1. Factors Associated with Kidney Transplant for Persons Living with Human Immunodeficiency Virus
Kyle Crawford1, Ruth Adekunle1
1. Infectious Diseases, Medical University of South Carolina, Charleston, SC, United States.
Purpose of Study: Persons living with HIV (PLWH) with chronic kidney disease are known to progress to end-stage renal disease (ESRD) at faster rates than individuals without HIV. Unfortunately, PLWH experience higher mortality on dialysis compared to the non-HIV population. Kidney transplant is an effective and preferred alternative to dialysis, with post-transplant outcomes similar to the non-HIV population. However, increasing data suggests that PLWH are less likely to be waitlisted for kidney transplant. This study aims to identify and barriers and mediators associated with kidney transplantation candidacy among PLWH at the Medical University of South Carolina.
Methods Used: This was a retrospective review of PLWH and ESRD who either received care at MUSC Health Care System or were referred for Kidney transplant at MUSC. Cases were included if a PLWH and ESRD received care or was referred between May 1st, 2012, and December 31st, 2023, and sufficient data of their transplant process were available in the medical record system. Descriptive statistics were used to analyze demographic and clinical characteristics and the transplant care continuum of PLWH and ESRD at MUSC.
Summary of Results: 156 PLWH and ESRD were included in the analysis. Demographics included 110 (71%) males and 143 (92%) of the Black race. The most common causes of ESRD were HIV-associated nephropathy (52%), hypertension (42%), and diabetes (18%). Most patients had hypertension (96%) and 35% of patients had diabetes, 50% of which were insulin dependent. Other prevalent comorbidities include psychiatric conditions (32%), history of obesity (29%), congestive heart failure (29%), and coronary artery disease (24%). Of the 156 patients, 134 were referred for transplant (86%) with a median age at the time of referral of 49 years (range 25 - 78). Of the original 156 patients, 90 (58%) started a transplant evaluation, 55 (35%) completed the transplant evaluation, 48 (31%) were waitlisted, and 35 (23%) were transplanted. Common reasons why patients did not complete transplant evaluation included failing to complete testing requirements (46%), not meeting HIV criteria for transplant (11%), and having too many comorbidities (17%). The median time from starting dialysis to referral in days was 579 (range 4 – 7169). The median times from referral to evaluation, waitlisting, and transplant in days were 137.5 (range 0 – 3886), 597 (range 11 - 4444), and 1056 (range 17 – 4448), respectively.
Conclusions: The majority of PLWH with ESRD seen at MUSC were referred for kidney transplant and started the evaluation process. However, there was a substantial decrease in the number of patients that completed evaluation. Moreover, PLWH and ESRD had a significant comorbidity load and were often faced with lengthy times associated with each step of the transplant process. More information is needed, though, to assist patients in completing the transplant evaluation process and making it to the transplant waitlist, with the goal of transplantation.
2. Incidence and Risk Factors for Non-AIDS Comorbidities Following COVID-19 in People Living with HIV in Atlanta, Georgia
Cecilia A. Castellano1, Minh L. Nguyen1, Caitlin Moran1, Vijay Ramesh1, Cecile Lahiri1
1. Medicine, Emory University, Atlanta, GA, United States.
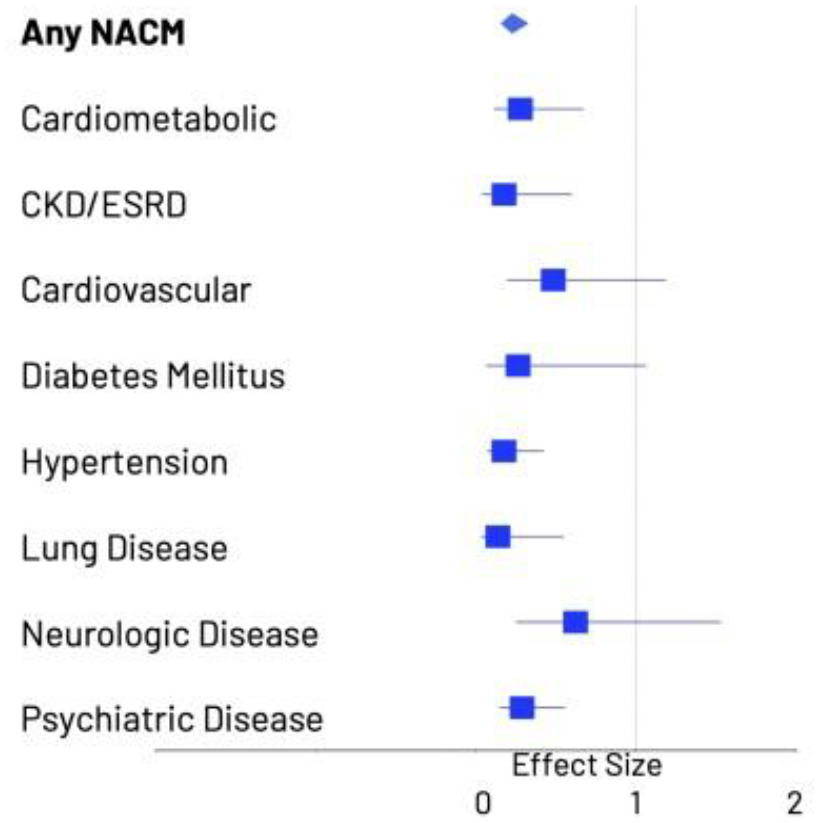
Purpose of Study: Non-AIDS comorbidities (NACM) are increasing in persons living with HIV (PLWH) despite potent antiretroviral therapy (ART). PLWH are infected with SARS-CoV-2 at a rate nearly double that of their seronegative counterparts. Incidence and risk factors for developing NACM following COVID-19 in PLWH remain unknown. We used data from PLWH enrolled in the Emory Centers for AIDS Research (CFAR) Registry who receive care at the Grady Ponce de Leon Center in Atlanta, Georgia to assess incidence, risk factors, and time to development of NACM following COVID-19.
Methods Used: PLWH with documented SARS-CoV-2 infection (by positive SARS-CoV-2 PCR or antigen test) between March 1, 2020, and September 30, 2021, with at least 1 follow-up visit within 12 months were included (COVID+) and compared to PLWH without SARS-CoV-2 (COVID-). Eight categories of NACM were identified using problem list diagnoses and ICD9/10 codes: cardiovascular, cardiometabolic, renal, hypertension, pulmonary, neurologic, and mental health disorders. We used cox proportional hazard regression model to calculate risk of developing incident NACM and assessed potential risk factors by adjusting the model for age, sex, race, CD4+, and HIV viral load.
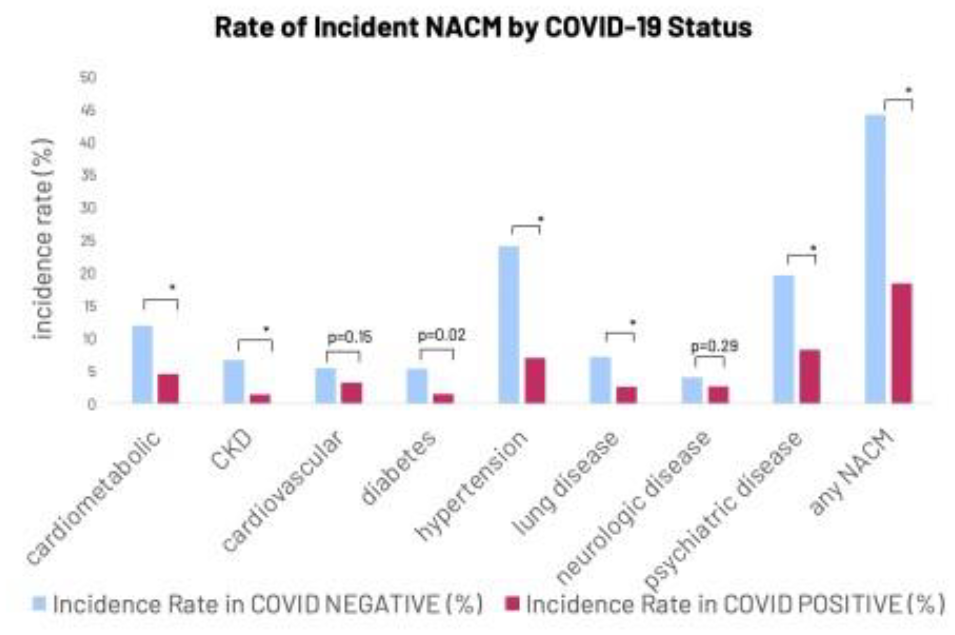
Summary of Results: 3540 PLWH met inclusion criteria, 261 of whom were COVID+ by documented testing. Median age was 50.9 years, most participants were black or African American, male, and had well-controlled HIV. There was a significant difference in NACM burden (number of pre-existing conditions) between COVID groups. When adjusting for age, legal sex, race, CD4+ count, and HIV viral load, the risk for any incident NACM in COVID+ PLWH was 0.224 (0.157, 0.321); findings were similar when assessing each NACM individually. Compared to COVID- PLWH, COVID+ PLWH had a longer median time to development of any NACM: 197 vs 96 days. Median time to event was longer for the COVID+ group for all NACM except for cardiometabolic disease. Women with COVID-19 were at increased risk of developing any NACM (HR = 1.43 (1.26, 1.63), p<0.0001) and were more likely to develop cardiometabolic (HR = 2.03), lung disease (HR = 2.28), and neurologic disease (HR = 1), p <0.0001 for all. Age and female sex were significant predictors for incident NACM overall and in the COVID- group but were not associated with greater risk of incident NACM in the COVID+ group.
Conclusions: PLWH with COVID-19 had a lower incidence rate and a longer time to development of any NACM compared to PLWH without COVID-19. PLWH with COVID-19 had a higher burden of NACM at the start of the study, indicating they were sicker and minimizing the possibility of developing new NACM as they had already many comorbidities. Healthier PLWH who did not get COVID-19 may have had more interaction with the healthcare system and more opportunities to be diagnosed with NACM. Longer follow-up of these patients is warranted to better understand the long-term impact of COVID-19 on NACM in PLWH.
3. Bacterial Small RNAs May Mediate Immune Response Differences Seen in Respiratory Syncytial Virus versus Rhinovirus Bronchiolitis
Kylie Krohmaly1, 2, Marcos Perez-Losada1, Ignacio Ramos Tapia3, Zhaozhong Zhu4, Kohei Hasegawa4, Carlos Camargo4, Brennan Harmon2, Janice Espinola4, Laura Cechinel2, Rachael Batabyal2, 5, Robert Freishtat1, Andrea Hahn5
1. The George Washington University, Washington, DC, United States.
2. Children’s National Research and Innovation Campus, Washington, DC, United States.
3. Universidad Andrés Bello, Santiago, Chile.
4. Department of Emergency Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, MA, United States.
5. Children’s National Hospital, Washington, DC, United States.
Purpose of Study: Bronchiolitis, a viral lower respiratory infection, is the leading cause of infant hospitalization in the U.S. and is associated with an increased risk for developing childhood asthma. Bronchiolitis can be caused by several respiratory viruses, including respiratory syncytial virus (RSV) and rhinovirus (RV). Studies have shown viral etiology-related differences between RSV and RV bronchiolitis in the immune response, human microRNA (miRNA) profiles, and dominance of certain airway microbiome bacteria, particularly of Haemophilus influenzae, Moraxella catarrhalis, Moraxella nonliquefaciens, and Streptococcus pneumoniae. Here, we examined how bacterial small RNAs (sRNAs), the prokaryotic equivalent to eukaryotic miRNAs, may impact response differences.
