
Abstract
The aim of our study was to evaluate oxidative stress and thiol–disulfide homeostasis in term newborns receiving phototherapy. The study was planned as a single-blind, intervention study in a single center with level 3 neonatal intensive care unit to investigate the effect of phototherapy on the oxidative system in term newborns with hyperbilirubinemia. Neonates with hyperbilirubinemia were treated with total body exposure phototherapy technique for 18 h using a Novos® device. Blood samples of 28 term newborns were taken before and after phototherapy. Total and native thiol, total antioxidant status (TAS) and total oxidant status (TOS), and oxidative stress index (OSI) levels were measured. The 28 newborn patients included 15 (54%) males and 13 (46%) females with a mean birthweight of 3080.1 ± 366.5 g. Native and total thiol levels were found to be decreased in patients receiving phototherapy (p = 0.021, p = 0.010). Besides, significantly lower TAS and TOS levels were found after phototherapy (p < 0.001, p < 0.001). We found that decreased thiol levels were related to increased oxidative stress. We also determined significantly the lower bilirubin levels after phototherapy (p < 0.001). In conclusion, we found that phototherapy treatment induced decreased oxidative stress associated with hyperbilirubinemia in neonates. Thiol–disulfide homeostasis can be used as a marker of oxidative stress due to hyperbilirubinemia in the early period.
Bilirubin plays a role in the balance between antioxidant and pro-oxidant agents in newborns.
Increased indirect bilirubin levels increase oxidative damage by increasing oxidative stress and lipid peroxidation, especially in the central nervous system.
Studies on thiol–disulfide balance, a new marker of the oxidative system, in newborns are very limited.
Native, total thiol, and disulfide levels, indicators of oxidative stress, were lower in patients receiving phototherapy.
Despite the decreased antioxidant effect of bilirubin and the oxidative effect of phototherapy, total oxidative stress index decreased after treatment.
These results support that the thiol–disulfide homeostasis can be used as a marker of oxidative stress in patients with hyperbilirubinemia in the early period.
Early detection of thiol–disulfide levels in newborns with hyperbilirubinemia will play an important role in the administration of appropriate treatment.
Introduction
Phototherapy used in the treatment of indirect hyperbilirubinemia in newborns increases photodynamic stress and lipid peroxidation, can cause oxidative damage, and contributes to the development of bronchopulmonary dysplasia, retinopathy of prematurity, necrotizing enterocolitis, and patent ductus arteriosus in very low birthweight newborns. 1 Development of the antioxidant system in newborns continues with growth, and bilirubin acts as a physiological barrier against oxidant molecules in cell destruction. Therefore, some studies have mentioned the pro-oxidant effect of bilirubin, 2 while others 3 have mentioned the antioxidant effect of bilirubin. Results from different studies show that the relationship between hyperbilirubinemia and oxidative stress is complicated.
Oxidative stress occurs as a result of overproduction of free radicals and deficiency in the antioxidant system. Thiols are compounds containing sulfhydryl groups (–SH) and are known to play an important role in preventing oxidative stress in cells. Thiols are exposed to oxidation reactions and form disulfide structures. The disulfide bonds formed can be reduced back to thiol groups, thus providing a dynamic thiol–disulfide balance. This balance has a vital role in antioxidant protection, detoxification, signal transduction, regulation of enzymatic activities, and cellular signaling mechanisms. 4
As one of the new indicator markers of the oxidative system, thiol–disulfide balance is widely used in adult diseases, and new studies are being carried out in children. The vast majority of thiols in plasma are protein-like albumin and can provide an important information in early diagnosis and biochemical progression of diseases. 5
In our study, we aimed to compare the thiol–disulfide balance before and after phototherapy in term newborns with hyperbilirubinemia and to emphasize the importance of thiol measurement, which is a new parameter in determining the effect of phototherapy on oxidative stress.
Materials and methods
Study design
The study was planned as a single-blind, intervention study in a single center with level 3 neonatal intensive care unit in Aksaray province of Turkey to investigate the effect of phototherapy on the oxidative system in term newborns with hyperbilirubinemia.
