
Abstract
Low-intensity laser radiation is characterized by its ability to induce athermic, nondestructive photobiological processes. Although it has been in use for more than 30 years, this phototherapy is still not an established therapeutic modality. We have summarized the main arguments being brought up against the use of this therapy and have reviewed the literature addressing both its in vitro and in vivo effects. We conclude that low-intensity laser irradiations might be of benefit in selected indications if the existing preliminary data can be confirmed by more prospective and well-controlled studies.
Introduction and Terminology
Laser irradiation as a phototherapeutic modality for the induction or acceleration of wound healing was first introduced by Mester and coworkers1 in the 1970s but still is not an established therapy. This is mainly because a substantial amount of research was originally done in Eastern European countries and published in non-peer-reviewed journals. Moreover, there has often been a lack of accuracy in the documentation of exact irradiation protocols and the incorporation of appropriate controls in the past. Additionally, the variety of laser systems and experimental conditions used made comparison of results difficult. Because more well-controlled studies have been performed and because the Food and Drug Administration has initiated research in the field of low-intensity laser therapy,2 this phototherapy is attracting increasing interest.
Light emitted by laser devices is characterized by its monochromaticity, parallelism, and coherence. In contrast to high-power lasers used in surgery and in dermatology for the treatment of pigmented or vascular lesions, hair removal, or skin resurfacing, devices used for low-intensity laser therapy are usually operated at output powers in the milliwatt range. The radiation emitted is athermic, which means that its biological effects are not caused by perceptible heating or cell damage. But because of the observed stimulatory effects of this type of laser irradiation, the term “biostimulation” was introduced. Because inhibitory attitudes of laser irradiation were noted, “biostimulation” was later replaced by “biomodulation.” Regarding the spectrum of laser devices available, the formerly most commonly used helium-neon (HeNe) laser-emitting red light at a wavelength of 632.8 nm is being replaced more and more by cheaper (partially noncoherent) diodes with wavelengths between 660 and 940 nm. Results from recent cell culture studies3,4 initiated discussions on the importance of light coherence, as they showed no difference in the biological responses to irradiation with (coherent) laser light and noncoherent light. The skepticism toward the necessity of coherence is additionally enhanced by the fact that coherence is lost after the incident beam has passed through the first layers of the stratum corneum. Therefore, among the characteristics of laser light, coherence seems to be of only minor importance, which means that lasers simply represent handy, monochromatic light sources.
Remarks on Dosimetric Parameters in Laser Irradiation
The fundamental parameters of a (laser) light irradiation protocol essential for proper comparison of data are as follows: wavelength, frequency, power output, spot diameter, irradiation time, intensity, dose, and treatment intervals. A definition of these terms, their correct units, and usually applied quantity are available from Calderhead5,6 and are summarized in the Table.
Characteristics and fundamental dosimetric parameters of low-intensity laser irradiation.
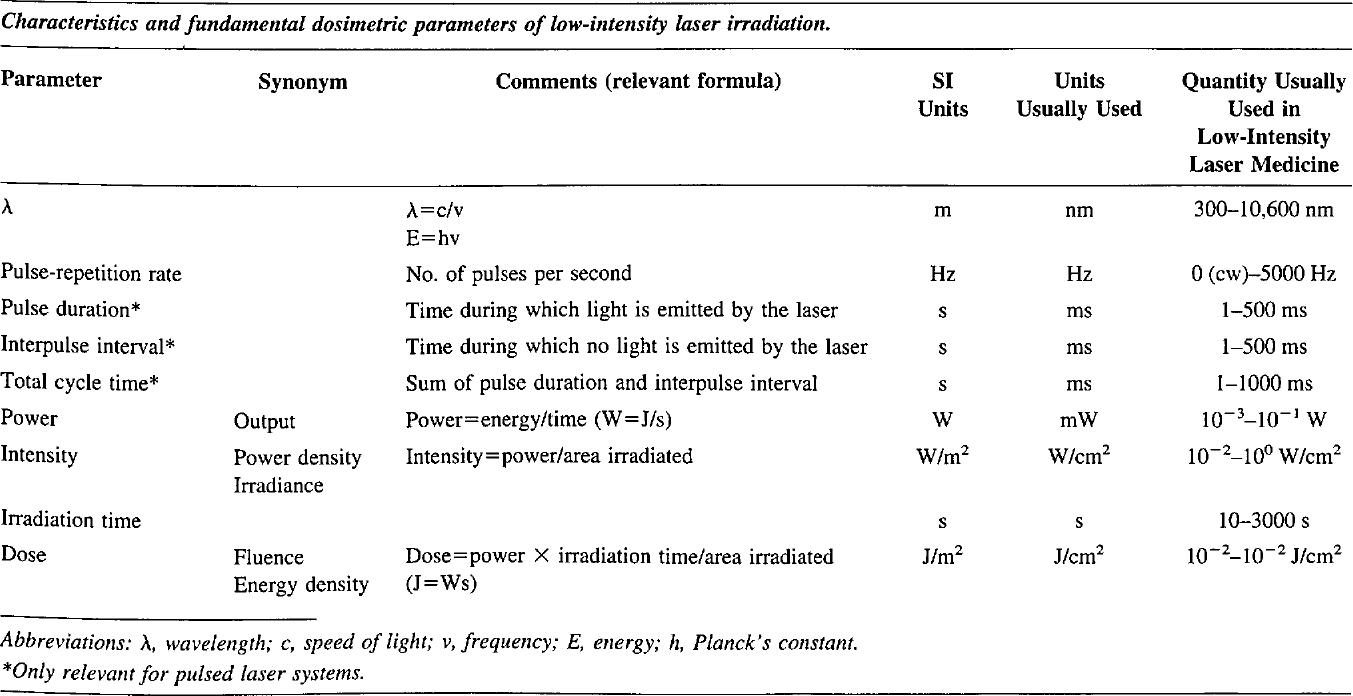
Abbreviations: λ, wavelength; c, speed of light; v, frequency; E, energy; h, Planck's constant.
