
Abstract
Cardiac disease in pregnancy is an important cause of maternal morbidity and mortality. In many high-income countries, acquired cardiac disease is now the largest cause of maternal mortality. Given its prevalence in low- and middle-income countries (LMICs), rheumatic heart disease is the most common cause of cardiac disease in pregnancy worldwide and is associated with poor maternal outcome. The diagnosis of cardiac disease in pregnancy is often delayed resulting in excess maternal morbidity and mortality. Maternal mortality review committees have suggested that prompt recognition and treatment of heart disease in pregnancy may improve maternal outcome. Given the similarities between symptoms of normal pregnancy and those of cardiac disease, the clinical diagnosis of heart disease in pregnancy is challenging with echocardiography being the primary diagnostic modality. Focused cardiac ultrasound (FOCUS) at the point of care provides supplemental data to the history and physical examination and has been demonstrated to permit early diagnosis and improvement in the management of cardiac disease in emergency medicine, intensive care, and anesthesia. It has also been demonstrated to be useful in surveillance for rheumatic heart disease in LMICs. The use of FOCUS may allow earlier and more accurate diagnosis of cardiac disease in pregnancy with the potential to decrease morbidity and mortality in both developed and developing countries.
Keywords
Cardiac disease with associated morbidity and mortality is an increasing problem in the pregnant patient. Focused cardiac ultrasound (FOCUS) has been demonstrated to improve the diagnosis and management of cardiac disease by non-cardiologists in a variety of clinical settings.
The emerging evidence for the use of cardiac ultrasound in pregnancy is reviewed.
Further research is needed to study the impact of FOCUS on cardiac morbidity and mortality in pregnancy. The increasing use of FOCUS in pregnancy is anticipated particularly in low- and middle-income countries.
Introduction
Focused cardiac ultrasound (FOCUS) refers to the use of ultrasound usually at the point of care to provide information about cardiac structure and function that is supplemental to data obtained by the history and clinical examination. 1 It has been demonstrated to improve the accuracy of clinical assessment and to allow for the evaluation and management of patients with suspected cardiac disease. 2 The utility and benefits of FOCUS have been demonstrated in several specialties including emergency medicine, intensive care, anesthesiology, and general medicine. 3
Cardiac disease is an important cause of maternal morbidity and mortality around the world. 4 In high-income countries (HICs), improved maternal care has reduced the incidence of the direct causes of maternal morbidity and mortality (such as postpartum hemorrhage and maternal sepsis), and cardiac and vascular diseases have risen to become the most common etiologies of maternal mortality.5,6
Low- and middle-income countries (LMICs) are also beginning to see a similarly increased burden of maternal morbidity and mortality as demographic transition and an increased prevalence of cardiovascular risk factors have fueled a rise in chronic noncommunicable diseases.7,8 Unfortunately, resource constraints in both physical and human capital worsen the impact of cardiac disease in pregnancy in these countries. Technological innovations that allow the delivery of care at low cost and that can lessen the need for highly trained specialists may allow for improvement in maternal outcome in these LMICs.
Cardiac disease in pregnancy
Cardiac disease occurs in 1%–4% of pregnant patients. 9 Congenital heart disease remains the most common cause of heart disease in pregnancy in the United States and much of the developed world 10 ; however, the incidence of other forms of cardiac disease particularly cardiomyopathies and coronary disease has risen. This rise is related to the increased prevalence of chronic noncommunicable diseases and the increasing ages at which women are becoming pregnant.11,12 Such acquired heart disease is more lethal than congenital heart disease in pregnancy and is responsible for the majority of maternal cardiac mortality in most developed countries.12–14
The epidemiology of cardiac disease in pregnancy in LMICs has large data gaps particularly for the African continent. Watkins et al. report that in South Africa valvular heart disease is the most common cause of cardiac disease in pregnancy, followed by cardiomyopathies and congenital heart disease. 15 Hu et al. report that in China congenital heart disease is most common followed closely by rheumatic heart disease, 16 while data from India suggest that up to 69% of cardiac disease in pregnancy may be secondary to rheumatic heart disease. 17 On a worldwide basis, rheumatic heart disease is the most common form of heart disease in pregnancy and unfortunately a significant portion of these patients are diagnosed during the antenatal period often presenting with acute cardiac disease.10,18
Maternal morbidity/mortality secondary to cardiac disease
