
Abstract
This study was designed to evaluate the effects of colchicine in the improvement of clinical outcomes of hospitalized COVID-19 patients. This prospective, randomized, double-blind, placebo-controlled clinical trial was conducted on adult patients (>18 years) with severe COVID-19. The included patients were randomly (1:1) assigned to the colchicine (2 mg loading dose followed by 0.5 mg twice daily for 7 days) or placebo group. Both groups received remdesivir and interferon beta-1b. The primary outcome of the study was to receive clinical response as ordinal scale of 1 or 2. Secondary outcomes were hospital complications and 28-day mortality. Between February and May 2021, 110 patients were included and 106 of them were analyzed. Baseline clinical characteristics and demographics were not significantly different. According to the ordinal scale, 30 patients in the control group (58.8%) responded to treatment within 7 days, while 35 patients (63.6%) in the colchicine group showed the same response (p = 0.61, odds ratio (OR) = 1.23, 95% CI [0.560–2.68]). On the 14th day, 87.3% of the colchicine group (n = 48) and 82.4% of the control group (n = 42) responded (p = 0.48, OR = 1.47, 95% CI [0.50.3–4.29]. In addition, 28-day mortality, intensive care unit admission, and hospital duration were not different between the groups (p = 0.99, 0.59, 0.06). Diarrhea and nausea were the major side effects dominant in the colchicine group. Colchicine showed no beneficial effects on clinical improvement and hospital complications in patients with COVID-19. Moreover, in case of prescription, the safety concerns of colchicine, specially gastrointestinal side effects, should be taken into account.
Keywords
Colchicine has been used as an anti-inflammatory agent for many years in various diseases.
Inflammatory process in COVID-19 plays an important role in the severity of the disease.
Colchicine triggers anti-inflammatory action with an acceptable safety profile.
In this randomized clinical trial, colchicine as an add therapy showed no superiority over placebo in improving clinical symptoms improvement in hospitalized COVID-19 patients.
Hospital complications were not significant different between two groups of the study.
The results of the study showed that higher body mass index and high dose of corticosteroids (1.5–2 mg/kg) were associated with a lower recovery rate.
Colchicine may not have any beneficial clinically effects on hospitalized COVID-19 patients when administered as adjunctive therapy for a short period of time.
Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection is a pandemic disease which causes lung damage and even acute respiratory distress syndrome in many patients with significant mortality and morbidity. 1 Despite the lack of any specific anti-COVID-19 drug, the efficacy of remdesivir has been approved. 2
Colchicine, a neutral lipophilic tricyclic alkaloid derived from Colchicum autumnale, has been used as an anti-inflammatory agent for many years in various diseases such as gout flares, familial Mediterranean fever, and systemic vasculitis such as Behcet’s disease. It has also been approved for cardiovascular diseases such as pericarditis and acute coronary syndrome. This drug has the ability to inactivate interleukin (IL)-18, IL-1ß, and IL-6. There is evidence supporting that IL-6 plays an essential role in cytokine storm production; hence, colchicine could be effective in inhibiting any inflammation or infection triggered by this storm.3,4 Colchicine also has inhibitory effects on neutrophil chemotaxis and response to vascular injury. 5 The concentration of colchicine, which accumulates in the neutrophils, is 16 times more than the plasma concentration. 6 Several mechanisms, most famously inhibition of microtubule polymerization, have been proposed for the anti-inflammatory effects of this drug. 7 It seems colchicine triggers anti-inflammatory action with an acceptable safety profile. 5
Using the current knowledge about the antiviral properties of colchicine and its effects on inflammatory pathways, this study assesses the safety of colchicine and its efficacy on clinical improvement in patients with COVID-19.
Material and methods
Study design and ethical consideration
This double-blind, placebo-controlled randomized clinical trial was performed on patients infected with COVID-19 between February and May 2021 and hospitalized at Ibn Sina Hospital, a referral tertiary teaching hospital affiliated with Mazandaran University of Medical Sciences, Sari, Iran. This research was approved by the Institutional Review Board and the Ethics Committee of Mazandaran University of Medical Sciences (IR.MAZUMS.REC.1399.914), and registered in the Iranian Registry of Clinical Trials (IRCT20190804044429N5). Patients or their caregivers were informed about the objectives and procedure of the study. Furthermore, all participants (or their caregivers) signed the consent form before the intervention.
