
Abstract
The clinical tolerability profiles of cyclosporine A (CsA) ophthalmic emulsions differ markedly between anionic (Restasis®, 0.05% CsA) and cationic (Ikervis®, 0.1% CsA) formulations, despite delivering the same active compound. Anionic emulsions are more frequently associated with transient blurred vision, whereas cationic emulsions are more frequently associated with instillation-site pain. The mechanistic basis for this divergence has not been clearly defined, and conventional evaluation has relied on animal-based irritation assays or large clinical trials. This Commentary proposes a two-phase physicochemical interpretive framework, aligned with New Approach Methodologies (NAMs) and Integrated Approaches to Testing and Assessment (IATA), in which rotational rheometry is used to characterize early instillation-phase behavior (0–5 min) and gas chromatography–mass spectrometry (GC–MS) is used to characterize sustained post-instillation-phase features (5–30 min). Preliminary observations on Restasis, Ikervis, and a 0.5% carboxymethylcellulose-sodium artificial-tear reference (a nonionic, nonsurfactant, low-nociceptive physicochemical control) are presented as supporting context. Restasis exhibited substantially higher viscosity than Ikervis across all shear rates, whereas Ikervis and the CMC reference showed comparable high-shear viscosity despite markedly different reported tolerability—a viscosity–discomfort dissociation. GC–MS putatively identified a long-chain tertiary amine signal exclusively in Ikervis (retention time ≈13.0 min), which was absent in Restasis and the CMC reference. The proposed framework is hypothesis-generating rather than mechanistically conclusive; it is intended to support future targeted validation studies rather than replace clinical evaluation. GC–MS may serve as a useful complementary fingerprinting tool within NAM/IATA-aligned ophthalmic formulation assessment.
Keywords
Introduction
Dry eye disease (DED) is a multifactorial disorder characterized by loss of tear-film homeostasis and ocular surface inflammation. 1 Topical cyclosporine A (CsA), a T-cell–targeted immunomodulator, 2 is widely used in moderate-to-severe DED and, owing to its lipophilicity, requires emulsion-based delivery systems. 3 Two principal CsA formulation technologies dominate clinical practice: an anionic emulsion (Restasis®, 0.05% CsA) and a cationic emulsion (Ikervis®, 0.1% CsA).
Although both deliver the same active compound, their clinical tolerability phenotypes diverge consistently across published data. Cationic emulsions are more frequently associated with instillation-site pain and stinging, whereas anionic emulsions are more frequently associated with transient blurred vision.4–8 Burning sensation, in contrast, has been reported at broadly comparable frequencies between formulations,6,8 suggesting that the divergent endpoints reflect formulation-dependent rather than drug-dependent mechanisms.
Conventional evaluation of formulation-dependent ocular tolerability has relied on animal irritation assays or large clinical trials. The current regulatory environment, however, is shifting toward New Approach Methodologies (NAMs) and Integrated Approaches to Testing and Assessment (IATA), which emphasize mechanistic physicochemical and in vitro data to reduce reliance on animal testing.9,10 Despite this shift, the relationship between laboratory-scale physicochemical fingerprints and patient-reported tolerability phenotypes remains insufficiently defined.
This Commentary proposes a two-phase physicochemical interpretive framework—not as a demonstrated causal mechanism, but as a hypothesis-generating tool for organizing disparate observations across formulations. We hypothesize that rheological behavior may be more relevant to the immediate instillation phase (0–5 min), whereas excipient-phase volatile features detectable by gas chromatography–mass spectrometry (GC–MS) may contribute to sustained post-instillation discomfort (5–30 min). 11 This framework is intended to support, rather than replace, future head-to-head clinical and biological validation studies.
Materials and Methods
Two commercial CsA ophthalmic emulsions, Restasis (0.05% CsA, anionic; Allergan, Irvine, CA, USA) and Ikervis (0.1% CsA, cationic; Santen, Osaka, Japan), were analyzed within their labeled shelf lives. A 0.5% carboxymethylcellulose-sodium (CMC) artificial tear (Refresh Plus®, Allergan) was included as a nonionic, nonsurfactant, low-nociceptive physicochemical control, not as a clinical comparator. Although the CsA concentrations differ between the two emulsions, the bulk rheological behavior of oil-in-water emulsions is governed primarily by excipient composition and emulsion microstructure rather than by active pharmaceutical ingredient (API) concentration.
Rheology
Steady-state shear viscosity was measured using a Discovery Hybrid Rheometer DHR-2 (TA Instruments, New Castle, DE, USA) equipped with a 40 mm, 1° cone-and-plate geometry, Peltier-controlled at 35°C. The shear rate was scanned across 0.1–100 s−1. Each formulation was measured in triplicate (n = 3), and results are reported as mean ± standard deviation (SD). CMC reliable measurements were limited to ≥2 s−1 owing to torque-resolution limits at lower shear.
