardized fixed-dose administration, interindividual variability in drug exposure remains substantial, and approximately 20%–40% of patients develop antidrug antibodies depending on disease context and concomitant immunosuppression.3,4 Antidrug antibody formation leads to reduced circulating drug concentrations, loss of clinical response, and treatment discontinuation. Given the potentially sight-threatening nature of uveitis and the limited number of approved biological alternatives, identifying patient-specific factors that contribute to pharmacokinetic variability is therefore central to optimizing treatment.
Therapeutic drug monitoring (TDM) 5 offers a practical approach to individualized management of anti-TNF agents, integrating drug concentrations and antidrug antibodies into clinical decision-making. We have previously demonstrated that TDM-guided treatment adjustments can improve outcomes in NIU, 3 and that higher body mass index (BMI) is associated with lower adalimumab serum concentrations and greater disease activity in both adult and pediatric uveitis.6,7 However, BMI does not directly reflect body composition and may inadequately represent the pharmacologically relevant tissue compartments that influence monoclonal antibody distribution. 8
Unlike small-molecule drugs, monoclonal antibodies primarily distribute within vascular and interstitial spaces, with their volume of distribution influenced by both lean tissue and adipose tissue compartments.9,10 Increased adiposity is associated with an expansion of the apparent volume of distribution, potentially leading to lower circulating drug concentrations at standard doses. 11 Moreover, obesity-related low-grade systemic inflammation may increase immunoglobulin clearance through Fc receptor-mediated pathways, altered neonatal Fc receptor (FcRn) recycling, and reticuloendothelial catabolism.12,13 Adipose tissue is also an immunologically active organ, secreting pro-inflammatory cytokines and adipokines that may promote antidrug antibody formation.14,15
Emerging evidence from rheumatology and gastroenterology suggests that adiposity affects monoclonal antibody pharmacokinetics through these mechanisms,16,17 yet data in uveitis remain scarce. NIU treated with fixed-dose adalimumab monotherapy provides a controlled clinical model for investigating these relationships, minimizing confounding from combination immunosuppression and dose escalation. Herein, we evaluated whether bioimpedance-derived body composition parameters are associated with adalimumab exposure and immunogenicity and whether they provide information complementary to BMI in patients with NIU.
Methods
This single-center cross-sectional study was conducted at the Eye Institute of Cleveland Clinic Abu Dhabi. Consecutive patients with NIU receiving adalimumab (Humira, AbbVie, Inc., North Chicago, IL, USA) monotherapy for at least 1 year were enrolled between January 2023 and October 2025. Serum adalimumab and anti-adalimumab antibody (AAA) measurements were obtained as part of a prospective research protocol on TDM, not in response to clinical treatment failure. The study was approved by the Cleveland Clinic Abu Dhabi Institutional Review Board (IRB, protocol no. A-2024-041). Informed consent was waived by the IRB due to the observational, non-interventional design, in accordance with institutional policy for minimal-risk research. The study adhered to the tenets of the Declaration of Helsinki.
Inclusion criteria comprised a confirmed diagnosis of NIU according to the Standardization of Uveitis Nomenclature criteria, 18 continuous adalimumab monotherapy (40 mg every 2 weeks) for a minimum of 12 months, and the availability of both serum adalimumab and AAA measurements. All enrolled patients had been on adalimumab monotherapy without concomitant systemic immunosuppression for the entire 12-month period preceding inclusion; any prior corticosteroids or disease-modifying antirheumatic drugs had been discontinued at least 12 months before enrolment. Patients were excluded in cases of noncompliance or irregular injection intervals, concomitant or recent use of systemic corticosteroids, disease-modifying antirheumatic drugs, or other biological agents, infectious uveitis, or incomplete data. No eye-specific clinical outcome data were collected; in patients with bilateral uveitis, the more severely affected eye was recorded for anatomical classification purposes only.