Only relevant for pulsed laser systems.
Definition of Low-Intensity Laser Irradiation
In addition to the parameters of the light source discussed above, the effect of the energy delivered to the tissue must be taken into account for the definition of low-intensity laser irradiation. For this purpose, the spot size and the exposure time are of significant importance because they determine the intensity and the dose and, therefore, the cell's response to the incident light. Athermic, photochemical reactions, being the basis of low-intensity laser therapy, occur with power densities between 10−2 and 100 W/cm2 and energy densities between 10−2 and 102 J/cm2. Changing the spot size, the exposure time, or both parameters automatically alters the intensity and the dose, thus leading to different types of responses such as coagulation, vaporization, and photoablation.
Although the biological responses in animals and humans using constant low intensities within the above mentioned range, in contrast to some cell culture studies,7 seem to be more closely related to the incident doses applied, we suggest the use of the term “low-intensity laser” irradiation, as it best reflects the independence from temperature changes of the induced effects.
Controversies about Low-Intensity Laser Therapy
In contrast to the usual structure of review articles9–12 and to focus on the most controversial issues concerning low-intensity laser therapy, we give a short overview of the major points of criticism toward this type of phototherapy and discuss each of them in the following section.
1) the Power of Low-Intensity Lasers is Too Small to Produce Any Effect at All13,14
The power output of lasers applied in low-intensity laser therapy are usually in the milliwatt range and, thus, four to five orders of magnitude smaller than radiation emitted by ordinary light bulbs. It, therefore, seems mysterious that such weak light sources could have any effect at all in biological systems.
Biological processes, however, do not necessarily need a large amount of energy to be triggered. In fact, the absorption of even one single photon results in hyperpolarization of the rod-cell plasma membrane, thereby inducing the complex cascade of light perception in the retina.15 Concerning the optical properties of human skin, a recently recognized phenomenon regarding the amplification of the light intensity in the epidermis and dermis seems of major importance: the apparent paradox of greater intensities of light within the skin than that of the incident light beam can be explained by the strong internal reflection and back-scattering of light upon its impact on the skin-air interface. More than 50% of the back-scattered light is reflected back into the skin; thus, what is seen returning from within the skin is only a fraction of that which is actually back-scattered.16 As a result of this phenomenon, the light intensity within the epidermis and the upper papillary dermis can exceed the intensity of the incident light. In the red and near-IR spectral region, this effect is found to be maximal, with an almost 5-fold increase in light intensity at wavelengths greater than 700 nm.17
2) Radiation of Low-Intensity Lasers Does Not Penetrate to Deeper Skin Layers10
Closely related to the argument about the low output power of the light sources used in laser medicine is the argument that, because of their weakness, hardly any energy is transferred to living cells in the epidermis and the dermis. HeNe laser light was found to penetrate as far as 0.5 mm into freshly excised human skin and to deliver the highest relative percentage of the incident energy to a certain volume of tissue as compared with infrared (IR) lasers and IR diodes.18 With longer wavelengths emitted by IR lasers, the depth of penetration has been shown to be even greater, reaching several millimeters.19–21 This can be explained by a sort of an optical window in the visible and IR portion of the electromagnetic spectrum, which means that wavelengths between 600 and 1300 nm are hardly absorbed and scattered in the epidermis and dermis and, thus, can penetrate deeper. In a recent paper by Kolarova et al,22 the influence of the anatomic site, skin thickness, and wavelength of light was investigated in terms of penetration depth. Results show that even in skin biopsies of 2-cm depth, 0.3 and 2.1% penetration for 632 and 675 nm of wavelength, respectively, were detected. In granulation tissue, a 2.5-fold increase in transmittance was noted compared with normal skin.22
In addition, dermal scattering in the visible spectrum is largely forward-directed, and therefore, more photons reach deeper layers. Jacques and coworkers23 found that the mean scattering angle of a HeNe laser (wavelength, 632.8 nm) is approximately 20°. Moreover, a penetration depth of even some microns can be regarded as sufficient, because most of the relevant target cells of low-intensity laser irradiation, eg, for the induction of wound healing (such as fibroblasts, keratinocytes, macrophages, and endothelial cells) are located within the epidermis and upper dermis.
3) the Effects Obtained after Low-Intensity Laser Irradiation Are Inconsistent and Even, in Part, Contradictory13,24
It is difficult to understand how a laser of a specific wavelength should be able to induce stimulatory and inhibitory effects on the same type of cell or tissue. How does the cell know what to do with the incident energy?
As a principle of photobiology, it is necessary for the excitation of a molecule that the energy of the absorbed photon match the difference between the molecule's ground state and its excited singlet state and is correlated with its chemical structure. The energy of an incident photon in turn is dependent on the wavelength. Therefore, it is not surprising that the action spectra of photochemically induced reactions (eg, DNA synthesis) usually do not show linear dependence from wavelength and dosage. This hypothesis is strongly supported by the work of Karu23 and Lubart et al,25 who outlined the influence of the cell's physiological status and the choice of the optimal treatment parameters on the expected radiation effect. Recently, Karu26 reported on seven different maxima in the action spectrum of chemiluminescence of murine cells and adhesion of HeLa cells obtained by irradiating these cells with a pulsed 820-nm diode laser and by varying the dose from 2×101 to 3×104 J/cm2 and the intensity from 4 to 1900 W/cm2. This experiment demonstrated the non-linear behavior of dose-dependence of radiation effects.
