
Abstract
The association between nonalcoholic fatty liver disease (NAFLD) with cardiovascular and cerebrovascular outcomes, as well as their clinical impact, has yet to be established in the literature. This meta-analysis aims to evaluate the association between the NAFLD patients and the risk of atrial fibrillation (AF), heart failure (HF), stroke, cardiovascular mortality (CVM), and revascularization incidence. We performed a systematic literature search using PubMed, Embase, Scopus, and Cochrane libraries for relevant articles from inception until August 2022. A total of 12 cohort studies with 18,055,072 patients (2,938,753 NAFLD vs 15,116,319 non-NAFLD) were included in our analysis. The mean age of the NAFLD patients group and the non-NAFLD group was comparable (55.68 vs 55.87). The most common comorbidities among the NAFLD patients group included hypertension (38% vs 24%) and diabetes mellitus (14% vs 8%). The mean follow-up duration was 6.26 years. The likelihood of AF (risk ratio (RR), 1.42 (95% CI 1.19, 1.68), p < 0.001), HF (RR, 1.43(95% CI 1.03, 2.00), p < 0.001), stroke (RR, 1.26(95% CI 1.16, 1.36), p < 0.001), revascularization (RR, 4.06(95% CI 1.44, 11.46), p = 0.01), and CVM (RR, 3.10(95% CI 1.43, 6.73), p < 0.001) was significantly higher in the NAFLD patients group compared to that of the non-NAFLD group. However, all-cause mortality was comparable between both the groups of patients (RR, 1.30 (95% CI 0.63, 2.67), p = 0.48). In conclusion, the patients with NAFLD are at increased risk of AF, HF, and CVM.
Introduction
Nonalcoholic fatty liver disease (NAFLD) is a clinicopathological entity that involves the accumulation of hepatic fat or steatosis without secondary causes such as alcoholism or viral hepatitis. Based on the presence of significant hepatic inflammation and hepatocyte injury with steatosis, often this condition can be termed nonalcoholic steatohepatitis (NASH). 1 NAFLD is the most common cause of liver disease in the western hemisphere and is rapidly becoming globally prevalent. 2 According to a recent study, it has escalated, rising from 25.5% in or before 2005 to 37.8% in or after 2016, with men substantially more likely to have NAFLD (39.7%) than women (25.6%). 3 Studies have reported a prevalence between 10% and 46% in the United States, and a new modeling study predicted it to rise to about 63% by 2030. 4 Biopsy-proven NASH is present in approximately 5%–12% of the U.S. population, and it may progress into cirrhosis and hepatocellular carcinoma.5,6 NAFLD and fibrotic liver disease is presently the leading cause of liver transplantation.7,8 It commonly coexists with other components of metabolic syndrome, including dyslipidemia, obesity, insulin resistance, and overt diabetes, causing its prevalence to be as high as 70%–90%.9,10
Cardiovascular disease (CVD) remains the leading cause of death in patients with NAFLD. 11 The development of atherosclerosis and endothelial dysfunction along with metabolic syndrome, as well as the release of proinflammatory and proatherogenic mediators from the steatotic liver, can be a potential threat for CVD, including coronary artery disease (CAD), cardiomyopathy, cardiac arrhythmias, AF, and stroke in the NAFLD patients.11–13 Few studies have tried to investigate the association between the two. However, the results in nonfatal CVD and fatal CVD have been conflicting. Some recent cohorts have reported a significant increase in the incidence and prevalence of CVD in patients with NAFLD as compared to patients without it.14,15 In contrast, other studies failed to confirm this association. 16 A large-scale study by Alexander et al. investigated about 18 million patients, which consisted of 120,795 patients diagnosed with NAFLD, and reported that, after adjusting for well-known cardiovascular risk factors, NAFLD does not appear to be associated with higher CVD and stroke risk. 17 Hence, we aim to perform a meta-analysis to evaluate the association between the NAFLD patients with cardiovascular outcomes such as atrial fibrillation (AF).
Materials and methods
This meta-analysis was conducted and reported following the Cochrane and PRISMA (preferred reporting items for systematic review and meta-analysis) 2020 guidelines and performed according to established methods, as described previously.18–21 The prespecified study protocol has been registered in the PROSPERO (
Search strategy
We conducted a systematic literature search in the PubMed, Embase, and Scopus using predefined MESH terms by using “AND” and “OR.” The following search terms were used: “NAFLD” OR “non-alcoholic fatty liver disease” AND “atrial fibrillation” OR “Arrhythmia” AND “heart failure (HF)” AND “Cardiovascular mortality (CVM)” AND “stroke” AND “ischemic heart disease” AND “revascularization,” respectively. The search was performed from inception up until August 2022 without any restrictions on language of the studies. All the studies were carefully screened and exported to Endnote 2020 library (Clarivate Analytics, Berkeley, California, USA). Two reviewers (VJ and AJ) reviewed the studies based on the title and abstract. A third author (NB) arbitrated discrepancies regarding the inclusion of studies.
Clinical outcomes
The primary outcome for this meta-analysis was the incidence of AF. The secondary outcome was the incidence of HF, stroke, revascularization, all-cause mortality, and CVM.