Study population
A total of 28 newborns, 15 males and 13 females, were included in the study from 54 neonatal patients who were admitted to the neonatal intensive care unit with the diagnosis of indirect hyperbilirubinemia and were treated with phototherapy between January and April 2021. The inclusion and exclusion criteria and the implementation of the study are shown in Figure 1 in detail. The neonates with hyperbilirubinemia were treated with total body exposure phototherapy technique for 18 h using Novos® device. Phototherapy was applied from a distance of 35–40 cm with a light intensity of 120 µW/cm2/nm and a wavelength of 420–480 nm, consisting of 16 blue light-emitting diode tubes. During the phototherapy, the vital follow-ups of the babies were closely monitored. Phototherapy treatment was continued except for the mother to breastfeed the baby.
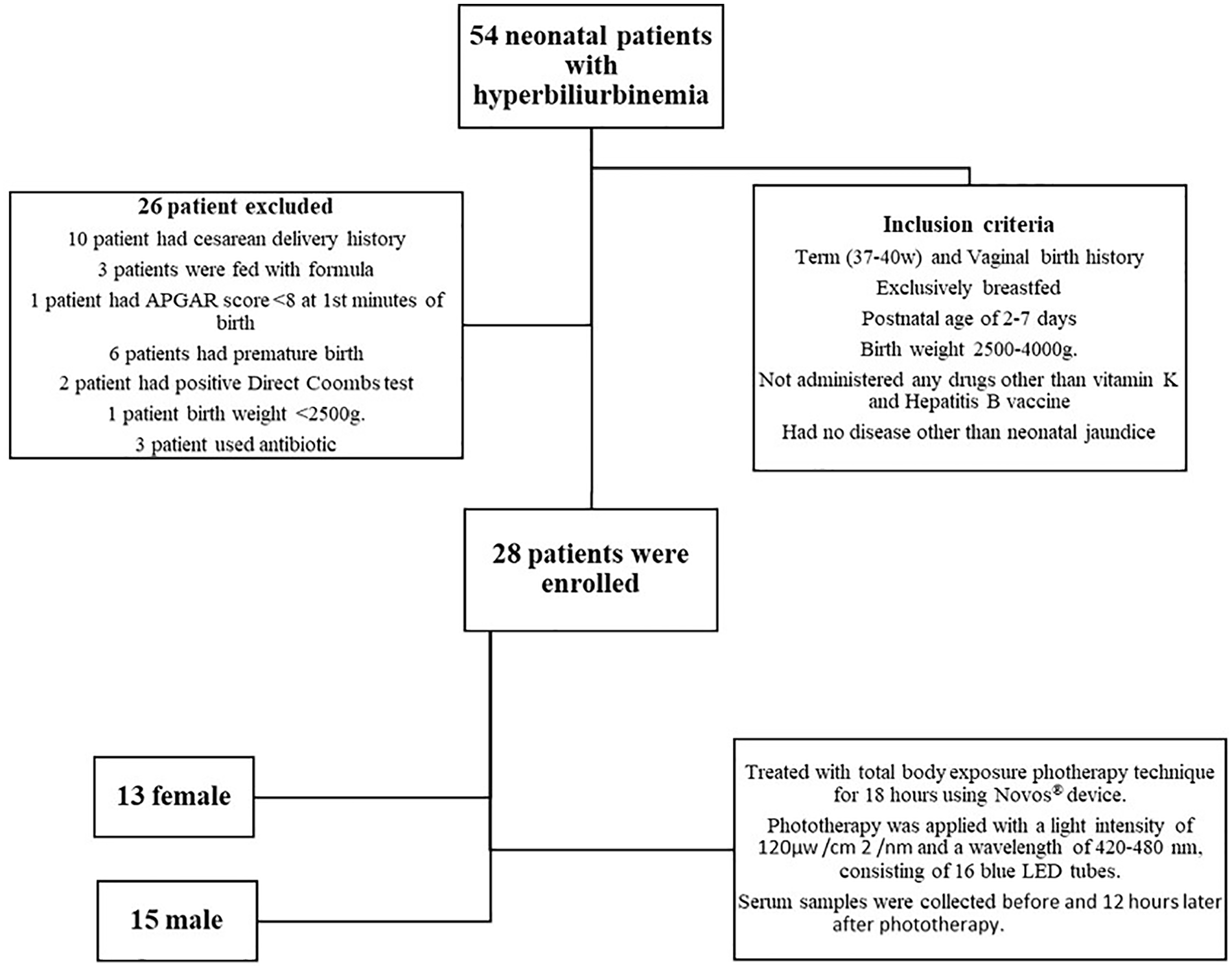
Enrollment of participants, and inclusion of data set analysis.