Body composition assessment
Body composition was assessed by use of the InBody 770 multifrequency bioelectrical impedance analyser (Biospace, California, USA). 19 Participants were instructed to fast for at least 3 hours and to avoid physical activity on the day of testing. All measurements were performed between 08:00 and 10:00 on the same day as blood sampling for trough concentration measurement. Height and weight were recorded to the nearest 0.1 cm and 0.1 kg, respectively. The device was calibrated according to the manufacturer’s guidelines. Subjects stood barefoot on the scale and held the electrodes with arms extended at approximately 15 degrees, ensuring full contact with the sensors. The analyser applies alternating electrical currents at six frequencies (1, 5, 50, 250, 500, and 1,000 kHz) to derive body composition parameters, including total body water, protein, mineral content, fat-free mass, skeletal muscle mass, total body fat mass (BFM), percent body fat (PBF), and visceral fat area (VFA). 20
Serum sampling and assays
A single 5 mL venous blood sample was collected immediately prior to the next scheduled adalimumab injection, corresponding to a steady-state trough concentration, and stored at −80°C until analysis. Serum adalimumab trough concentrations and anti-adalimumab antibodies were quantified using standardized commercial assays (LabCorp, Calabasas, CA, USA). The lower limit of quantification (LOQ) for adalimumab was 0.6 µg/mL; concentrations below this threshold were measurable by the assay but are reported as below the LOQ. AAA positivity was defined as antibody levels exceeding 25 ng/mL, corresponding to the manufacturer-validated positivity threshold of the drug-sensitive assay.
Outcomes
The primary outcome was the association between body composition parameters and serum adalimumab trough concentration. Secondary outcomes included the relationship between body composition indices and AAA levels.
Statistical analysis
Data were analyzed using Python (version 3.11) and R (version 4.3). Distributional assumptions were assessed using the Shapiro–Wilk test. Continuous variables are reported as mean ± standard deviation for normally distributed data and as median with interquartile range (IQR) for non-normally distributed variables. Categorical variables are reported as counts and percentages.
Associations between serum adalimumab trough concentrations and anthropometric or body composition parameters were evaluated using Pearson correlation coefficients (interpreted as weak |r| < 0.3, moderate 0.3–0.5, or strong > 0.5). Comparisons across body-fat-mass tertiles were performed using the Kruskal–Wallis test. Categorical variables were compared using the χ2 test or Fisher exact test.
To explore independent determinants of variability in adalimumab trough concentrations, separate multivariable linear regression models were constructed for each adiposity parameter (BMI, total BFM, PBF, VFA), each adjusted for age and sex. Models were compared using adjusted R2 and Akaike information criterion (AIC). Unstandardized regression coefficients (β) were reported to provide clinically interpretable estimates of the change in adalimumab concentration per unit change in each adiposity parameter.
Receiver operating characteristic (ROC) curve analyses were performed to compare the ability of BMI and body composition parameters to discriminate patients with trough concentrations below the LOQ (0.6 µg/mL). Areas under the curve (AUCs) were calculated with 95% confidence intervals (CIs), and pairwise comparisons were performed using the DeLong test.
The study was exploratory and not formally powered for immunogenicity outcomes; therefore, antibody-related analyses should be interpreted cautiously. Statistical significance was defined as a two-sided P value less than 0.05.
Results
A total of 45 patients were enrolled (44 with complete body composition data; one patient had missing anthropometric values). The median age was 38.5 years (IQR 19.2–44.2; range 12–65), with an equal sex distribution (50% female). All patients had been receiving adalimumab monotherapy for at least 12 months at the time of assessment. Baseline demographic, anthropometric, body composition, and laboratory characteristics are presented in Table 1.
Baseline Patient Characteristics (n = 45)
Baseline demographic, anthropometric, and body composition measurements for patients with noninfectious uveitis.
BMI, body mass index; SD, standard deviation.
The median serum adalimumab trough concentration was 6.70 µg/mL (IQR 3.57–12.25). Trough concentrations were above the LOQ (≥0.6 µg/mL) in 35 patients (78%); the remaining 10 patients (22%) had concentrations below the LOQ but still measurable by the assay. Anti-adalimumab antibodies were detected in 13 patients (29.5%) at concentrations exceeding 25 ng/mL.
Associations between body composition and adalimumab trough concentrations
BMI was found to be moderately inversely correlated with adalimumab trough concentration (r = −0.51, P = 0.0004; unstandardized β = −0.53 µg/mL per kg/m2) (Fig. 1A). Bioimpedance-derived adiposity indices demonstrated comparable negative associations: BFM (r = −0.51, P = 0.0004; β = −0.25 µg/mL per kg; Fig. 1b), PBF (r = −0.48, P = 0.001; β = −0.24 µg/mL per %; Fig. 1c), and VFA (r = −0.53, P = 0.0002; β = −0.05 µg/mL per cm2; Fig. 1d). These correlations were similar in magnitude to that observed with BMI. No significant correlation was observed between adalimumab levels and lean mass parameters, including total body water, protein, minerals, fat-free mass, and skeletal muscle mass (all P > 0.05).