Blinding and randomization
Using a permuted block randomization, we divided the patients into 20 blocks of four individuals, who randomly received either colchicine or placebo for 7 days. Colchicine (made by Mofid company) and placebo (prepared at the pharmaceutical laboratory of Mazandaran University of Medical Science) tablets were totally identical in color, shape, and packaging. The patients, the physician, and the pharmacist who was responsible for study evaluation were blind to the intervention assignment.
Setting and patients
Adult patients with SARS-CoV-2 symptoms admitted at Ibn Sina Hospital who were ≥18 years old and whose COVID-19 was confirmed by the reverse transcription polymerase chain reaction (RT-PCR) or chest computed tomography scan were included in the study. Patients with renal impairment (glomerular filtration rate, <30 ml per minute), hepatic impairment (Child-Pugh C), hypersensitivity to colchicine, as well as breastfeeding and pregnant women were excluded from the study.
Study intervention and outcome measurement
Based on the results of the permuted block randomization generator, patients were assigned to the colchicine or placebo group for a 1-week period. The intervention group received colchicine tablet 2 mg as loading dose followed by colchicine 0.5 mg twice daily as maintenance dose for 7 days. The control group received placebo tablets similar to the intervention group. Treatment modality at admission for both groups—including antiviral therapy, antibiotics if needed, corticosteroid therapy (dexamethasone 4 mg administered intravenously three times a day or a high dose of methylprednisolone 1.5–2 mg/kg administered intravenously daily), prophylactic dose of anticoagulants (unfractionated heparin 5000 units administered subcutaneously three times a day or low molecular weight heparin 40 mg administered subcutaneously daily)—and the standard supportive care were based on the official national policy for COVID-19 treatment in Iran. The antiviral therapeutic regimen included remdesivir (200 mg on the first day followed by 100 mg daily for 5 days and interferon beta-1b 250 mcg administered subcutaneously every other day for three doses).
All demographic characteristics as well as medical and drug history were recorded before the intervention. Vital signs including oxygen saturation, temperature, respiratory rate, and blood pressure were evaluated daily. We also assessed the following laboratory data at baseline and every other day: complete blood count, lymphocytes, alanine aminotransferase, aspartate aminotransferase, alkaline phosphatase, urea, serum creatinine, lactate dehydrogenase, C-reactive protein (CRP), erythrocyte sedimentation rate, albumin, troponin, and serum electrolytes.
Outcomes
We measured the clinical status of patients on Days 7 and 14, and used an eight-point ordinal scale to assess the primary outcomes of the study. 8 This scores of this scale were defined as follows: (1) not hospitalized and no activity limitation; (2) not hospitalized with activity limitation or needing home oxygen, or both; (3) hospitalized, no need for supplemental oxygen and continuous medical care (applied in case hospitalization is prolonged for infection control or other nonmedical reasons); (4) hospitalized, no need for supplemental oxygen yet requiring continuous medical care (because of COVID-19 or other medical conditions); (5) hospitalized, needing supplemental oxygen; (6), hospitalized, needing noninvasive ventilation or high-flow oxygen devices; (7) hospitalized, receiving invasive mechanical ventilation or extracorporeal membrane oxygenation; and (8) death. A score 1 or 2 was considered as clinical recovery.
The patients were followed up to 28 days after intervention. The secondary outcomes, which were compared between the two groups, consisted of intensive care unit (ICU) admission, ICU days, and intubation rate. Possible side effects of colchicine were monitored and reported as safety outcomes. If any observed adverse drug reaction (ADR) was life threatening, the drug was discontinued and all therapeutic measures were considered for the patient. The ADRs were classified in accordance with the definition proposed by the World Health Organization.
Statistical analysis
At first, the Kolmogorov–Smirnov test was done to check the distribution status. Then we reported the quantitative variables as mean (standard deviation) or median (interquartile range) based on their respective normal or non-normal distribution. Qualitative variables were presented as frequency and percentage. Independent samples t-test or Mann–Whitney U Test was used for comparing the quantitative variables. The qualitative variables were evaluated using Pearson’s chi-square test and Fisher’s exact test; p values were calculated when needed. Ordinal scores were compared based on Kendall’s tau-b between the two groups. The recovery rate ratio was calculated and compared between the two groups. Kaplan–Meier survival curve of time to death was calculated. We also conducted Breslow test to compare time to recovery between the two groups. ORs for clinical endpoints were calculated using univariate logistic regressions. To determine factors affecting recovery, we performed univariate analysis and considered statistically significant variables for multiple logistic regression. Furthermore, ordinal logistic regression was used to compare the clinical outcomes between the two groups on Days 7 and 14. All analyses were performed in R 3.6.1. p < 0.05 was considered statistically significant.