Worldwide, maternal mortality has been recognized as an important public health issue and efforts to reduce this have occurred at international and national levels. Much progress has been made in reducing mortality attributable to the direct pregnancy complications including hemorrhage, maternal sepsis, and eclampsia/preeclampsia. 19 With this progress however, cardiac disease has risen to be the largest cause of maternal mortality in HICs including the United States, the United Kingdom, and the Nordic countries where cardiac disease represents 17%–30% of maternal deaths.14,20,21 The European Registry on Pregnancy and heart disease has found that structural heart disease including congenital heart disease, cardiomyopathies, coronary artery disease, and valvular heart disease resulted in a maternal mortality rate of 1% compared with a maternal mortality rate of 0.007% in women who do not have structural heart disease. 4 In developed countries, the majority of cardiac deaths in pregnancy are a result of acquired heart disease with congenital heart disease representing only 2.8% of deaths.7,13,14
Obtaining accurate maternal mortality data from LMICs is challenging; however, most of these countries report falling direct causes of maternal mortality with an increasing proportion of deaths resulting from indirect causes including cardiac disease. 7 In many of these countries, direct causes of maternal mortality remain more frequent than cardiac causes. 7
Cardiac disease in pregnancy is also an important cause of maternal morbidity. Morbidity figures vary quite widely and appear to be lower in HICs. 4 Pfaller et al. 22 from the Carpreg (Canadian Cardiac Disease in Pregnancy) group reported an incidence of serious cardiac events in 1313 pregnant women of 3.6% (cardiac death or arrest, heart failure, arrhythmias, and urgent interventions). Magun et al. 23 showed that 8.8% of high-risk pregnancies managed by a cardio-obstetric team in New York City required ICU admission for delivery. The European registry on pregnancy and heart disease involved 28 countries and reported on a cohort of 1321 pregnant women with known heart disease prior to pregnancy. They found that 26% of patients were admitted into the hospital during the antenatal period, with the majority of admissions being for cardiac reasons. 4 Lumsden et al. 24 found that at a national referral hospital in Kenya congestive heart failure occurred in 42% of patients with predominantly rheumatic heart disease. Studies in India have suggested that patients with rheumatic heart disease in pregnancy have high rates of morbidity with atrial fibrillation, pulmonary edema, and a need for valve intervention.17,25
Most often pregnant women with cardiac disease in pregnancy have been diagnosed prior to becoming pregnant. In these women, risk assessment tools exist to quantify risk, direct appropriate management, and to hopefully improve outcomes.26–28 However, in both HICs and LMICs, a significant number of patients are diagnosed either during the antenatal period or in the 1 year following pregnancy. In these cases, retrospective studies that have reviewed maternal mortality and its causes have suggested that the diagnosis of cardiac disease in pregnancy is often delayed and this delay often results in excess morbidity and preventable mortality.13,29–31
In a study of cardiac disease in pregnancy from a tertiary hospital in Kenya, researchers found that roughly half of these patients with cardiac disease (55.7%) were diagnosed prior to pregnancy. Of those not known to have heart disease prior to pregnancy, the vast majority (86%) were diagnosed in the third trimester or after delivery. 24 Campanharo et al. 32 in a review of complications in pregnancy in Brazilian women noted that of patients with heart disease 17% were diagnosed during pregnancy. This subgroup of women accounted for 48% of all cardiac deaths during pregnancy.
Current efforts to reduce pregnancy-associated cardiac mortality
Given the trend of increasing pregnancy deaths in the United States, efforts are being directed to reducing this mortality.9,33 State Maternal mortality review committees along with the Centers for Disease Control suggest the opportunity for mortality reduction with early intervention.12,13,34 Studies have suggested a significant number of cardiac pregnancy-related deaths occur in patients who were not known to have heart disease prior to pregnancy.12,24,32 As noted above, studies have also demonstrated the association of cardiac pregnancy-related deaths with incomplete, delayed, or inappropriate diagnosis of cardiac disease in pregnancy.13,33 In peripartum cardiomyopathy, a delay in diagnosis has been found to be related to adverse events. 31 Given these findings, early detection and prompt intervention have the potential to reduce pregnancy-associated mortality. Reports have suggested the opportunity to prevent 50% of pregnancy-associated cardiac mortality and serious cardiac clinical events in pregnancy. 22 Given that cardiac disease in pregnancy is the most common cause of pregnancy-related death in many countries, efforts to reduce the impact of cardiovascular disease on pregnancy outcomes are warranted.