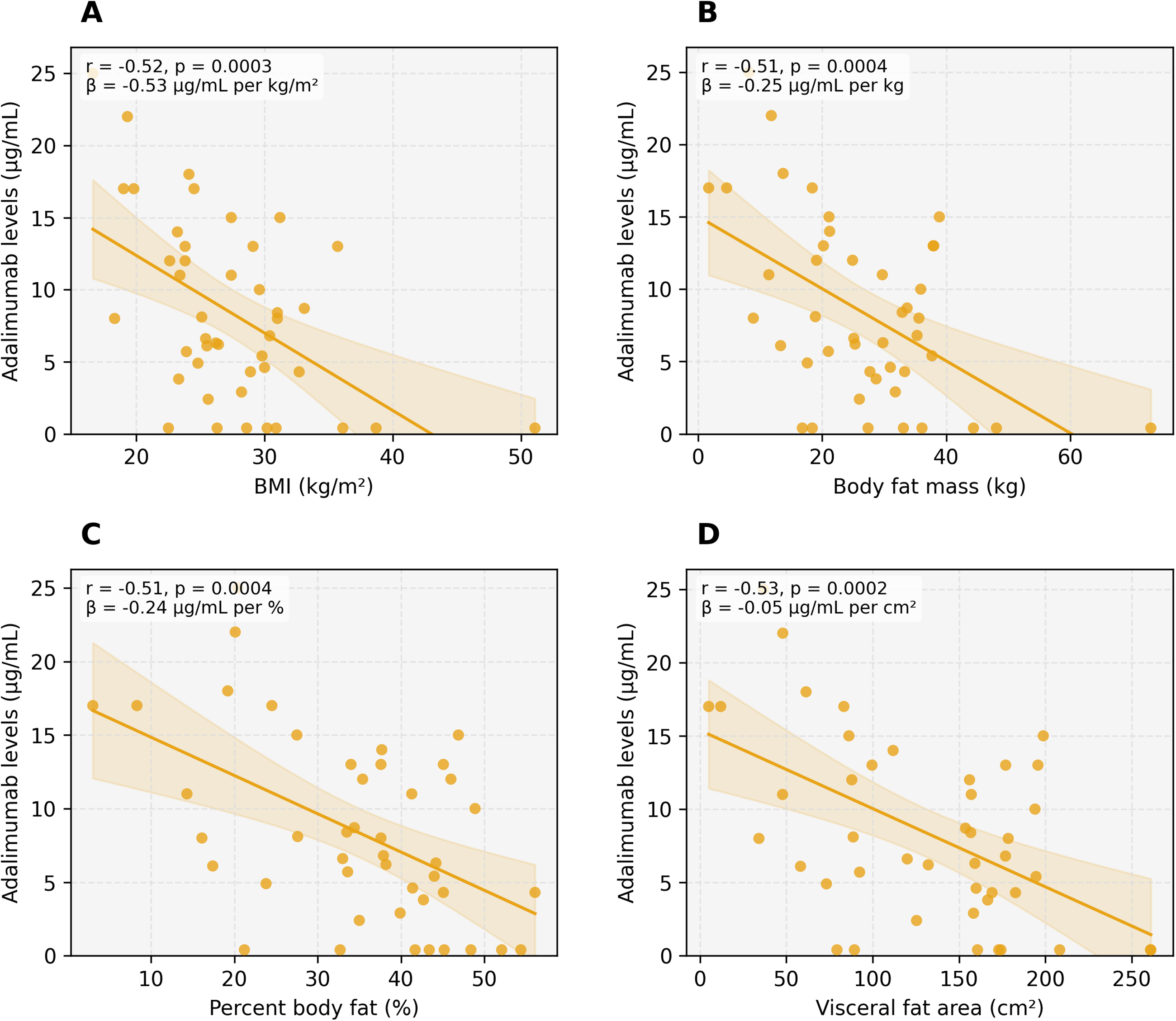
Scatter plots showing the relationship between adalimumab trough concentrations and
When patients were stratified into tertiles of total BFM (low: 1.7–20.2 kg, n = 15; mid: 21.0–31.8 kg, n = 14; high: 32.9–73.0 kg, n = 15), mean adalimumab concentrations were 11.26 µg/mL in the lowest tertile, 6.92 µg/mL in the middle tertile, and 5.82 µg/mL in the highest tertile (Kruskal–Wallis P = 0.054; ANalysis Of VAriance, ANOVA P = 0.038) (Fig. 2).