Gas chromatography–mass spectrometry
Liquid–liquid extraction was performed by mixing 500 µL of formulation with 1.5 mL of ethyl acetate (1:3 v/v), vortexing for 2 min, centrifuging at approximately 900 × g for 10 min, drying the upper organic phase under N2 at 40°C, and reconstituting the residue in 200 µL ethyl acetate. Analysis used an Agilent 7890B GC/5977B MSD with HP-5MS UI column (30 m × 0.25 mm × 0.25 µm); helium 1.0 mL/min; oven 50°C (2 min) → 180°C at 10°C/min (2 min) → 280°C at 5°C/min (10 min); and EI 70 eV, m/z 40–550. Compounds were assigned using the NIST 23 library matching at a ≥70% match-score threshold. Assignments are reported throughout as putative identifications; authentic-standard confirmation was not performed within this study.
Framework and clinical context mapping
Physicochemical descriptors were mapped against published tolerability data extracted from regulatory documents6,8 and peer-reviewed clinical trials.4,5,7,12 No head-to-head RCT directly comparing Restasis and Ikervis exists; cross-study data are presented as an indirect contextual juxtaposition, not as direct comparison, with explicit recognition of cross-study heterogeneity. Detailed methodological parameters are provided in Supplementary Data.
Ethics
This work analyzed only commercial formulations and published aggregate data. No human participants or animals were involved; therefore, institutional review board approval was not required.
Supporting observations
Rheological fingerprints (phase 1 candidate)
At 35°C, both CsA emulsions exhibited non-Newtonian shear-thinning behavior, whereas the CMC reference exhibited near-Newtonian behavior across its measurable range (Fig. 1A). At a shear rate of 0.1 s−1, Restasis viscosity (0.6542 ± 0.0450 Pa·s) was ∼5-fold higher than that of Ikervis (0.1281 ± 0.0320 Pa·s); at 100 s−1, the ratio expanded to >100-fold (0.2520 ± 0.0210 vs. 0.0024 ± 0.0002 Pa·s). At blink-associated high-shear rates, Ikervis (0.0024–0.0042 Pa·s) and the CMC reference (∼0.003–0.004 Pa·s) showed comparable viscosity, consistent with the normal human tear-film range (∼1.5–4 mPa·s). 13 Despite this rheological similarity at high shear rates, their reported tolerability profiles differ substantially, providing the central observation underlying the framework: Viscosity alone is insufficient to account for instillation-site discomfort.
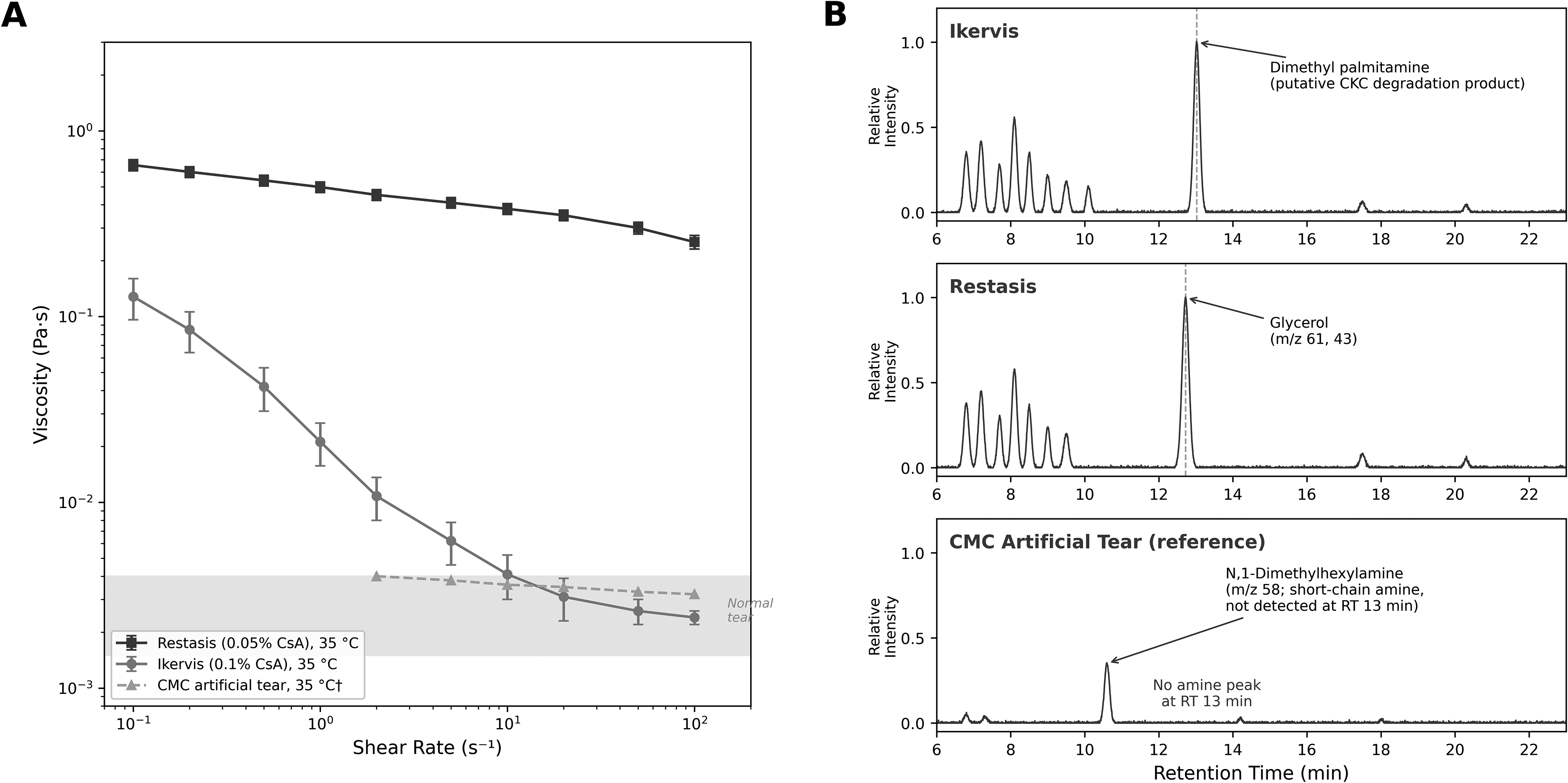
Two-panel summary of physicochemical fingerprinting observations supporting the proposed two-phase NAM framework.
Excipient-phase chemical fingerprints (phase 2 candidate)