The state of California has had success in reducing pregnancy-associated mortality through the California Maternal Quality Collaborative. 33 They have developed a toolkit which integrates symptom-based clinical assessment and management strategies in an attempt to reduce mortality from cardiac disease in pregnancy. Validation of this toolkit has suggested that 88% of patients who died of cardiovascular causes could have been identified by this algorithm. 33 Patients with abnormal findings are evaluated further with testing including echocardiography and maternal–fetal medicine/primary care/cardiology consultation. It has been documented that when compared with echocardiography, the use of clinical symptoms and signs is less sensitive for the diagnosis of cardiac disease.2,35 The evaluation of possible cardiac symptoms in a pregnant patient is also challenging. It is suggested that by making FOCUS available at the point of care, an improvement in the initial diagnostic accuracy can be made and an expedited evaluation by maternal–fetal medicine or cardiology can be obtained. This has the potential to improve maternal outcome and reduce cardiac pregnancy-related mortality.
Where can FOCUS improve maternal outcome?
FOCUS can serve in aiding in the rapid diagnosis of cardiac disease in the pregnant female. It also facilitates the diagnosis of cardiac disease in low-resource environments with limited cardiovascular services. Currently, aside from anecdotal reports, there is limited outcome data for the utility of FOCUS in this setting. This is an opportunity for further research in strategies that may improve maternal morbidity and mortality.
FOCUS can possibly be applied in three scenarios:
(1) Screening for cardiac disease in pregnancy (particularly rheumatic heart disease in LMICs)
(2) Evaluation of antenatal/postnatal patients who have symptoms that may suggest the possibility of cardiac disease
(3) Evaluation of patients who present in extremis, who need urgent evaluation of cardiac structure and function.
Screening for cardiac disease in asymptomatic pregnant women with FOCUS
FOCUS can be applied to screen for the presence of undiagnosed cardiac disease during the antenatal period. Generally, we should screen in scenarios in which there is a relatively high prevalence of disease and where early identification, and management of disease may affect outcome. These parameters may be fulfilled in many LMICs which still have a significant presence of rheumatic heart disease.36–38 Of great concern is the late discovery of heart disease in these patients. For example, in the study from Kenya, 22.6% of patients with rheumatic disease in pregnancy were first diagnosed in the third trimester or in labor and 17% after delivery. The risk of death in patients who have rheumatic heart disease in pregnancy is 10-fold that for controls. Rheumatic heart disease particularly with mitral valve involvement significantly increases the risk of mortality in pregnancy and may be an important factor in the worse outcomes noted in cardiac disease in pregnancy in LMICs. 39
Echocardiography has been used to screen for rheumatic heart disease in LMICs, particularly in pediatric populations.38–40 A few studies have demonstrated that the use of FOCUS in LMICs can identify cardiac disease in antenatal patients without a history of cardiac disease. Otto et al. 41 reported on their experience in screening asymptomatic pregnant females in Eritrea and found that found that 2.3% had valvular changes consistent with rheumatic heart disease. More recently, Nascimento et al. reported their experience screening 1112 asymptomatic women in Brazil. They found an incidence of significant heart disease of 9%. Moderate to severe mitral regurgitation was found in 4.2%, tricuspid regurgitation in 1%, mild left ventricular dysfunction in 0.4%, left ventricular hypertrophy in 0.2%, and suspected rheumatic heart disease in 3.2%. 42 These studies demonstrate that screening is feasible in LMICs.
In HICs where the incidence of rheumatic heart disease is low, there may not be benefit from a screening approach. However, several studies have identified clinical and socioeconomic factors that elevate the risk of being diagnosed with cardiac disease in pregnancy.34,43–46 Whether there may be clinical utility in performing either screening FOCUS studies or formal echocardiograms in these patients remains to be determined.
Use of FOCUS in pregnant women with symptoms of cardiac disease
For patients who are not known to have cardiac disease prior to pregnancy, diagnosis of cardiac disease is often delayed with adverse outcomes for the mother and fetus.12,29 Retrospective maternal mortality reviews have suggested that in many cases of maternal mortality signs and symptoms were present that, if recognized early, offered the opportunity for early treatment and potentially improved outcome.12,13 A retrospective review of maternal mortality in California found that 84% of women who died of cardiac disease in pregnancy had symptoms suggestive of cardiac disease. 12 Of these patients with symptoms only, 61% were referred to cardiologists with only 7% of the referrals taking place in the antenatal period. In 48% of the women, the cardiac diagnosis was made postmortem with only 53% of patients who died undergoing echocardiography prior to death. 12 It is currently felt that a significant amount of maternal cardiac deaths is preventable if cardiac disease is recognized earlier. 13
Algorithms have been developed to aid clinicians in recognizing heart disease in the pregnant female. 33 Given the fact that many symptoms of heart disease are found in a normal pregnancy (such as dyspnea), there is a strong emphasis on obtaining urgent cardiology consultation and echocardiographic imaging. These algorithms serve to identify pregnant women with symptoms concerning for heart disease and to decrease the time between a patient developing symptoms and a cardiac diagnosis being recognized by the obstetric provider. The use of echocardiography as the preferred method of initial imaging is common among these algorithms.