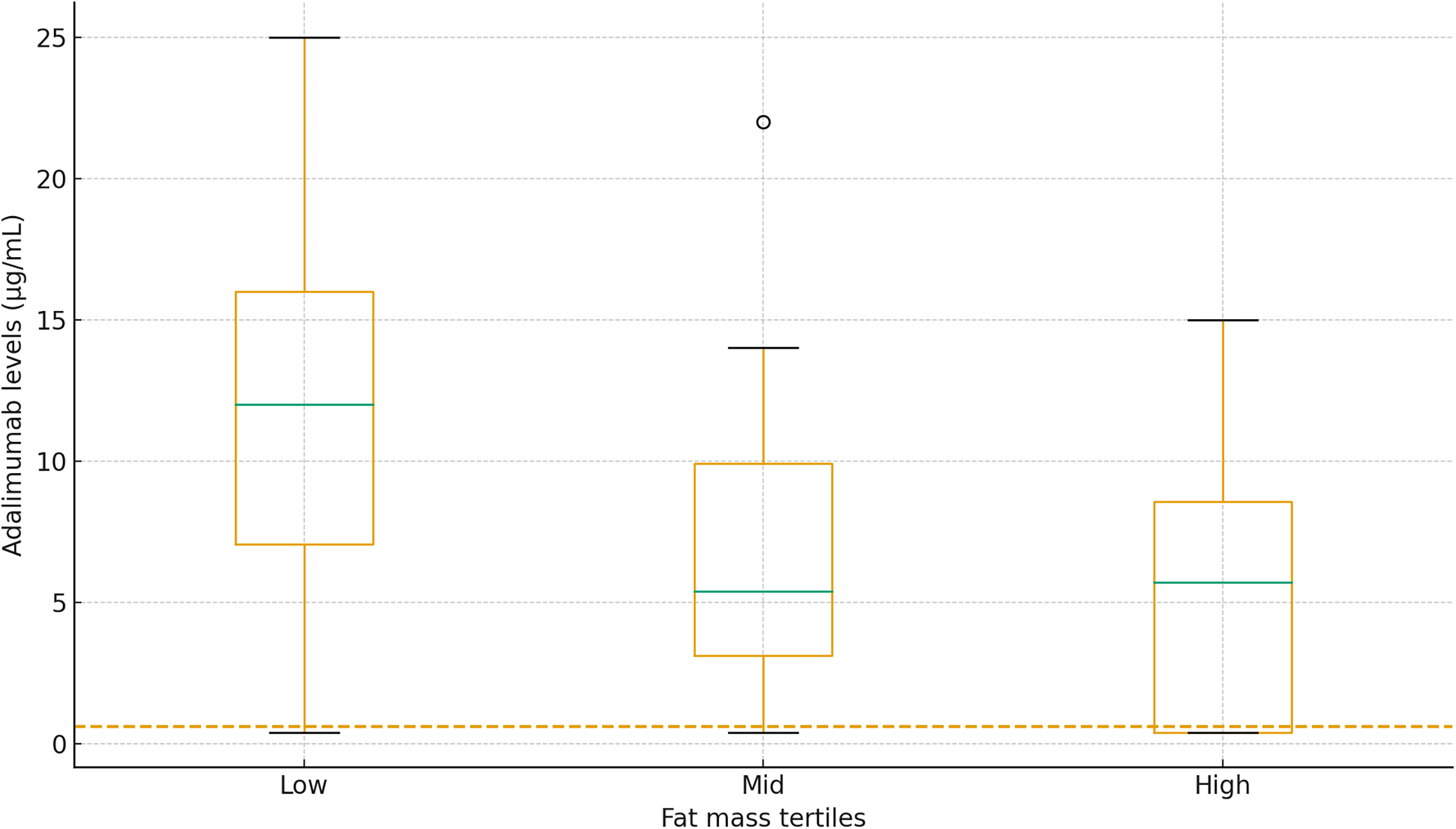
Boxplot of adalimumab trough concentrations across tertiles of body fat mass (low: 1.7–20.2 kg; mid: 21.0–31.8 kg; high: 32.9–73.0 kg). The dashed line represents the lower limit of quantification of the assay (0.6 µg/mL). P value refers to Kruskal–Wallis test.