Methods Used: We first derived reference sRNA datasets from cultures of four bacteria known to be associated with bronchiolitis (i.e., H. influenzae, M. catarrhalis, M. nonliquefaciens, and S. pneumoniae). Using these reference sRNA datasets, we identified sRNAs associated with bronchiolitis either caused by a singular RSV infection or singular RV infection in human nasal RNA-Seq data from infants of the 35th Multicenter Airway Research Collaboration cohort. We also determined potential human transcript targets of the bacterial sRNAs and compared expression of the sRNAs between RSV and RV cases.
Summary of Results: There were 4 sRNAs significantly overexpressed in RSV bronchiolitis cases (compared to RSV bronchiolitis), and 26 sRNAs significantly overexpressed in RV bronchiolitis (compared to RV bronchiolitis). Bacterial sRNAs overexpressed in RSV bronchiolitis were predicted to activate the interleukin (IL)-6 and IL-8 pathways, while those associated with RV bronchiolitis were predicted to activate the IL-17A pathway. These results support that bacteria may be contributing to inflammation differences seen in RSV and RV bronchiolitis, and, for the first time, indicate that bacteria may do so through sRNAs.
Conclusions: We identified 30 bacterial sRNAs, the prokaryotic equivalent to eukaryotic miRNAs, that differ between infants with RSV versus RV bronchiolitis. These sRNAs may alter cytokine signaling contributing to the clinical differences seen between viral etiologies.
4. Respiratory Pathogen Surveillance in Pediatric Healthcare Workers
Mubasshira M. Khan1, Clara El Nakib1, Noelle Ortiz2, Ghina Fakhri1, Lucia Janovicova1, Joseph Domachowske3, Manika Suryadevara3, Heather Wasik4
1. Pediatrics, SUNY Upstate Medical University, Syracuse, NY, United States.
2. SUNY Upstate Medical University, Syracuse, NY, United States.
3. Pediatric Infectious Diseases, SUNY Upstate Medical University, Syracuse, NY, United States.
4. Pediatric Nephrology, SUNY Upstate Medical University, Syracuse, NY, United States.
Purpose of Study: Pediatric healthcare workers (HCWs) may be exposed to respiratory pathogens at work. Few large-scale surveillance studies have analyzed respiratory infections in pediatric HCWs. This study aims to assess respiratory pathogen detection rates among pediatric HCWs and analyze factors associated with pathogen detection
Methods Used: Pediatric HCWs obtain self-collected nasal swabs and complete surveys bi-monthly. Survey data includes demographics, respiratory symptoms, household sick contacts, and occupational location. Samples tested for 21 respiratory pathogens using multiplex PCR (BioFire Respiratory Panel 1.7). Associations between pathogen detection and demographic, household, and occupational characteristics were assessed using Chi-squared tests and rank sum tests
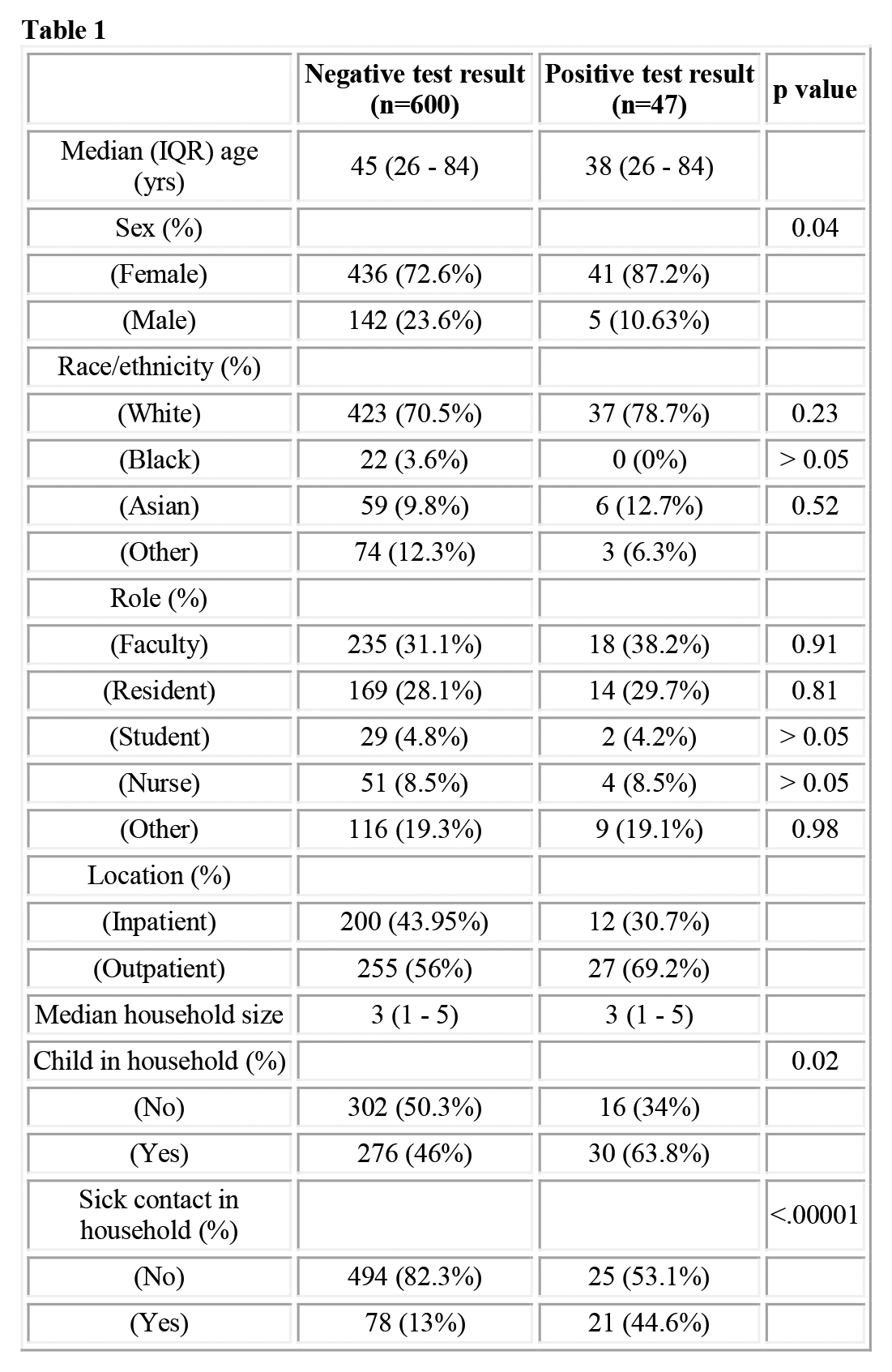
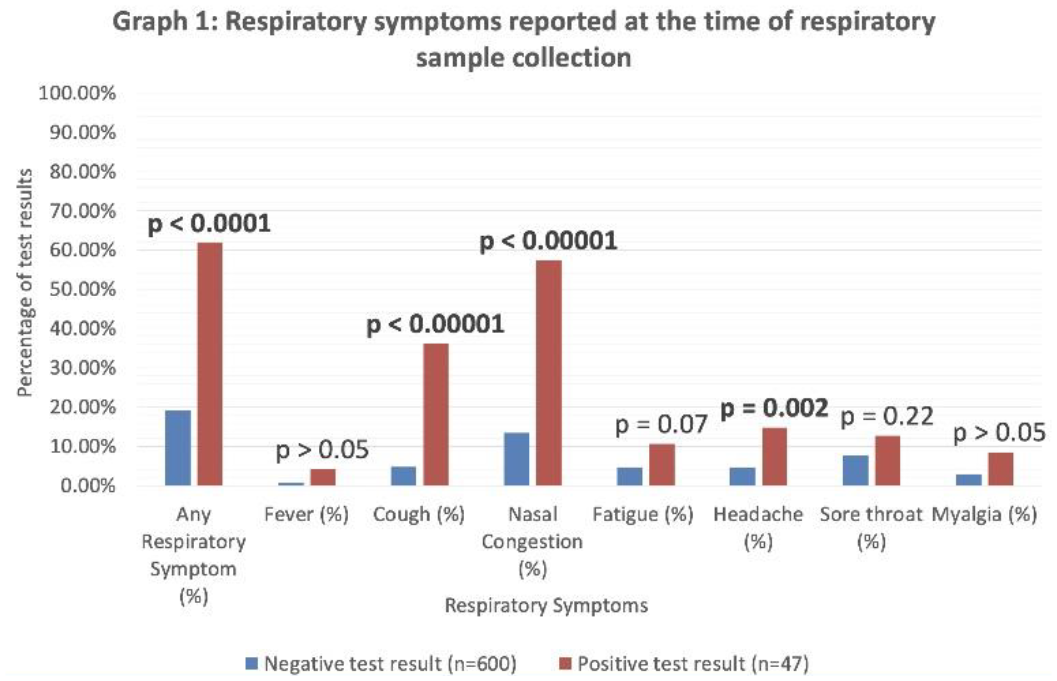
Summary of Results: 647 samples were obtained from 44 pediatric HCWs 2/2022–12/2023. Multiplex PCR yielded 47 positive results (7.26%): 20 Rhinovirus/Enterovirus, 4 Respiratory syncytial virus, 1 Adenovirus, 1 Parainfluenza virus type 3, 11 Coronavirus-19, 4 Human metapneumovirus, 1 Coronavirus 229E, 2 Coronavirus NL63, 1 Coronavirus HKU1, 1 Rhinovirus/Enterovirus & Adenovirus co-detection and 1 Rhinovirus/Enterovirus & Coronavirus-19 co-detection. Pathogen detection was positively associated with household sick contact (44.6% vs 13%, p < 0.00001), children in the household (63.8% vs 56%, p = 0.02), and female sex (87.2% vs 72.6%, p = 0.04) but no other demographic or occupational factors (Table 1). Any respiratory symptom (61.7% vs 19.1%, p < 0.00001), cough (36.1% vs 4.8%, p < 0.00001), nasal congestion (57.4% vs 13.5%, p < 0.00001) and headache (14.8% vs 4.6%, p = 0.002) were associated with respiratory pathogen detection but fever, myalgias, fatigue and sore throat were not (Graph 1)
Conclusions: Respiratory infections in pediatric HCWs are common and associated with children in the household, sick household contacts and female sex but not clinical role or location. Identification of factors associated with respiratory infections in HCWs may lead to mitigation strategies to prevent the spread of respiratory pathogens in health care settings
Demographic, household, and occupational data reported at time of respiratory sample collection
Negative test result (n=600)
Positive test result (n=47)
p value
Median (IQR) age (yrs)
45 (26 - 84)
38 (26 - 84)
Sex (%)
0.04
(Female)
436 (72.6%)
41 (87.2%)
(Male)
142 (23.6%)
5 (10.63%)
Race/ethnicity (%)
(White)
423 (70.5%)
37 (78.7%)
0.23
(Black)
22 (3.6%)
0 (0%)
> 0.05
(Asian)
59 (9.8%)
6 (12.7%)
0.52
(Other)
74 (12.3%)
3 (6.3%)
Role (%)
(Faculty)
235 (31.1%)
18 (38.2%)
0.91
(Resident)
169 (28.1%)
14 (29.7%)
0.81
(Student)
29 (4.8%)
2 (4.2%)
> 0.05
(Nurse)
51 (8.5%)
4 (8.5%)
> 0.05
(Other)
116 (19.3%)
9 (19.1%)
0.98
Location (%)
(Inpatient)
200 (43.95%)
12 (30.7%)
(Outpatient)
255 (56%)
27 (69.2%)
Median household size
3 (1 - 5)
3 (1 - 5)
Child in household (%)
0.02
(No)
302 (50.3%)
16 (34%)
(Yes)
276 (46%)
30 (63.8%)
Sick contact in household (%)
<.00001
(No)
494 (82.3%)
25 (53.1%)
(Yes)
78 (13%)
21 (44.6%)