The ability of an obstetric practitioner to perform a FOCUS ultrasound at the point of care may allow for a rapid evaluation of several cardiac conditions, allowing for urgent formal echocardiographic imaging and referral for cardiac consultation. Information that could be obtained rapidly includes left ventricular size and function and the presence of clinically significant valvular heart disease.40,47,48 In LMICs where echocardiographic evaluation may mean a wait of days to months (if available at all), this information could potentially be lifesaving for the pregnant female. In many HICs, non-emergency same day echocardiographic services are not universally available for outpatients. The early identification of structural heart disease may prove useful, even as this needs to be followed with a formal echocardiographic examination.
FOCUS in patients with severe cardiopulmonary symptoms
The least common indication is likely that of the pregnant patient who presents critically ill with hemodynamic collapse, or with severe acute cardiopulmonary symptoms. Although this is a rare occurrence and often times the cause is clinically evident, anecdotal reports in pregnant females 49 along with data from the emergency medicine and intensive care literature have demonstrated the utility of FOCUS in this setting.48,50
Acquiring competence in FOCUS
Numerous reports have attested to the attainment of competency in FOCUS in disparate clinical groups.51–54 Generally, training includes didactic lectures and proctored imaging experience. Skill acquisition can be achieved in a relatively short timeframe with multiple studies showing that 6 h of didactic lectures and 6–10 h of proctored imaging are sufficient for competence in imaging and interpretation. 52 Still unresolved, however, is the ideal minimum number of studies that should be performed under supervision. The American Society of Echocardiography found that “an acceptable level of skill” can be obtained in novice users after 20–30 studies. The European Society of Cardiovascular Imaging has suggested imaging experience of 50 cases including a diverse range of pathologies.54,55
Skill acquisition
In many developed countries, experience in FOCUS is usually obtained during postgraduate training.56–58 Trainees will usually obtain experience in FOCUS imaging that provides information useful for their specialty. There is also an opportunity to acquire skill after formal residency/fellowship training with several professional organizations offering certification. In the context of a hospital, it is possible that these skills may also be acquired with the aid of cardiovascular physicians or other physicians who have previously had training in FOCUS.
The ease of skill acquisition in LMICs is likely to be affected by various factors, including the availability of cardiovascular specialists, funding for equipment purchase, method of delivery of obstetric services, etc. Countries at higher levels of development may find physician imagers playing the prominent role in pathways of skill acquisition. In countries at lower levels of development, much of the obstetric care takes place in low-resource environments. 59 Nonetheless, even in challenging circumstances, FOCUS can be introduced into clinical care in these settings. Nurse imagers have been used to screen for rheumatic heart disease in Fiji. 51 In Brazil, nurses and technicians have been trained to acquire images with remote reading of the images obtained. 38
Waweru-Siika et al. 60 described their experience in establishing a FOCUS training program in a tertiary care hospital in Kenya and elucidated some of the challenges. Training consisted of didactic instruction, 10 mentored studies and 10 studies which were reviewed offline. They found that 3 months after completion of training, review of trainee images found that 75% of scans were reported as good quality. The trainees displayed relatively poor sensitivity 51% and specificity 79% for major cardiac findings. These results are poor when compared to findings in HICs 58 and possible explanations included the absence of pathology during training, lack of consistent performance after training, and limited time for FOCUS studies in busy clinical environments.
In contrast in a program in which nurses performed FOCUS echocardiography for management of patients with congestive heart failure in rural Rwanda, the nurse images displayed competent imaging and interpretation. When compared with a cardiologist, the nurse imagers had sensitivity and specificity, respectively, of 93.8% and 90.1% for cardiomyopathy; 93.8% and 97.5% for mitral stenosis; 86.8% and 89.0% for congenital heart disease; 71.4% and 99.6% for hypertensive heart disease; and 80.0% and 97.7% for isolated right heart failure. 61 An important distinction may have been the level of training that these nurses received. They had over 3 months of training with the performance of 100 FOCUS studies and continuing mentorship once monthly by a visiting cardiologist.