Eligibility criteria
We included studies with patients of age ≥ 18 years of age without any restrictions of language barrier. All randomized-controled trials and prospective and retrospective cohort studies were sought to be eligible for inclusion into the study. It was decided to include studies with two arms so that comparison can be made in which g is with the NAFLD group of patients while the other group is with the non-NAFLD group of patients. Those studies compare the patients with varying baseline characteristics and pathologies along with data for outcomes of interest. Any study involving animals, reviews, case reports, case series, studies on patients <18 years, abstracts, studies with single arm without two groups, or studies without outcomes of interest were excluded from the review.
Data extraction and quality assessment
All the included articles were extracted for the following data: study type, author name, location of study, number of patients in both groups, patient characteristics (age, sex, comorbidities, and risk factors), follow-up period, and primary and secondary outcomes. Two investigators (VJ and SN) independently appraised the potential risk of bias for observational studies using the Newcastle-Ottawa scale. 22 We then classified studies as low, moderate, or high quality based on the scores after evaluation.
Statistical analysis
For each included study, the number of patients who developed a primary or secondary outcome was recorded for the NAFLD and the non-NAFLD groups. Baseline continuous variables were summarized in mean (standard deviation), whereas dichotomous variables were described in frequency or percentage. We performed a conventional meta-analysis for primary and secondary outcomes and adopted the DerSimonian-and-Laird and Hartung-Knapp-Sidik-Jonkman random-effect model for the study variations. 23 Outcomes were reported as pooled risk ratio (RR) and their corresponding 95% confidence interval (95% CI). Statistical significance was met if 95% CI did not cross the numeric “1” and the two-tailedp-value was less than 0.05. We considered a two-tailed p-value of less than 0.05 to be statistically significant. In addition, we assessed the between-study heterogeneity using the Higgins I-square (I2) test, with I2 values <75% considered mild-moderate and >75% considered high. 24 We performed a sensitivity analysis by leave-one-out methods for studies with high heterogeneity. Subgroup analyzes based on the follow-up period and sample size were carried out for primary outcome to assess the robustness of the analysis. Assessment of publication bias was via visualization of the funnel plot. 25 All statistical work, inclusive of analysis, and graphical illustrations were conducted using STATA (version 17.0, Statacorp) Lakeway Drive College Station, Texas, USA.
Results
Our initial comprehensive search identified a total of 6452 articles. After exclusion of duplicates (255) and irrelevant (6115) studies based on title and abstract, 82 studies were reviewed in full-text form. However, 72 studies were further excluded based on inclusion criteria. A total of 12 studies qualified for the final analysis,12–14,16,17,26–32 of which 10 were prospective studies and 2 were retrospective studies (Figure 1).
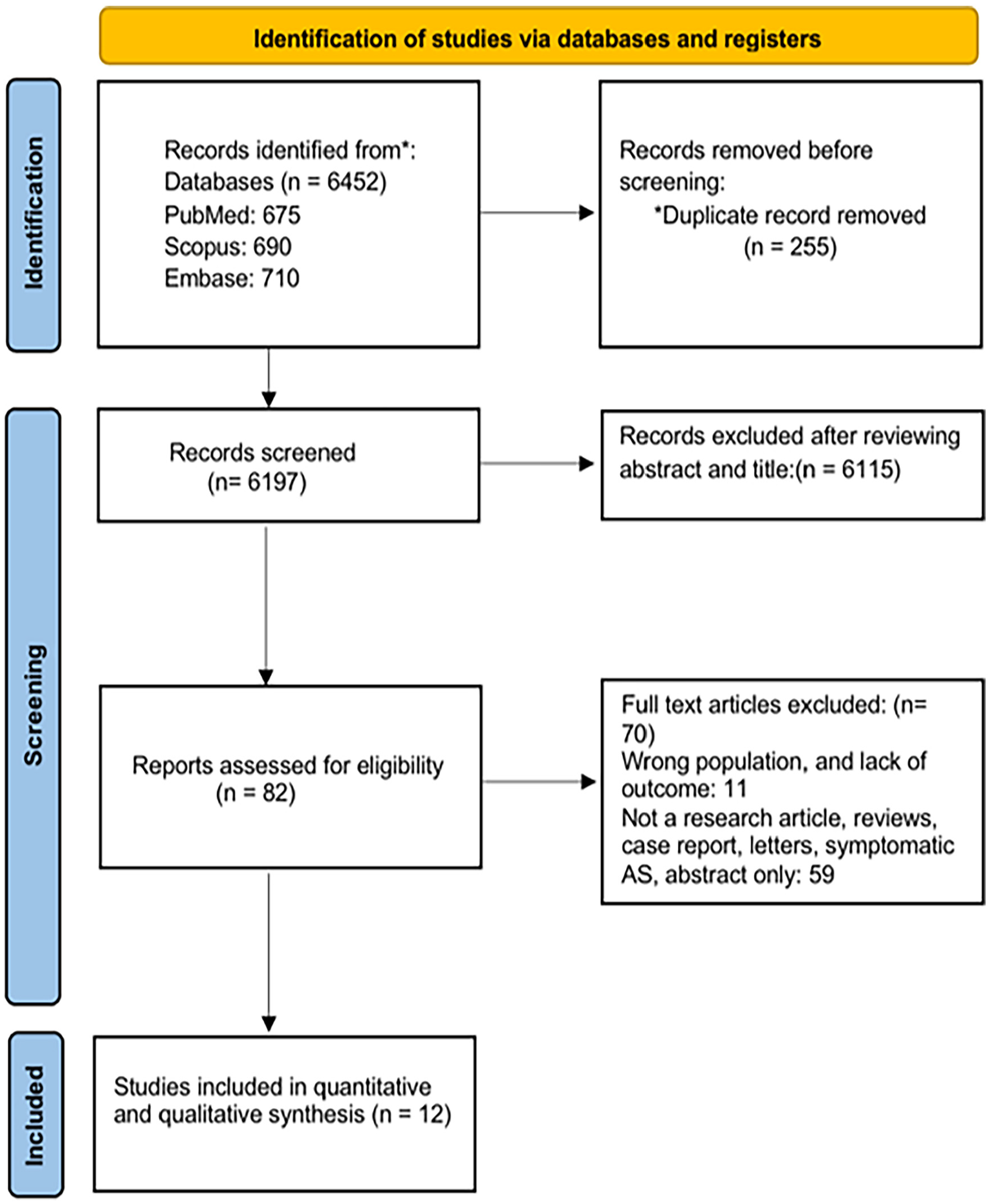
Prisma flowchart of the search strategy for systematic review and meta-analysis.
