
Abstract
Our investigation aimed at evaluating the relationship between metabolic syndrome, alanine aminotransferase (ALT), aspartate aminotransferase (AST), gamma glutamyl transferase (GGT), and alkaline phosphatase (ALP) in the Rafsanjan cohort study (RCS). We used data obtained from the RCS, as a part of the prospective epidemiological research studies in Iran. In this cross-sectional research, 9895 participants from the baseline phase of RCS who completed medical questionnaire were included. Metabolic syndrome (MetS) defined using NCEP-ATP III criteria. The relationship between elevated serum liver enzymes levels even within the normal range and metabolic syndrome was evaluated by logistic regressions. The prevalence of MetS was 34.42% in the participants of study. The mean concentrations of AST, ALT, ALP, and GGT increased with increasing MetS components. After adjusting for all potential confounders, elevated serum concentrations of ALT, AST, GGT, and ALP even within the normal range were related with an increased odds of MetS. MetS was associated with increased levels of liver enzymes even within the normal range. These results indicated the potential for elevated liver enzymes as biomarkers for the possible presence of MetS.
Keywords
In some studies, increased levels of hepatic enzymes even within the normal range have been associated with an increased risk of MetS, and the results of these studies have been inconsistent.
After adjusting for all potential confounders, elevated serum concentrations of ALT, AST, GGT, and ALP even within the normal range were related with an increased odds of metabolic syndrome.
These results indicated the potential for elevated liver enzymes as biomarkers for the possible presence of MetS.
Introduction
Metabolic syndrome (MetS) is a combination of cardiovascular risk factors including abdominal obesity, elevated blood lipid levels, hyperglycemia, and hypertension. 1 This is a public health problem with global high prevalence. The global prevalence of MetS has been reported between 14% and 30%. 2 Recently, the incidence of MetS in Iran has appreciably increased. According to the latest research conducted in 2020, about 41.10% of the population of Iran had MetS according to NCEP-ATP III criteria. 3 Age, sex, smoking status, region, and place of residence have been reported as factors associated with this disease.3,4
The liver is a vital organ in metabolism and plays an important role in regulating blood sugar homeostasis. Markers of hepatic impairment such as alkaline phosphatase (ALP), alanine aminotransferase (ALT), aspartate aminotransferase (AST), and gamma glutamyl transferase (GGT) have been identified as good criteria for measuring liver health and are also associated with diabetes, hypertension, and metabolic syndrome. Among liver enzymes, ALT is a specific marker of liver damage that is often found in the liver and has been reported to be closely associated with fat accumulation in the liver, while AST is a less specific marker of liver damage because it is also found in other tissues. 5 GGT mediates glutathione uptake and is thought to be associated with oxidative stress and chronic inflammation, both of which are important pathways in the progression of diabetes. GGT is very active in the liver, pancreas, and kidneys. 6
Non-alcoholic fatty live disease (NAFLD) is a common disorder that was first reported in obese diabetic women in 1980. 7 NAFLD is defined as the storage of more than 5% of fat in the liver in the absence of any other cause of chronic liver disease. The disease may progress from simple liver steatosis to various degrees of fibrosis and cirrhosis, and liver cancer. 8 Markers of liver damage in NAFLD are elevated liver enzyme levels. Epidemiological studies have shown that NAFLD, which is the most common cause of elevated liver enzymes, has been associated with MetS.9,10 In some studies, increased levels of hepatic enzymes even within the normal range have been associated with an increased risk of MetS.11,12 Recently, special attention has been paid to the role of liver enzymes in predicting MetS. Although previous studies have shown an association between elevated liver enzyme levels and MetS, the results of these studies have been inconsistent.11,13–15 Some previous studies have shown a significant relationship between elevated levels of ALT, GGT, ALP, and AST with MetS.11,13 In another study, there was a relationship between elevated ALT and GGT but not AST level with MetS. 15 On the other hand, some studies have shown that only a significant increase in GGT level is associated with all components of the MetS. 14 Considering the high prevalence of MetS in Iran and the effect of this risk factor on the progression of cardiovascular disease, 16 determining the relationship between hepatic enzymes and MetS is helpful for the possible presence of this disorder.