Respiratory symptoms reported at the time of respiratory sample collection
5. Protective Effects of Booster Dose COVID-19 Vaccine Against Post-Acute COVID-19: A Systematic Review
Ved Patel1, Joseph Cervia1, 3, Maximilian Korsun2
1. Donald and Barbara Zucker School of Medicine at Hofstra/Northwell, Hempstead, NY, United States.
2. Hospital for Special Surgery, New York, NY, United States.
3. Healthcare Partners, IPA, & MSP, Garden City, NY, United States.
Purpose of Study: Post-Acute COVID-19 Syndrome, also known as “Long Covid (LC),” is a debilitating sequela of SARS-COV-2 infection. LC has occurred in at least 10% of patients who have previously been infected with SARS-COV-2 and presented with a myriad of symptoms including post-exertional malaise, fatigue, brain fog, dizziness, palpitations, and gastrointestinal symptoms. Vaccinations have been useful in decreasing the incidence of COVID-19. Further studies have noted a protective effect of the initial dose of COVID-19 vaccines and LC; however, less is known about the effects of multiple booster vaccination doses. We aimed to investigate the protective effect of COVID-19 booster doses on patients previously infected with SARS-CoV-2 against LC. The aim of this study was to identify the protective effects of COVID-19 booster vaccination against the LC. This was a systematic review to identify and review the efficacy of COVID-19 booster vaccination against the incidence of LC.
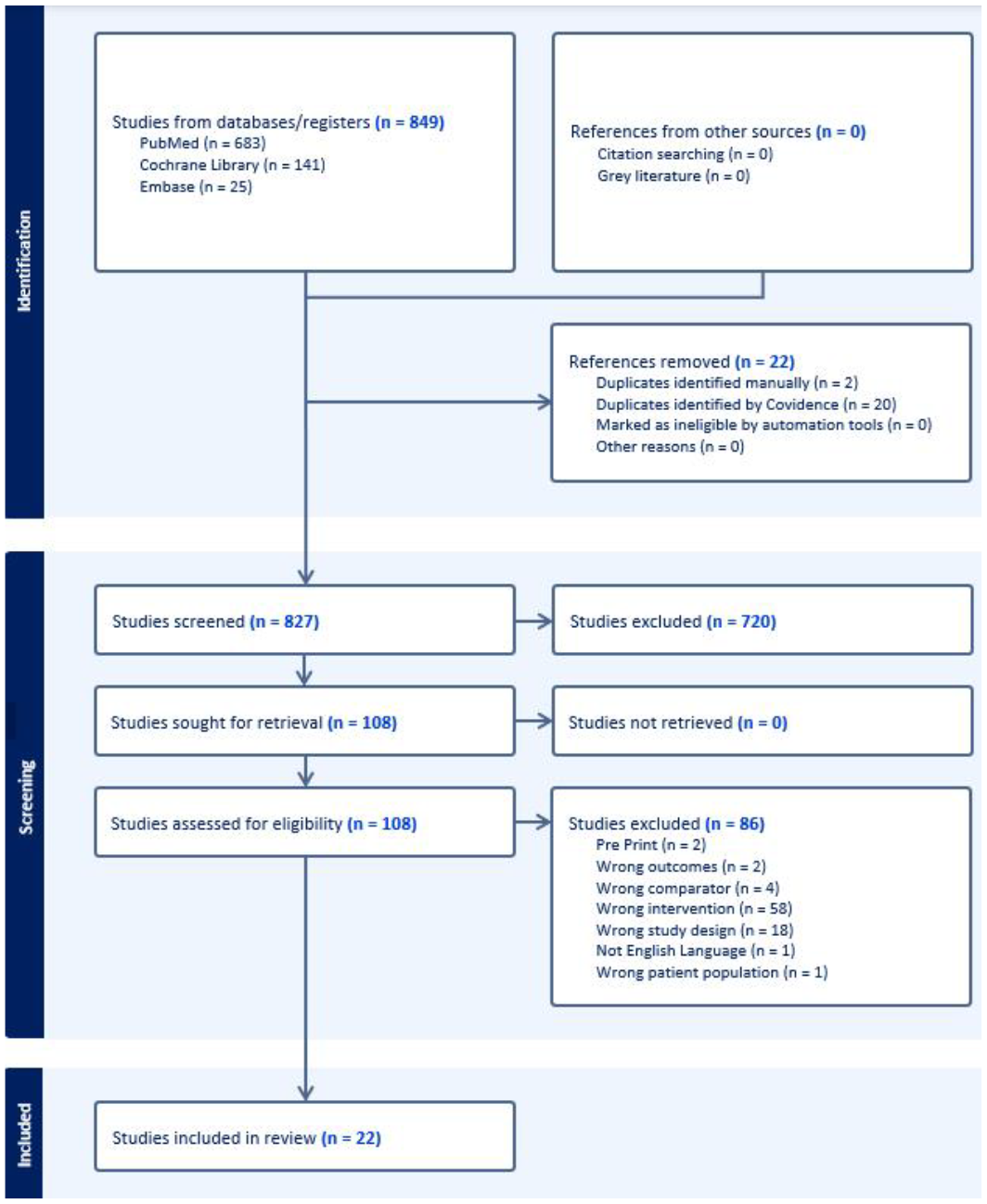
Methods Used: A systematic search was conducted of the electronic databases PubMed, Embase, and Cochrane Library according to PRISMA guidelines. This search was conducted to identify studies regarding the incidence of LC among patients who received a COVID-19 booster dose and those who did not. Search results were then examined further to determine studies of relevance for review. Studies involving participants who were diagnosed with COVID-19 and were previously vaccinated compared to those who also received a prior booster. The main outcome was the incidence of LC. The risk of bias was assessed using the JBI critical appraisal tool for systematic reviews.
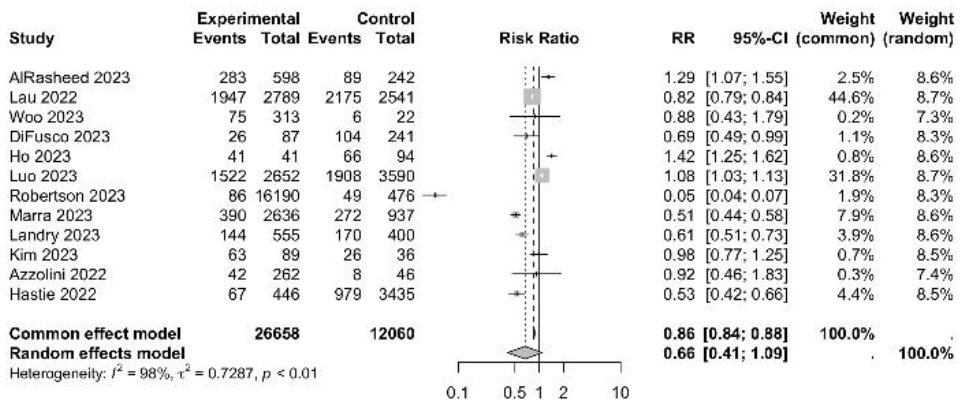
Summary of Results: Search results identified 827 unique studies for screening. Of these, 720 were excluded for failing to meet inclusion criteria, and 108 full-text studies were assessed for eligibility. A further 86 studies were excluded with the majority due to the wrong comparator. Of the 22 included studies, 12 studies were identified to report LC rates in accordance with booster administration and there was a statistically lower risk of LC symptoms within a common effects model (RR: 0.86; 95% CI: 0.84; 0.88). Despite substantial heterogeneity in study populations, there appeared to have been a significant protective effect of booster vaccinations against LC.
Conclusions: Literature on LC has indicated a marked decrease in incidence in vaccinated populations with limited information on booster doses. There was a statistically significant effect observed regarding the protective effect of booster vaccination against LC when compared to the base vaccination series. However, there was a high degree of heterogeneity with this meta-analysis. There is a need for more comprehensive research about the direct effects of booster vaccinations on LC incidence.
PRISMA flowchart.
Forest plot indicating effects of base vaccination (control) vs booster vaccination (experimental) on the incidence of LC (events) within the population (total).
6. Influenza and Covid-19 Booster Vaccine Hesitancy among Healthcare Workers in the Metro-Atlanta Area
1. Medicine, Emory School of Medicine, Atlanta, GA, United States.
2. Hospital Medicine, Emory School of Medicine, Atlanta, GA, United States.
3. Tennessee Department of Health, Nashville, TN, United States.
4. Family Medicine, Emory School of Medicine, Atlanta, GA, United States.
Purpose of Study: Vaccine hesitancy has been well-described for both the Influenza vaccine and the Covid-19 vaccine, but there is limited data on Covid-19 boosters and post-pandemic influenza vaccine uptake data in healthcare workers (HCW). Many healthcare institutions mandated the primary COVID vaccines series, however, boosters have not been mandated. Alternatively, the influenza vaccine is a commonly mandated vaccine for HCW. The purpose of this study is to evaluate perceptions of the Covid-19 booster and the annual influenza vaccine among HCW in the metro-Atlanta area in the early post-pandemic era.
Methods Used: We conducted a cross-sectional survey (using Qualtrics) of HCWs via email from September to December 2023. Question items included demographics, occupation role (clinical or nonclinical), and whether or not both the Influenza and Covid-19 booster vaccines were received. General attitudes and perceptions about COVID-19 booster and Influenza vaccines and reasons for not receiving the vaccine were collected using a 5-point Likert scale for agreement. We defined “vaccine-hesitant” individuals as those who had neither received nor planned to receive the latest Covid-19 booster and/or the Influenza vaccine at the time of the survey. Descriptive statistics were analyzed using SAS 9.4.