Baseline patient demographics
A total of 18,055,072 patients (2,938,753 NAFLD vs 15,116,319 non-NAFLD) were included in our analysis. The mean age of the NAFLD patients group and the non-NAFLD group was comparable (55.68 vs 55.87). Number of males in the NAFLD group was higher compared with the non-NAFLD group (72.2% vs 47.2%). Most common comorbidities among patients with NAFLD and non-NAFLD were DM (14.33% vs 7.58%), HTN (37.71% vs 24.39%), and dyslipidemia (28.06% vs 14.50%), respectively. The study characteristics, demographics, and comorbidities are presented in Table 1. The quality assessment of the observational studies was low risk on NOS for all observational studies on bias assessment (Table S1).
Baseline demographics, comorbidities, and study characteristics of studies included in the meta-analysis (arranged in NAFLD/non-NAFLD form).
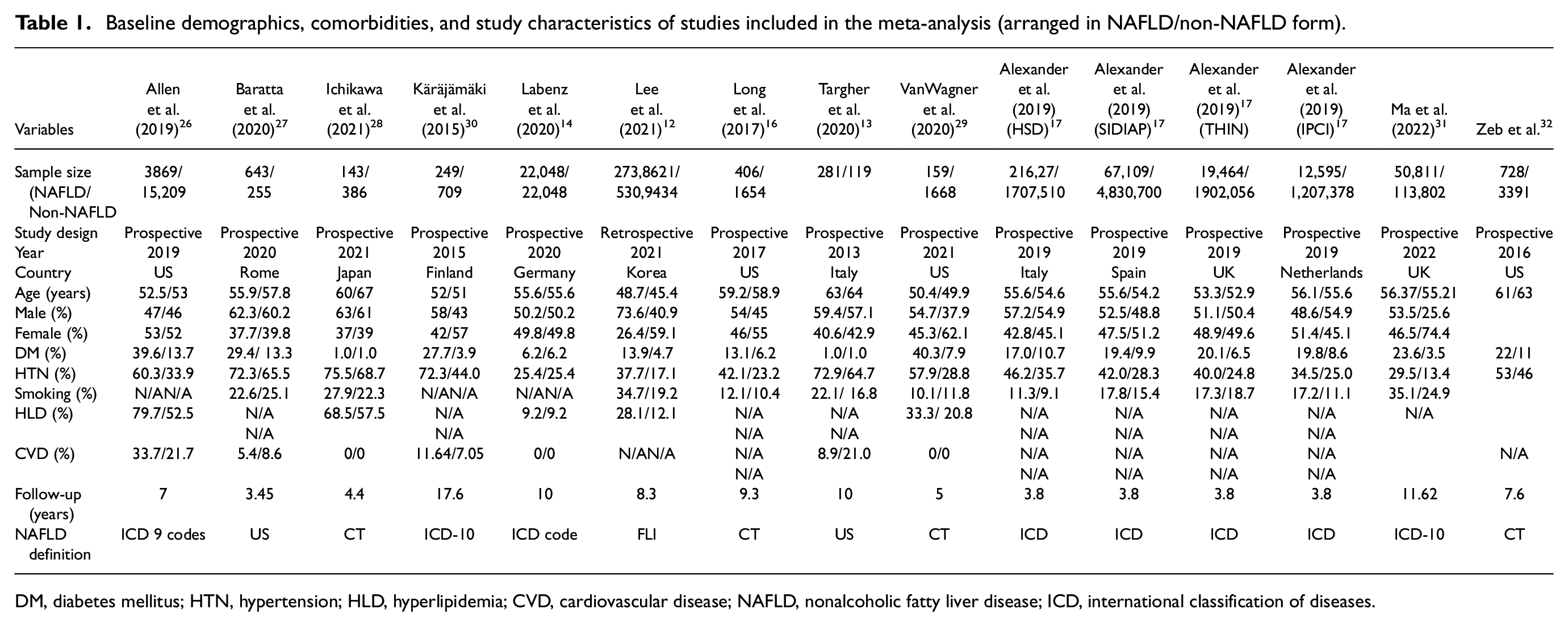
DM, diabetes mellitus; HTN, hypertension; HLD, hyperlipidemia; CVD, cardiovascular disease; NAFLD, nonalcoholic fatty liver disease; ICD, international classification of diseases.