Due to the discrepancy between the results of different studies, the purpose of this study was to investigate the relationship between the level of hepatic enzymes (normal and elevated) and MetS in a larger sample size in the adult population of Rafsanjan.
Materials and methods
Study design and patient selection
This cross-sectional study was conducted using the Rafsanjan cohort study (RCS) data, as a part of the prospective epidemiological research studies in Iran (PERSIAN). 17 RCS is a population-based prospective cohort of participants aged 35–70 years of both genders, launched in August 2015. In the enrollment phase, subjects from diverse socioeconomic levels and lifestyles were recruited from four urban and suburban areas of Rafsanjan. A total of 9991 subjects accepted to participate. All the subjects gave written informed consent. Questionnaire-based interviews and anthropometric measurements were completed and bio-specimens (blood, urine, hair, and nail) were collected for all participants. 18 Study protocol was designed according to the PERSIAN cohort study and approved by the Ethics Committee of Rafsanjan University of Medical Sciences (Ethical codes: ID: IR.RUMS.REC.1400.044). The enrollment phase ended in December 2017, and a 15-year follow-up is planned.
Data collection
Through a standardized interview and validated questionnaires, we collected data on socioeconomic status, smoking habits, opium use, alcohol consumption, disease history, nutrition, and physical activity. Height, weight, waist circumference, and systolic and diastolic blood pressure were measured as described elsewhere. 18 Socioeconomic status was measured according to the Wealth score index (WSI). This index was determined using multiple correspondence analysis of the participants’ economic and social variables. 19 According to WSI, participants of study were divided into four groups based on the 25th, 50th and 90th: low class, low-middle class, middle-high class, and high class. The intensity of physical activity was evaluated base on metabolic equivalent of task (MET). Physical activity was categorized according to the 24-h physical activity and a 22-item questionnaire and was categorized as low (≤35.29 MET-hours per week), moderate (35.30–40.32 MET-hours per week), and heavy (≥40.32 MET-hours per week) groups based on the 25th and 75th. 19 Questionnaires were validated in the PERSIAN cohort study. 17 History of fatty liver was evaluated based on a question “has fatty liver diagnosed by a physician.” The answer was yes or no.
Biochemical measurements
All participants were asked to fast for at least 12 h before the examination. Blood samples were taken between 7:00 and 9:00 AM. Fasting blood sugar (FBS), total cholesterol, high-density lipoprotein cholesterol (HDL cholesterol), low-density lipoprotein cholesterol (LDL cholesterol), triglycerides (TG), SGOT (Serum glutamic-oxaloacetic transaminase) (AST), SGPT (Serum glutamic pyruvic transaminase) (ALT), GGT, and ALP were measured by a biotecnica analyzer (BIOTECNICA INSTRUMENTS S.p.A via licenza, 18-00156 ROMA, BT 1500-A-A S/N 47152615, Italy) at the Central Laboratory in Cohort Center. Serum ALT and AST activities were measured using kinetic method (Pars Azmoon Co, Tehran, Iran). Serum ALP and GGT activities were determined using p-nitrophenol phosphate and p-glutamyl-3-carboxy-4-nitroanilide phosphate as a substrate, respectively (kinetic method, Pars Azmoon Co).