Summary of Results: There were 2884 respondents out of approximately 30,000 HCW giving us a response rate of approximately 9.6%. Of the 2884 respondents, 2449 (83.4%) were female; 1328 (46%) were Black and 1125 (39%) were White. [KA2] Of the 1834 (63.6%) clinical HCW,38.4% were nurses (38.4%) while 10.6% were advanced practice providers or physicians. 646 (22.4%) had a masters degree while 985 (34.2) had a bachelors degree. 1095 received a Covid-19 booster in 2022 and this number dropped to 570 in 2023. Approximately 10% of HCW do not believe in COVID-19 vaccine and have not changed their opinion since the start of the pandemic. Almost 24% of HCW no longer want to receive future COVID boosters. With regards to the influenza vaccine, 1604 (59%) voluntarily received an influenza vaccine since 2022 while 908 (33.4%) only received it because it was mandated. Similarly, 1740 (64.1%) will continue to get it voluntarily while (31.3%) will receive it only if mandated. Of the 1604 (59%) that voluntarily received the flu vaccine, 948 (59.1%) were likely to receive future Covid-19 vaccines. 554 (20.3%) changed their opinion of the influenza vaccine and felt that it was more important since the Covid-19 pandemic. 318 (11.6%) were more likely to receive the Covid-19 vaccine since the pandemic began.
Conclusions: While vaccine hesitancy persists for both Covid-19 and Influenza vaccines, the Covid-19 pandemic and vaccine development may have instigated a change in perception around both the annual Influenza and future Covid-19 vaccines. Continued vaccine promotion for the Influenza and future Covid-19 vaccines is necessary to address vaccine hesitancy.
7. Zinc Supplementation Associated With a Decrease in Mortality in COVID-19 Patients: A Meta-Analysis
Spencer Rheingold1, Chirag Raval1, Antonio M. Gordon2, Patrick Hardigan1
1. Dr. Kiran C. Patel College of Allopathic Medicine, NOVA Southeastern University, Fort Lauderdale, FL, United States.
2. Internal Medicine, University Health Care, Hialeah, FL, United States.
Purpose of Study: The COVID-19 pandemic has had a significant impact on the world, resulting in millions of deaths worldwide and imposing economic, political, and social problems. The use of nutritional supplementation for the prevention and mitigation of COVID-19 remains controversial. This meta-analysis aims to investigate the association between zinc supplementation, mortality, and symptomatology, among COVID-19-infected patients.
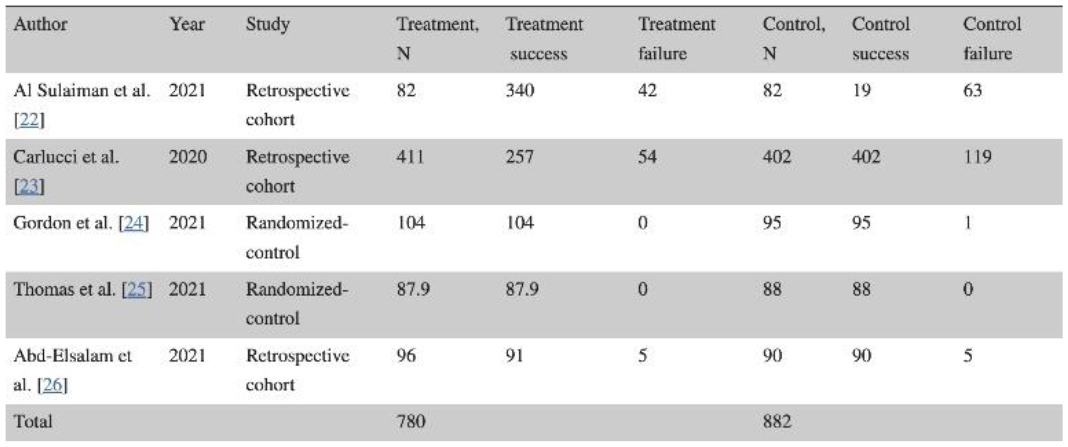
Methods Used: A meta-analysis was conducted to compare the outcomes of mortality and symptomology of patients with COVID-19 receiving zinc supplementation and those not receiving zinc supplementation. PubMed/Medline, Cochrane, Web of Science, and CINAHL Complete were independently searched with the search terms "zinc" AND "covid" OR "sars-cov-2" "COVID-19" OR "coronavirus". After duplicates were removed, 1215 articles were identified. Five of these studies were used to assess mortality outcomes, and two were used to assess symptomatology outcomes. The meta-analysis was conducted through R 4.2.1 software (R Foundation, Vienna, Austria). Heterogeneity was evaluated by calculating the I2 index. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used.
Summary of Results: It was found that COVID-19-infected individuals treated with zinc supplements had a reduced risk of mortality compared with individuals not treated with a zinc supplement RR=0.63 (95%CI;0.52,0.77), p=0.005. For symptomology, it was found that COVID-19-infected individuals treated with zinc had no difference in symptomology than individuals not treated with a zinc supplement RR=0.52 (95%CI;0.00,24315.42), p=0.578.
Conclusions: This data indicates that zinc supplementation is associated with decreased mortality in those with COVID-19 but does not change symptomatology. This is promising as zinc is widely available and may be valuable as a cost-effective way to prevent poor outcomes for those with COVID-19.
8. Exploring the Associations between Self-Reported Sleep Disturbance and Cognitive Impairment among Survivors of COVID-19 Hospitalization
Ayah Eltoum1, Rahima Begum1, Laura S. Gold2, James S. Andrews1
1. Clinical Immunology and Rheumatology, University of Alabama at Birmingham, Birmingham, AL, United States.
2. Radiology, University of Washington, Seattle, WA, United States.
Purpose of Study: Cognitive impairment following COVID-19 infection is common and risk factors remain poorly understood. Sleep disturbance increases risk of cognitive impairment in the general population, and sleep disturbance is common after COVID-19. This study assessed whether new sleep disturbance at 1-month is associated with risk of cognitive impairment at 6-months after COVID-19 hospitalization.
Methods Used: English-speaking adults aged ≥18 years at the University of Washington Medical Center who survived to 1-month post-COVID-19 hospitalization were enrolled. Self-reported sleep disturbance, cognitive function, cognitive abilities, and fatigue severity at 1- and 6-months after discharge were assessed by the Patient-Reported Outcomes Measurement Information System (PROMIS®) short forms. Pre-COVID-19 hospitalization status was assessed retrospectively. New sleep disturbance was defined as a ≥5 point increase at 1-month compared to pre-COVID. Significant worsening in cognitive function and cognitive abilities were defined as a ≥5 point decrease and worsening fatigue severity as a ≥5 point increase, each at 6-months compared to 1-month. Linear and logistic regression models analyzed associations of new sleep disturbance at 1-month with cognitive function, cognitive abilities, and fatigue severity outcomes at 6-months.
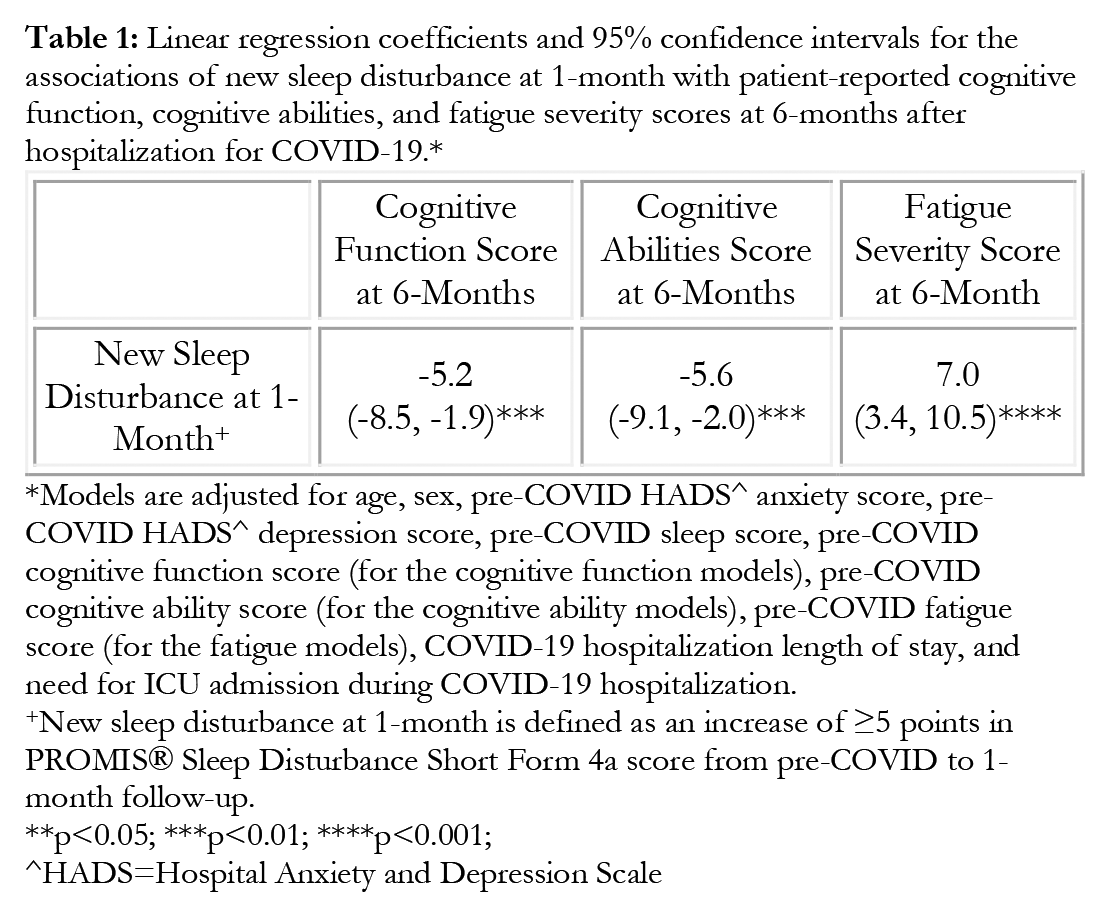
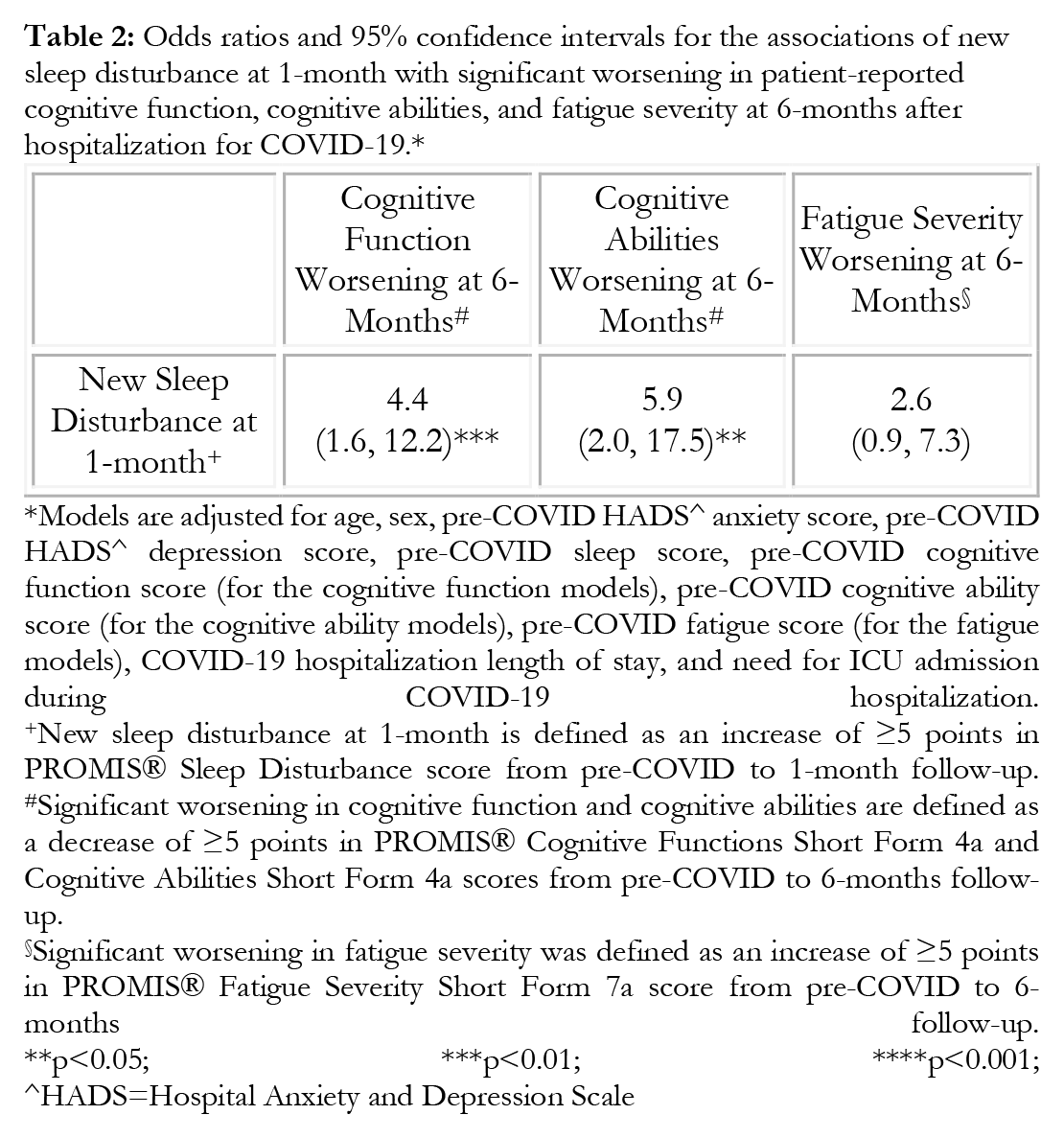
Summary of Results: Participants (n=120) had mean age of 56.5±15.7 years, and 35% developed new sleep disturbance at 1-month. Among those with versus without new sleep disturbance at 1-month, 74% versus 40%, 76% versus 37%, and 64% versus 50% developed significant worsening in cognitive function, cognitive abilities, and fatigue severity at 6 months, respectively. Tables 1 and 2 present associations of new sleep disturbance at 1-month with outcomes at 6-months.