Meta-analysis of outcomes among patients with NAFLD and non-NAFLD
The mean follow-up duration was 6.26 years. The risk of AF (RR, 1.42(95% CI 1.19, 1.68), p < 0.001, I2 = 91%) (Figure 2), HF (RR, 1.43(95% CI 1.03, 2.00), p < 0.001, I2 = 12%), stroke (RR, 1.26(95% CI 1.16, 1.36), p < 0.001, I2 = 64%), revascularization (RR, 4.06(95% CI 1.44, 11.46), p = 0.01, I2 = 8%), and CVM (RR, 3.10 (95% CI 1.43, 6.73, p < 0.001, I2 = 11%) was significantly higher in the NAFLD patients compared to that of the non-NAFLD group. However, all-cause mortality was comparable between both the groups of patients (RR, 1.30 (0.63, 2.67), p = 0.48, I2 = 95%), respectively (Figure 3(a)–(e)).
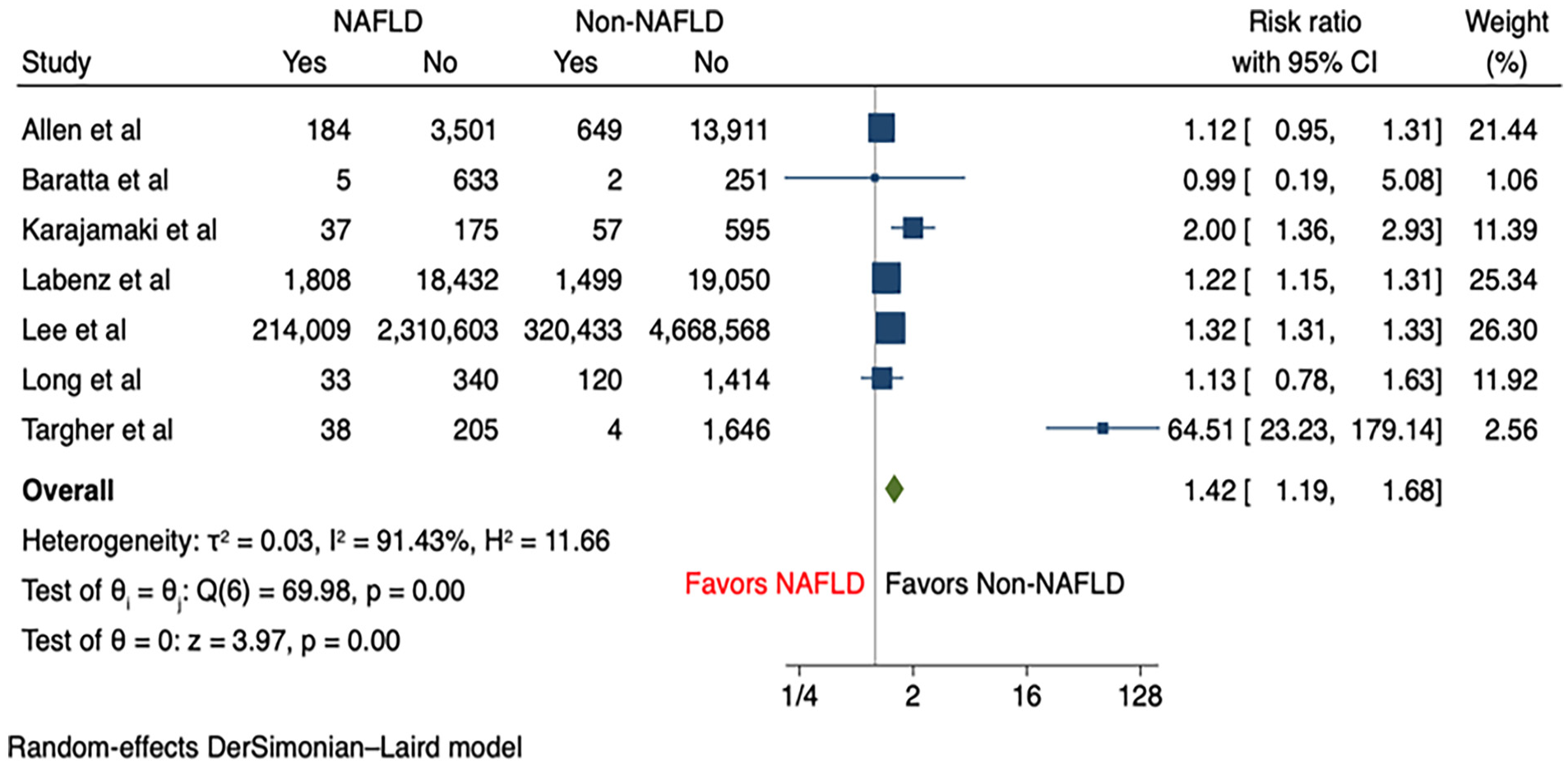
Forest plot of primary outcome: atrial fibrillation.