Multivariable regression analysis
In separate multivariable linear regression models adjusted for age and sex, each adiposity parameter was independently associated with adalimumab trough concentrations. The model including VFA showed the highest explanatory capacity (adjusted R2 = 0.25, AIC = 277.1), followed by BMI (adjusted R2 = 0.24, AIC = 278.1), BFM (adjusted R2 = 0.22, AIC = 279.1), and PBF (adjusted R2 = 0.18, AIC = 281.0). In all models, age and sex were not significant independent predictors (all P > 0.2). The similar adjusted R2 values across models are consistent with the strong intercorrelation among adiposity parameters.
ROC analysis
ROC curve analysis compared the ability of BMI and InBody-derived indices to identify patients with trough concentrations below the LOQ (n = 10 patients; Fig. 3). The AUC was 0.74 (95% CI 0.54–0.92) for VFA, 0.74 (95% CI 0.53–0.92) for PBF, 0.70 (95% CI 0.48–0.89) for total BFM, and 0.69 (95% CI 0.45–0.90) for BMI.
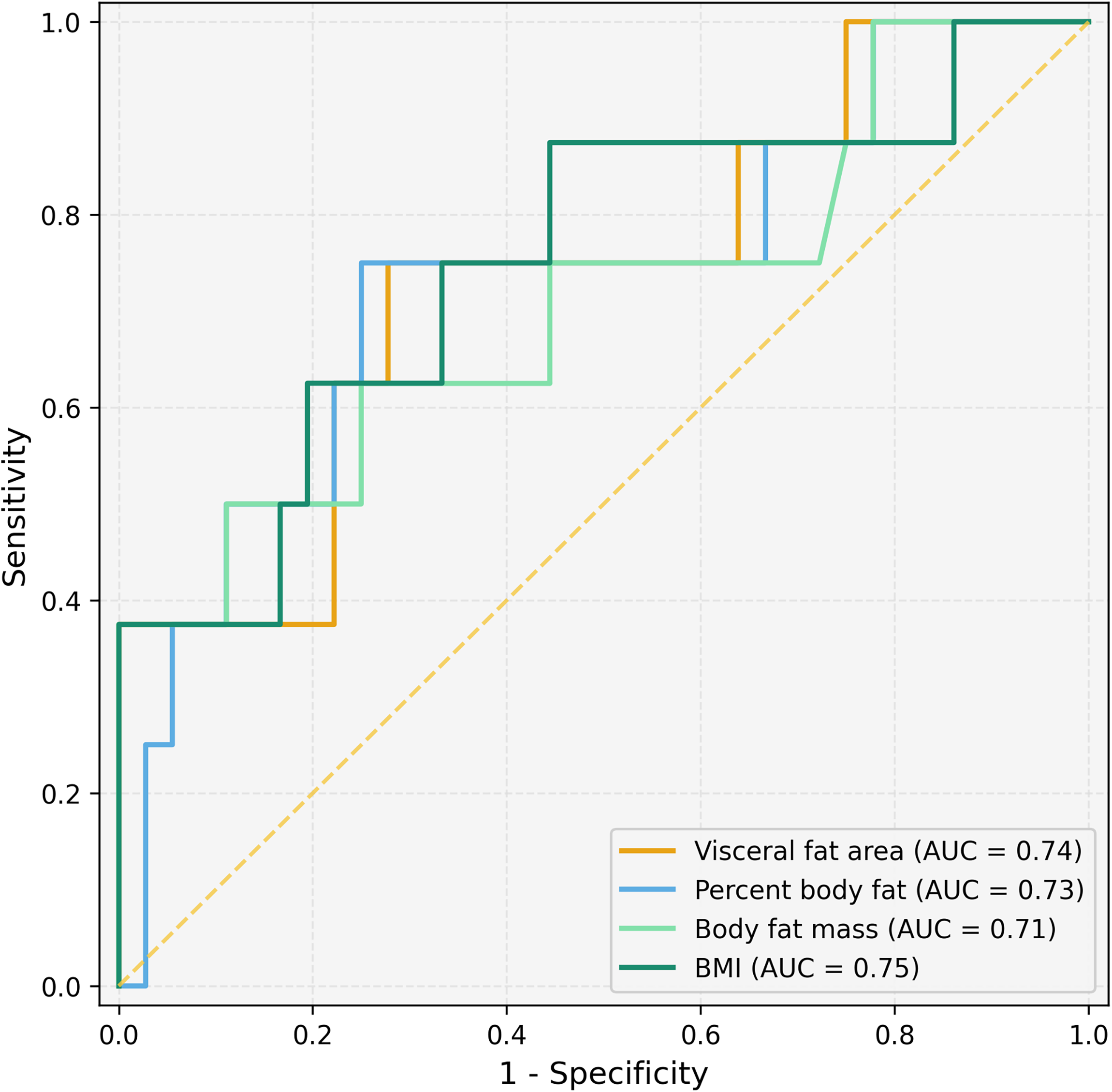
Receiver operating characteristic (ROC) curves for BMI, total body fat mass, percent body fat, and visceral fat area in discriminating adalimumab trough concentrations below the lower limit of quantification (<0.6 µg/mL). Areas under the curve (AUC) with 95% confidence intervals are reported. Pairwise DeLong test comparisons showed no significant differences (all P > 0.5). BMI, body mass index.
