
Abstract
Background
Preclinical research suggests that interleukin-10 (IL-10) is associated with susceptibility to and severity of systemic lupus erythematosus. Chronic cutaneous lupus erythematosus is thought to be immunogenetically different from systemic lupus erythematosus. We hypothesized that high innate production of IL-10 underlies systemic but not chronic cutaneous lupus erythematosus.
Methods
IL-10 production was determined after endotoxin stimulation of whole-blood samples. In whole-blood samples, disease activity and medication influence the IL-10 production in patients. Therefore, healthy first-degree relatives of patients were evaluated. One hundred sixty-six first-degree relatives of patients with systemic lupus, 50 first-degree relatives of patients with chronic cutaneous lupus, and 133 control persons were studied. Innate IL-10 production of the patient was estimated as the mean IL-10 production of the unaffected relatives. Polymorphisms located −1082, −819, and −592 base pairs relative to the IL-10 gene were typed by allele-specific oligohybridization of polymerase chain reaction-amplified DNA fragments.
Results
IL-10 production was higher in the families of patients with systemic lupus than in the control families (1517±94 vs 1180±59 pg/mL; P=0.003). IL-10 production in the families of patients with chronic cutaneous lupus was similar to that in control families (1216±82 vs 1180±59 pg/ml; P=0.74). IL-10 production was also similar in families of patients with severe compared with nonsevere systemic lupus (P=1.0). The frequency of −1082/–819/–592 haplotypes GCC, ACC, and ATA was similar among patients and compared with the control persons (P=0.29).
Conclusions
High innate IL-10 production underlies susceptibility for systemic lupus erythematosus but not the severity of the disease. It is not related to chronic cutaneous lupus erythematosus.
Introduction
Production of interleukin-10 (IL-10) plays an important role in the pathogenesis of systemic lupus erythematosus (SLE), a chronic autoimmune disease that is characterized by increased production of autoantibodies. In vitro experiments have established the stimulating properties of IL-10 on B-cell function.1 In line with these experiments, autoantibody production could be abrogated by addition of anti-IL-10 blocking antibodies.2 Mice that are prone to SLE also show a high endogenous production of IL-10. Moreover, these mice show a less severe disease course after administration of anti-IL-10 antibodies.3 The relation between systemic expression of these cytokines and the localized variant, chronic cutaneous lupus erythematosus (CCLE), is yet unknown. The disease has been described as a subset of SLE with essentially similar pathogenesis.4 Alternatively, CCLE is considered an entity with different immunogenetic features from generalized SLE.5–7
Twin studies have shown that susceptibility to SLE is largely genetically determined.8 Not only susceptibility to SLE, but also severity of SLE (end-stage renal disease) clusters in families.9 The candidate genes that are identified encompass the genes encoding IL-10 and Fc receptors and are located on the long arm of chromosome 1.10–13 Earlier we have shown that production of IL-10 in a whole-blood stimulation assay varies widely between individuals.14 This variation in IL-10 production seems to be largely under genetic control and was associated with outcome of infectious disease.15 By use of an unstimulated assay, it was found that innate production of IL-10 is higher in families in which several patients have developed SLE.16
We hypothesize that innate production of IL-10 is associated with susceptibility to SLE but not CCLE. Production of IL-10 was assessed by a whole-blood stimulation assay in first-degree relatives of the patient to avoid influence of medication and disease activity on cytokine production. Partners with their first-degree relatives served as controls. First-degree relatives of patients with CCLE were studied as a second control group. To examine whether innate production of IL-10 is associated with severity of SLE, the production of IL-10 was determined separately in first-degree relatives of patients with clinically severe and clinically nonsevere SLE.
Methods
Design
Cytokine production ex vivo is a heritable characteristic. In patients, however, cytokine production may be influenced by active disease and medication. Therefore, first-degree relatives were studied. This means that in this study the family, not the patient, was the unit of observation.