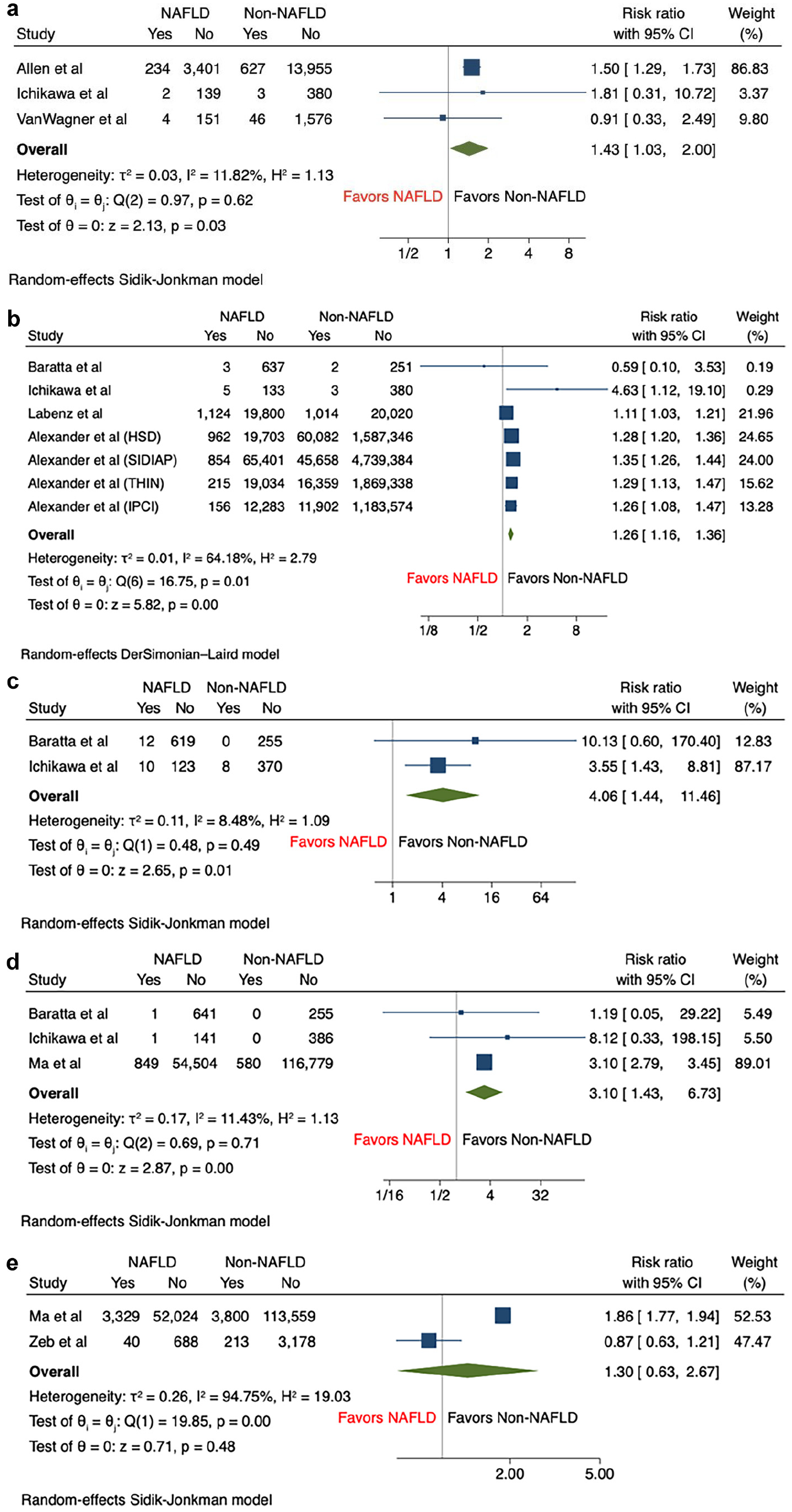
Forest plot for secondary outcomes: (a) heart failure, (b) stroke, (c) revascularization, (d) CV mortality, and (e) all-cause mortality.
Sensitivity analysis
Sensitivity analysis was performed for AF and stroke, given the high heterogeneity observed in the primary analysis. Sensitivity analysis via the leave-one-out method showed that NAFLD remained significantly associated with the increased risk of AF and stroke, suggesting the robustness of the results (Figures S1 and S2).