Conclusions: New sleep disturbance at 1-month post-COVID-19 hospitalization is associated with subsequent significant worsening in cognitive function, cognitive abilities, and fatigue severity at 6-months. These findings suggest that sleep disturbance may be an important risk factor for persistent neurocognitive impairment after COVID-19. Additional studies should validate these relationships in other post-COVID-19 cohorts and examine whether improving sleep quality may reduce the risk of cognitive impairment in these patients.
Linear regression coefficients and 95% confidence intervals for the associations of new sleep disturbance at 1-month with patient-reported cognitive function, cognitive abilities, and fatigue severity scores at 6-months after hospitalization for COVID-19.*
Models are adjusted for age, sex, pre-COVID HADS^ anxiety score, pre-COVID HADS^ depression score, pre-COVID sleep score, pre-COVID cognitive function score (for the cognitive function models), pre-COVID cognitive ability score (for the cognitive ability models), pre-COVID fatigue score (for the fatigue models), COVID-19 hospitalization length of stay, and need for ICU admission during COVID-19 hospitalization.
New sleep disturbance at 1-month is defined as an increase of ≥5 points in PROMIS® Sleep Disturbance Short Form 4a score from pre-COVID to 1-month follow-up.
p<0.05; ***p<0.01; ****p<0.001;
^HADS=Hospital Anxiety and Depression Scale.
Odds ratios and 95% confidence intervals for the associations of new sleep disturbance at 1-month with significant worsening in patient-reported cognitive function, cognitive abilities, and fatigue severity at 6-months after hospitalization for COVID-19.*
Models are adjusted for age, sex, pre-COVID HADS^ anxiety score, pre-COVID HADS^ depression score, pre-COVID sleep score, pre-COVID cognitive function score (for the cognitive function models), pre-COVID cognitive ability score (for the cognitive ability models), pre-COVID fatigue score (for the fatigue models), COVID-19 hospitalization length of stay, and need for ICU admission during COVID-19 hospitalization.
New sleep disturbance at 1-month is defined as an increase of ≥5 points in PROMIS® Sleep Disturbance score from pre-COVID to 1-month follow-up.
Significant worsening in cognitive function and cognitive abilities are defined as a decrease of ≥5 points in PROMIS® Cognitive Functions Short Form 4a and Cognitive Abilities Short Form 4a scores from pre-COVID to 6-months follow-up.
Significant worsening in fatigue severity was defined as an increase of ≥5 points in PROMIS® Fatigue Severity Short Form 7a score from pre-COVID to 6-months follow-up.
p<0.05; ***p<0.01; ****p<0.001;
^HADS=Hospital Anxiety and Depression Scale.
9. Does Artificial Intelligence-Aided Technology Allow for Improved Detection of Polyps in Difficult Locations Among Experienced Endoscopists?
Mohammed Ahsan1, Zackary Anderson1, Maged Bakr1, Raymond Phillips1
1. NCH Healthcare System, Naples, FL, United States.
Purpose of Study: Colonoscopy serves as the gold standard for the detection of precancerous lesions, as polypectomy drastically reduces the risk of the progression of adenomas to colorectal cancer (CRC). Some polyps are difficult to remove given their size and location. Traditionally, polyps located in the cecum, right colon, ileocecal valve, or behind folds are challenging and easy to miss with conventional colonoscopies. AI-assisted colonoscopies aim to overcome these discrepancies, as current literature shows such technology has allowed for better detection of adenomas in not only the distal colon but in the proximal colon. Our study aims to explore this further, as we look at the rate of polyp detection among experienced endoscopists after the incorporation of the GI-GENIUS program, and to see if it has improved the detection of polyps in previously difficult locations.
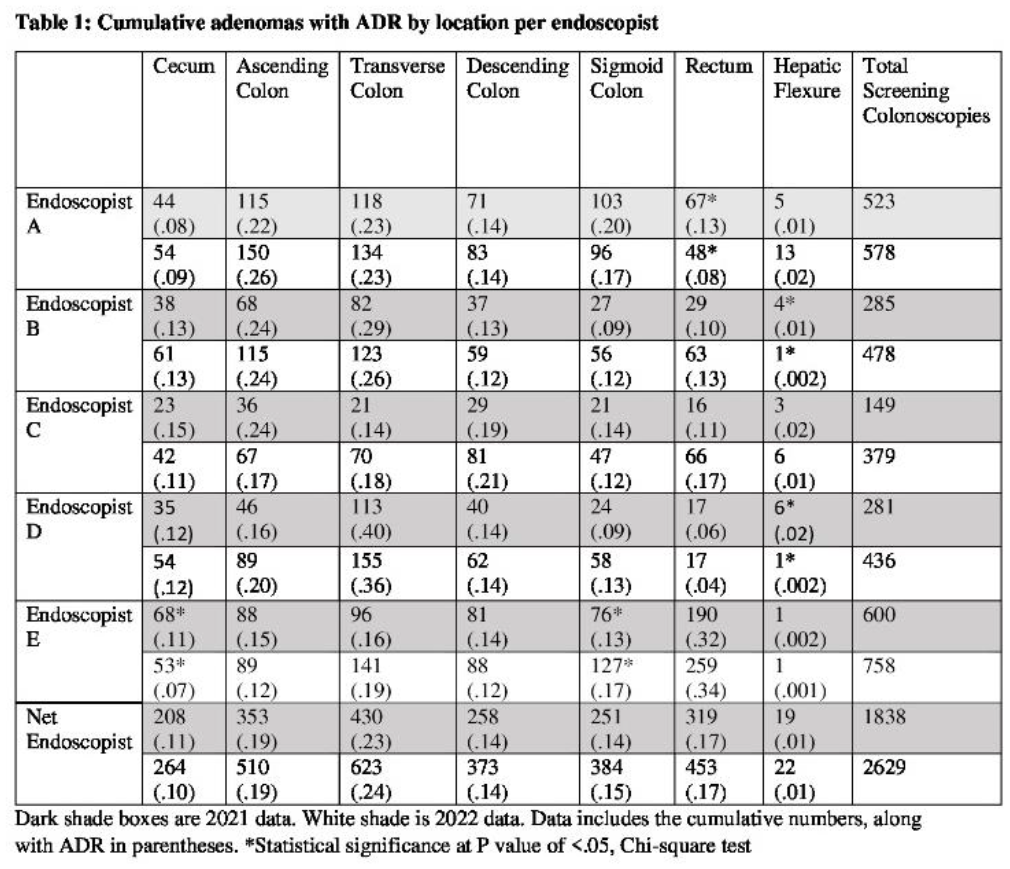
Methods Used: A single-center retrospective study was performed at Naples Community Hospital (NCH) Endoscopy Center. The information was obtained from digital records maintained at NCH through PROVATION and EPIC. Data from five experienced endoscopists was collected for the years of 2021 and 2022 for comparison since the AI technology “GI GENIUS” was implemented in 2022. For the years of 2021 and 2022, data was recorded regarding the location of the polyp and was organized via the following categories “Ileocecal valve, cecum, ascending colon, hepatic flexure, transverse colon, descending colon, splenic flexure, sigmoid colon, rectum”.
Summary of Results: When evaluating the differences in polyp detection among all endoscopists before and after the initiation of the GI GENIUS, it appears that there is no significant difference between the two groups based on polyp location. With that said, when looking at the data individually, based on trends of various endoscopists. We found that 2/5 endoscopists had a statistically significant difference in polyp detection in the hepatic flexure, 1/5 endoscopists were found to have a significant difference in polyp detection via GI Genius in the sigmoid colon and cecum. Finally, 1/5 of endoscopists had statistically significant differences in the rectum.
Conclusions: Our study showed that while there was some variability in finding difficult polyps among experienced endoscopists, the overall difference among all endoscopists in a community setting, before and after the incorporation of the GI GENIUS was not significant. Since this was the first year with the incorporation of the AI model, some of the variation among the endoscopists may be attributed to inexperience with the program, and therefore a follow-up study should be conducted with a more standardized protocol. Finally, given that the GI GENIUS technology is still in its infancy, a future aim should be to enhance the algorithm and techniques to detect polyps in difficult locations such as in mucosal folds and the right colon.