GC–MS revealed distinct chemical signatures across the three formulations (Fig. 1B). In Ikervis, a peak with a retention time 13.024 min was putatively identified as a long-chain volatile tertiary amine species (dimethyl palmitamine, C16; m/z 58, 269)—a candidate thermal degradation product or structural analog of cetalkonium chloride (CKC), the cationic surfactant present in Ikervis. In Restasis, the dominant peak at 12.722 min was putatively assigned to glycerol (m/z 61, 43). In the CMC reference, no signal consistent with a long-chain tertiary amine was detected in the 12–14 min region; only a minor peak at ∼10.6 min, putatively assigned to N,1-dimethylhexylamine (short-chain amine, C6; m/z 58), was observed. All assignments are based on NIST 23 library matching and have not been confirmed against authentic standards; the potential for thermal degradation or fragmentation artifacts inherent to GC–MS analysis of surfactant-like species is acknowledged.
Mapping to published tolerability data
Phase 1: Restasis is associated with transient blurred vision (1%–5% per FDA prescribing information), 6 consistent with its higher viscosity profile. Ikervis is associated with a lower incidence of visual disturbance (2.1% in the SANSIKA RCT). 4 Phase 2: Ikervis-associated instillation-site pain has been reported at 29.2% at 6 months (SANSIKA), 4 12.1% in a pooled Phase III analysis (n = 734), 7 and 7.8% at 12 months of continuous treatment in the SANSIKA open-label extension 5 —a trajectory that is consistent with corneal nerve adaptation. Restasis-associated eye pain is reported at 1%–5% according to the FDA label. 6 The long-chain tertiary amine signal detected exclusively in Ikervis represents a candidate formulation-specific excipient-phase feature whose relevance to this pain pattern is hypothesized—not demonstrated.
Internal specificity check
Burning sensation was reported at broadly comparable frequencies across formulations (∼17.5% Ikervis, EMA SmPC 8 ; 17% Restasis, FDA prescribing information). 6 Because this nonspecific endpoint did not show a formulation-dependent directional difference, it functions as an internal specificity control: The divergent patterns in pain and blurred vision against the comparable burning rates support the specificity of the proposed two-phase framework rather than reflecting a generalized irritation difference.
Implications and Limitations
The principal contribution of this Commentary is not the establishment of clinical causality but the proposal of a tractable physicochemical framework that may help interpret formulation-dependent tolerability patterns and guide future targeted validation.