Sample size was estimated at a minimum of 50 patients in each group; this was obtained on the basis of the results of the study by Scarci et al., 9 the effect of colchicine versus placebo on the hazard of death (hazard ratio 0.151), and considering a statistical power of 80% and Cronbach’s alpha of 0.05.
Results
Patients
Out of 110 patients who met the inclusion criteria, 106 individuals were analyzed (Figure 1). The mean age of patients was 54.62 (SD = ±13.92); besides, 53.8% of participants (n = 57) were female, and 46.2% of them were male (n = 49). With the exception of vomiting (p = 0.04), there was no significant difference in baseline demographic and clinical characteristics as well as laboratory data between the two groups (Table S1 in Supplemental Index).
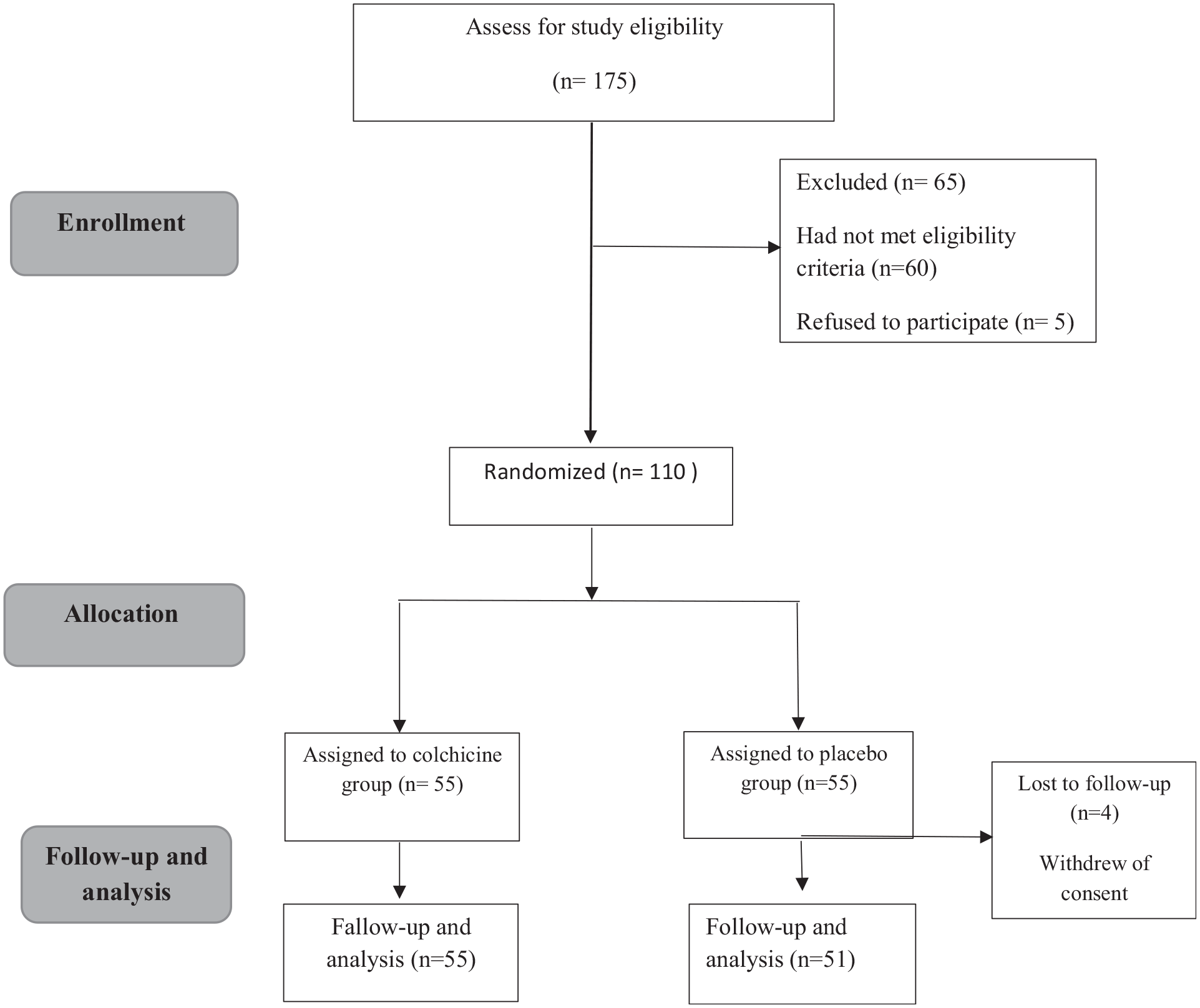
Consort diagram of the study.