Subgroup analysis
Subgroup analyzes were conducted for primary outcome based on the follow-up period (<10 years vs ≥10 years) and sample size (<1500 vs ≥1500). It was found that studies with a longer follow-up period (RR, 4.56 (95% CI 1.35, 15.35)) showed a higher incidence of AF among the NAFLD patients compared to studies with a shorter follow-up period (RR, 1.24 (95% CI 1.11, 1.39)), with a significant subgroup difference (p = 0.04) (Figure S3). However, it should also be noted that studies with a shorter follow-up period still showed a significantly higher incidence of AF among the NAFLD patients but with a substantially lower heterogeneity across studies (I2 = 38%), explaining that the heterogeneity observed in the primary analysis was largely derived from studies with a longer follow-up period. Secondly, we observed that there was no significant subgroup difference between studies with a larger sample size against those with a smaller sample size (Figure S4). Nevertheless, it was shown that the heterogeneity among studies with larger sample size (I2 = 69%) is relatively lower than that of studies with a smaller sample size (I2 = 95%), thus partially contributing to the substantial heterogeneity observed in primary analysis.
Publication bias
The assessment of publication bias was performed through the visualization of the funnel plot, and it showed that there was minimal/no funnel plot asymmetry, indicating there was no evidence of publication bias on risk of AF and stroke (Figures S5 and S6).
Discussion
Globally, the prevalence of NAFLD has increased from 25.5% to 37.8% and is projected to continue rising with increases of up to 122% by 2030.3,33 Currently, metabolic syndrome and insulin resistance are the strongest independent risk factors correlated with NAFLD and NASH, which are often exacerbated by a lack of physical activity and a high BMI. 34 Though the pathophysiological mechanisms linking NAFLD and CVD are multifactorial, it is not entirely clear whether these cardiovascular conditions share common pathophysiological mechanisms or whether these factors are causative. Moreover, the variable and inconclusive results of adverse cardiovascular outcomes in NAFLD highlight further need to establish effective prevention strategies. To the best of our knowledge, this is the most comprehensive meta-analysis with the largest sample size, including almost 2 million patients in our NAFLD cohort, to date on a wide range of variables tested (Figure 4).
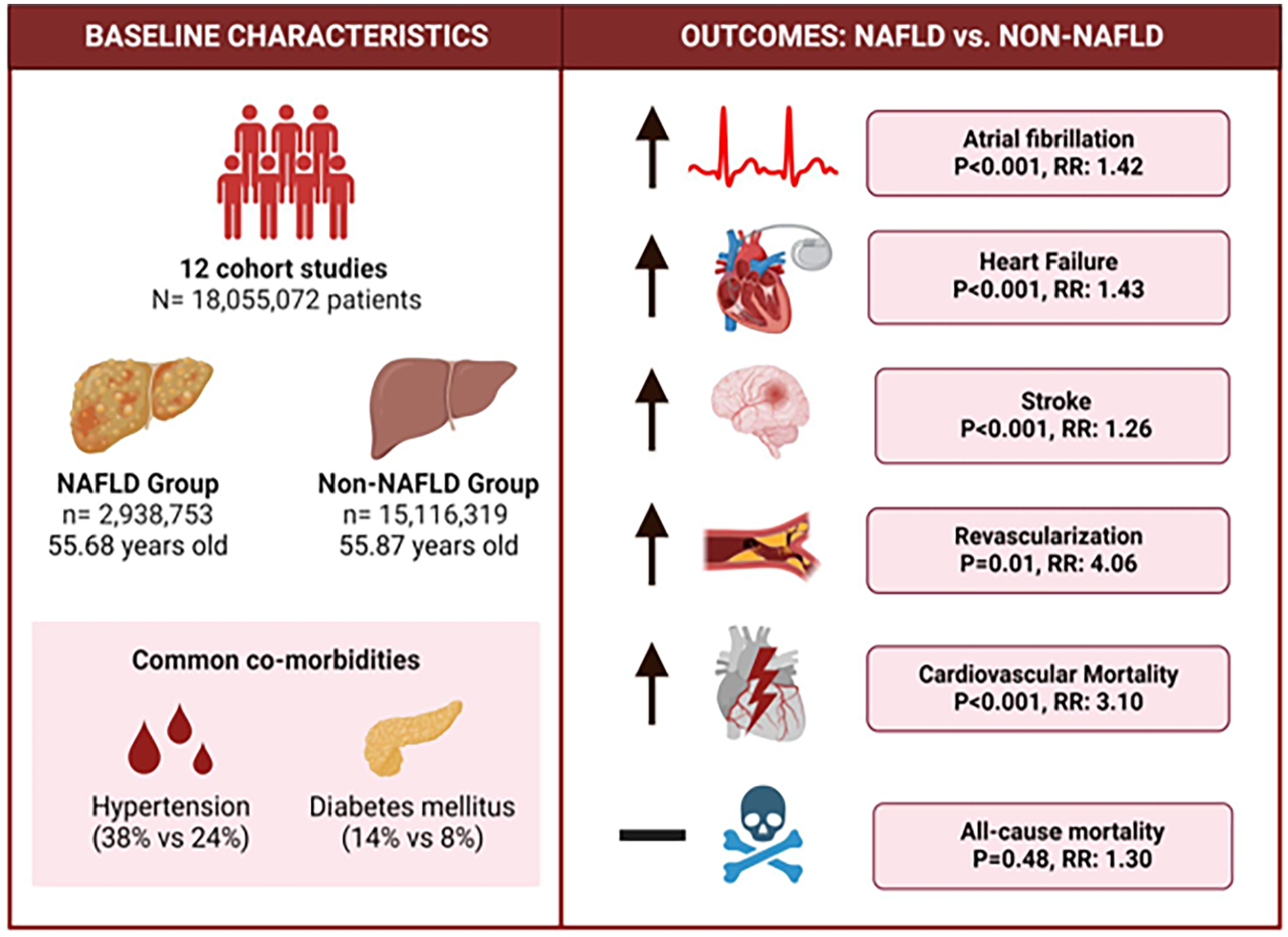
Graphical abstract highlighting key findings among patients with nonalcoholic fatty liver disease (NAFLD) compared with the non-NAFLD patients in terms of cardiovascular outcomes.