Study Persons
After approval by the institutional medical ethics board, patients with at least four American College of Rheumatology (ACR) criteria for SLE17 were identified from the institutional diagnosis registration. Patients were classified as having severe SLE when they had been treated with cyclophosphamide at any time since diagnosis for multiorgan involvement (neuropsychiatric involvement and/or nephritis). Patients were classified as having nonsevere SLE when they had never been treated with cyclophosphamide and were at least 10 years free of multiorgan disease. Central nervous system involvement was diagnosed by physician-confirmed presence of magnetic resonance imaging scan abnormalities, cognitive deterioration, as confirmed by a neuropsychological examination, epileptic seizures, depression, or psychosis. Nephritis consisted of histopathologically confirmed glomerulonephritis and/or proteinuria of at least 0.5 g/24 h during at least 1 month. Accumulated organ damage was measured by the Systemic Lupus International Collaborating Clinics /ACR Damage Index (0- to 46-point scale).18 Current disease activity was scored using the SLE Disease Activity Index.19 Patients who could be classified according to the criteria mentioned above were interviewed for eligibility, and their first-degree relatives (parents, brothers and sisters, and/or children) were also invited. After being interviewed, 53 patients with 173 first-degree relatives free of disease were enrolled in the study. Three first-degree relatives of patients had SLE or cutaneous LE themselves. These were not included in the study.
Records of patients registered as having chronic discoid lupus erythematosus in the period from 1979 through 1989 were checked to confirm the clinical and histopathological diagnosis. All had been observed for a period of at least 10 years to exclude the possibility that generalized disease had developed. Twenty-one patients with CCLE agreed to participate, with 51 of their first-degree relatives using a procedure similar to that used by the SLE families. The clinical diagnosis was confirmed at the interview in all cases. One of these patients had been treated in the past year with dapsone and azathioprine because of therapy-resistant skin complaints.
If the patients agreed, spouses and their first-degree relatives were invited to participate as control persons. Fifty-six spouses and 84 of their first-degree relatives were enrolled in a similar procedure, yielding 140 control persons for sampling.
Whole-Blood Stimulation System
Stimulation of whole-blood samples was performed as described previously.14 Briefly, blood samples were taken between 8 and 11 AM to minimize the influence of circadian rhythms. Blood was collected in pyrogen-free heparinized tubes (Endotube®, Chromogenix, Mölndal, Sweden). Eight-milliliter whole-blood samples were diluted 1:1 with RPMI 1640 (Gibco Life Technologies, Paisley, United Kingdom) and stimulated with 10 ng/mL Escherichia coli lipopolysaccharide (Difco Laboratories, Detroit, Mich), within 60 to 75 minutes after blood sampling. One:1 medium-diluted blood without lipopolysaccharide was used as negative control. After 4-hour (tumor necrosis factor [TNF]) and 24-hour (IL-10) incubation, samples were centrifuged twice (600g) and the supernatants stored at −70°C. TNF and IL-10 production was measured by enzyme-linked immunoadsorbent assay (Central Laboratory of the Blood Transfusion Service, Amsterdam, the Netherlands) in supernatants. The limit of detection was 4 pg/mL, the intra-enzyme-linked immunoadsorbent assay coefficient of variation was 4 to 8%, and the day-to-day variations were 8.1% (TNF) and 10% (IL-10). Because of technical errors or non-negative cytokine production on incubation with medium only (IL-10>100 pg/mL or TNF>100 pg/mL), 15 samples (seven relatives of patients with SLE, one relative of a patient with CCLE, and seven controls) were excluded from analysis. Comparison of unstimulated cytokine production between the groups revealed no significant differences (P>0.5).
Polymorphism Genotyping
The genotyping of the single nucleotide polymorphisms was described previously.20 Briefly, DNA was isolated from peripheral-blood cells by phenol-chloroform extraction. Fragments of the IL-10 promoter were amplified using the primer combination ATC.CTC.GAG.CCT.TCT.TTT.GCA.AGT.CTG.T13 and GAC.GGT.ACC.CTG.ACT.ATA.GAG.TGG.CAG-1413. Polymerase chain reaction fragments were subsequently dot blotted on Hybond N+ membranes and hybridized according to described methods.21 Sequences of the oligonucleotides and washing temperatures were as follows: for −1082A: ACT.TCC.CCT.TCC.CAA.AGA.A, 52°C; for −1082G: TTC.TTT.GGG.AGG.GGG.AAG, 51°C; for −819C: CAG.GTG.ATG.TAA.CAT.CTC.TGT.GC, 62°C; for −819T: GCA.CAG.AGA.TAT.TAC.ATC.ACC.ACG.TGT, 63°C; for-592C: CCG.CCT.GTC.CTG.TAG.GAA, 50°C; and for −592A: TTC.CTA.CAG.TAC.AGG.CGG.G, 52°C.