Definition of terms
Based on NCEP-ATP III criteria, having three or more of the following risk factors was defined as MetS:
(1) Waist circumference ≥102 cm for men and ≥88 cm for women, (2) triglyceride ≥150 mg/dL or use of medication, (3) HDL < 40 mg/dL in men or <50 mg/dL in women or use of medication, (4) hypertension (systolic blood pressure ≥130 mmHg or diastolic pressure ≥85 mmHg) or use of medication, and (5) hyperglycemia (FBS ≥ 100 mg/dL or use of medication). 3
Elevated serum ALT, AST, GGT, and ALP levels were defined according to the reference range of the laboratory in cohort center. Elevated serum both ALT and AST levels were defined as >40 U/L (males) and >35 U/L (females). Elevated serum GGT levels were defined as >54 U/L (males) and >37 U/L (females). Elevated serum ALP levels were considered as >306 U/L in both genders. Within the normal range, AST, ALT, GGT, and ALP levels were divided into the following quartiles: for ALT ≤14, 15–19, 20–25, and 26–40 U/L (males) and ≤12, 13–15, 16–20, and 21–35 U/L (females); for AST ≤16, 17–19, 20–23, and 24–40 U/L (males) and ≤14, 15–16, 17–20, and 21–35 U/L (females). The quartiles for GGT were including ≤18, 19–23, 24–31, and 32–54 U/L (males); and ≤14, 15–18, 19–23, and 24–37 U/L (females). The ALP quartiles were including ≤177, 178–209, 210–244, and 245–306 U/L in both genders.
Statistical analyses
To describe the data, frequency (%) for categorical variables and the mean (standard deviation (SD)) for the quantitative variables were used and baseline characteristics of individuals were compared across the groups of our study (non-MetS, MetS using chi-square (χ2) and t-test for categorical and continuous variables, respectively). Also, subjects were divided across numbers of positive MetS components (0–5 components) into six category. Then, specific mean (SD) of each class for each liver enzyme was computed and trend linear regression analysis was used to assess trends in mean liver enzyme concentrations according to each class of positive MetS components. In addition, we used dichotomous logistics regression models to determine the odds ratios (ORs) and the corresponding 95% confidence intervals (CI) for the relation of MetS to the level of liver enzymes. We used four models in the regression analysis. Potential confounding variables were sequentially entered into models according to their hypothesized strengths of association with serum concentrations of liver enzymes and MetS. Variables with a p value <0.25 were selected as confounders. Moreover, baseline model (crude model) has been stratified on the condition of serum concentrations of liver enzymes. In addition, the adjusted model 1 included for gender, age, education years, and wealth status index and model 2 had further adjustment to the variables that were related with the life style (cigarette smoking, alcohol drinking, opium consumption), body mass index (BMI: continuous variable) as well as the level of the physical activities (continuous variable). The adjusted model 3 had additional adjustment for family history of hypertension in first-degree relatives (yes/no), family history of diabetes in first-degree relatives (yes/no), hepatotoxic drugs (yes/no), and fatty liver (yes/no). All analyses were performed through Stata V.14. All p values are two-sided.
Results
A total of 9895 participants from the baseline phase of Rafsanjan adult cohort Study who completed medical questionnaire were included. The overall prevalence of MetS was 34.42%. Elevated FBS (58.10%), waist circumference (53.92%), elevated triglyceride (47.45%), elevated blood pressure (28.83%), and low HDL (10.05%) were the most common components of MetS. Table 1 shows the sociodemographic, habits, clinical and biochemical characteristics of all the subjects with or without MetS in the Rafsanjan cohort participants. The ages of the subjects ranged from 35 to 70 years, with a mean age of 49.97 ± 9.56 (MetS: 53.34 ± 8.97 years; non-MetS: 48.20 ± 9.39 years).
Demographic, selected medical, and laboratory characteristics of study participants (n = 9895).