Pairwise DeLong comparisons showed no statistically significant differences between ROC curves (VFA vs BMI: ΔAUC = 0.054, P = 0.52; PBF vs BMI: ΔAUC = 0.054, P = 0.57; BFM vs BMI: ΔAUC = 0.014, P = 0.85). These results indicate that BMI and bioimpedance-derived adiposity metrics have comparable ability to identify patients at risk of low drug exposure.
Immunogenicity
In exploratory analyses limited by the small number of AAA-positive patients (n = 13), lean mass parameters were not significantly correlated with anti-adalimumab antibody titers (all P > 0.1). BMI was found to have the strongest positive correlation with antibody levels (r = 0.58, P < 0.0001), followed by BFM (r = 0.45, P = 0.002) and VFA (r = 0.30, P = 0.049). PBF was not significantly correlated with antibody levels (r = 0.22, P = 0.16).
A composite drug-to-antibody ratio [adalimumab (µg/mL) divided by antibodies (ng/mL)] declined with increasing adiposity (Fig. 4), correlating inversely with VFA (r = −0.48, P = 0.0009), BMI (r = −0.48, P = 0.001), BFM (r = −0.46, P = 0.002), and PBF (r = −0.43, P = 0.003). These findings suggest that adiposity may be associated with both reduced drug exposure and increased immunogenicity, although they require confirmation in larger cohorts.
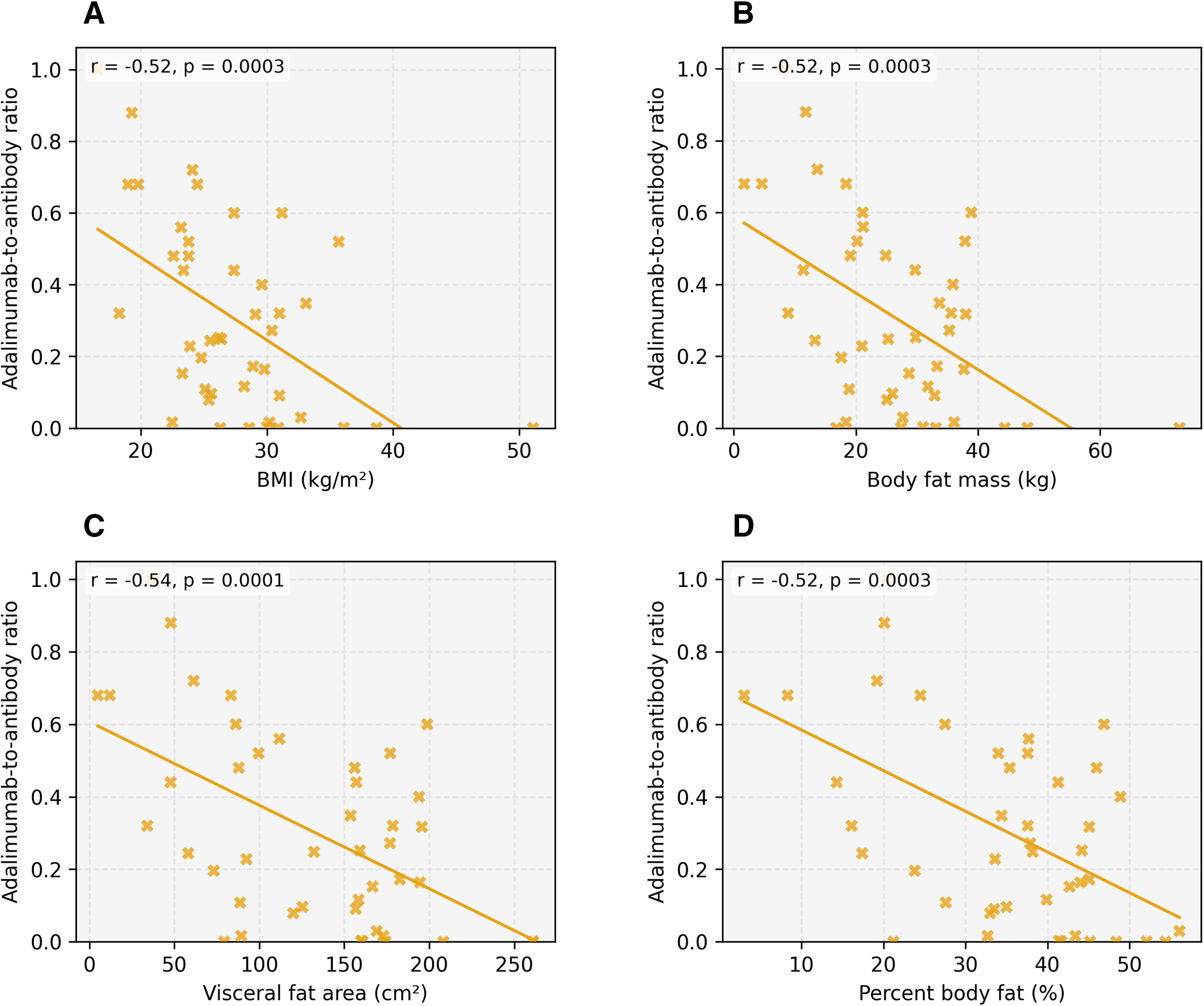
Relationship between adiposity measures and the adalimumab-to-antibody ratio (adalimumab trough concentration divided by anti-adalimumab antibody titer). Panels show
Discussion
The present study demonstrates that both BMI and objective measures of body composition are associated with interindividual variability in adalimumab exposure and immunogenicity under fixed-dose therapy in NIU. BMI and bioimpedance-derived adiposity parameters showed comparable inverse correlations with trough concentrations. The present data do not demonstrate clear superiority of body composition metrics over BMI; however, they confirm that adiposity is a relevant determinant of adalimumab pharmacokinetic variability and suggest that bioimpedance-derived measures may provide biologically complementary information.
Of note, these findings are of particular relevance in the setting of uveitis, where adalimumab is the only biological currently approved and where maintaining adequate drug exposure is essential to prevent disease flares that may lead to irreversible vision loss.1,2 We have previously reported that higher BMI is associated with lower adalimumab concentrations and greater disease activity in both adult and pediatric uveitis6,7 and that TDM-guided management can improve clinical outcomes. 3 The present study extends these observations by characterizing how specific body composition compartments relate to drug exposure.