Data collection
Serum samples were collected in vacutainer tubes containing ethylenediaminetetraacetic acid before and 12 h later after phototherapy treatment, and routine blood samples were taken for the measurement of bilirubin values and were centrifuged at 1500g × 10 min after sampling. Then, serum samples were portioned and stored at −80°C in the Eppendorf tube until the time of assay.
Measurement of thiol–disulfide homeostasis
In this study, total antioxidant status (TAS) 6 and total oxidant status (TOS) levels were measured spectrophotometrically with the method developed by Erel. 7 Native and total thiol levels were measured with a new spectrophotometric method developed by Erel and Neselioglu. 4 Disulfide levels and disulfide/native thiol, disulfide/total thiol, and native/total thiol percentages were calculated with the following formulas: disulfide levels (µmol/L) = (total thiol – native thiol)/2 and disulfide/native thiol percentage (%) = (disulfide × 100)/native thiol).
Serum samples were labeled by the technician in the biochemistry laboratory according to the names of the patients. The blinded researcher worked on the labeled samples without knowing any information about patients. Therefore, the researcher did not have any information about the patients and was blinded in the study.
Statistical analysis
In this study, the data were analyzed using the SPSS 22.0 (IBM, New York, NY, USA) statistical package program. Shapiro–Wilk test was used to determine the distribution patterns of the variables. Numerical values were expressed as mean ± standard deviation, and categorical values were expressed as n (%). The relationship between two quantitative parametric