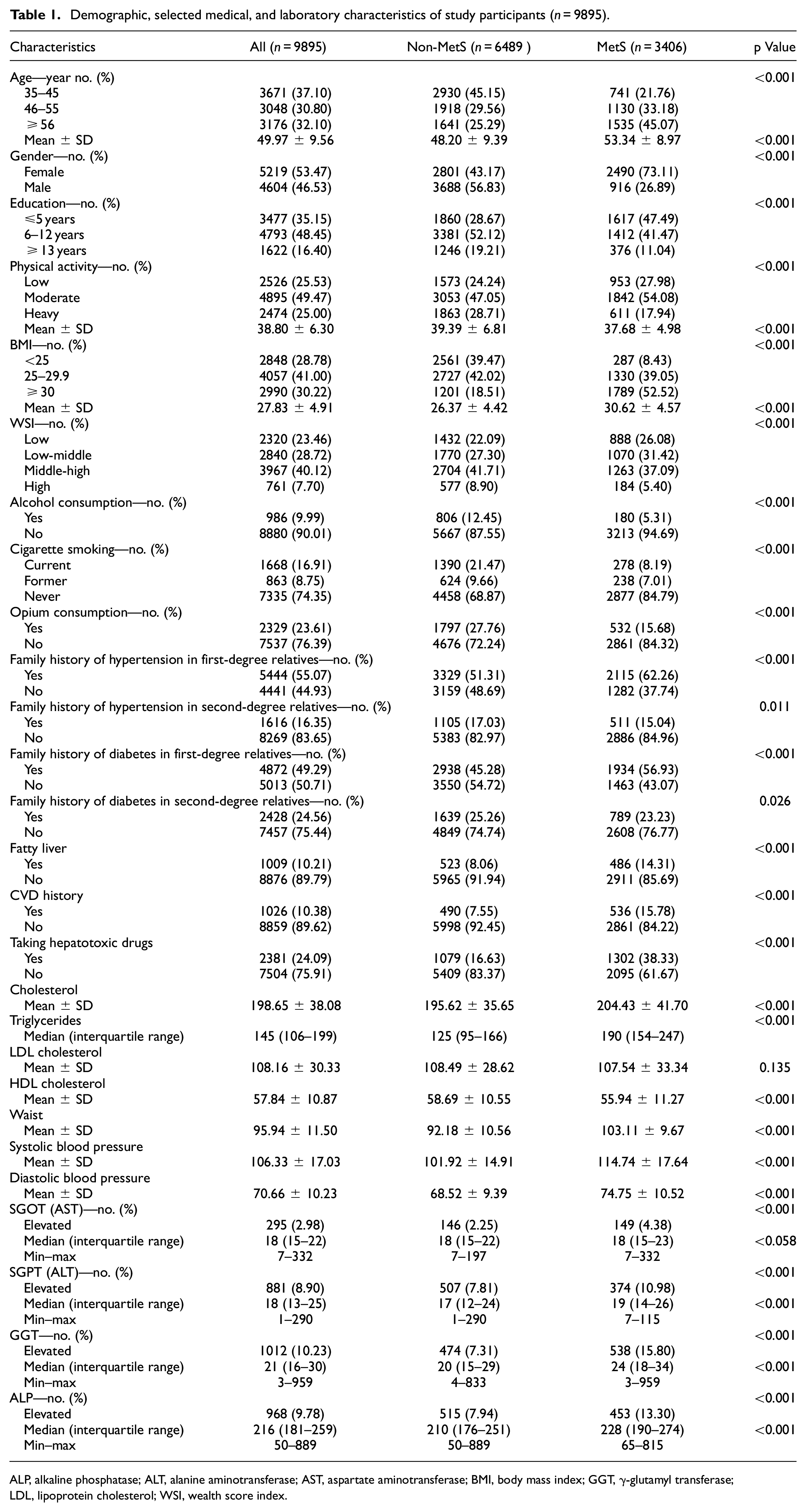
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; GGT, γ-glutamyl transferase; LDL, lipoprotein cholesterol; WSI, wealth score index.
The prevalence of MetS was significantly higher in women (26.89% of men and 73.11% of women) and less educated subjects. Approximately 9.9%, 16.91%, and 23.61% of participants reported being consumers of alcohol (MetS: 5.31% and non-MetS: 12.45%), cigarette (MetS: 8.19% and non-MetS: 21.47%), and opium (MetS: 15.68% and non-MetS: 27.76%), respectively.
Subjects with MetS compared to those without MetS had significantly greater levels of BMI, systolic blood pressure, diastolic blood pressure, total cholesterol, triglyceride, ALT, GGT, and ALP but lower levels of HDL cholesterol, WSI, and physical activity. Family history of hypertension and diabetes in first-degree relatives, fatty liver, and taking hepatotoxic drugs were significantly higher in subjects with MetS compared with those without MetS.