Outcomes
The majority of patients had an ordinal score of 4 at baseline (58.2% of colchicine group and 59.6% of control group). According to the ordinal scale, 30 patients in the control group (58.8%) and 35 patients (63.6%) in the colchicine group achieved clinical response within 7 days (p = 0.61, OR = 1.23, 95% CI [0.560–2.68]). On the 14th day, 87.3% of the colchicine group (n = 48) and 82.4 % of the control group (n = 42) responded to treatment (p = 0.48, OR = 1.47, 95% CI [0.50.3–4.29], Table 1). Totally, 88.2% of patients in the control group and 89.1% of patients in the colchicine group reached clinical response with no significant differences (rate ratio = 1.07, 95% CI [0.713–1.60]; p = 0.746). The median time to recovery in survived patients who received colchicine was 6 days, which is not significantly different from the 7 days in the control group (p = 0.06). Also, Kaplan–Meier curve predicted 72.5% survival in the colchicine group versus 78.5% in the control group, indicating no significant difference (p = 0.438, Figure 2).
Clinical outcomes of the study.
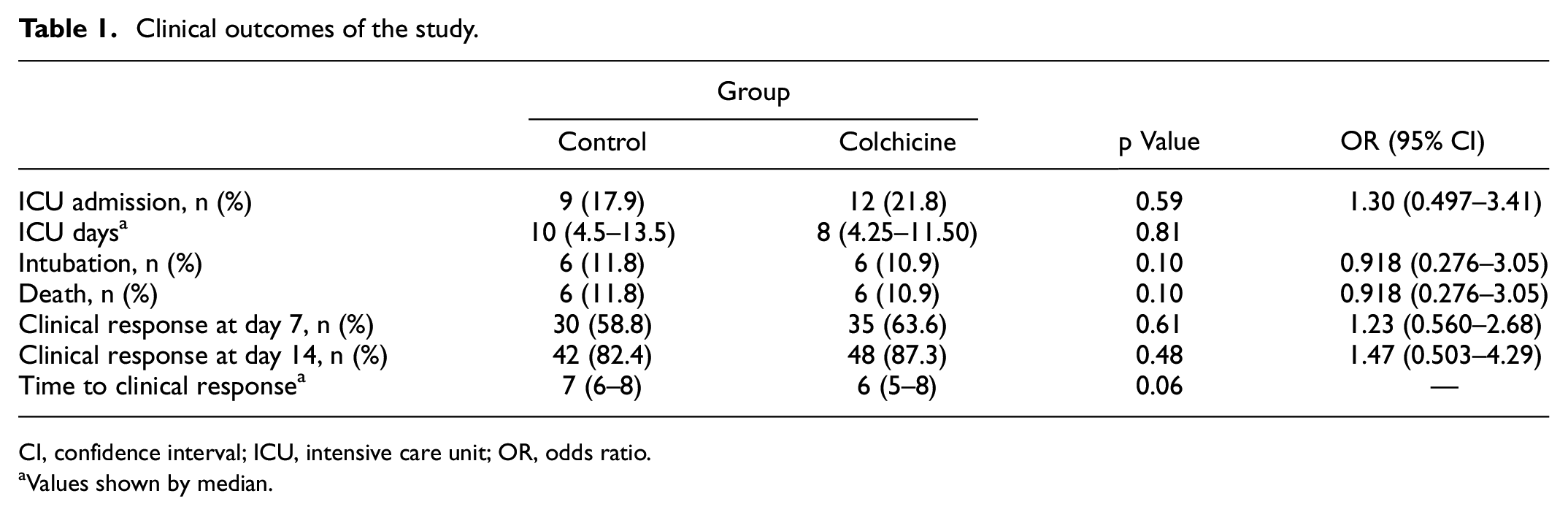
CI, confidence interval; ICU, intensive care unit; OR, odds ratio.
Values shown by median.