10. Quantitative Advancements in Clinical Accuracy of Successive Generative Pre-Trained Transformer Models
Hudson Tate1, Ben Hambright1, Abby Clark2, Cory Dixon3, Ben Kronz4, James Ricks5, Olivia Spaedy6, Sydney Whalen7, Danner Butler8, Brenton Bicknell1
1. UAB Heersink School of Medicine, Birmingham, AL, United States.
2. UT Southwestern Medical School, Dallas, TX, United States.
3. Alabama College of Osteopathic Medicine, Dothan, AL, United States.
4. Medical College of Georgia, Augusta University, Augusta, GA, United States.
5. Harvard Medical School, Boston, MA, United States.
6. School of Medicine, St. Louis University, St. Louis, MO, United States.
7. University of Illinois College of Medicine, Chicago, IL, United States.
8. Whiddon College of Medicine, University of South Alabama, Mobile, AL, United States.
Purpose of Study: As artificial intelligence (AI) continues to develop, Generative Pre-trained Transformer (GPT) large language models (LLMs) are being investigated for their clinical utility. Less characterized is their ability to generate differential diagnoses and their clinical decision-making. This study’s objective was to methodically assess the potential utility of one GPT LLM, the ChatGPT Series, in generating helpful and accurate diagnoses and choosing the best diagnosis.
Methods Used: 342 clinical vignette-based multiple-choice questions (MCQs) sourced from various question bank resources available to medical students across the United States were presented to OpenAI’s ChatGPT 3.5 (GPT-3.5), ChatGPT 4 (GPT-4), and an Enhanced ChatGPT 4 (En-GPT-4) from the OpenAI GPT platform. The vignettes and answer choices were input following the instruction, “Answer the following question.” Assessments for comparison included overall response accuracy and categorical clinical accuracies (based on the MCQ stem), including determining the most likely diagnosis and best next step in management. An additional prompt was used for questions assessing the most likely diagnosis without provided answer choices: “Generate a differential diagnosis for the following clinical case.” 164 MCQs were assessed for an underlying diagnosis.
Summary of Results: There was a statistically significant higher response accuracy with successive GPT models. GPT 3.5 established a baseline accuracy of 70.5% (CI: 65.7–75.3, n=342), with diagnostic and differential diagnosis accuracy of 72.6% (CI: 65.7-79.5, n=164) and 84.1% (CI: 78.5-89.7, n=164) respectively. GPT-4 demonstrated a substantial increase in accuracy to an overall rate of 81.9% (CI: 77.8–86.0, n=342), with marked improvements in diagnostic accuracy to 81.7% (CI: 75.8–87.6, n=164) and differential diagnosis accuracy to 93.3% (CI: 89.5-97.1 n=342). En-GPT-4 showcased a further leap in accuracy, achieving 84.2% (CI: 89.5–97.1, n=164) in overall accuracy. It also showcased marked improvements in selecting the correct diagnosis, achieving 85.4% (CI: 80.0-90.8, n=164) accuracy, signifying a significant improvement from its predecessors. After analysis, we found a significant difference in the ability of En-GPT-4 over GPT-3.5 in total outcomes (X2 =18.427, p<.0001) and its ability to generate an accurate differential diagnosis (X2 =6.854, p<.01).
Conclusions: This study highlighted a sequential improvement in the performance of GPT models. Our data corroborates a profound improvement in the ability of successive iterations of LLMs to generate differential diagnoses accurately and demonstrates the potential for continued improvements of LLMs. GPT large-language models are a potential clinical tool for physicians in patient care with a starting point in medical education. However, further critical analyses and development are needed before their implementation.
11. Assessing the Management of Hypertension at Equal Access Birmingham, a Student-Run Free Clinic at University of Alabama Birmingham School of Medicine
Peter Abdelmessih1, Katherine Smith1, Nicholas Van Wagoner1
1. University of Alabama Birmingham School of Medicine, Birmingham, TN, United States.
Purpose of Study: Student-Run Free Clinics (SRFCs) aim to serve underprivileged communities and are a key part of the safety-net healthcare system. Little is known about SRFC patient outcomes. This study assessed the management of hypertension (HTN) at Equal Access Birmingham (EAB), a SRFC at University of Alabama Heersink School of Medicine. The study aimed to (1) assess how effective hypertension is managed at EAB and (2) identify variables associated with blood pressure control.
Methods Used: This retrospective study monitored blood pressure control for 6 months in persons diagnosed with hypertension. Data was collected from August 2020 through August 2022. Controlled blood pressure was classified as a systolic reading of <140 and a diastolic reading of <90 at the last visit. Univariate analyses were performed to identify variables (age, sex, body mass index, presence of comorbid disease (diabetes, hyperlipidemia, heart failure, stroke, and mental illness) associated with blood pressure control. Significant variables identified in univariate analysis (P, 0.05) were planned for assessment in multivariable modeling.
Summary of Results: A total of 137 patients were diagnosed with hypertension; 66 met inclusion criteria and were included in the study. Mean age was 48.7 years (SD ± 14.0), and 60% were male. Average number of clinic visits per patient was 6.3 (SD ± 4.1). On initial clinic evaluation, mean systolic blood pressure was 151mmHg (SD ± 31mmHg) and mean diastolic pressure was 90mmHg (SD ± 17mmHg). Mean systolic and diastolic blood pressures were significantly reduced in during the study period (SBP 140mmHg (p=0.004), DBP 85mmHg (p=0.02). Only 44% of patients achieved blood pressure control. No studied variables demonstrated an association with blood pressure control.
Conclusions: Hypertension is a common problem among patients seen at EAB. Retention in care and achievement of blood pressure control is difficult in this population. Variables associated with blood pressure control were not identified, potentially related to small study population, or related factors not captured in this study.
12. Is Computer-aided Detection Technology Effective in Mitigating Physician Fatigue among Experienced Endoscopists in the Community Setting?
Mohammed Ahsan1, Medjine Jarbath1, Zackary Anderson1, Maged Bakr1, Raymond Phillips1
1. NCH Healthcare System, Naples, FL, United States.
Purpose of Study: Various modalities have been implemented to improve adenoma detection rate (ADR) and decrease mortality from colorectal cancer (CRC). The development of artificial intelligence (AI) aims to reduce performance variability during colonoscopies, as physicians may fall subject to error in visualizing polyps as a result of operator fatigue. Prospective studies have demonstrated a 27% polyp detection rate in morning colonoscopies compared to evening cases, using the time of day as a surrogate marker for fatigue. Computer-aided detection (CAD) systems can accurately detect polyps in 82% of cases when compared to expert endoscopists. Our study aims to investigate the impact of endoscopists’ fatigue on ADR and the effects of AI in improving ADR.
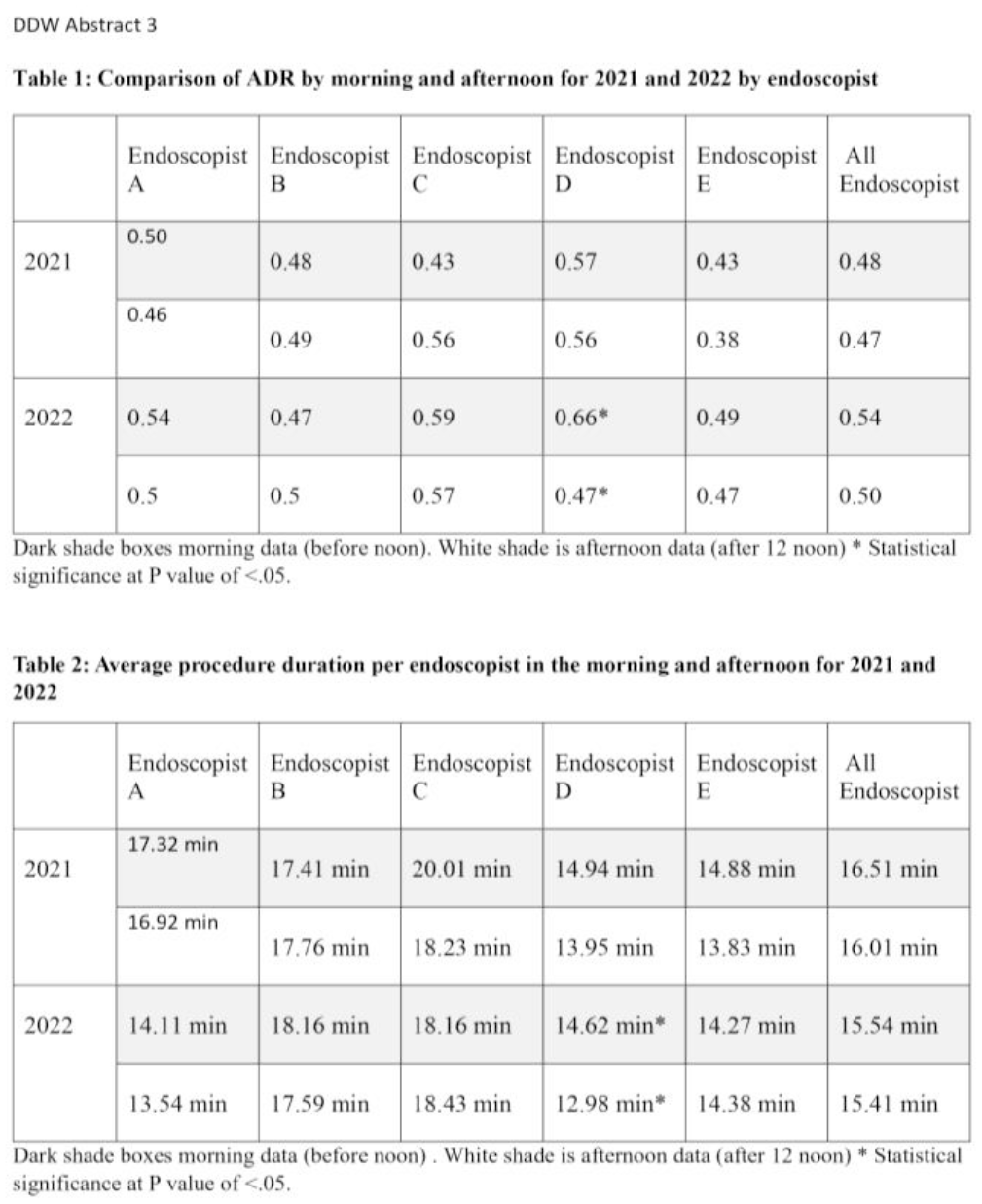
Methods Used: A single-center retrospective study was performed at Naples Community Hospital (NCH) Endoscopy Center. The information was obtained from digital records maintained at NCH through PROVATION and EPIC. Data from five experienced endoscopists was collected for the years of 2021 and 2022 for comparison since the CAD technology “GI GENIUS” was implemented in 2022. For the years of 2021 and 2022, data was recorded regarding time the procedure was done (morning versus afternoon), and total duration of the procedure. A Chi-Square test was performed comparing the ADR between the morning and afternoon colonoscopies for each year. The average procedure duration for each year (2021 vs 202) was compared via an unpaired T-test.