Table 2 shows the mean concentration of liver enzymes stratified by number of risk factors of MetS. Overall, mean concentrations of AST, ALT, ALP, and GGT increased with increasing MetS components.
The mean concentration of liver enzymes stratified by number of risk factors of metabolic syndrome (n = 3406).
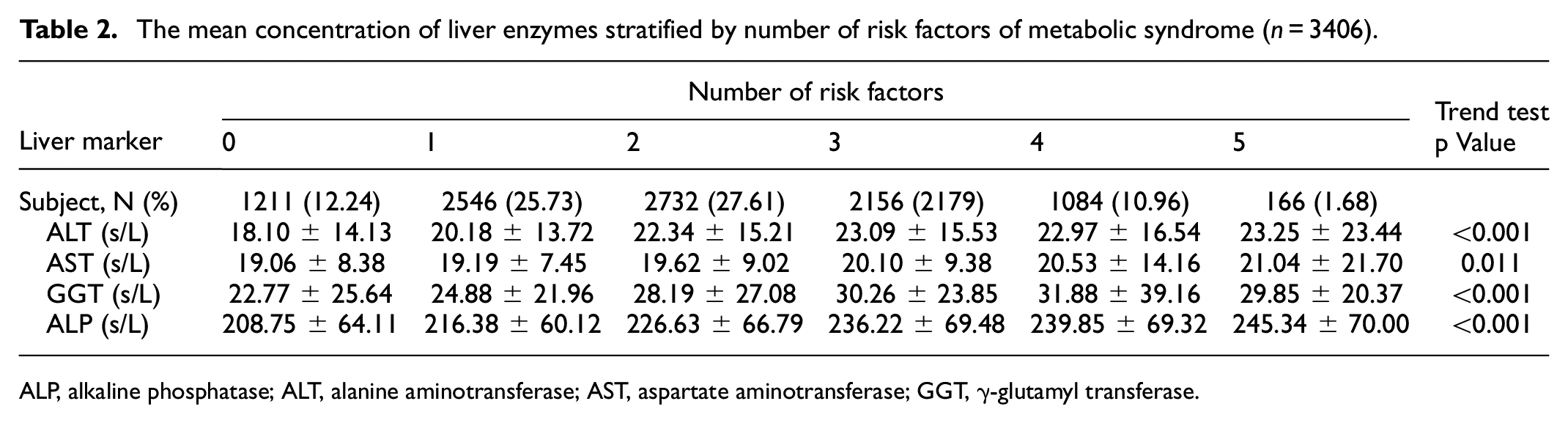
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; GGT, γ-glutamyl transferase.
Table 3 presents the association of the levels of liver enzymes with MetS. The normal ranges of AST, ALT, GGT, and ALP levels were divided into the four quartiles. Elevated ALT, GGT, AST, and ALP levels in all crude and adjusted models were significantly associated with higher odds of MetS. In all crude and adjusted models, in subjects with normal levels of ALT, AST, GGT, and ALP dose–response increases for MetS were observed with the highest ORs in the fourth quartile. In fully adjusted model, the OR of MetS in normal quartile 4 of all liver enzymes was significantly higher than that of the subjects in normal quartile 1 (OR for ALT: 1.88 (1.62–2.18), OR for AST: 1.38 (1.20–1.58), OR for GGT: 3.23 (2.76–3.80), and OR for ALP: 1.52 (1.30–1.77)). Also, subjects with elevated levels of four liver enzymes showed increased odds of MetS compared with subjects in normal quartile 1 (OR for ALT: 2.61 (2.14–3.18), OR for AST: 2.01 (1.50–2.68), OR for GGT: 4.06 (3.34–4.92), and OR for ALP: 1.93 (1.60–2.33)).
Odds ratios (95% confidence interval) for metabolic syndrome by the level of liver enzymes.