Another explanation for the occurrence of both stimulatory and inhibitory effects after laser irradiation of specific parameters is provided by Friedmann and coworkers.27 According to their findings, low doses of light intensify the formation of a transmembrane electrochemical proton gradient in mitochondria, which is followed by a calcium release from the mitochondria into the cytoplasm by an antiport process, which, in turn, subsequently triggers mitosis and cell proliferation. At higher doses, however, too much calcium is released, which causes hyperactivity of calcium-adenosine triphosphatase (ATPase) calcium pumps and exhausts the ATP pool of the cell, thereby inhibiting cell metabolism.
4) Low-Intensity Laser Irradiation Shows No Effect at All
Perhaps the most striking argument against the use of low-intensity (laser) light irradiation comes from a variety of studies in both in vitro28,29 and in vivo30–33 settings in which no detectable effects of the light exposure could be found. The reason for the lack of detectable effects after light exposure can be explained by 1) the true absence of biological responses in the selected setting, 2) inappropriate dosimetry, and 3) inappropriate culture conditions and clinical indications.34
Because most of the low-intensity light-inducible biological reactions were found to occur with doses between 1 and 50 J/cm2, experiments using much lower28,35 or much higher dosages36,37 are unlikely to induce nonthermic photobiological responses. Another cause for the mis-interpretation of data may arise from incorrectly calculated radiation parameters and inappropriate specification of dosimetric terms.38 It is worth noting that reporting the exact irradiation parameters is essential for understanding and reproducing results. A certain lack of accuracy in this respect can be observed, however, even in peer-reviewed journals.39 The need for more detailed information on the irradiation protocols seems to gain importance because there is increasing evidence for the invalidity of the reciprocity between dose and intensity (ie, the regime by which the respective dose is applied seems to influence the biological response).40,41 As stated above, the magnitude and direction (ie, stimulation or inhibition) of the expected biological response seems to depend on the redox potential or, more generally speaking, on the physiological condition of the cell at the time of light exposure.42,43 Thus, it is not surprising that only minor or no effects at all are inducible in normally growing cell cultures and in healthy individuals, respectively.44 Moreover, when in vivo studies are performed in which irradiated and control sites are located in close vicinity (ie, intraindividual controls),30,45,46 the possible induction of systemic effects,47–50 eg, resulting from the paracrinic or systemic secretion of (soluble) growth factors or other cytokines,51–55 has to be considered as an additional factor. In almost all wound healing studies in which interindividual controls have been chosen, a significant improvement was noted after laser irradiation.7,24,44,56 Therefore, as a gold standard, both intraindividual and interindividual controls should be included.47,57,58
5) the Basic Mechanisms of Low-Intensity Laser Irradiation Are Not Understood
Although the mechanisms of action of ultraviolet radiation have been investigated more intensively, there are several well-established hypotheses for the induction of photobiological effects in cells by low intensities of visible and near-IR light. Basically, two sorts of reactions can be distinguished in photobiology: primary (light-induced) reactions and secondary (dark) reactions.
Olson et al59 stated that the primary absorption of light by mitochondrial enzymes results in local heating resulting from enhancement of molecular vibration. Karu60 and others61 suggest that (laser-) light-induced stimulatory and inhibitory effects, respectively, are a result of light absorption by flavins and cytochromes in the mitochondrial respiratory chain, leading to alterations of the electron transfer in the redox pairs being located there. Singlet oxygen being photoinduced by endogenous porphyrins was assumed to be another likely pathway and was extensively investigated by Lubart and others.43,62–64 Finally, Smith,65 by modifying Karu's model, proposed that near-IR radiation in an additional pathway could directly activate Ca2+ channels in the cell membrane by photophysical modifications, thus inducing Ca2+ influx and cell proliferation.
Most likely, two or more of these pathways can be influenced simultaneously by low-intensity light irradiation and contribute to the observed biological responses.
6) There is a Lack of Double-Blinded, Placebo-Controlled Studies
The putative lack of properly controlled, double-blinded studies is one of the most commonly stated argument in the discussion about the effects of low-intensity lasers.14 Despite the growing evidence for the efficacy of low-intensity laser irradiation arising from properly controlled cell culture studies4,42,69 and animal models,8,44,49 the number of double-blinded, placebo-controlled clinical studies is somewhat smaller. Nevertheless, there exists a remarkable number of properly controlled trials in the fields of rheumatology,70,71 rehabilitation medicine,72,73 neurology,74–77 and dermatology (see below).
7) Lasers Can Cure Everything
On the basis of the encouraging results of the early days of laser medicine, the popular medical media praised the cold beam as a magic therapy that could, free from any adverse effects, be used to cure disorders from A (acne) to Z (zoster). Unfortunately, this type of propaganda is still ongoing and nourishes the skepticism toward low-intensity laser therapy.
Although low-intensity laser irradiations seem to be useful in a variety of indications, they should only be applied if they can be expected to be more effective, less invasive, or less expensive than other established therapeutic means. By critically judging the indication, one can avoid criticism that states that the main indication for using the mysterious beam is the readiness of the patient to pay for it.
Summarizing the results of the available properly controlled in vitro and in vivo studies, the following indications of low-intensity (laser-) light irradiations may be regarded as realistic.
Dermatological Indications of Low-Intensity Laser Irradiation with Special Respect to Dermatology
Herpes Infection, Postherpetic Neuralgia, and other Pain Syndromes
Starting with a number of uncontrolled clinical studies, the influence of low-intensity laser therapy on herpes simplex infection has been investigated mainly by German researchers. Haichenberger-Wildner and Michels78 treated 96 patients with herpes simplex infection using a HeNe laser without giving further irradiation parameters. Within 1 to 3 days, healing of the lesions was achieved, and none of the treated patients experienced recurrence at the treated site. Landthaler et al79 used a 647-nm krypton laser operated at an intensity of 50 mW/cm2 and a dose of 4.5 J/cm2 for the treatment of 13 patients with recurrent herpes simplex infections. After 10 sessions of laser therapy, the remission-free interval was prolonged from 30 to 73 days. Interestingly, patients with labial herpes infection showed better results than those with genital infection. These results are in accordance with a recent study by the author's (A.S.) department demonstrating a significant increase in remission intervals in patients with chronic recurrent herpes labialis infection after 10 sessions of low-intensity laser therapy.80 Körner et al81 used a Nd:YAG laser operated at doses between 5 and 183 J/cm2 and found no direct virus-inactivating effect on herpes simplex virus (HSV)-1 cultures but a 50% reduction in virus yield in cultures incubated with irradiated leukocytes. Perrin et al82 observed that in an ear experimental model of HSV latency, repeated exposure to IR laser radiation of the cervical ganglia after HSV inoculation specifically hindered the establishment of virus latency in mice.