Statistical Analysis
Innate production of IL-10 by the patient was estimated by the mean family production of IL-10 of two to six healthy relatives. The cytokine production of the patient was not included. For control persons, the estimate was determined by calculating the mean cytokine production of each separate control family, including the partner. Family means were grouped according to the disease status of the proband (SLE, CCLE, and controls), and group means were then tested with analysis of variance to detect any significant difference of the group means from the overall mean. If any significant differences were detected, unpaired t tests between the groups were performed. In a second analysis, we directly compared all first-degree relatives of patients with all control persons. Genotype distributions were compared between groups with the χ2 test.
Results
Demographic and Clinical Characteristics
The first-degree relatives of patients with SLE were similar to the first-degree relatives of the patients with CCLE and to the control persons with respect to age, sex, and family size (Table 1). In the patients, the ratio of females to males was different from that in the spouses. These characteristics were also similar for the first-degree relatives of patients with severe SLE compared with the first-degree relatives of the patients with nonsevere SLE. There was a higher proportion of non-Caucasians among the SLE relatives, particularly among the relatives of patients with severe SLE.
As expected from the group definitions, the ACR Damage Index scores and the prevalence of neuropsychiatric manifestations and nephritis was higher in the severe group. Seventeen patients with severe SLE (65%) had either central nervous system or renal involvement, and nine with severe SLE (35%) had both. Six patients (22%) with nonsevere SLE had either central nervous system or renal involvement, and 20 (78%) with nonsevere SLE had neither. Disease duration was longer in the nonsevere and CCLE groups. There were no substantial differences in the prevalence of malar rash, arthritis, pleuropericarditis, or arthritis between the patients with severe SLE and those with nonsevere SLE.
IL-10 Production in Relation to Disease Susceptibility and Severity
The family estimates of the IL-10 production for patients with severe SLE, those with nonsevere SLE, those with CCLE, and controls were significantly different (P=0.013) (Table 2). The production of TNF in these groups was similar. Groupwise testing subsequently revealed a significantly higher production of IL-10 in families of patients with nonsevere SLE and families of patients with severe SLE than in control families (P=0.012 and P=0.006, respectively). The production of IL-10 in the families of patients with nonsevere SLE was not significantly different from that in the families of patients with severe SLE (P=1.0). Moreover the production of IL-10 in the families of patients with severe and nonsevere SLE was not correlated with ACR Damage Index scores (data not shown).
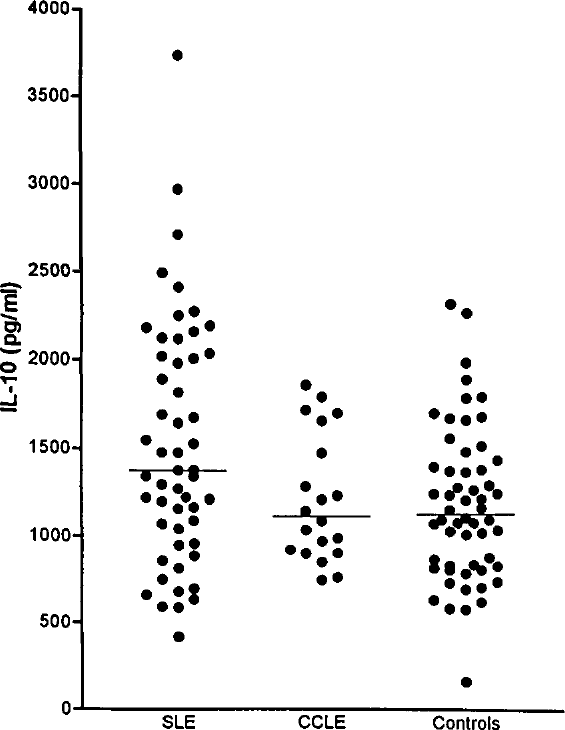
To examine the innate production of IL-10 in relation to susceptibility for SLE, the families of patients with nonsevere SLE and the families of patients with severe SLE were combined (Figure). The mean production of IL-10 in the SLE families was 30% higher than that in the control families (P=0.003). In contrast, the IL-10 production in CCLE families was similar to that in control families (P=0.74). In a second analysis, high IL-10 production in families of patients with SLE was also present when the first-degree relatives were analyzed as individuals and not grouped per family. IL-10 production in the 80 relatives of patients with SLE was 1509±65 versus 1182±46 in 133 control persons (P<0.001). IL-10 production in the 50 relatives of patients with CCLE was 1186±69 pg/mL and not different from that of control persons (P=0.96). Production of IL-10 was not correlated with age (P=0.2; age range, 8–85 years) and gender (males: production of IL-10=1367±60 pg/mL; females: 1314±48 pg/mL; P=0.49).