variables was evaluated using Pearson correlation analysis, and nonparametric variables were evaluated using Spearman correlation. Paired sample t-test was used for parametric variables to compare the continuous variables in two dependent groups, and Wilcoxon test was used in nonparametric cases. Linear regression analysis was applied to evaluate the relationship between dependent and independent variables. The p value of less than 0.05 was considered statistically significant.
Results
Overall 28 term newborns with hyperbilirubinemia were enrolled. The infants’ mean birthweight was 3028 ± 366 g and median gestational age was 39 (37–40) weeks. The mean total serum bilirubin concentration at admission was 17.08 ± 3.67 mg/dL. Before phototherapy, the native thiol (μmol/L), total thiol (μmol/L), and disulfide (μmol/L) of the patients with hyperbilirubinemia were found to be 344.1 ± 85.16, 391.69 ± 91.23, and 23.8 ± 14.26 μmol/L, respectively.
After phototherapy, the native thiol, total thiol, and disulfide of the patients with hyperbilirubinemia were found to be 298.38 ± 47.11, 340.42 ± 51.46, and 21.02 ± 7.08 μmol/L, respectively (Table 1).
Comparison of biochemical parameters before and after phototherapy
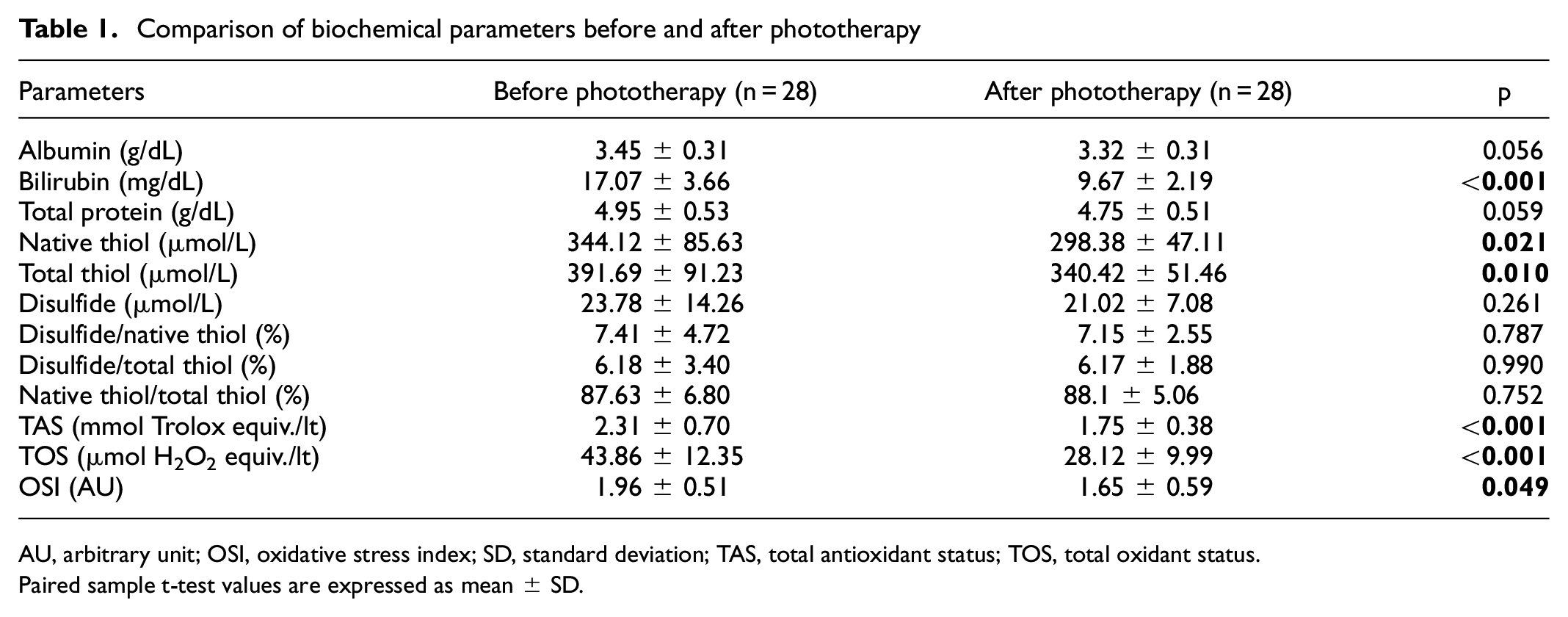
AU, arbitrary unit; OSI, oxidative stress index; SD, standard deviation; TAS, total antioxidant status; TOS, total oxidant status.
Paired sample t-test values are expressed as mean ± SD.
When we examine the changes in biochemical parameters in newborns before and after phototherapy treatment, we found a decrease in bilirubin, TOS, TAS, oxidative stress index (OSI) levels (p < 0.001, p < 0.001, p < 0.001, p = 0.049, respectively, Table 1). The level of albumin was low in the after phototherapy group; however, it did not reach the significant level (p = 0.056). Native thiol level was decreased after phototherapy (p = 0.021).