The three adiposity parameters assessed in the present study—total BFM, PBF, and VFA —reflect different aspects of adiposity with distinct biological relevance to monoclonal antibody pharmacokinetics. Total BFM is an absolute measure of fat tissue and is most directly related to the expansion of the apparent volume of distribution, which dilutes circulating drug in proportion to total fat burden. 11 PBF normalizes fat mass to total body weight, capturing the relative contribution of adiposity independent of body size; this may be particularly informative in patients at the extremes of body weight, where BMI can be misleading. 8 VFA specifically quantifies metabolically active intra-abdominal adipose tissue, which is the primary source of pro-inflammatory cytokines and adipokines implicated in Fc receptor-mediated clearance and antidrug antibody formation.14,15,21 The observation that VFA showed the strongest correlation with trough concentrations (r = −0.53) and the highest adjusted R2 in regression analysis (0.25), while PBF was not correlated with antibody levels, is consistent with this mechanistic framework: visceral adiposity may contribute to both volume-of-distribution effects and inflammation-driven clearance, whereas total and relative fat mass primarily influence the former.
The complementary value of body composition metrics over BMI lies in their ability to distinguish between distinct pharmacokinetic mechanisms. BMI conflates fat mass and lean mass into a single index; a patient with high BMI due to muscle mass is pharmacokinetically different from one with high BMI due to visceral adiposity. Bioimpedance analysis separates these compartments, allowing clinicians to identify whether low drug exposure is driven primarily by volume-of-distribution expansion (reflected by BFM), relative adiposity (PBF), or inflammation-driven clearance (VFA). Although these parameters did not outperform BMI in the present cohort, their biological specificity may prove informative in individual patients where BMI poorly reflects true adiposity—such as highly muscular or sarcopenic individuals.