Demographic and clinical characteristics of families of patients with SLE and CCLE and control families.

Plus-minus values are mean±SE.
Accumulated organ damage was measured by the Systemic Lupus International Collaborating Clinics/ACR Damage Index.
Disease activity at time of blood sampling was measured by the SLE Disease Activity Index.
Production of IL-10 and TNF in families of patients with SLE and CCLE and control families.
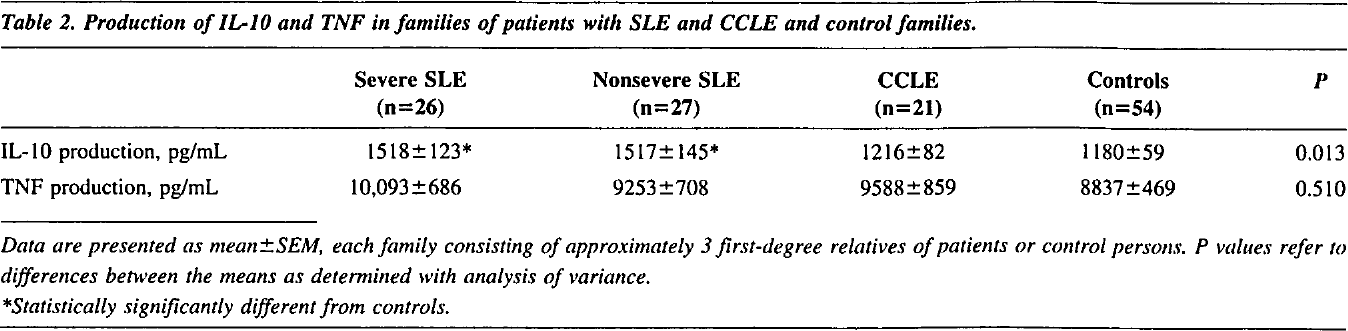
Data are presented as mean±SEM, each family consisting of approximately 3 first-degree relatives of patients or control persons. P values refer to differences between the means as determined with analysis of variance.
Statistically significantly different from controls.
Production of IL-10 in families of patients with SLE, families of patients with CCLE, and control families. Each dot represents the mean of the endotoxin-induced IL-10 production of approximately 3 first-degree relatives of that family. The horizontal lines represent the mean IL-10 production of the family means for each group.
To control for population admixture, the analysis was then limited to Caucasian families only (44 SLE families, 21 CCLE families, and 51 control families). Production of IL-10 in the families of patients with severe SLE (1575±156 pg/mL) and families of patients with nonsevere SLE (1549±147 pg/mL) was higher than that in the control families (1197±61 pg/mL; P=0.008 and P=0.011, respectively).
Patients Only
Production of IL-10 was lower among patients with SLE than in their first-degree relatives (1030±114 vs 1517±94 pg/mL; P<0.001). Of all patients with SLE, 30 (56%) had used cyclophosphamide, azathioprine, and/or corticosteroids in the 6 months before blood sampling. The production of IL-10 in patients on these drugs was significantly lower than that in those without drug treatment (763±116 vs 1362±214 pg/mL; P=0.014). In the 19 patients with nonsevere SLE who did not use immunosuppressive medication, the production of IL-10 was 1531±261 pg/mL. Production of IL-10 in patients with localized CCLE was not statistically significantly higher than that in controls (1399±110 vs 1182±46 pg/mL; P=0.09).
IL-10 Promoter Gene Polymorphisms
To test a possible explanation for the increased innate production of IL-10 in patients with SLE, single nucleotide polymorphisms in the promoter of the gene encoding IL-10 were investigated in patients. These single nucleotide polymorphisms combine to form three exclusive haplotypes in the IL-10 promoter, namely, ACC, GCC, and ΑΤΑ (−1082, −819, −592).20 The frequency of three polymorphisms at 1082, −819, and −592 base pairs from the IL-10 transcription initiation site was analyzed in Caucasian patients and Caucasian controls only. There was no statistically significant over-representation of alleles of the 1082 or −819/–592 polymorphism in the patients with SLE compared with controls (−1082 A vs G: X12=0.64, P=0.43; −819/–592 C/C vs T/A: x12=0.86, P=0.35) (Table 3). These allele frequencies were similar in patients with severe SLE compared with those with nonsevere SLE (−1082 A vs G in severe SLE vs controls: X12=0.96, P=0.33; nonsevere SLE VS controls: X12=0.093, P=0.76). Likewise, the frequency of −819 T versus C in patients with severe SLE was not significantly different from that in controls (χ12=0.84; P=0.36), as was the case in the patients with nonsevere SLE versus controls (χ12=0.28; P=0.60). When these single nucleotide polymorphisms were combined into haplotypes, no significant allelic imbalance was observed in the SLE patients compared with external controls (χ22=2.4; P=0.31).