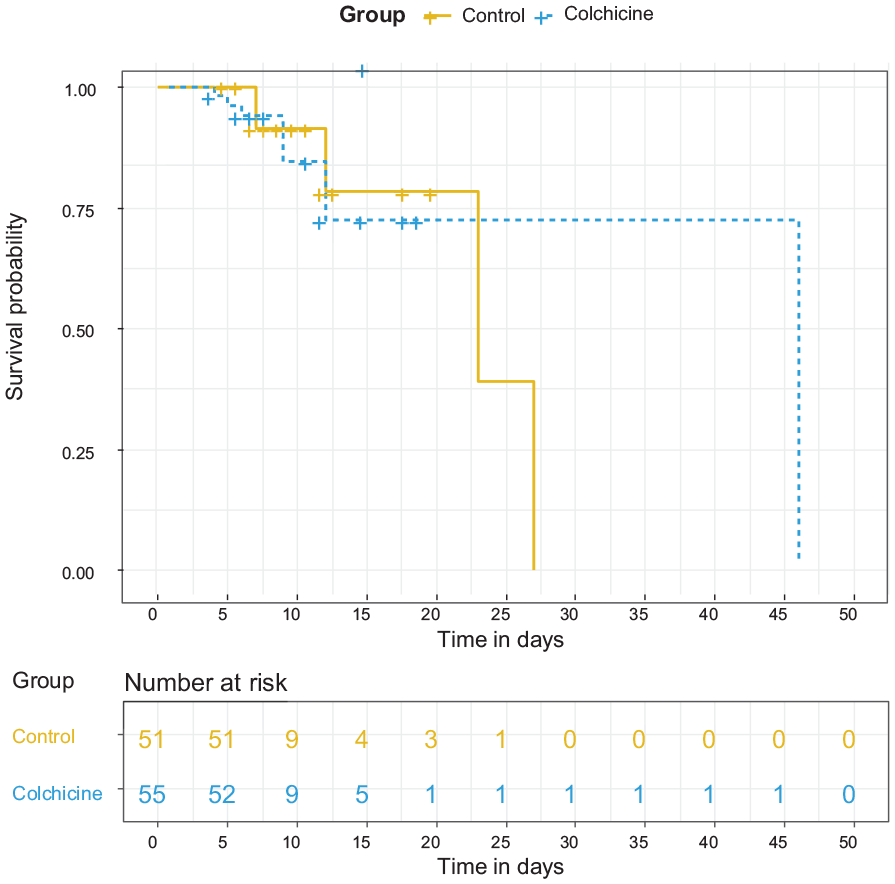
Kaplan–Meier survival curve for study groups.
In addition, 9 patients (17.6%) from the control group and 12 patients (21.8%) from the colchicine group were admitted to the ICU, which was not statistically significant (p = 0.59). Also, the rates of intubation in the control and colchicine groups were, respectively, 11.8% (6 patients) and 10.9% (6 patients). All intubated patients of the control group died, but one intubated patient from the colchicine group survived (Table 1).
The results of logistic regression analysis revealed that some factors such as higher body mass index and high dose of corticosteroids (methylprednisolone 1.5–2 mg/kg) were associated with a lower recovery rate (p = 0.033, 0.015; OR = 0.48, 0.74). However, it is important to note that patients with worse clinical conditions were administered high dose of methylprednisolone. Moreover, higher baseline ordinal scores reduced the chance of recovery by 86%, which is marginally significant (p = 0.057, OR = 0.14; Figure 3).