Before phototherapy, positive correlation was determined between native and total thiol. Similarly, positive correlation was found between bilirubin and TAS and TOS and TAS levels. However, correlation analysis revealed a negative correlation between OSI and bilirubin and TAS and OSI levels (Table 2).
Correlation of oxidative stress parameters and bilirubin before phototherapy
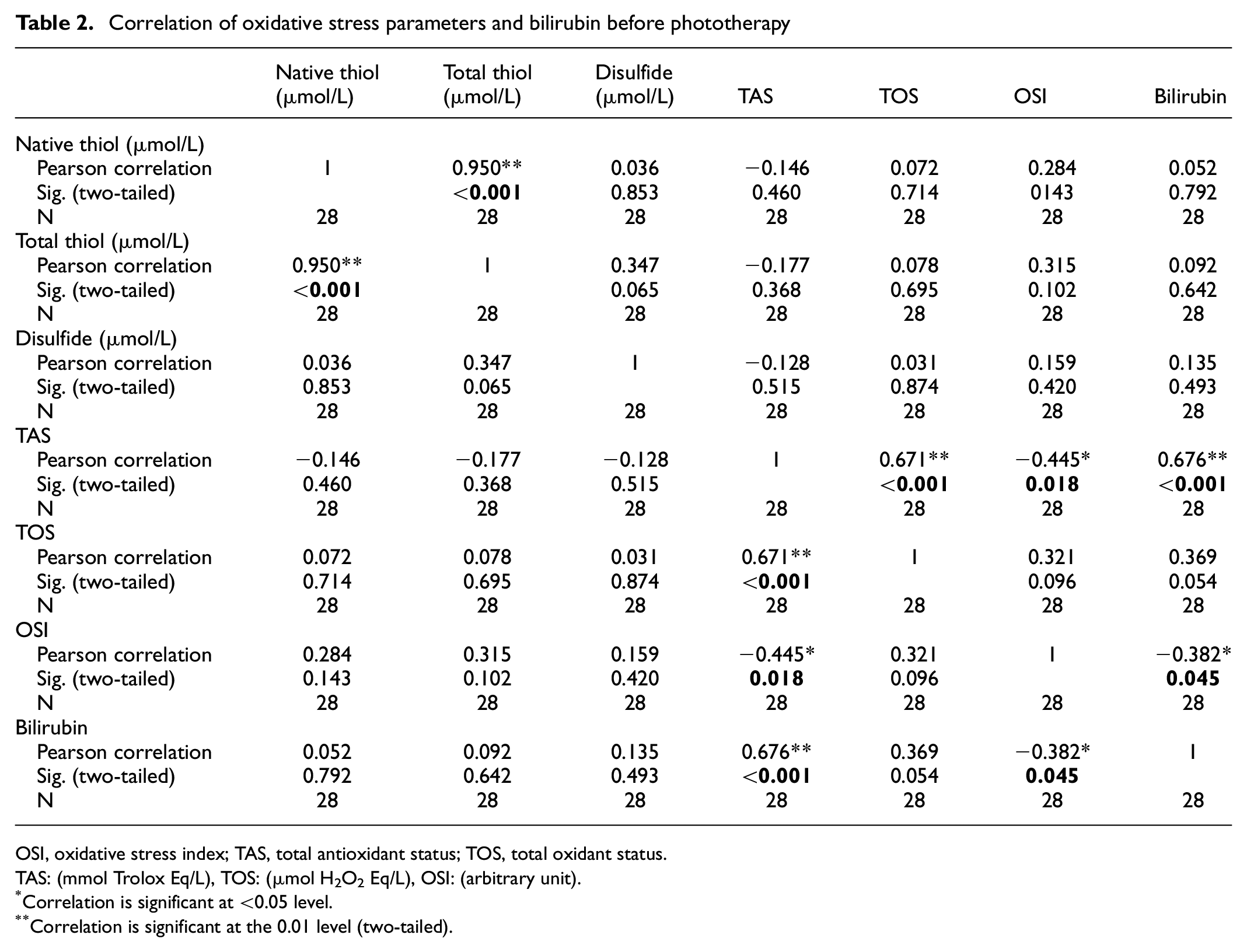
OSI, oxidative stress index; TAS, total antioxidant status; TOS, total oxidant status.
TAS: (mmol Trolox Eq/L), TOS: (µmol H2O2 Eq/L), OSI: (arbitrary unit).
Correlation is significant at <0.05 level.
Correlation is significant at the 0.01 level (two-tailed).
After phototherapy, we indicated positive correlation between TOS and OSI and native and total thiol (Table 3).
Correlation of oxidative stress parameters and bilirubin after phototherapy
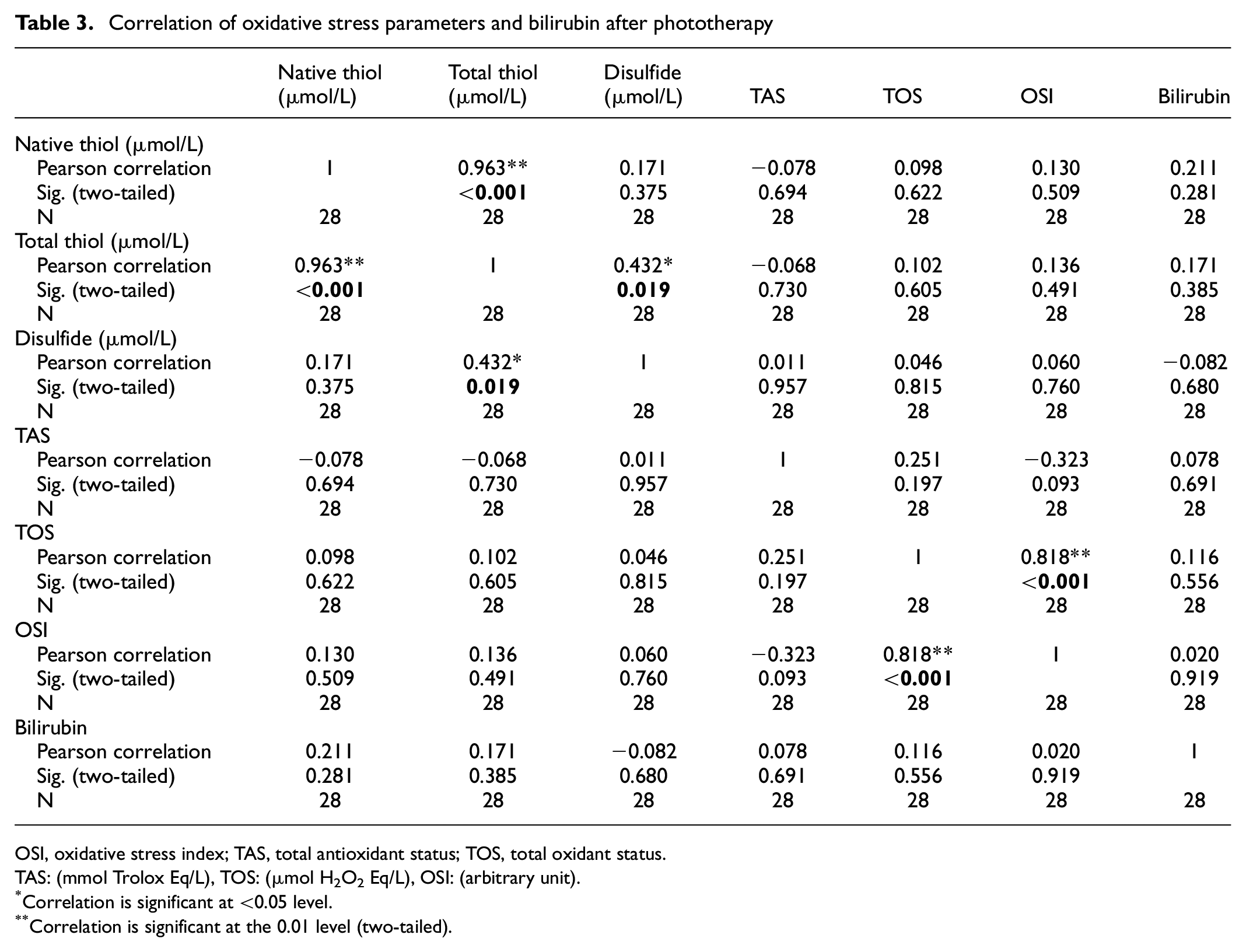
OSI, oxidative stress index; TAS, total antioxidant status; TOS, total oxidant status.
TAS: (mmol Trolox Eq/L), TOS: (µmol H2O2 Eq/L), OSI: (arbitrary unit).
Correlation is significant at <0.05 level.
Correlation is significant at the 0.01 level (two-tailed).
The percentage of difference in bilirubin change and oxidative stress markers was calculated, and the relationship between them was examined by linear regression analysis. It was found to be significant in the linear regression analysis, in which the 14.7% change in the native thiol value and the 15.1% change in the total thiol value were explained depending on the change in the total bilirubin (R = 0.38, R 2 : 0.147, p = 0.044; R = 0.38, R 2 : 0.151, p = 0.041 respectively). No correlation was found between the differences in changes in other oxidative stress parameters.