Concerning low-intensity laser therapy for the treatment of herpes zoster infection, there is only one case report in which a patient with early-stage herpes zoster infection was treated with a combination of low-intensity (6.4 mJ/cm2) HeNe laser therapy and epidural block therapy.83
The influence of laser treatment (830-nm diode laser; intensity, 3 W/cm2) on long-term postherpetic neuralgia in a double-blinded crossover assessment was investigated by Kemmotsu et al,84 who showed both short-term and long-term analgesia with a dependence of this effect on the duration of pain (ie, patients with shorter duration responded better). Interestingly, the hypoalgesic effect was found to be accompanied by an increase in local skin temperature as recorded by means of IR-thermography. Moore and coworkers76 used the same wavelength (830 nm) in a double-blinded crossover study design in patients suffering from postherpetic neuralgia for more than 6 months and applied twice weekly four laser irradiations and sham irradiations. Concomitant medication was left unaltered throughout the trial period. Pain severity was assessed using a linear analog scale and was found to be reduced by approximately 75% by laser irradiation. During a follow-up period of 3 to 6 months, 80% of the patients had maintained their improvement in pain level.
In a placebo-controlled study, Moore and colleagues85 documented a reduction in extent and duration of postoperative pain after abdominal surgery. The 830-nm diode laser was used at an intensity of 3 W/cm2 and a dose of 24 J/cm2. Irradiations were carried out around the incision immediately after wound suture. The amount of additional analgesics administered to the patients on demand was significantly lower in the laser-treated group.
The mechanisms by which laser irradiation attenuates pain, albeit not yet fully understood, are becoming more and more elucidated. Besides the possible alteration of endorphin secretion86 induced by laser exposure, a reduction of abnormal crosstalk between various nerve fibers, which has been assumed to be responsible for neurogenic pain, could be another pathway of action.87 The findings reported by Walker75 and Zarkovic et al88 point to the possibility that laser irradiation could alter the metabolism of serotonin. The ischemia-induced pain sensation can also be relieved by laser therapy. In these cases, pain reduction is most probably a result of the improvement of microcirculation resulting from both short-term and long-term effects of light exposure.89,90
Surgery
Especially in dermatological and plastic surgery, different types of flaps are routinely used. It is therefore interesting that laser irradiation could have a positive influence on flap perfusion and survival. Kubota and Oshiro91 reported on an improvement of microcirculation in caudal-based random pattern flaps in rats measured by means of laser speckle flowmetry after a single 830-nm diode laser treatment. Intensity in this study was 600 mW/cm2 and, because the irradiation time was set to 1 minute, the dose applied was 36 J/cm2. Moreover, at a 5-day follow-up, the survival area in the laser-treated group was greater than that of the sham-irradiated control group. The same wavelength was used by Kami and colleagues,92 who irradiated caudal-based skin flaps in rats applying 800 mW/cm2 and 20 J/cm2, respectively, pre-and postoperatively for 5 consecutive days and compared survival areas with a nonirradiated control group. In both laser-treated groups, the survival areas were significantly larger. In separately performed experiments, skin blood flow, as determined by an electrolytically generated hydrogen clearance monitor, and histology-based blood vessel counts were found to be significantly higher in the laser group. In an article by Zhang et al,93 a defocused CO2 laser was used to treat full-thickness cranial-based dorsal skin flaps in a rat model. The intensity was 300 mW/cm2, and irradiation was performed twice daily on 7 consecutive days. In addition to a significantly longer flap survival period found in the laser group, a smaller extent of skin necrosis was seen histologically, and a decrease in lactate dehydrogenase activity was noted. The authors concluded that the latter could be responsible for a reduced total lactate content, thus helping to control acidosis at the cellular level.
Wound Healing
Disturbed wound healing often has a multifactorial genesis and still represents a challenge to physicians. Low-intensity laser irradiation has been investigated for its possible beneficial influence in recalcitrant wounds. In the past few decades, a great number of publications has documented the effects of (laser) light on different cellular and humoral components of wound healing in vitro and in vivo. Because of the great variety of experimental settings and laser parameters used, the findings are difficult to compare and sometimes conflicting. In the following, we give a short overview of the influence of lasers (and other light sources emitting low doses of visible and IR radiation) on epidermal, dermal, and blood cells that are involved in wound healing.
Effects of Low-Intensity Laser Irradiation on Cellular Components of Wound Healing
Fibroblasts. Fibroblasts are cells of paramount importance in the process of wound healing. Therefore, it is not surprising that a large amount of data exists on their behavior after light exposure. In the work by Lubart et al,25 a nonlinear dose and intensity dependence of the mitosis rate of human fibroblasts was reported after irradiation with two different wavelength ranges of noncoherent light. Similar results were obtained by Dyson's group,94 who used an 860-nm diode laser to irradiate human fibroblasts. Their results suggested a relationship between fibroblast proliferation and succinic dehydrogenase (an enzyme located in the respiratory chain of the cell's mitochondria). At a dose of 2 J/cm2, both cell proliferation and enzyme activity were significantly increased, whereas at a dose of 16 J/cm2, inhibition of both parameters was noted, once more pointing to the dose dependence of biological responses after light exposure. In a study performed by Yu and colleagues,95 cell proliferation and release of basic fibroblast growth factor (bFGF), a potent mitogen and chemotactic factor for fibroblasts and endothelial cells, after irradiating fibroblast cultures with a 660-nm laser was found to be maximal at a dose of 2.2 J/cm2.