Discussion
This study shows that the endotoxin-induced IL-10 production in whole-blood samples in families of patients with SLE is increased when compared with that of control families. No increased production of IL-10 was found in families of patients with CCLE. The findings indicate that high innate production of IL-10 contributes to the susceptibility of SLE but not CCLE. No relation was found between innate IL-10 production and the severity of SLE. The present data are in line with data on constitutive production of IL-10 using unstimulated peripheral-blood mononuclear cells from Mexican multicase SLE families.16
We used an endotoxin-stimulated whole-blood assay, because measuring cytokine production on a standard stimulus allows an estimation of an individual's inherent capacity to produce an inflammatory response. This inflammatory response is in part under genetic control.15 The inflammatory response of healthy first-degree relatives was therefore measured and grouped into family means to provide the best estimate of the innate IL-10 production of the patient. The assay is capable of discriminating high producers from low producers.14 Moreover, the clinical relevance of endotoxin-stimulated whole-blood samples has been demonstrated in earlier studies on infectious diseases.15 Another technical issue is that unstimulated production of cytokines by healthy individuals was low or undetectable.22 This has repeatedly been reported by other investigators.23–26
IL-10 promoter polymorphism allele and haplotype frequencies in patients with SLE and patients with CCLE and control persons.
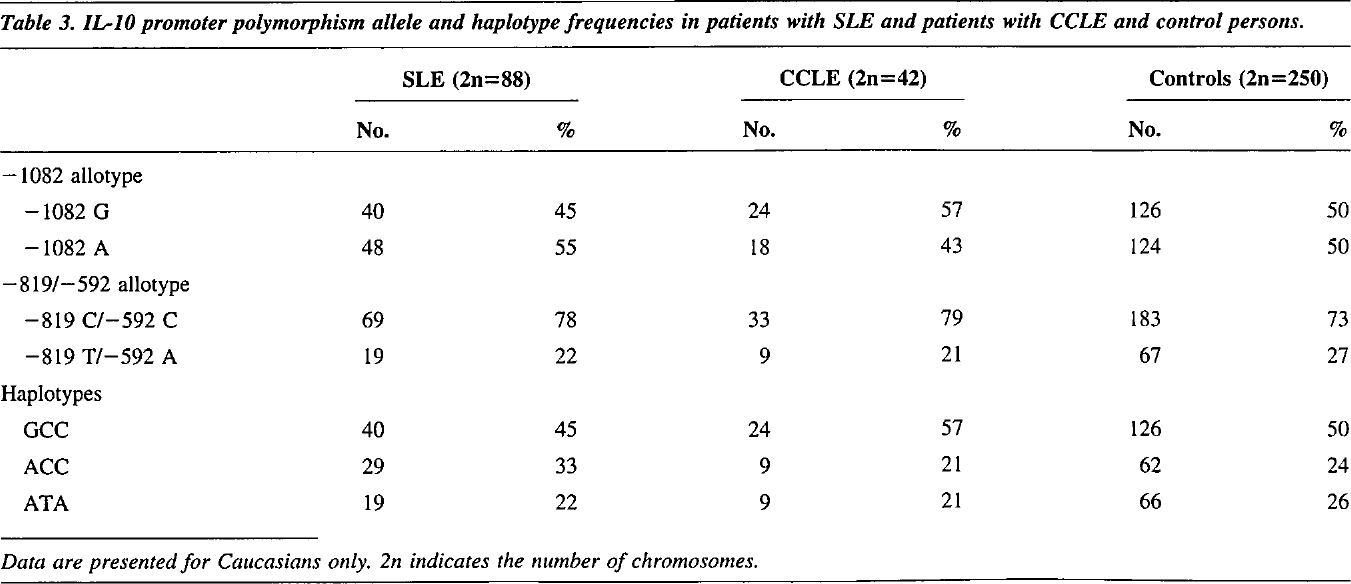
Data are presented for Caucasians only. 2n indicates the number of chromosomes.