Discussion
We demonstrated that native and total thiol and disulfide levels were lower in patients receiving phototherapy. Moreover, TAS and TOS levels were found to be significantly lower in patients receiving phototherapy. Similarly, we found OSI levels were decreased but not significantly.
Hyperbilirubinemia in newborns is a condition that increases oxidative stress, which occurs as a result of excessive bilirubin production due to therapeutic destruction of erythrocytes and insufficient clearance of bilirubin by the immature liver.8,9 Hyperbilirubinemia, which is the most common clinical problem in the neonatal period of infants, is a condition that can have potentially toxic effects on the central nervous system such as kernicterus, seizures, and permanent neurodevelopmental damage in newborns.10,11 Brito et al. showed that unconjugated bilirubin increases nitric oxide 12 levels via stimulated glutamate receptors, increasing oxidative stress, and causing damage to neuronal cells. 13 Doğan et al. demonstrated that malondialdehyde levels were highest in the group with kernicterus, and that high bilirubin levels increased oxidative stress. 14 The decrease in TOS levels (p < 0.001) in parallel with decrease in bilirubin levels (p < 0.001) after phototherapy shows that increased oxidative stress is due to high bilirubin levels. Doğan and Gopinathan14,15 also showed that TOS levels decreased after phototherapy, similar to our study.