The association of NAFLD and nonfatal CVD
Our main findings support that patients diagnosed with NAFLD carry an increased risk of AF, HF, cerebrovascular complications, and peripheral vascular diseases. The OPERA study corroborates with our findings and found the NAFLD patients to have a higher probability of developing AF (Hazard Ratio (HR) 1.96 (95% CI) 1.29, 2.97). 30 Similarly, a correlation was found wherein increased AF risk was more pronounced if patients had a higher fibrosis-4 index score even after adjusting for traditional risk factors of atherosclerosis such as coronary heart disease.35,36 Though the incidence of stroke is proportionally higher in AF and may be tightly linked to adverse stroke events, a previous Chinese cohort study of 79,905 patients confirms our results indicating that NAFLD independently increases the risk of cerebrovascular complications after adjusting for confounding variables. 15
The EUROSTROKE case–control study also found that elevations in gGT, a sensitive marker for NAFLD, were strongly associated with stroke risk without T2DM or established CVD history. 37 The event of new-onset HF was reported to be 1.5 times higher in patients diagnosed with NAFLD compared to healthy liver controls in a recent systematic review, but observational studies that were analyzed were unable to establish a direct causality. 38 HF and AF are well-reported risk factors in the literature that have direct correlations with the progression of fibrosis in the NAFLD patients with or without atherosclerotic history.39,40 As such, it is unique to note that CVM is an extremely variable outcome in the literature with studies citing no differences and other advocating mortality to be significantly increased in NAFLD.41–43 Peripheral artery disease (PAD) has been previously associated with a 92% increase in the risk of fibrotic liver changes (OR: 1.92, 95% CI 1.24, 2.98) and a 3.85-fold increase in fibrosis deterioration in the coexistence of insulin resistance with PAD (95% CI 2.06, 7.18). 44 However, the likelihood of peripheral revascularization is not well documented in previous reviews, and this is the first to be reported as a significant outcome in the literature.
CVM in our study was found to be significantly increased; patients with NAFLD were three times more likely to suffer from CVM compared with healthier individuals. Compared with previous meta-analyzes, this risk in fatal CVD outcomes seems to be the highest in our study irrespective of gender differences.45–47 However, the variable outcomes in mortality remain controversial. For example, a substantial body of text also suggests there are no differences in CVM while other proponents reported a significant increase in all-cause mortality, an outcome that was not a predictor in our results.48–50 This may be largely due to patients being at various stages of hepatic steatosis, as the progression of cirrhosis and fibrosis often translates to increased mortality-related events. 42 This was evident in our subgroup analysis on outcomes for AF, where longer follow-up periods translated to the NAFLD patients at a four times higher risk than the non-NAFLD participants. Moreover, the status of NAFLD participants hospitalized due to CVD-related outcomes and their differences in body weight (i.e., lean NAFLD patients) can influence outcomes in mortality. 51 The discrepancy in results should require more additional investigations, as the large sample size studied in this paper may have inflated the RR.
Pathophysiological mechanisms
CVD can be attributed to a plethora of etiologies that cause NAFLD such as insulin resistance, dyslipidemia, and inflammatory processes that dysregulate adipokine metabolism. 52 The prevalence of NAFLD is often predominantly in older demographics and increases in the presence of diabetes, obesity, or hallmarks of metabolic syndrome. 52 Given that hypertension and diabetes were one of the common comorbidities, it is not uncommon to observe atherosclerotic events that increase the risk of HF, stroke, AF, and PAD. The emergence of evidence in the literature shows that NAFLD is strongly associated with hypertension and can be attributed to multiple pathophysiological changes that cause adverse outcomes. 2 Hepatic fat accumulation can be caused by imbalances in de novo lipogenesis or inadequate fatty acid oxidation, thus increasing the accumulation of hepatic triglyceride and inevitably secreting circulatory VLDL particles to peripheral sites.53,54 The subsequent rise in low-density lipoproteins containing apolipoprotein-B often precipitates the development of atherosclerosis by acting as damage-associated molecular patterns, leading to the chronic production of proinflammatory cytokines (IL-6, TNF-a) and reductions in anti-inflammatory adiponectin. 55 Additional insults from hepatic insulin resistance and abnormal glucose metabolism can further compromises the metabolic cycle and precipitate systemic inflammation.