Whole-blood cultures in patients may be affected by medication and active disease, which precludes causal inference on functional immunological tests and susceptibility of disease.27,28 A similar reasoning holds when measuring levels of IL-10 during the disease course. High and low circulating levels of IL-10 may be a reflection of activity of the disease.29 In the current study, production of IL-10 was indeed lower in the patients than in their first-degree relatives, especially in those patients who used cytostatic drugs and corticosteroids.
Of all living family members of the patients, a random fraction participated in the study. There is a possibility that family members with a latent genetic predisposition to autoimmune disease died before the time of inclusion. This may have biased the results on cytokine production in the remaining relatives. However, the mean survival time of first-degree relatives of patients with SLE, if anything, was longer rather than shorter than that of the general population, which makes this possibility unlikely.30
Despite recent insights that severity of SLE might be related to an underlying innate cytokine production profile,31 families of patients with severe SLE were not characterized by a detectable increase in production of IL-10. This may be a result of a lack of statistical power, because a difference resulting from disease severity might be smaller than a difference resulting from disease susceptibility.
An alternative explanation for the increased production of IL-10 in families of patients with SLE might be aspecific immunoactivation in vivo. To study this possibility, the production of TNF was also determined. The production of TNF was similar between the families of patients with SLE and control families, virtually excluding the possibility that the difference in production of IL-10 is explained by aspecific immunoactivation. The present data cannot be explained on the basis of a putative association of TNF production with HLA-DR3, a known genetic risk factor for SLE.32 Despite equal production of TNF, an increased frequency of HLA-DR3 was present in the SLE patients under study (53% of SLE patients vs 23% of controls were DR3 carriers).33
If CCLE, characterized by a sustained absence of generalized disease, is regarded as a mild subset of SLE, then an elevated IL-10 production in CCLE families compared with control families is expected. However, no statistically significantly increased production of IL-10 was observed in these relatives of patients with CCLE. Therefore, these results support the view that CCLE may be considered as a disease that is immunogenetically different from generalized SLE. Innate production of IL-10 is probably only involved in an excessive immune response that characterizes generalized SLE.
Differences in innate IL-10 production in patients may be explained by structural differences in the IL-10 promoter. Three single nucleotide polymorphisms have been identified at positions −1082, −819, and −592 base pairs from the transcription initiation site, forming three haplotypes in Caucasians: ACC, GCC and ATA (−1082, −819, −592).34 The immediate vicinity of these polymorphisms to the transcription initiation site and suggestions for a relation between these haplotypes and in vivo endotoxin-induced IL-10 production provided the rationale for studying these haplotypes. An association between IL-10 production and these polymorphisms was suggested by two groups, though with conflicting results.34,35 Associations between IL-10 promoter single nucleotide polymorphisms and SLE have only been reported with regard to specific disease subsets, ie, renal involvement in Chinese patients with SLE36 or cerebral involvement in Caucasian patients.20 No increased frequency of the haplotype ATA in patients with SLE was observed in the present study. Genetic factors possibly causing differences in IL-10 production may include polymorphisms further downstream in the IL-10 promoter. Haplotypes of the IL-10 promoter as defined by a combination of two variable-length CA repeats, located 1.1 and 4.0 kilobases downstream in the 5’ flanking region of the IL-10 gene, were associated with endotoxin-induced production levels of IL-10 and with SLE.37,38 Thus, the structural basis for differences in IL-10 production may be in these polymorphic elements on chromosome 1q. Alternatively, the structural basis for differences in IL-10 production may be in polymorphisms in transcription factors with variable expression or binding affinity for the IL-10 promoter.
Because the structural basis of innate IL-10 production is as yet unknown, the best estimate of the innate IL-10 production is measured with a functional assay. Using a whole-blood stimulation assay in a large number of first-degree relatives of patients with SLE and CCLE as well as controls, the innate IL-10 production was identified as a susceptibility factor for SLE but not for CCLE. Future studies may reveal the underlying genetics of this trait of enhanced innate IL-10 production.
Footnotes
Acknowledgments
V. Keijsers (Rheumatology), T. Tong Tan Quoc (Rheumatology), M. van Schie (Clinical Chemistry), and M. van Kersbergen (Clinical Chemistry) are each gratefully acknowledged for their contribution in laboratory work. J.P. Vandenbroucke (Clinical Epidemiology) and F.C. Breedveld (Rheumatology) are acknowledged for their critical revision of the article.