Echocardiographic findings of clinical utility in the pregnant female
A full echocardiographic evaluation is a comprehensive assessment of cardiac structure and function, cardiac hemodynamics, and evaluation of the great vessels that lie in relation to the heart. A FOCUS echocardiographic study is tailored to the clinical information that is useful for the evaluating physician. For a pregnant female, important findings include the following:
(1) Evaluation of the left ventricular size
(2) Evaluation of left ventricular systolic function
(3) Evaluation of the left-sided cardiac valves
In HICs, some studies have found that cardiomyopathies represent the largest proportion of cardiac disease resulting in mortality. 12 The skills of evaluation of left ventricular size and the qualitative evaluation of left ventricular systolic function have been demonstrated to be easily achieved in relatively short timeframes.47,48 For LMICs with a high prevalence of rheumatic heart disease, the effects of rheumatic heart disease on the left-sided cardiac valves are easily recognizable for non-cardiologist imagers. 40 The limited number of images needed for a FOCUS study need only add a few minutes to the clinical encounter to obtain this information. 47
Imaging for a FOCUS study in pregnancy
Cardiac ultrasound is usually performed from “cardiac windows” where the myocardium is directly adjacent to the chest wall. This prevents the attenuation of ultrasound waves by air in the lungs or obstruction by the ribcage. The cardiac windows used in routine cardiac ultrasound are the left parasternal, apical, subcostal, and suprasternal. 62 The subcostal views are usually not available in the gravid abdomen of late pregnancy. For the obstetric patient, left ventricular size and systolic function along with the morphology and flow across the left-sided valves (which are most commonly affected by rheumatic heart disease) should be the initial aim of imaging. For the novice imager, it may be best to have a mental template of normal findings with abnormal findings prompting referral for formal echocardiography or initiation of acute management depending on resources available and the clinical context. We believe that the views most likely to be of use in obstetric FOCUS are the left parasternal and apical windows.
The left parasternal windows
The left parasternal window is located to the left of the sternum in the fourth or fifth intercostal space, with the ultrasound probe pointed toward the right shoulder as shown in Figure 1. In this view, the heart is imaged along its long axis with visualization of the proximal and mid-left ventricle, the left atrium, the right ventricular outflow tract, the mitral valve, and the aortic valve as demonstrated in Figure 2, Supplemental Videos 1 and 3. Rotation of the ultrasound probe by 90° displays short axis views of the left ventricle (see Supplemental Video 4), left atrium, outflow portion of the right ventricle, mitral, and aortic valves. The aortic and mitral valves are normally well seen in this window, along with the morphologic changes/valvular flow abnormalities that would suggest rheumatic heart disease. 63 Qualitative assessment of aortic and mitral valve regurgitation and global left ventricular systolic function is easily obtained. The parasternal windows are the easiest for inexperienced sonographers to image.47,64

Imaging in the left parasternal window with the probe adjacent to the sternum in the left fourth intercostal space.
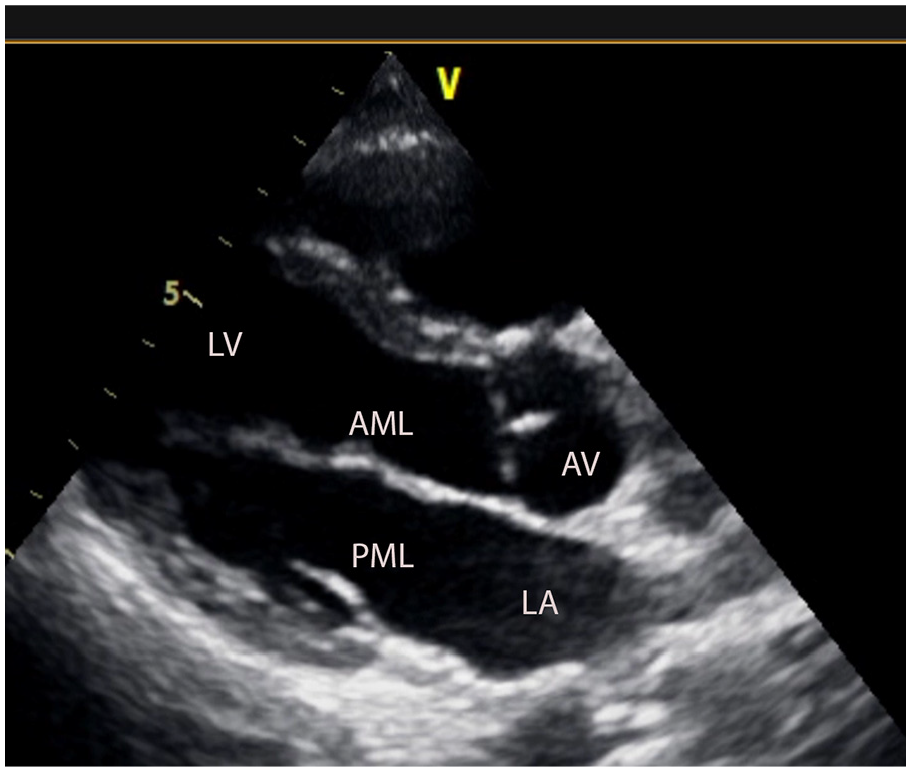
Image from the left parasternal long axis view demonstrating normal mitral and aortic valves and a normal sized left ventricle.