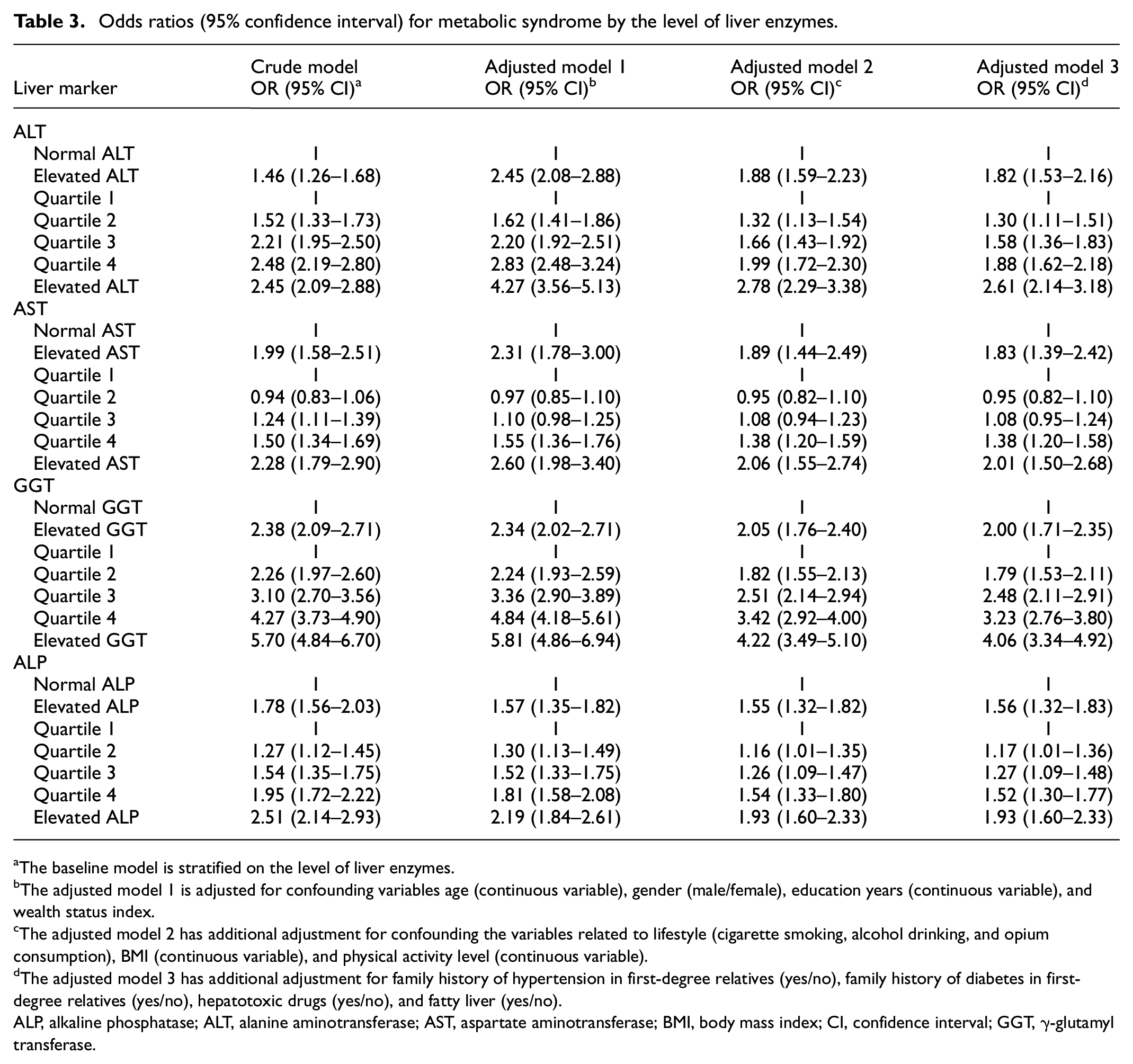
The baseline model is stratified on the level of liver enzymes.
The adjusted model 1 is adjusted for confounding variables age (continuous variable), gender (male/female), education years (continuous variable), and wealth status index.
The adjusted model 2 has additional adjustment for confounding the variables related to lifestyle (cigarette smoking, alcohol drinking, and opium consumption), BMI (continuous variable), and physical activity level (continuous variable).