Interpretive value of phase 1
Restasis maintained substantially higher viscosity than Ikervis across the full shear range, providing a plausible mechanical context for the higher reported frequency of transient blurred vision.1,4 The lower viscosity of Ikervis is consistent with rapid spreading on the ocular surface, in line with cationic surface-active behavior promoting interaction with the negatively charged mucin layer.14,15 Recent clinical work integrating rheology with tear-film phenotype-specific outcomes further supports the view that vehicle architecture—rather than CsA concentration alone—is a primary determinant of differential clinical response. 16
Interpretive value of phase 2
The viscosity–discomfort dissociation between Ikervis and the CMC reference at high shear is the core observation motivating Phase 2: A viscosity-independent feature is needed to account for the reported difference in instillation-site pain. The long-chain tertiary amine signal detected exclusively in Ikervis is offered as a candidate feature consistent with this hypothesis. Recent in vitro work demonstrating dose-dependent CKC-induced cytotoxicity in corneal epithelial and endothelial cells, mediated through oxidative stress and disruption of prosurvival signaling pathways, provides biological context for the plausibility of CKC-related excipient contributions to discomfort.17,18 The chain-length contrast between Ikervis (C16) and the CMC reference (C6) is consistent with the broader principle that longer-chain aliphatic amines exhibit greater membrane permeability and nociceptor activation potential. 19
Methodological context
Given that the Draize eye test has long been criticized for limited reproducibility and imperfect translation to human tolerability, 20 the present framework is proposed as a complementary physicochemical strategy aligned with NAM/IATA principles,9,10 providing mechanistic insights rather than seeking to entirely replace biological or clinical evaluations.
Limitations
Several substantial limitations bound the interpretation. First, no head-to-head randomized controlled trial (RCT) directly comparing Restasis and Ikervis tolerability exists; clinical data are derived from independent regulatory documents and vehicle-controlled trials, and cross-study heterogeneity in populations, endpoints, and time points limits direct comparability. Second, the in vitro analytical conditions cannot replicate the dynamic tear-film environment, where mucins, proteins, lipids, salts, blink-induced shear, and rapid dilution all modulate excipient fate; the GC–MS observations therefore describe intrinsic physicochemical fingerprints of the as-formulated product, not predictors of in vivo ocular surface chemistry. Third, compound assignments are putative; authentic standards have not been used, no orthogonal analytical method has been applied to the signal of interest, and no biological assay has tested whether the candidate compound activates nociceptive pathways. Fourth, CMC rheology was restricted to ≥2 s−1 owing to torque resolution limits.
Future Directions
Within the limits set above, the framework defines a tractable validation agenda. Future work will, where feasible, employ (1) authentic-standard GC–MS confirmation of the long-chain tertiary amine signal, (2) orthogonal high-resolution mass spectrometry, (3) in vitro nociception assays—including TRPV1- and TRPA1-related models—to test whether the candidate compound or post-instillation formulation activates ocular surface nociceptive pathways, and (4) ex vivo corneal models that better approximate the dynamic tear-film environment. Eventual head-to-head clinical evaluation under harmonized endpoints would be the definitive test of the framework. The intent of this Commentary is to render the proposed mechanism testable, not to assert that it is true.
Conclusions
This Commentary proposes a two-phase physicochemical interpretive framework—rheology-governed early phase and a GC–MS-detectable excipient-phase contributions to a sustained phase—as a NAM/IATA-aligned, hypothesis-generating tool for ophthalmic formulation tolerability. Preliminary observations on Restasis, Ikervis, and a CMC physicochemical reference are consistent with the framework but do not establish its mechanistic validity. GC–MS fingerprinting may serve as a useful complementary tool alongside rheology in future formulation tolerability assessment. Targeted validation through authentic-standard analytical confirmation and in vitro nociception models remains essential.
Author’s Contributions
J.K.: Conceptualization, data curation, formal analysis, investigation, methodology, visualization, writing—original draft, and writing—review and editing.
Data Availability Statement
The original rheological and GC–MS data supporting the conclusions of this article are available from the corresponding author upon reasonable request.
Supplemental Material
sj-docx-1-opt-10.1177_10807683261466540 — Supplemental material for Physicochemical Fingerprinting of Cyclosporine A Ophthalmic Emulsions as a New Approach Methodology for Clinical Tolerability
Supplemental material, sj-docx-1-opt-10.1177_10807683261466540 for Physicochemical Fingerprinting of Cyclosporine A Ophthalmic Emulsions as a New Approach Methodology for Clinical Tolerability by JaeWoong Koh
Footnotes
Acknowledgment
During the preparation of this work, the author used Anthropic Claude for language editing. After using this tool, the author reviewed and edited the content as needed and takes full responsibility for the content of the publication.
Author Disclosure Statement
The author declares no conflicts of interest with the materials presented herein.
Funding Information
This work was supported by research fund from Chosun University Hospital 2025.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.