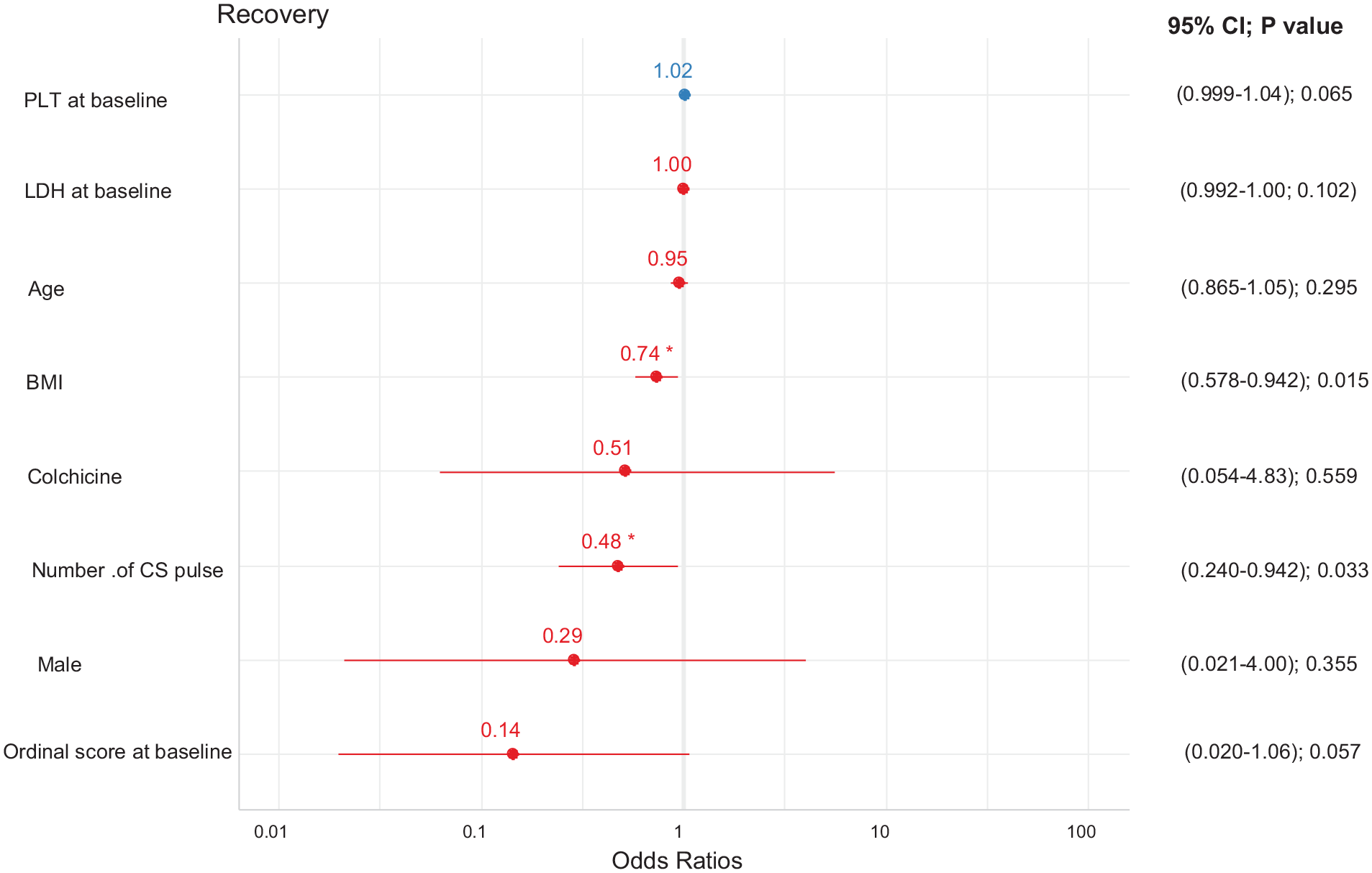
The results of multiple logistic regression of recovery of patients.
Safety concerns
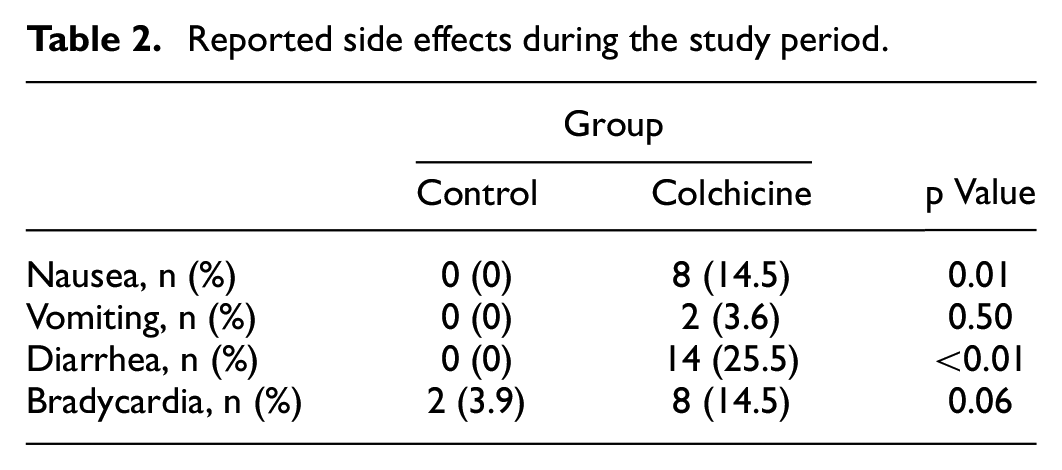
The ADRs were monitored during the study period. Most of the reported side effects were related to the gastrointestinal system, with nausea and diarrhea occurring significantly more in the colchicine group (p = 0.006, p < 0.001, respectively, Table 2). One patient in the colchicine group discontinued the treatment regimen due to severe diarrhea. No alarming sign was detected.