The adjusted model 3 has additional adjustment for family history of hypertension in first-degree relatives (yes/no), family history of diabetes in first-degree relatives (yes/no), hepatotoxic drugs (yes/no), and fatty liver (yes/no).
ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; BMI, body mass index; CI, confidence interval; GGT, γ-glutamyl transferase.
Discussion
This study found that the prevalence of MetS was 34.42 in the participants of the Rafsanjan cohort study, an area in the southeast of Iran, according to ATP III criteria. Elevated FBS (58.10%) and waist circumference (53.92%) were the most common components of MetS. According to the best of our knowledge, this study is the first report of the prevalence of MetS in a large population-based cohort study in this area. Almost similar to our results, in a systematic review study in 2015, the prevalence of MetS in Iranian general population who were aged 18 years and over was reported 36.9% (95% CI: 32.7%–41.2%) according to ATP-III criteria. 8 The prevalence of MetS in the present study was higher than the study of Dalvand (29%) and lower than the study of Bahar (41%) 3 in the Iranian population8,20 that this could be due to differences in their BMI, age ranges, cultures, lifestyle habits, socioeconomic status, and environmental factors.
The main finding of this study was that subjects with elevated ALP, ALT, AST, and GGT levels were more likely to have odds of MetS even after adjustment for covariates such as demographic variables, variables related to lifestyle, family history of hypertension and diabetes, use of hepatotoxic drugs, and fatty liver. These results further confirmed the existence of a link between the elevated liver enzymes and odds of MetS.
Furthermore, we found a positive linear trends between higher ALP, ALT, AST, and GGT concentrations and the presence of increasing numbers of metabolic abnormalities that this finding was consistent with the results of previous study in Thailand. 21 Also, in a study of Taki in Japan, a dose–effect significant relationship with the number of MetS abnormalities was seen with increased ALT, AST, and GGT but not ALP concentrations. 22
The association between MetS prevalence and elevated concentrations of liver enzymes is supported by some previous studies.5,11,21,23,24 Gaeini et al. in Tehran Lipid and Glucose Study showed that elevated serum concentrations of AST, ALT, GGT, and ALP were positively associated with odds of developing MetS. 11 Perera et al. in a cross-sectional study among Thai adults showed that the mean concentrations of ALT, AST, and ALP increased with increasing the number of metabolic abnormalities. They observed that after adjusting for confounders, elevated liver enzymes might be related with MetS risk. 21 In a recent meta-analysis, Ballestri et al. analyzed a pooled population of 81,411 patients. Subjects were followed-up for 4.5 years. NAFLD was associated with an increased risk of incident MetS with a pooled OR of 1.98 and 1.80 for GGT and ALT, respectively. 25
Also in the present study, the association between MetS and serum levels of ALP, ALT, AST and GGT within the normal range was assessed. Our findings showed that with increasing liver enzyme concentrations even within normal range, odds of MetS increased with a dose–response relationship. Participants had higher odds of MetS from the lowest quartile to the highest quartile within the normal range of ALP, ALT, AST, and GGT. Our results indicated that subjects with elevated liver enzyme levels even within normal range should be considered at high odds for MetS. This odds for subjects in the fourth quartile was approximately two- and three-fold for ALT and GGT respectively, in fully adjusted models. It seems that cutoff level of liver enzymes should be revised at lower level. The updated cutoff levels could help clinicians for possible presence of non-liver-related disorders such as MetS.