Our findings are in line with previous pharmacokinetic studies in other immune-mediated diseases. In rheumatoid arthritis, body weight and BMI have been identified as significant covariates of adalimumab clearance in population pharmacokinetic models. 22 In inflammatory bowel disease, obesity has been associated with lower trough concentrations and higher rates of treatment failure with anti-TNF agents.16,17,23 Similarly, studies using dual-energy X-ray absorptiometry in infliximab-treated patients have reported comparable associations between fat mass and drug exposure. 24 The correlation magnitudes observed in our cohort (r = −0.48 to −0.53) and the regression slopes (β = −0.53 µg/mL per kg/m2 for BMI) are consistent with those reported across indications, suggesting that the influence of adiposity on monoclonal antibody pharmacokinetics may be a general phenomenon not limited to specific disease settings.
The comparable performance of BMI and body composition metrics in both correlation and ROC analyses warrants careful interpretation. BMI, despite its known limitations as a measure of adiposity, is itself moderately correlated with BFM and VFA, which may explain the similar magnitude of associations observed. In a sample of this size (n = 45), detecting statistically significant differences between closely correlated predictors would require substantially greater statistical power. It remains plausible that in larger or more heterogeneous populations, body composition metrics could provide incremental predictive value, particularly in patients where BMI poorly reflects true adiposity, such as highly muscular or sarcopenic individuals.
Notably, adiposity was also associated with immunogenicity in exploratory analyses. Higher fat mass and VFA were linked to increased anti-adalimumab antibody levels and a progressive reduction in the drug-to-antibody ratio. The stronger correlation of BMI with antibody levels (r = 0.58) compared with individual body composition parameters was unexpected and may reflect BMI’s composite capture of both fat mass and metabolic status or may be a consequence of the small AAA-positive subgroup (n = 13). In the setting of uveitis, where antidrug antibody formation is a major cause of secondary treatment failure and may necessitate switching to alternative agents with less clinical evidence, understanding factors that predispose to immunogenicity has practical implications. However, these findings should be considered hypothesis-generating.
Limitations of the present study include the modest sample size (n = 45), which limits statistical power for detecting differences between closely correlated predictors, and the small number of AAA-positive patients (n = 13), which particularly limits immunogenicity findings. The study population includes both pediatric and adult patients (age range 12–65 years); although age was included as a covariate in multivariable models, age-related differences in body composition represent a potential confounding factor. The cross-sectional design captures data at a single time point and does not allow assessment of longitudinal exposure dynamics or causal relationships. Body composition was assessed by use of bioimpedance analysis, which, while practical and noninvasive, is less precise than imaging-based modalities such as Dual-Energy X-ray Absorptiometry (DXA) or computed tomography. 25 Other factors known to influence monoclonal antibody pharmacokinetics, including serum albumin levels, inflammatory burden, and disease activity, were not systematically incorporated.
Notwithstanding these limitations, the controlled clinical context of fixed-dose adalimumab monotherapy minimizes several confounders typically present in pharmacokinetic studies of biologics, including dose escalation and concomitant immunosuppression. The convergent associations observed across multiple adiposity parameters strengthen the finding that body fat is a relevant determinant of adalimumab exposure.
Conclusions
In this cohort of patients with NIU, bioimpedance-derived adiposity measures and BMI showed similar associations with adalimumab exposure. Body composition parameters may offer complementary biological context for interpreting pharmacokinetic variability and immunogenicity in the setting of biological therapy for sight-threatening uveitis. Future prospective studies with larger sample sizes are warranted to determine whether integrating body composition data into TDM improves identification of patients at risk of low exposure and immunogenicity.
Authors’ Contributions
F.P.: Conceptualization, methodology, formal analysis, investigation, writing—original draft, and supervision. R.S.: Investigation and data curation. P.N.: Conceptualization, methodology, writing—review and editing, and supervision.
Ethics Approval
The study was approved by the Cleveland Clinic Abu Dhabi Institutional Review Board (protocol no. A-2024-041). Informed consent was waived due to the observational, non-interventional design. The study adhered to the tenets of the Declaration of Helsinki.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Footnotes
Author Disclosure Statement
Francesco Pichi, Rauda Shehab, and Piergiorgio Neri declare that they have no conflicts of interest relevant to this article.
Funding Information
No external funding was received for this study.