The apical windows
The apical windows are imaged from the cardiac apex. This is normally the point of maximum cardiac impulse on the chest wall (usually in the fifth intercostal space in the midclavicular line) as demonstrated in Figure 3. The heart is imaged along its long axis. By rotation of the probe around the long axis of the heart, the three-dimensional heart can be imaged in a number of two-dimensional slices allowing assessment of all four chambers, the mitral, aortic, and tricuspid valves as shown in Figure 4, Supplemental Videos 2 and 5. Quantitative evaluation of left ventricular function is obtained in these views, along with Doppler evaluation for regurgitation and stenosis of the mitral and aortic valves.62,65 These views are more challenging for the novice sonographer; however, studies have found that within relatively short timeframes, non-cardiologists can become competent in acquiring images.47,66

Imaging from the apical window with the probe at the cardiac apex.
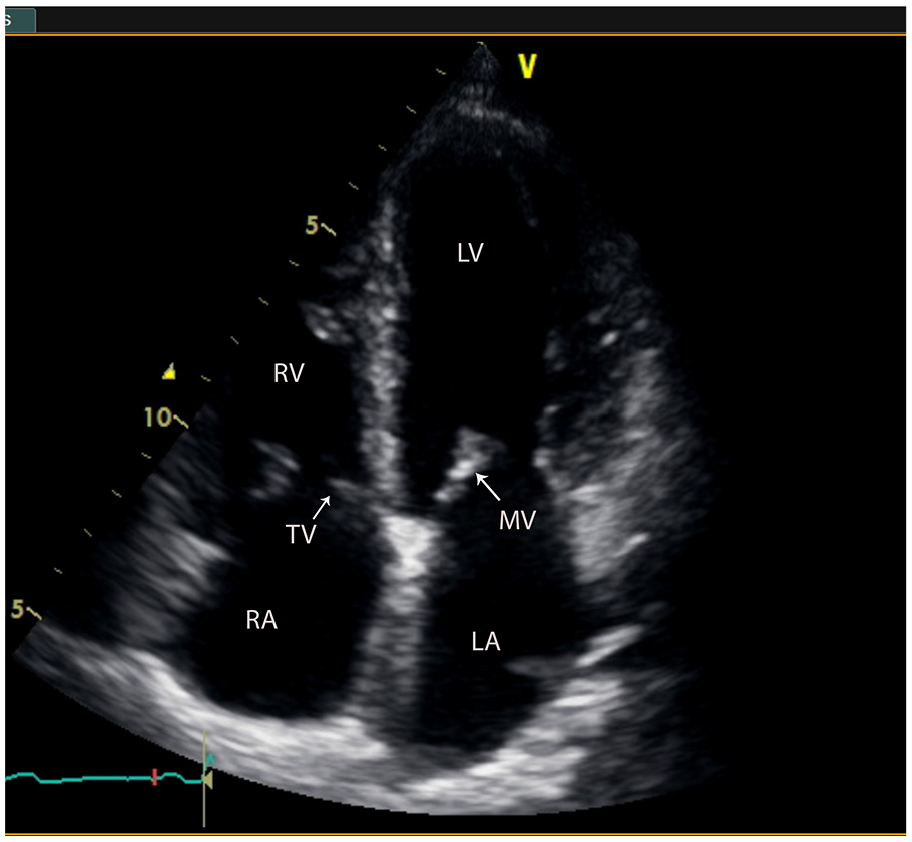
A normal four-chamber view. The four cardiac chambers are seen along with the mitral and tricuspid valves.