The association between MetS and elevated ALT and AST levels within the normal range observed in this research was consistent with the results of a previous relevant study among similar population group. 11 Furthermore, in a cross-sectional study on Korean adults, elevated ALT and AST concentrations were associated with MetS, and the highest quartile of ALT and AST was associated with prevalence of MetS (OR: 7.90 and 3.81, respectively). 12 In a large prospective cohort study in China, subjects in higher quartiles of GGT and ALT in both genders had increased risk of MetS. 24 In another study of Chinese adults, serum ALT level even within the reference range was significantly associated with the prevalence of MetS. However, there was no relationship between MetS and AST levels within the reference range. AST levels were positively associated with MetS only in elevated levels. 5
A limited number of previous studies have assessed association between the MetS and ALP.11,13,14,21,22,26 In a cross-sectional study in Thailand, elevated ALP was associated with MetS, and participants in the highest quartile of ALP had a 3.72-fold increased risk of MetS. 21 Also, in study of Hanley et al., subjects had a higher risk of MetS in the upper quartile of ALP compared with those in the lowest quartile (OR: 2.28, 95% CI: 1.24–4.20). 26 In study of Taki in Japan, MetS was significantly associated with elevated ALT (OR: 3.37, 95% CI: 1.19–9.52), elevated GGT (OR: 4.96, 95% CI: 2.31–10.66), and elevated C-reactive proteins levels (OR: 2.77, 95% CI: 1.20–6.41). The researchers found no significant relationship between MetS and elevated AST and ALP levels. 22
The relationship between MetS and elevated liver enzyme levels has not been fully elucidated, but there are several potential mechanisms: The most probable explanation is excess fat deposition in the liver, which is a characteristic symptom of NAFLD. Clinically, the most common etiology of elevated ALT level is NAFLD. 5 Excess fat deposition in the liver has detrimental effects on components of the MetS and is considered to be associated with metabolic disorders, including obesity, hypertension, hyperglycemia, and dyslipidemia, which are the components of the MetS.5,27 Furthermore, central obesity may increase insulin resistance due to increased expression of proinflammatory adipocytokines and decreased expression of insulin-sensitizing and anti-inflammatory adiponectin. 21 GGT is a marker of oxidative status. Increased oxidative stress could be involved in reduced responsiveness to the insulin and ultimately causes hyperglycemia. 28 Another possible mechanism is vascular calcification due to increased level of bone-type ALP in vascular smooth muscle cells that may play a role in the progress of hypertension. 29
This study has strengths and limitations. One of the main strengths of our study included the population-based design with a large sample size and extensive data for potential confounders (e.g., life style, demographic variables, etc.). Unlike some pervious investigations, the use of hepatotoxic drugs that could influence liver enzyme levels was considered as a confounder.
However, a limitation of this study is the cross-sectional design where both cause and consequence variables were assessed at one time. So, the cross-sectional nature of the study did not allow deriving any causal inferences and the possible role of elevated values of liver enzymes in developing MetS. It is suggested that this relationship be re-evaluated in the follow-up phase of this study. Because of the budget shortage, the blood parameters were assessed only once. More important, serologic data to exclude participants with viral hepatitis that could influence liver enzyme levels were not available. In addition, fatty liver disease was determined by asking patients if they had ever been diagnosed with this disease not based on imaging.
Conclusion
MetS was associated with increased levels of liver enzymes even within the normal range. These results indicated the potential of elevated liver enzymes as biomarkers for the possible presence of MetS.
Footnotes
Acknowledgements
We thank the people who participated in the study, the study-site personnel, and members of the Rafsanjan cohort center in Rafsanjan, Iran.
Author contributions
ZJ and AEN designed the study and supervised the project. FK and MA collected the data. FA prepared Tables 1–3. PK performed the statistical analysis. ZJ and PK wrote the initial paper. CLV revised the paper. All the authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Iranian Ministry of Health and Medical Education has contributed to the funding used in the PERSIAN cohort through Grant no 700/534. This study has also been supported by the Vice Chancellery for Research & Technology of Rafsanjan University of Medical Sciences. The context of this article are the views of the authors and the funder had no role in design of the study and collection, analysis, and interpretation of data, decision to publish and writing the manuscript.
Ethics approval and consent to participate
The ethics committee of Rafsanjan University of Medical Sciences approved this study (Ethical codes: ID: IR.RUMS.REC.1400.044). Written informed consent was obtained from the participants. The data of Participants kept confidential and were only accessible to the study investigators.
Consent for publication
Not applicable.
Availability of data and materials
The datasets used during the current study are available on the PERSIAN Adult Cohort Study Center, Rafsanjan University of Medical Sciences, Iran. The data are not available publicly. However, upon a reasonable request, the data can be obtained from the authors.