Reported side effects during the study period.
Discussion
The results of the study showed the clinical response caused by colchicine was not superior to placebo in patients with COVID-19 in terms of time of recovery, need for ICU admission, and mortality rate. Concerning the safety profile, colchicine had an even higher risk of gastrointestinal ADRs than placebo.
The idea of administering colchicine for COVID-19 complications is inspired by its pharmacological properties as an immunomodulatory. 10 It has been suggested that the severity of the infection is highly correlated with the strength of patients’ immune response. 11 Studies have revealed the relationship between immune dysregulation and severe COVID-19 accompanied by high levels of inflammatory cytokines, a condition which is known as acute systemic inflammatory response syndrome. IL6, IL12, and TNF-α are the main inducers of the cytokine release syndrome; hence, it seems reasonable to administer cytokines inhibitors in combination with antiviral agents.11,12
Deftereos et al. conducted a prospective, open-label clinical trial on 105 hospitalized patients who had been randomly assigned to the colchicine and control groups. Colchicine was administered at a loading dose of 1.5 mg followed by 0.5 mg twice daily for maximum 3 weeks. The primary outcomes of the study included biochemical and clinical evaluation. Regarding the biochemical dimension, no significant differences were observed in CRP levels and high-sensitivity cardiac troponin (p = 0.73, 0.34). However, time to improved clinical outcomes was significantly better in the colchicine group (p = 0.02) and diarrhea was a dominant ADR. 3 Despite the similarity of this research with our study in terms of colchicine initiation before any need for ventilation, the dosing regimen in the study of Deftereos et al. was different from our study in that we administered a lower loading dose and a shorter duration of maintenance dose. Moreover, concomitant COVID-19 regimen also differed between the two studies, whereas Deftereos et al. mainly used hydroxychloroquine or chloroquine, lopinavir or ritonavir and azithromycin, we used remdesivir and interferon beta 1b as the standard regimen. The mortality rate in our study was higher than in the other study (11.3% vs 4.8%). This variation might be explained by the fact that the median time of hospital admission in the other study was earlier than in the case of our patients (less than 7 days), which means patients in that study received medical care at an earlier stage of the disease. The earlier the stage of COVID-19 is, the more effective the antiviral medications will be.13,14 However, similar to our results, colchicine showed no benefit on hospital duration. In spite of their promising results, Deftereos et al. did not mention the number of predicted patients whose clinical outcomes needed to be assessed. Besides, lack of blinding of the study (of Deftereos et al.) should be considered while interpreting the results.
In another study, which was a randomized, double-blind clinical trial, the benefits of colchicine were assessed in 72 patients with moderate to severe COVID-19. Colchicine was used at a loading dose of 0.5 mg three times daily for the first 5 days followed by 0.5 mg twice daily for another 5 days. The authors reported that the supplemental oxygen requirement and length of hospital stay were reduced significantly in the colchicine group (median time 4 vs 6.5, 7 vs 9.5 days). CRP levels also showed a declining trend. 15 The total dose of colchicine in that study was more than our trial (12.5 mg vs 9 mg), and the COVID-19 regimen they administered was also different as it consisted of hydroxychloroquine and azithromycin. While the authors confirmed the beneficial effects of colchicine on hospital duration and the need for oxygen support, they did not address the effects of colchicine on ICU admission and mortality rate. Furthermore, the results of their study should be interpreted with caution due to their small sample size and their different management strategy for corticosteroids during the study period.
In an observational study, the efficacy of colchicine was evaluated in hospitalized COVID-19 patients. At two separate intervals, 122 patients received colchicine 1 mg daily, and their results were compared with those of 140 patients who received standard care including hydroxychloroquine, lopinavir/ritonavir, and dexamethasone. The findings showed colchicine, compared to the standard regimen, could lead to a better survival rate. 9 The clinical characteristics of patients and the treatment strategy were different between the two groups. Moreover, disease severity, intervention duration, and the main outcomes were not clearly defined in the method section of that study.