Imaging in the second and third trimesters of pregnancy
A potential concern for the use of FOCUS in pregnancy is the quality of images that will be obtained, as in the general population increasing weight has been correlated with poor image quality. 67 Jain et al. found in their study of the feasibility of FOCUS in late pregnancy that in 40 patients with a gestational age of greater than 37 weeks, all patients had image quality sufficient for diagnosis, with 97% of images being of good or high quality. 68 They hypothesize that cranial displacement of the diaphragm displaces the heart anteriorly and laterally (which would have the effect of bringing the heart closer to the ultrasound probe). Other echocardiographic studies have confirmed the feasibility of imaging of the heart in late pregnancy.69,70
Evaluation of left ventricular systolic function
Evaluation of left ventricular systolic function is one of the most common indications for echocardiography. FOCUS has been demonstrated to significantly improve the diagnosis of congestive heart failure or valvular heart disease when compared to clinical evaluation. 2 An important aspect of this is the evaluation of left ventricular size and systolic function. Left ventricular systolic function can be evaluated qualitatively or quantitatively. The quickest and easiest evaluation is by a visual estimation of left ventricular systolic function. This can be done in a binary manner (normal or reduced systolic function), 71 semiquantitative (normal, mildly reduced, moderately reduced, or severely reduced), 72 or experienced observers may visually estimate the ejection fraction. 73 The major advantage of visual assessment is that evaluation of left ventricular function can be achieved with reasonable accuracy when compared to cardiology readers or quantitative methods, it can be performed rapidly in a busy clinic setting or in a critically ill patient and it is less dependent on image quality than quantitative measurements. An example of normal left ventricular systolic function is shown in Supplemental Videos 3–5.
Quantitative measurements are routinely performed in formal echocardiography by calculating left ventricular systolic and diastolic volumes and deriving an ejection fraction. This is done by the modified Simpson’s method which requires tracing of the endocardial border during systolic and diastolic in orthogonal views.65,74 Volumetric discs are calculated which can be summed to generate left ventricular volumes and derive an ejection fraction. This method does require good endocardial definition which may not be available in all patients and takes more time than visual estimation. Simpler methods which require less measurements, but which make geometric assumptions about the ventricular shape can also be used with good accuracy in many patients however may be inaccurate in patients with irregularly shaped ventricles or wall motion abnormalities. 65 FOCUS can also be used to provide hemodynamic information including cardiac output, cardiac filling pressures, and pulmonary pressures. 75 Cardiac output measurement from the suprasternal notch window can be quickly performed in pregnancy and may have prognostic value for fetal outcome in patients with advanced maternal age. 76 Potentially, this approach could also be useful in the bedside management of critically ill pregnant patients.
Given the potential use cases of screening, evaluation of cardiac symptoms in the clinic setting, labor, and delivery suite or in remote areas in LMICs, we believe that competence in acquiring the parasternal and apical windows would be ideal. This would allow for recognition of rheumatic heart disease and evaluation of left ventricular systolic function. For assessment of left ventricular systolic function, visual estimation of the ejection fraction should provide enough information for bedside decision-making as opposed to quantitative measurements. It may be easiest for novice imagers to image the left-sided cardiac valves and decide if they look normal or abnormal, with abnormal patients going on to formal echocardiographic studies. Similarly, in assessing left ventricular size and function, the distinction between normal and abnormal should be sufficient for bedside decision-making. Physicians who work in obstetric critical care who need to manage critically ill patients or who have greater interest can develop more advanced imaging techniques.
Barriers to implementation
Efforts to improve maternal outcome by identifying and managing cardiac disease earlier have suggested the need for early imaging of the heart with echocardiography as the most suitable modality for most patients. We believe that putting this skill into the hands of those directly responsible for the clinical care can potentially lead to important benefits. There will however be challenges to this introduction and these challenges will likely be different in HICs as opposed to those in LMICs. In both scenarios, skill acquisition is an important first step.
In HICs, there is a trend toward the introduction of portable ultrasound imaging and interpretation skills both in initial medical training and in selected specialties.52,57,77 Physicians undergoing obstetric residency are uniformly exposed to ultrasound imaging of the abdomen and female genital tract. 78 It should be possible to include sufficient exposure to FOCUS over the training period so that graduating physicians have acquired this skill set. This will however require changes to syllabi, finding those with skills to teach and having an informal or formal method to evaluate competency.