Loevschall and Arenholt Bindslev96 investigated the effect of 812-nm laser irradiation on DNA synthesis of human buccal fibroblasts, as measured by 3H-thymidine uptake. In this study, relatively low energy densities, between 0.0005 and 5 J/cm2, were administered. With a constant intensity of 4.5 mW/cm2, a maximal increase in DNA synthesis was found at a dose of 0.5 J/cm2.
Porreau-Schneider et al97 investigated the ability of a single HeNe-laser irradiation (dose, 1.2 J/cm2) to transform fibroblasts into myofibroblasts both in vitro and in vivo. These modified fibroblasts play a role in granulation tissue contraction during wound healing. The results obtained showed a direct and massive transformation of the cultured fibroblasts into myofibroblasts starting 24 hours after light exposure. Moreover, a greater amount of myofibroblasts was found in the connective tissue of laser-treated gums than in unirradiated control sites. A dose-dependent enhancement of cell proliferation resulting from low-intensity HeNe-laser irradiations was observed by Atabey et al98 in normal human fibroblasts.
An excellent overview of both inhibitory and stimulatory effects of laser irradiation on the control of connective tissue metabolism and their possible dermatological relevance is available from Abergel et al.99 They also reported on significant increased procollagen production by cultured fibroblasts after 632.8- and 904-nm laser irradiation.100
Keratinocytes and epithelial cells. Haas and coworkers69 investigated the effects of low-intensity HeNe-laser irradiation on cell proliferation and migration in artificially wounded cultures of keratinocytes. The radiation (intensity, 6.5 mW/cm2; dose, 0.8 J/cm2) was applied three times during a 20-hour period. Although there was no significant change in the proliferation rate, cell motility was found to be significantly greater in the irradiated cultures, thus giving another possible explanation for the laser-induced stimulation of wound healing. Using the same wavelength (632.8 nm) at doses between 0.5 and 1.5 J/cm2, Yu et al55 recently demonstrated the induction of interleukin (IL)-1 and IL-8 secretion by cultured human keratinocytes. These cytokines are supposed to play a major role in the process of wound healing. Steinlechner and Dyson42 used confluent and subconfluent cultures of keratinocytes grown in either 5 or 1% fetal calf serum to determine the influence of culture conditions on the proliferation rate. Two different wavelengths were tested: 632.8 nm (continuous wave), 904 nm (200-ns pulses at frequencies of 1.2 and 3.1 kHz). The results indicated that all wavelengths stimulated keratinocyte proliferation when energy densities between 0.5 and 4 J/cm2 were applied and that the effect was more pronounced in cultures grown in the medium containing only 1% fetal calf serum. Moreover, in this study, the delay in proliferation observed in keratinocytes taken from confluent cultures could be reduced by laser irradiation. These observations, once again, underline the dependence of the cell's physiological status on light-induced effects. By repeated administration of much higher doses of HeNe-laser light (intensity, 40 mW/cm2; energy densities, between 12 and 140 J/cm2) to cultures of rat kidney epithelial cells, Gross and Jelkmann101 found significant inhibition of proliferation rate, whereas a single exposure with 140 J/cm2 was followed by an increase in mitosis rate.
In a recent study by Grossman and colleagues,63 the role of reactive oxygen species for the induction of laser-induced proliferation of normal human keratinocytes was investigated: normal human keratinocytes were exposed to a single dose of 0 to 3.6 J/cm2 (wavelength, 780 nm), and the incorporation of 3H-thymidine, as well as the percentage of dividing cells and total number of cells, was measured. The results indicated that irradiation at doses between 0.45 and 0.95 J/cm2 enhanced keratinocyte proliferation 1.3- to 1.9-fold and that this stimulatory effect could be suppressed by adding antioxidants, which indicates an apparent involvement of reactive oxygen species in this response.
Macrophages. Because macrophages are an important source of various mediators of tissue repair, many research activities have been performed, particularly by Dyson's group, to elucidate their role in light-mediated wound healing. In several studies, the ability of (laser) light to alter the secretion of growth factors from macrophage-like U-937 cells has been documented: 12 hours after irradiating the U-937 cells, the supernatant was removed and added to fibroblast cultures to determine the effect of soluble growth factors expressed as a result of light exposure. By use of this experimental setting, a great variety of irradiation parameters, such as degree of polarization,53 coherence, dose,102 and pulse repetition rate,103 were tested. In summary, these experiments showed that coherent as well as noncoherent light with wavelengths in the red and IR region at doses between 1 and 8 J/cm2 and pulse frequencies ranging from 2 to 300 Hz are apparently able to indirectly stimulate fibroblast proliferation via the enhanced secretion of growth factors from macrophages. Moreover, there is growing evidence that the increase in membrane permeability to calcium ions after laser light exposure is of importance for the observed effects.104 Zheng and coworkers50 investigated the ability of HeNelaser irradiation to activate mouse macrophages. After exposure to different energy densities (3–47 J/cm2), the amount of lysozyme and the activity of acid phosphatase in lysosomes of peritoneal macrophages were found to be significantly higher than in nonirradiated control cultures.