Although phototherapy converts bilirubin to oxidation products and also to structural isomers that are easily eliminated via the gastrointestinal tract in neonatal hyperbilirubinemia, it may cause oxidative damage, especially in newborns with limited antioxidant protective capacity, as it increases photodynamic stress and lipid peroxidation.16,17 The effectiveness of phototherapy depends on the intensity and wavelength of the light chosen in the treatment. 17 Bilirubin absorbs light the most in the blue region of the spectrum near the wavelength of 460 nm. 18 Blue light (400–500 nm) used in phototherapy has a longer wavelength than ultraviolet light A (300–400 nm), so photons of blue light are less energetic than A photons of ultraviolet light. Exposure to blue light is considered less toxic than ultraviolet light due to the relative energies associated with the different wavelengths.9,19 It has been shown in some studies that after phototherapy, their ability to fight increased and oxidative stress is weakened by reducing the levels of antioxidants such as glutathione and ascorbic acid.20–22 Dynamic thiol–disulfide homeostasis in newborns has an important role in many oxidant–antioxidant mechanisms such as detoxification, antioxidant protection, regulation of enzyme activity. 23 Thiol–disulfide homeostasis has been associated with diseases that increased inflammation such as neonatal sepsis and hepatitis, and conditions that increase stress such as hyperbilirubinemia.24,25 Erol et al. showed that native and total thiol levels were significantly lower in patients receiving phototherapy compared with healthy infants. 26 They also demonstrated that disulfide levels were lower but not statistically significant in patients receiving phototherapy as compared with the controls. In line with the literature, our results indicate that thiol levels were lower as in the previous study. We concluded that decreased thiol levels may elucidate increased oxidative stress after phototherapy in neonates with hyperbilirubinemia. Considering the pro-oxidant and antioxidant effects of bilirubin, we can say that thiol can play an effective role in making the right and effective phototherapy decision.
Stress management has started to be a part of treatment protocols for infants hospitalized in the neonatal intensive care unit, and precautions are taken every day to reduce the stress factors.27,28 The management of conditions is a factor that enables the newborn to struggle against diseases and stressful situations. 29 It is known that antioxidant defense mechanisms against oxidant stress are insufficient in newborns. The antioxidant system in the newborn consists of many units, and as one unit decreases, the other increases, creating a balance. 30 Jaundice observed in the first week of more than 60% of term newborns and more than 80% of preterm is associated with bilirubin being one of the molecules that makes the biggest contribution to the antioxidant defense system. 31 Under physiological conditions, uric acid, vitamin C, and –SH groups decrease in plasma in newborns, while bilirubin and vitamin E levels increase and maintain the antioxidant effect.15,32,33 Therefore, when evaluating oxidative status in the newborn, the measurement of total antioxidant capacity provides more valuable information than the measurement of individual antioxidants. The decrease in TOS, bilirubin, and thiol levels (p < 0.001, p < 0.001, p < 0.001, respectively) after phototherapy supports the decrease in OSI levels (p < 0.005) and this result shows us that oxidative stress decreases after phototherapy. The unexpected decrease in TAS (p < 0.001) capacity after treatment with the decrease in oxidative stress after treatment was attributed to the rapid decrease in bilirubin value of phototherapy and the insufficient increase in other antioxidant elements. This was one of our important results supporting our idea that hyperbilirubinemia in neonates above the phototherapy limit increases oxidative stress.
Strengths and limitations
First, our study was in a single center due to sample conditions, and our patient population was small. Second, oxidative stress may increase in newborns due to conditions other than hyperbilirubinemia, such as separation from the mother due to phototherapy.
Conclusions
Phototherapy treatment reduced the increased oxidative stress associated with hyperbilirubinemia in newborns. In addition, the decrease in bilirubin levels, which has an antioxidant effect in the physiological range and a pro-oxidant effect at high levels, and also an important element of antioxidant capacity in the first week of the newborn, is another determining factor in phototherapy treatment. We think that thiol–disulfide homeostasis can be used as a marker of oxidative stress in patients with hyperbilirubinemia in the early period. The clinical significance of this study is that the determination of dynamic thiol–disulfide levels in newborns with hyperbilirubinemia will help the clinician in the follow-up of the disease prognosis in clinical situations that may occur related to oxidative stress. Our study has been a pioneering study in randomized controlled experimental studies and cohort studies that can contribute to the literature.
Footnotes
Acknowledgements
The authors thank the patients and their parents to participate in the study on a voluntary basis.
Authors’ contributions
Conception and design of the research: MSD, Acquisition of data: HE and MSD. Analysis and interpretation of data: MSD, HE. Statistical analysis: MSD. Drafting the manuscript: MSD. Revision of manuscript for important intellectual content: MSD, HE.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study protocol was approved by the ethical committee of Hatay Mustafa Kemal University (protocol number: 2021/06). Informed consents were obtained the participants parents.