Though the direct mechanism linking cardiac arrhythmias to NAFLD are unknown, in vivo animal studies have postulated that AF can be precipitated in fatty liver disease due to (1) the production of IL-1beta in the setting of TLR2 inflammasome activation of cardiac macrophages, and (2) the disruption of ion currents due to the deposition of adipocytes in epicardial tissue. 56 Alternatively, inflammatory phenotypes from epicardial fat deposits can destroy microvascular systems and increase pro-fibrotic factors (TGF-b). 57 These alterations can impact the electrophysiological and structural integrity of the myocardium, ultimately leading to AF and HF, respectively. 57 Coupled with vascular endothelial dysfunction and oxidative stress, the precipitation of cardiac remodeling due to myocardial lipid toxicity and fibrosis from ectopic fat deposits may also underlie the progression of new-onset HF.58,59 It is likely that stroke and PAD risk are precipitated by an atherosclerotic occlusion of cerebral arteries and distal femoral arteries, respectively, but the lack of literature establishing this connection warrants future investigations determining its pathology.
CVD prevention
The prevalence and evidence of increased CVD risk makes early prevention and stratification prominent in the general population. The preponderance of NAFLD among all demographics regardless of age, race, and preexisting comorbidities highlights the emerging need for clinicians to create suitable recommendations in clinical practice and requires the usage of risk assessment parameters that capture CVD risk. The adoption of cardioprotective care in NAFLD should focus on lifestyle modifications to manage modifiable risk factors, such as exercise and improvements in blood pressure management. 60 Often, statin therapy is the first-line pharmacological therapy for dyslipidemia, characterized with elevated LDL-C levels above 190 mg/dl, diabetes mellitus, >40 years old, and/or elevated ASCVD scores, as recommended by the 2019 ACC/AHA guidelines. 61 Metformin is also recommended for first-line treatment in diabetic patients and can act as a nidus to CVD prevention, given the strong correlation of insulin resistance to premature atherosclerosis and subsequent CVD outcomes. 62
Though the American hepatology guidelines have addressed the need to modify metabolic risk factors that link the association of CVD with NAFLD, current cardiovascular guidelines have not identified NAFLD as an independent risk factor. 1 Traditional cardiovascular risk factor scores such as the Framingham Risk Score and surrogates such as atheroma formation focus on hypertension and hyperlipidemia as important markers for CVD.63,64 However, select studies have found that certain biomarkers specific for NAFLD can identify CVD risk. The early NHAHES3 population-based study determined that patients with a 10-year risk of cardiovascular events correlated significantly elevated ALT levels to a higher Framingham Risk Score. 65 Moreover, the STABILITY study also found IL-6 levels to be independently associated with the risk of adverse CVD events, a marker that is often correlated with a higher degree of fibrosis and inflammation in NAFLD.66,67 However, it is still undetermined whether these markers are specific or sensitive in clinical practice; for instance, a recent study conducted through the CANVAS program found that though raised γGT was associated with the risk of HF, ALT levels were independently associated with lower risk. 68
Screening protocols should be equipped to identify certain parameters that would indicate increased CVD risk in NAFLD outside of traditional metabolic markers. Currently, the literature has not reached a consensus on the validity of lipid profiles (i.e., LDL-C levels) or liver enzymes in determining CVD risk within the NAFLD population. As a result, there is a need to refine and further investigate the specificity and sensitivity of CVD risk biomarkers related to NAFLD to guide clinical practice. Clinicians should continue to exercise a higher degree of suspicion for CVD events in patients with benign and advanced stage liver fibrosis and should routinely screen for smoking history, diabetes, and hypertension. The need to create stringent guidelines of NAFLD-specific CVD risk scores should be considered in conjunction with traditional markers and can improve risk-stratification tools that would allow for personalized evidence-based management.
Limitations
The major limitation was that the results were derived from observational studies, where confounding bias could not be ruled out. In addition, adjusted estimates were not present in the majority of studies, thus the meta-analysis adjusted for possible confounders would not be possible. While heterogeneity was observed in AF and stroke, sensitivity analyzes confirmed that the results remained robust after exclusion of each study. Further meaningful analytical methods including meta-regression were also limited by the number of studies for each individual outcome. Therefore, further well-designed multicenter studies or randomized-controled trials are warranted to confirm these findings.
Conclusions
Patients with NAFLD demonstrated increased risk of AF, HF, stroke, and CVM. Patients with associated comorbidities were at higher risk of CVD, implying a greater need for screening and adoption of cardioprotective measures amongst the NAFLD patients.
Supplemental Material
sj-docx-1-imj-10.1177_10815589231164777 – Supplemental material for Association between nonalcoholic fatty liver disease and atrial fibrillation and other clinical outcomes: a meta-analysis
Supplemental material, sj-docx-1-imj-10.1177_10815589231164777 for Association between nonalcoholic fatty liver disease and atrial fibrillation and other clinical outcomes: a meta-analysis by Vikash Jaiswal, Song Peng Ang, Helen Huang, Navroop Kaur Momi, Maha Hameed, Sidra Naz, Nitya Batra, Angela Ishak, Neel Doshi, Asmita Gera, Medha Sharath, Madeeha Subhan Waleed, Nishchita Raj and Victor Hugo Aguilera Alvarez in Journal of Investigative Medicine
Footnotes
Author contributions
Disclosure
The abstract of this study’s initial data has been presented in European Society of Cardiology Asia 2022.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval not required as this is a review article
Supplemental material
Supplemental material for this article is available online.
Data availability statement
Data is contained within the article and supplementary material.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.