Endothelial cells. Although endothelial cells play a pivotal role in wound healing because of their ability to form new capillaries (angiogenesis) and to express growth factors and chemotactic cytokines, there are hardly any data on a possible effect of low-intensity laser irradiation on these cells. Ghali and Dyson105 examined alterations in the proliferation rate of human umbilical vein endothelial cells after irradiation with HeNe and diode lasers and found both inhibition and stimulation in dependence of wavelength, dose, and time point of determination. In a study by Bouma et al29 on the influence of IR-laser exposure (904 nm, 0.3–9.0 J/cm2) on spontaneous and endotoxin-induced expression of tumor necrosis factor-a, IL-6, and IL-8 by endothelial cells, no effect of laser was noted. Again, negative results were seen in a set of experiments conducted by Colver and Priestley,28 which showed no influence of HeNe irradiation on the proliferation of endothelial cells.
Effects of Low-Intensity Laser Irradiation on Wound Healing in Animal Models
In the following, we discuss some of the most relevant publications regarding the effects of low-intensity laser irradiation on wound healing in different animal models.
Kana et al58 investigated the influence of HeNe and argon laser, as well as of noncoherent lamps emitting corresponding wavelengths, on wound healing of full-thickness wounds in rats. The intensity was kept constant at 45 mW/cm2, whereas the energy densities were varied between 4 and 20 J/cm2. Irradiation was performed once daily for 18 days. Concerning the acceleration of wound closure, a significant increase was found only with the HeNe laser between days 3 and 12. Significantly enhanced collagen production was not only found in laser-treated wounds, but also in contralateral nonirradiated wounds after argon laser exposure but not after HeNe laser exposure.
Al-Watban and his group examined the influence of a variety of irradiation protocols and other factors related to wound healing in rats.8,24,106,107 In summary, the 632-nm wavelength of the HeNe laser was most effective and energy densities of 7 and 25 J/cm2 were found to be optimal, whereas altering the intensity (3.7–15.9 mW/cm2) at a constant dose did not affect the results. Investigations of the influence of wound size and age of animals revealed that larger wounds in older animals healed faster than smaller wounds in young rats. Regarding the treatment schedule, six irradiations per week were most effective. More evidence for the efficacy of HeNe lasers in wound healing comes from a study by Strassl et al,108 who investigated healing times, fibroblast numbers, collagen content, and strength of surgical wounds in dogs after HeNelaser and placebo irradiation. No exact dosimetric data are given (output, 2 mW; spot diameter, 0.5 mm; exposure time, 2 minutes), but results showed increased numbers of fibroblasts, higher content of collagen, and faster healing in the laser-treated wounds compared with the contralateral sham-irradiated wounds.
Yu et al44 used genetically diabetic mice to compare the effect of bFGF, laser irradiation (660 nm), and a combination of growth factor and laser therapy. Their results indicated that all three treatment regimes significantly enhanced wound closure, with light therapy alone or in combination with topical application of bFGF being most effective. Zhang et al109 used a HeNe laser (dose, 0.05 J/cm2; intensity, 0.17 mW/cm2) for the irradiation of burn wounds in mice and measured serum lipid peroxide (LPO) concentrations. Initially elevated serum lipid peroxide levels were found to decrease in the laser-treated animals but remained high in nonirradiated controls. These findings seem to confirm the hypothesis of systemic effects induced by topical light exposure. Further evidence for the possibility of inducing systemic effects by light exposure comes from Braverman and coworkers.56 They found significant differences in tensile strength in both irradiated and contralateral, sham-irradiated full-thickness wounds compared with nonirradiated rabbits. This effect was observed at 632.8 nm, 904 nm, and with a combination of these two wavelengths. Epidermal growth was greater in the HeNe-laser-treated area compared with unexposed tissue, but the difference was not significant.
Extensive histopathological studies in dairy cattle were performed by Ghamsari and colleagues110,111 during and after wound healing induced by different energy densities of helium neon laser irradiation. In addition to the observed healing acceleration after laser exposure, more advanced epithelialization and epithelial differentiation, as well as a significantly higher content of hydroxyproline, was noted in biopsies from laser-treated wounds. A dose of 3.6 J/cm2 exhibited the most prominent effect. Atabey et al98 found epidermal thickening and an increase in dermal vascularity after HeNe-laser irradiation (dose, 3.8 J/cm2) of full-thickness wounds in rabbits. The acceleration in wound epithelialization in the laser-treated wounds compared with the nontreated contralateral controls observed in this study was not significant.
No effect on the acceleration of wound healing was observed by Hall et al 31 after irradiating full-thickness wounds in rats with a 904-nm laser at a dose of 0.5 J/cm2. Although intra- and interindividual controls were performed, no histological changes were found between the different groups. Hunter et al46 and Basford13 used pigs for their experiments because their tissue characteristics and dimensions are closer to those of humans. Neither reported benefits from laser therapy. Hunter et al46 created full-thickness wounds on both sides of the back of swine and irradiated them with an HeNe-laser (dose, 0.96 J/cm2; intensity, 64 mW/cm2). Measuring the percentage of wound healing over time, these investigators found no significant difference between the irradiated and nonirradiated wounds. Also in this study, intraindividual controls were used.
Using noncoherent monochromatic light at a wavelength of 890 nm (dose, 0.18–0.54 J/cm2; intensity, 13.8 mW/cm2; pulse frequency, 270 Hz), Lowe et al32 investigated the effect of low-intensity light therapy on wound healing in X-ray-exposed mice. Seventy-two hours after irradiation with 20-Gy X-ray, surgical wounds were inflicted in the irradiated area. Wound healing in the X-ray-pretreated mice was delayed compared with that of non-exposed animals between day 7 and 18 after wounding. Subsequent low-intensity laser irradiation at 0.18 and 0.54 J/cm2 did not alter the healing process. A dose of 1.45 J/cm2, however, caused a significant delay in wound healing by day 14. Because of the short time delay in wound healing resulting from X-ray exposure, the authors state that their model is not directly comparable to pathological wounds found clinically.