Summary of Results: When comparing the net ADR for the morning and afternoon procedures for all endoscopists at the community hospital in 2021 and 2022, a statistically significant difference was not found, In 2021, the ADR for all endoscopists in the morning was .48, while in the afternoon, it was found to be .47. In 2022, the ADR for all endoscopists in the morning was .54, while it was .50 in the afternoon. When looking at average procedure duration, 4/5 endoscopists had reduced duration in procedure time in 2022 compared to 2021, with endoscopist A being the only one with a statistically significant difference of 13.88 minutes in 2022 compared to 17.16 minutes in 2021.
Conclusions: In this retrospective community-based study of CAD among a group of experienced endoscopists, no statistically significant reduction in ADR was found in 2021 or 2022 to suggest operator fatigue. With that said, a general trend of decreased ADR was noted in the afternoon for 4/5 of the endoscopists. This decline persisted in 2022 when the CAD model was implemented, suggesting that CAD was not able to overcome or mitigate this phenomenon of operator fatigue. Interestingly the average procedure time was noted to be less in the 2022 year compared to 2021 year for most of the endoscopists, suggesting that perhaps the CAD model did help in making the workflow for the endoscopists more efficient. Further studies should investigate if this trend persists among inexperienced endoscopists with less than 5 years of experience in the community setting.
13. Exploring the Neurologic Impact of Licorice-induced Hypertensive Encephalopathy: Emphasizing the Critical Role of Timely Intervention
Christopher Fiechter1, 2, Melissa Tebaldi1, 2, Madison Morris2, Aleatha Reitsma-Mathias1, 2
1. Graduate Medical Education, Naples Community Hospital, Naples, FL, United States.
2. College of Medicine, University of Central Florida, Orlando, FL, United States.
Purpose of Study: Apparent mineralocorticoid excess (AME) is a condition that presents with hypokalemia, low aldosterone levels, and hypertension that can result in encephalopathy, coma, and death. Although rarely caused by excessive licorice intake, licorice toxicity leading to AME must not be overlooked when taking a detailed history of a patient presenting with uncontrolled hypertension. AME can be a difficult diagnosis, especially when working with memory impaired patients.
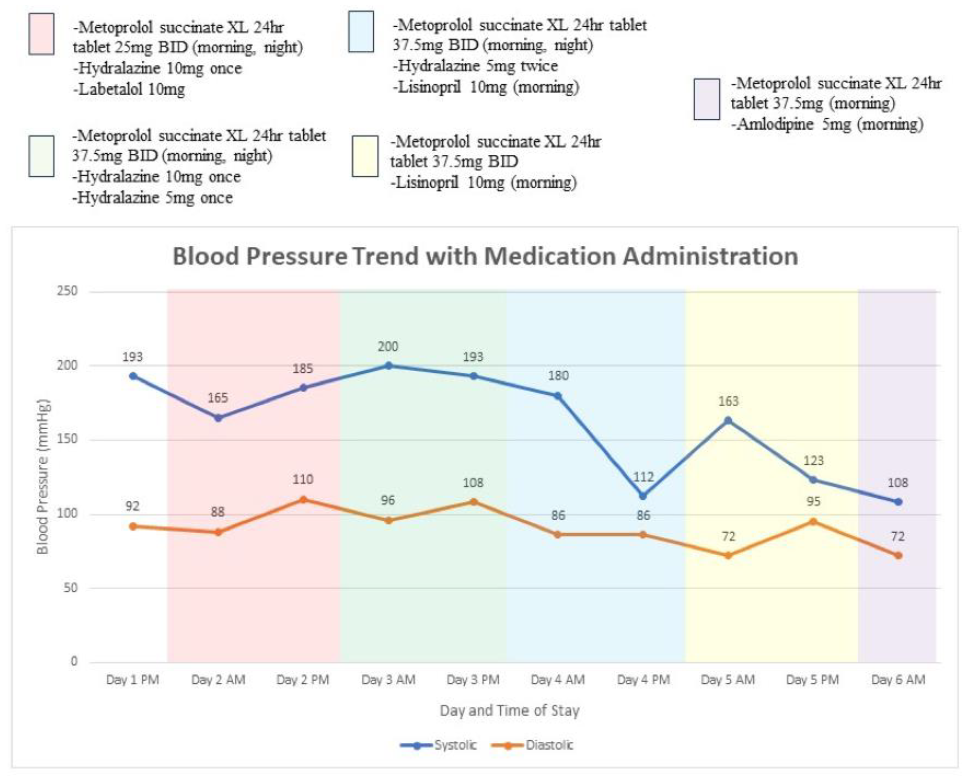
Methods Used: An 88-year-old male with a history of hypertension on metoprolol succinate 25 mg daily, hyperlipidemia, and dementia oriented x4 at baseline presented with altered mental status (AMS), generalized weakness, and incontinence of stool and urine. Vitals on arrival were remarkable for blood pressure (BP) of 193/92 and varied to a peak of 200/111 while hospitalized. Physical exam revealed a non-focal neurologic exam but patient was disoriented to place and time. Pitting edema was also present in both lower extremities.
Summary of Results: Workup for AMS was performed, including blood cultures, urinalysis, abdominal x-rays, CT and MRI of the brain, thyroid function, transthoracic echocardiogram, vitamin B12 and folate levels, all of which were unremarkable. Chest X-ray revealed mild vascular congestion. Discussion with the patient’s family revealed medication compliance, although he was reported to have consumed excessive quantities of black licorice in prior days, for which renin (0.17ng/mL/hr, ref: 0.7-3.3ng/mL/hr) and aldosterone ( < 1ng/dL, ref: 3.1-35.4ng/dL) levels were collected. Initial management with increased metoprolol was inadequate, and subsequent treatment with lisinopril 10mg daily resulted in overtreatment with acute kidney injury. He was treated successfully with amlodipine 5mg daily, however with instruction to withhold licorice intake and monitor for over-treatment of BP as an outpatient.
Conclusions: This case demonstrates a valuable contribution to the literature as black licorice is often overlooked in initial AMS workup. There is potential for severe complications with licorice toxicity leading to AME and ultimately encephalopathy, which may be reversible if the provoking agent is identified. It was determined that the patient was suffering from encephalopathy secondary to a hypertensive emergency, with BP recorded as high as 200 systolic and 111 diastolic. This was recognized in the setting of excess licorice intake after collecting a dietary history, for which a syndrome of pseudoaldosteronism was suspected. Consistent with this, hypokalemia was present, and renin and aldosterone levels were characteristically low. The patient was ultimately treated with metoprolol succinate 37.5 mg and amlodipine 5 mg with spontaneous improvement in BP and mentation. Guidance on presentation, diagnosis, and BP treatment is limited in the literature. Recognizing this syndrome and treating with licorice cessation and combination BP therapy may prove optimal to prevent end organ damage.
Line graph depicting daily blood pressure readings and BP medications patient received each day.
14. Adult-onset Kawasaki Disease: An Updated Review of the English-Language Literature from 1980 through 2023
Frank Adusei Poku, MD MS1, Bernice Biney, MD1, Samuel Akaakole Mensah, MBChB2, Joshua Oppong Ampadu, MBChB3, Henry Okafor, MD4
1Meharry Medical College, Dept. of Internal Medicine, Nashville, TN, 2West Virginia University, School of Medicine, Morgantown, WV, 3Greater Accra Regional Hospital, Accra, Ghana, 4Vanderbilt University Medical Center, Nashville, TN
Frank Adusei Poku1, Bernice Biney1, Samuel A. Mensah2, Joshua O. Ampadu3, Henry Okafor4
1. Internal Medicine, Meharry Medical College, Nashville, TN, United States.
2. Internal Medicine, West Virginia University, School of Medicine, Morgantown, WV, United States.
3. Greater Accra Regional Hospital, Accra, Ghana.
4. Vanderbilt University Medical Center, Nashville, TN, United States.
Purpose of Study: Kawasaki disease (KD) is a pan-vasculitis that primarily affects children and rarely adults. Available data on adult-onset KD are based on case reports and case series, both of which are limited by small sizes. We aimed to characterize the epidemiology, presentation, hospital course, and outcomes of adult-onset KD published in the English literature from 1980 through 2023.
Methods Used: We retrospectively reviewed and included published articles with a diagnosis of KD in patients age ≥18 years. We searched PubMed and Google scholar for case reports/series published in English using the keywords “adult”, “Kawasaki disease”, and “mucocutaneous lymph node syndrome”. We extracted data from individual articles onto an Excel spreadsheet for analysis. Outcomes of interest were the demographic characteristics of patients, clinical presentation and hospital course, management, and complications. Descriptive statistics were used to analyze the data.
Summary of Results: A total of 137 patients from 29 countries were included in this study. The majority were male (90/137, 64.9%; M:F ratio 1.8) and the median age was 25 years (range, 18-68). The median time to clinical presentation was 5 days (range, 4-60). The main signs and symptoms were fever (95.7%), skin rash (92.9%), conjunctivitis (89.3%), extremity changes (84.3%), oral changes (85.7%), and cervical lymphadenopathy (73.7%). The majority of the patients had no co-morbidities (125/137, 91.2%). EKG changes were not reported in 48 patients (35%). In the remaining 89, 26 (29.2%) had normal EKG or sinus tachycardia, 9 (10.1%) had ST segment elevation, and 9 (10.1%) had arrythmias or abnormal EKGs. Pharmacotherapy included IVIG (80/137, 58.4%), Aspirin (105/137, 76.6%), steroids (31/137, 22.6%) and antibiotics (68/137, 49.6%). For complications, 18.2% (25/137) had aneurysms, 8% (11/137) had myocardial infarction, 10.9% (15/137) had myocarditis, 10% had pericarditis/pericardial effusion, and 10.9% (15/137) had KD shock syndrome. The median length of stay was 14 days (range, 1-60 days). Three patients (2%) died from KD
Conclusions: Adult-onset KD is rare and is associated with significant cardiovascular complications. Clinicians should have high index of suspicion for prompt diagnoses and initiate appropriate treatment to improve outcomes.
15. Inpatient Status and Contrast-Associated Acute Kidney Injury and Long-term Outcomes after Coronary and Peripheral Angiography and Intervention
John Sadler1, 2, Annette Min1, 2, Sumon Roy1, 2, Robert Perera1, 2, Muhammad S. Pir1, 2, Ion S. Jovin1, 2
1. Richmond VAMC, Richmond, VA, United States.
2. VCU Health, Richmond, VA, United States.
Purpose of Study: Contrast-associated acute kidney injury (CA-AKI) is considered a complication of contrast administration during diagnostic angiography and percutaneous coronary and endovascular intervention. We investigated the association between inpatient status and the development of CA-AKI.