For physicians who have completed residency, training skill acquisition will likely be more challenging. There are however programs through which FOCUS imaging can be learned. This will, however, require time away from clinical practice and testing to prove competence. At the hospital level, academic and large nonacademic hospitals may have the ability to provide skill acquisition to interested providers. In the context of the United States, there may be possible concerns regarding billing issues as a FOCUS study is considered part of the physical examination and therefore reimbursement may not be possible in the current environment. This may also result in revenue loss for imaging departments which may not be recoverable. There may also be a need to purchase portable or handheld ultrasound machines although in some settings if ultrasound machines are located in clinics, the solution may be as simple as probe and software upgrades.
As challenging as introduction of FOCUS is in HICs, these difficulties are magnified greatly in LMICs, particularly those with poorly developed healthcare systems. These countries generally have limited amount of specialty physicians, which make skill acquisition challenging. There are many problems that will need to be addressed including training an adequate number of imagers to deliver care and ensuring that imaging competence is maintained. Another challenge is that there are high volumes of patients in clinic where even a few additional minutes per patient may not be available. Handheld portable echocardiography machines which are available at a relatively low cost in developed countries are prohibitively expensive in LMICs. The absence of consistent power supply and medical consumables are also perennial problems in many of these countries. Lastly even as abnormalities are identified on FOCUS, then these countries may lack resources to perform formal echocardiography or prompt referral for appropriate management.
Conclusion
FOCUS has demonstrated clinical usefulness in several aspects of clinical medicine. The importance of cardiac disease in pregnancy as a cause of maternal morbidity and mortality worldwide is increasingly being recognized. Echocardiography plays an important role in the diagnosis and management of cardiac disease in pregnancy. FOCUS imaging skills can be relatively easily acquired, particularly if they form part of initial training. The use of FOCUS at the point of care by obstetric providers has the potential to allow for earlier diagnosis of heart disease in pregnancy and particularly in LMICs to expand the reach of cardiac testing. Further research will be needed in the future to evaluate whether deployment of FOCUS can result in improved maternal outcomes.
Supplemental Material
sj-docx-1-imj-10.1177_10815589221142195 – Supplemental material for Focused cardiac ultrasound in pregnancy
Supplemental material, sj-docx-1-imj-10.1177_10815589221142195 for Focused cardiac ultrasound in pregnancy by Paul Edwards, Chinyere Anyaogu, Kenechukwu Mezue, Dainia Baugh, Ahmed Goha, Obiora Egbuche, Felix Nunura and Ernest Madu in Journal of Investigative Medicine
Footnotes
Authors’ note
Echocardiographic imaging was performed on a pregnant female as part of her clinical care. She had signed a general consent to allow the use of her images. She returned to the Heart Institute for her routine cardiology follow-up. At that time, further imaging was performed to minimize the appearance of the patients face and to exclude the brand/identifying features of the ultrasound machine. She was able to review the article/images and to sign the BMJ consent form.
Author contributions
Dr Paul Edwards: Conducted a review of FOCUS literature. Oversaw preparation of second half of manuscript with FOCUS ultrasound and applicability to the pregnant female.
Dr Chinyere Anyaogu: Conducted a review of maternal morbidity and mortality, causes and the changes that have been noted over time. She oversaw preparation of the first half of manuscript discussing maternal mortality/morbidity and efforts to improve the same.
Dr Kenechukwu Mezue: Manuscript revision. Reviewed the epidemiologic transition in LMICs, the current status of rheumatic heart disease in Africa. Reviewed the outcomes of rheumatic heart disease in the pregnant female particularly in the african continent and India.
Dr Dainia Baugh: Reviewed the changes in cardiac disease in pregnancy particularly as it relates to the increasing frequency of chronic non-communicable disease and increasing materal age.
Dr Obiora Egbuche: Reviewed the role of echocardiography/FOCUS in the diagnosis of cardiac disease particularly among non cardiologists. Reviewed the training requirements for competence in FOCUS.
Dr Ahmed Goha: Reviewed cardiac disease in pregnancy in LMIC. Reviewed the data supporting FOCUS for the diagnosis of heart disease in low and middle income countries.
Dr Felix Nunura: Reviewed the technical issues of performing a FOCUS ultrasound in a pregnant female, including technical successs rates, echocardiographic windows needed, information which can be obtained. Was the primary cardiologist for the patient imaged in the study and obtained the images used.
Dr Ernest Madu: Senior Author and Guarantor. Reviewed healthcare delivery in low-resource environments and adapting technology for use in low- and middle-income countries.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.