Effects of Low-Intensity Laser Irradiation on Wound Healing in Humans
Wound healing disturbance resulting from microangiopathies. Both short-term and long-term effects of low-dose laser irradiation on the vascular system have been reported. At the cellular level, Ghali and Dyson105 found a significant increase in the proliferation rate of endothelial cells after low-dose laser radiation, which can be regarded as a basis for the induction of long-term improvement of microcirculation. The author's group (A.S.) used an animal model to study the influence of laser irradiation on the quantity and duration of neovascularization in the bradytrophic tissue of rabbit cornea.48 After inducing an Arthus reaction, the thereby newly formed capillaries were found to be of greater length and to be perfused for a longer period in the animals receiving daily laser irradiations than those in the sham-irradiated control group. In the above-mentioned study by Kami and coworkers,92 blood flow in rat skin was measured by means of electrolytically generated hydrogen clearance after exposure to diode laser light (wavelength, 830 nm; intensity, 800 mW/cm2; dose, 20 J/cm2). Compared with nonirradiated control animals, a significantly higher blood flow was found. In another experiment using the same irradiation protocol on 2 consecutive days, the skin was dissected and microangiograms were produced 1 hour after irradiation and on the second day of irradiation. In the early phase, hypovascular areas underlying the irradiated sites could be detected, which were surrounded by zones of vasodilatation. In the late phase, no more hypovascular areas could be found and blood vessels were more numerous in the irradiated group than in the control group. The authors interpreted these findings as being laser-induced inflammatory reactions.
After a single-case study on the beneficial effect of low-intensity laser therapy on a recalcitrant diabetic neuropathic foot ulcer112 and a pilot study on the influence of laser therapy on bone affections in diabetic patients,113 we directed further research to the field of wound-healing disorders caused by diabetic complications. In a double-blinded, placebo-controlled study114 including 30 patients with diabetic microangiopathy, the author's (A.S.) group demonstrated a significant increase in skin circulation detected by means of IR-thermography, which started after 30 minutes of laser irradiation using a HeNe-laser with a dose of 30 J/cm2.
Mester et al,115 in reviewing more than 1100 cases of recalcitrant ulcers of different origin, reported a response rate of approximately 90% after low-energy laser treatment using various laser systems emitting in the red and near-IR region and applying a dose of approximately 4 J/cm2.
Venous ulcers. Publications focusing on laser therapy for chronic venous leg ulcers exhibit conflicting results. Santoianni and associates116 found no difference between the application of antiseptic compresses and low doses (1 and 4 J/cm2) of 632.8-nm laser light in a study design using intraindividual controls. In an uncontrolled setting, Kleinman achieved complete healing of recalcitrant leg ulcers in an overall 87.5% of patients treated with either 785-nm or a combination of 632.8- and 765-nm laser light. In two of these patients, recurrence occurred within a period of 2 years.117
Wound healing disturbance resulting from ionizing radiation or chemotherapy. Although a protective effect of low-intensity laser irradiation against cell damage resulting from α- and X-radiation under in vitro conditions has already been described more than a decade ago,23,118,119 the influence of light on the healing of chemo- or radiotherapy-induced skin damage was investigated only recently.120–122 The author's group (A.S.) described two cases, in which long-term ulcers resulting from skin damage after radiotherapy could be healed completely by low-intensity HeNe-laser radiation. In one case,123 the ulcer on the patient's sole had persisted for more than 40 years, whereas in the second case,124 the patient's wound healing capacity had been additionally reduced by the coexistence of systemic lupus erythematosus and diabetes mellitus. A subsequently performed pilot study for the evaluation of the efficacy and safety of laser therapy in patients with chronic radiation ulcers after breast cancer showed complete closure of the ulcers with no recurrence of either the ulcers or the tumor during a follow-up of up to 24 months.125 This is in accordance with the findings of Dyson's group, who demonstrated the beneficial effects and safety of diode lasers in malignant ulcers.126
Burn wounds. Although treatment of epithelial defects resulting from burn injury could possibly profit from low-intensity laser therapy, there is only one report on this topic in the literature. Rochkind induced burn injury bilaterally in rats by means of hot water. Daily irradiations of one side with an HeNe laser (dose, 10 J/cm2) for 21 consecutive days resulted in complete re-epithelialization in the irradiated side and faster healing in the nonirradiated side compared with a control group of animals. This healing pattern has been interpreted as being a result of the induction of a systemic effect by topical light exposure.47
Meta-Analyses on Wound Healing
During the first consensus conference on low-intensity laser therapy hosted by the Food and Drug Administration in October 1999, two yet unpublished meta-analyses on low-intensity laser therapy in human subjects were presented. Brannon and colleagues had analyzed 24 clinical studies (case reports and insufficiently documented trials were excluded), of which 31 effect sizes could be defined. An overall therapeutic effect of +2.2±2.8 (SD) was calculated. Despite the large SD, this effect was found to be significant, because the fail-safe number was calculated to be 509 (ie, 509 additional studies with no benefit or negative outcome would be necessary to overrule the laser-induced therapeutic effect). Similar results were reported by Parker et al, who included nine clinical studies, finding an overall therapeutic effect size of +1.1±1.0 (SD) and a fail-safe number of 41. A subanalysis on the applied wavelengths showed effect sizes of +1.6 for 830 nm and +0.5 for 904 nm.
Low-Intensity Laser Therapy in other Medical Fields
In traumatology and orthopedics, there is evidence for the usefulness of low-intensity laser therapy from studies dealing with bone fracture healing and mineralization. Most experiments used either experimental bone fractures or other experimentally-induced bone lesions with subsequent transcutaneous irradiation127–131 or irradiation of osteoblastic cell lines.132,133 The only publication on clinical effects of low-intensity laser therapy on bone healing describes enhanced mineralization in diabetic patients with bone fractures who were irradiated primarily because of gangrenes.113 The observed effects in experimental trials include faster healing after fractures, improvement of bone metabolism, higher calcium content and accumulation, increase in alkaline phosphatase activity, and enlargement of Golgi apparatus in irradiated bone cells.