The effects of colchicine on 141 COVID-19 patients were assessed in a retrospective, observational study. Colchicine was administered 1 mg daily until clinical improvement or maximum 21 days. The colchicine group showed a lower cumulative incidence of death (7.5% vs 28.5%, p = 0.006) and a better 21-day clinical improvement rate (40% vs 26.2%, p = 0.048). 16 It is important to address patients’ heterogeneity in terms of disease severity and antiviral treatment, in addition to the retrospective nature of this study when interpreting the results.
In a randomized, double-blind, multicenter clinical trial, the effects of colchicine on COVID-19 patients who were not hospitalized (COLCORNA trial) were evaluated. 17 Colchicine was administered for a month (0.5 mg twice daily for 3 days and then once daily). In comparison with the placebo group, a lower rate of death or hospitalization was reported only in the colchicine group among patients with PCR-confirmed diagnoses. The authors recommended colchicine to patients at risk of COVID-19 complications. It should be noted that the beneficial effects were not reported for all the treated patients, and, as a whole, the clinical superiority over placebo was not shown.
In a recent large randomized, open-labeled, multicenter clinical trial (RECOVERY), 1 mg of colchicine was administered followed by 0.5 mg twice daily for 10 days or until discharge. 18 Colchicine did not show any significant effect versus placebo on 28-day mortality, hospital stay, and the need for invasive mechanical ventilation. The results of the study are consistent with our findings.
A case series of five patients with iatrogenic allogenosis (IA) reported the clinical outcomes of patients with COVID-19 and IA concurrence who took colchicine. Colchicine was prescribed for these patients to relieve the symptoms of IA. Until achieving remission, they received colchicine at a dosing regimen recommended for gout attack. Although their COVID-19 PCR tests were positive, all of them were infected with mild COVID-19 without the need for hospitalization, while some of their close contacts experienced severe disease or even died (due to COVID-19). 19 Patient demographics, clinical characteristics, and duration of colchicine usage were different among patients.
The significant adverse events following colchicine administration in our trial were nausea and diarrhea, which is in line with other randomized controlled trials.3,15 But no other adverse effects including neuropathy, myopathy, liver failure, hematologic or infectious event, and death have been observed. The gastrointestinal effects of colchicine could be linked to increased prostaglandin and bowel movements. 20 Another study investigating the hypothesis of colchicine efficacy in the prevention of COVID-19 complications has pointed to the increased risk of pneumonia in colchicine receivers. 21
Our study has some limitations. First, because of insufficient resources, RT-PCR test was not done for all patients (15 of 105 patients). Also, in addition to the single-center design of the study, another limitation was that we did not evaluate the levels of inflammatory cytokines because of our primary hypothesis of possible anti-inflammatory effects of colchicine. The results of studies that support colchicine administration suggest that increased loading dose of this drug and its longer administration contribute to improving its efficacy. It should be noted that most of our patients had baseline ordinal scores of 3 and 4, which made it difficult to draw a definitive conclusion.
Conclusion
The results of our study showed no superiority for colchicine over placebo in improving clinical outcomes of patients with COVID-19. Furthermore, diarrhea as a major problem of colchicine can be troublesome. Multicenter, and randomized controlled clinical trials with larger number of patients are needed to further explore the role of colchicine in the management of hospitalized patients with COVID-19.
Supplemental Material
sj-pdf-1-imj-10.1177_10815589221141815 – Supplemental material for The effects of colchicine on hospitalized COVID-19 patients: A randomized, double-blind, placebo-controlled clinical trial
Supplemental material, sj-pdf-1-imj-10.1177_10815589221141815 for The effects of colchicine on hospitalized COVID-19 patients: A randomized, double-blind, placebo-controlled clinical trial by Hossein Kasiri, Mobin Ghazaiean, Nima Rouhani, Fahimeh Naderi-behdani, Monireh Ghazaeian and Robabeh Ghodssi-Ghassemabadi in Journal of Investigative Medicine
Footnotes
Author contributions
Hossein Kasiri and Mobin Ghazaiean: Data Curation, Investigation. Nima Rouhani: Project Administration. Fahimeh Nader-behdani: Writing—original draft. Monireh Ghazaeian: Conceptualization, Methodology, Supervision, Writing—review & editing. Robabeh Ghodssi-Ghassemabadi: Formal analysis and Data Curation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Vice Chancellery for Research Affairs of Mazandaran University of Medical Sciences (Grant number: IRMAZUMS8653).
Ethics approval
This study abides by the Declaration of Helsinki and was approved by the Ethics Committee of Mazandaran University of Medical Sciences (IR.MAZUMS.REC.1399.914).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.