Neurology
Rochkind et al47 showed increased compound action potentials and reduced retrograde degeneration of motor neurons of the spinal cord in crushed, injured sciatic rat nerves, and Schwartz et al134 reported on improvement of posttraumatic degeneration of the optic nerve in rabbits after exposure to HeNe-laser. Using a model for transient brain ischemia by transient exposure of hippocampal brain slices to a perfusion medium lacking oxygen and containing reduced glucose concentrations, Iwase and colleagues135 found prolongation of time required for the loss of electrical excitability and improvement of recovery for ischemic injury by low-intensity laser irradiations. Other studies revealed analgesic effects of low-intensity laser therapy.75,77,90 Lowe et al136 investigated the influence of 830-nm laser irradiations on skin temperature and antidromic conduction latencies in human median nerves. Results showed a decrease in skin temperature and an increase in negative peak latencies at a dose of 1.5 J/cm2.
Immunological Aspects and Possible Future Indications of Low-Intensity Laser Irradiations
Recently, increasing research activity has been directed toward the elucidation of possible immunological effects of low-intensity laser therapy. Agaiby et al136a used a 820-nm diode laser to investigate the role of laser light on lymphocyte proliferation. At a pulsing frequency of 5 kHz and doses of 1.2 and 3.6 J/cm2, significantly enhanced proliferation was noted, whereas higher doses were inhibitory. When phytohemagglutinin was added, all doses were inhibitory.136 The 904-nm wavelength of a gallium arsenide laser was found to induce both inhibition and stimulation of lymphocyte proliferation in the presence of phytohemagglutinin in a dose-dependent manner.137 Similar results were reported by Ohta et al.138 Manteifel et al139 observed a significant decrease of mitochondria and formation of giant mitochondria upon irradiation (0.0056 J/cm2 and 0.56 mW/cm2) of lymphocytes with an HeNe laser.
In an animal model for sepsis (cecal ligation and puncture), Yu found elevated ex vivo lymphocyte proliferation and higher survival rates on intraperitoneal irradiation with a 630-nm laser (20 mW/cm2, 5 J/cm2). Irradiation of lymphocytes in vitro at 2.4 and 4.8 J/cm2 induced lymphocyte proliferation and enhanced ATP synthesis.140 In a similar animal model, elevated numbers of lymphocytes were noted 20 hours after transcutaneous irradiation at 632.8 and 660 nm.49
After irradiation with an 830-nm diode laser, a suppressive effect on contact sensitivity was reported by Katsuyama et al.141 This effect was found to be limited to the site of irradiation, with no systemic effect being inducible.141 In contrast, Inoue et al142 observed a systemic inhibitory effect on delayed hypersensitivity reactions in guinea pigs.
As mast cells not only are involved in the early phases of wound healing but also in inflammatory responses of the skin, the possible effect of low-intensity laser irradiation on their total number and degree of degranulation was investigated. El Sayed and Dyson143 used a cluster of laser diodes of different wavelengths (660–950 nm; intensity, 45 mW/cm2; dose, 10.8 J/cm2) and single diodes of the respective wavelengths (intensity, 120 mW/cm2; dose, 10.8 J/cm2) for the irradiation of intact and wounded rat skin. In all irradiation protocols except for the 870- and 880-nm diodes, a significant increase in the total number of mast cells was noted in both intact and wounded skin. The degree of degranulation, however, was only increased in wounded skin after irradiation with both the cluster and the respective single diodes. On the contrary, Trelles et al144 found a significant reduction in mast cell count and histamine content of rat tongue tissue upon irradiation with an HeNe laser (632.8 nm). The intensities and dose used, however, were much lower than in the protocol of El Sayed and Dyson (4 and 15 mW/cm2, and 2.4 J/cm2, respectively).
Ulcerative and bullous skin diseases, such as mucosal Lichen ruber, graft-versus-host disease, systemic sclerosis, necrobiosis lipoidica, pemphigus vulgaris, bullous pemphigoid, and pyoderma gangrenosum might represent additional future indications for low-intensity laser therapy. Furthermore, it was only recently that therapeutic effects of low-intensity laser therapy were described in the field of dentistry.145,146
Conclusion
Research in the field of low-intensity laser therapy has occasionally been lacking accuracy in reporting exact irradiation protocols and establishing appropriate controls in the past. Moreover, the variety of laser systems and experimental conditions used makes comparison of results difficult. However, summarizing the data of the existing controlled in vitro and in vivo studies that address the biological effects of low-intensity (laser-) light irradiation, we conclude that this type of phototherapy should be considered a valuable (adjuvant) therapy for selected therapy-refractory conditions such as the impairment of wound healing. Further research on additional possible indications seems to be justified.
Perspectives
The possible future role of low-intensity laser therapy in medicine in a world of growing life expectancy might be that of an adjuvant treatment aiming at reducing costs and raising patients’ quality of life. One simple example should illustrate the potential meaning of low-intensity laser therapy. According to estimations of the World Health Organization, the number of patients suffering from diabetes mellitus will double by the year 2050 to 250 million. Diabetic patients have a 22-fold higher risk for nontraumatic foot amputation compared with the nondiabetic population.147 The overall costs for foot amputation, including costs induced by subsequent invalidity, were estimated to be approximately $1 million (US) per patient.148,149 Despite a long-term program aiming at reducing the rate of diabetic late complications expressed in the St Vincent Declaration of the World Health Organization, even an increase in foot amputations has been noted recently.150 In light of these data, any measure that could possibly lower the rate of limb loss (such as low-intensity laser therapy) should be considered worthwhile. However, large well-controlled studies are needed to prove or disprove such speculations and will require multidisciplinary collaborations.