Methods Used: We studied 5481 patients undergoing peripheral and coronary angiography and percutaneous coronary and endovascular intervention at a Veterans’ Administration Medical Center. We analyzed the incidence of CA-AKI at 72 hours and of renal dysfunction at 3 months. CA-AKI was defined as either a rise in creatinine of 25% or an absolute rise in creatinine of 0.5 mg/dl.
Summary of Results: The mean age was 64.3 years. The inpatients (n=2851, 52%) were significantly older, had a higher baseline creatinine, and lower rates of hypertension and diabetes compared to the outpatients. Information on creatinine at 72 hours and at 3 months was available for 3063 patients and 3885 patients, respectively. CA-AKI occurred in 215 (8.8%) inpatients and in 36 (5.7%) outpatients at 72 hours after the procedure (P=0.01). At 3 months, renal dysfunction was seen in 365 (15.9%) inpatients versus 214 (13.4%) outpatients (P=0.03). A paired analysis based on the propensity score reflecting the probability of being an inpatient was performed adjusting for the baseline variables. The adjusted odds ratio (OR) for CA-AKI at 72 hours in inpatients was not significantly different compared to outpatients (OR 1.26, CI 0.96 – 1.66; P=0.09), and the adjusted OR for renal dysfunction at 3 months was also not significantly different between groups (OR 1.03, CI 0.87 – 1.22; P=0.70).
Conclusions: In this cohort of veterans, inpatient status was not associated with the development of AKI at 72 hours, or the development of renal dysfunction at 3 months post angiography or intervention.
16. Characterizing Response Accuracy of an AI Language-Learning Model, ChatGPT, with 200 Urologic Clinical Cases
John Michael W. Kaylor1, Brenton Bicknell1, Priti Dutta1, Danner Butler2, Adam Klein3, 1
1. UAB Marnix E. Heersink School of Medicine, Birmingham, AL, United States.,
2. Whidden College of Medicine at the University of South Alabama, Mobile, AL, United States.,
3. Department of Urology, UAB Medicine, Birmingham, AL, United States.
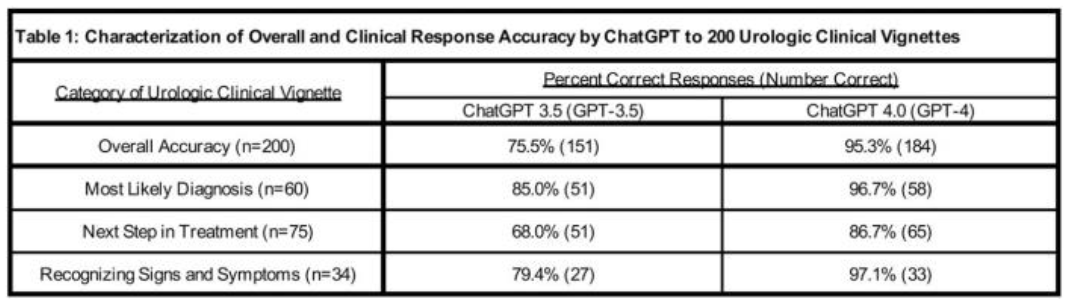
Purpose of Study: The discussion surrounding artificial intelligence (AI) language-learning models as a physician tool continues to develop as software such as ChatGPT, LlaMA, and BARD rapidly improve. While some studies have investigated the accuracy rates of these applications with various board exams and clinical cases, few studies have sought to categorize accuracy rates based on clinical elements such as diagnostic accuracy, recommendations in management, or recognition of signs and symptoms. This study aimed to characterize the accuracy of ChatGPT 3.5 (GPT-3.5) and ChatGPT 4.0(GPT-4) in response to urologic clinical vignettes and provide further characterization of their clinical response accuracy.
Methods Used: We utilized 200 randomly generated multiple-choice clinical vignettes from the “Urology” section of the AMBOSS education platform, an accredited continuing medical education resource by the ACCME. Vignettes were placed into GPT-3.5 following the instruction, “Answer the following question.” The same 200 vignettes were then input in the same manner to GPT-4. Overall accuracy and categorical accuracies of diagnostic, treatment recommendations, and recognizing signs and symptoms were collected.
Summary of Results: In response to the 200 urologic clinical vignettes, GPT-3.5 and GPT-4 responded accurately to 75.5% and 95.3% of vignettes, respectively. In the clinical categories of diagnosis, management, and signs and symptoms, GPT-3.5’s response accuracies were 85.0%, 68.0%, and 79.4%, respectively. GPT-4’s response accuracies in diagnosis, management, and signs and symptoms were 96.7%, 86.7%, and 97.1%. When using Pearson’s chi-squared, GPT-4’s response accuracy was markedly higher than GPT-3.5 (p<0.001).
Conclusions: This study demonstrated a reasonable level of accuracy in response to urologic clinical vignettes by GPT-3.5 with potential for improvements with updated models such as GPT-4. Limitations included the exclusion of imaging findings. As continual improvements to AI language learning models and new AI platforms develop, future studies should validate and characterize the accuracy of such software and discuss the ethical and societal considerations of AI utilization in healthcare settings.
17. Predicting Surgical Case Time: Using Machine Learning to Optimize Operating Room (OR) Scheduling
1. NYU Langone Health, New York, NY, United States.
2. CUNY School of Medicine, New York, NY, United States.
Purpose of Study: Operating rooms (ORs) constitute a significant portion of hospital revenue and expenses, ranging from $22 to $133 per minute. Cost reduction strategies, such as reducing 7 minutes per case over 250 cases, can yield up to $100,000 in savings. Current surgical case time prediction at NYU Langone Health primarily involves EPIC-generated estimates, in addition to surgeon inputs and scheduling team forecasts. Our study aims to develop and leverage an operation-specific machine learning model to more accurately predict surgical case times.
Methods Used: Robotic-assisted hysterectomies and myomectomies were selected because of their average case time, high surgical throughput, and poor baseline predictions. The machine learning model was constructed from operation-specific patient and surgical characteristics anticipated to influence case time. Retrospective data determined the relative importance of these characteristics on case time, and model predictions were retrospectively and prospectively validated. The primary outcome was the difference in model predictions compared to baseline predictions, quantified by 15-minute time blocks.
Summary of Results: The model successfully predicted case times for both hysterectomies and myomectomies, outperforming the institutional standard. We found that the hysterectomy and myomectomy models reduced 15-minute time blocks by 7% and 24% compared to baseline, respectively.
Conclusions: Our operation-specific machine learning model offers a state-of-the-art means to predict surgical case times for robotic-assisted hysterectomies and myomectomies. Optimizing OR scheduling using machine learning holds broader implications for improving patient satisfaction, reducing costs, and increasing surgical throughput, aligning with the pursuit of value-based care in surgical departments. We are currently expanding our model to include other surgical operations.
18. Evaluating Atrial Fibrillation-Related Content on TikTok: A Social Media Analysis
Azeem Rathore1, Jahanzaib Ekram2, Syeda F. Zaidi3, Mobeen Z. Haider4, Dinesh Kadariya5
1. Internal Medicine, University of Florida Health Science Center, Jacksonville, FL, United States.
2. Morsani College of Medicine, University of South Florida, Tampa, Florida H. Lee Moffitt Cancer Center and Research Institute, University of South Florida, Tampa, FL, United States.
3. Queen Mary University, London, United Kingdom.
4. Internal Medicine, Carle Foundation Hospital, Jacksonville, IL, United States.
5. Cardiology, University of Florida Health Science Center, Jacksonville, FL, United States.
Purpose of Study: Atrial fibrillation (AF) is a prevalent cardiac arrhythmia affecting millions worldwide. Given the growing influence of social media as a source of healthcare information, there is a need to investigate the dissemination of AF-related content on popular platforms such as TikTok. This study aims to evaluate the credibility and content sources of AF-related information on TikTok, focusing on healthcare professional involvement, content categorization, and the presence of evidence-based information.
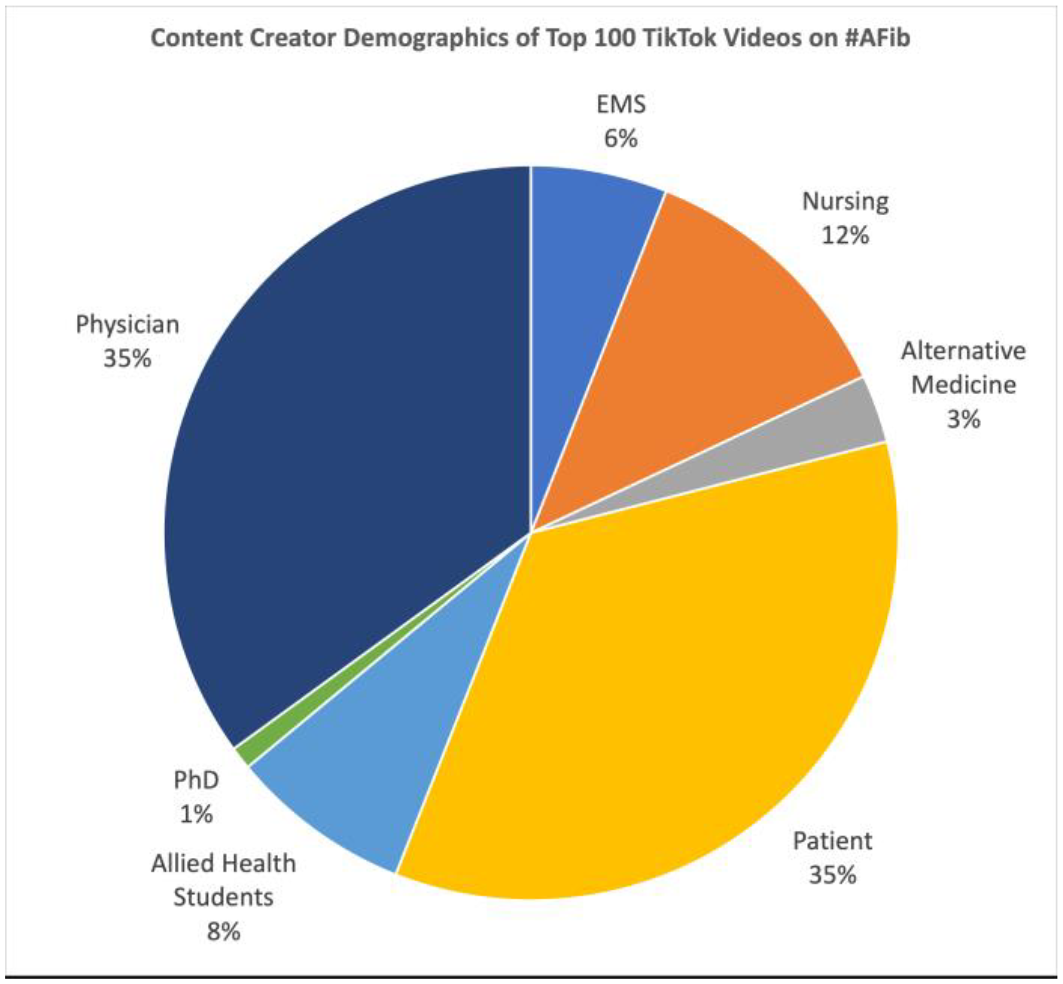
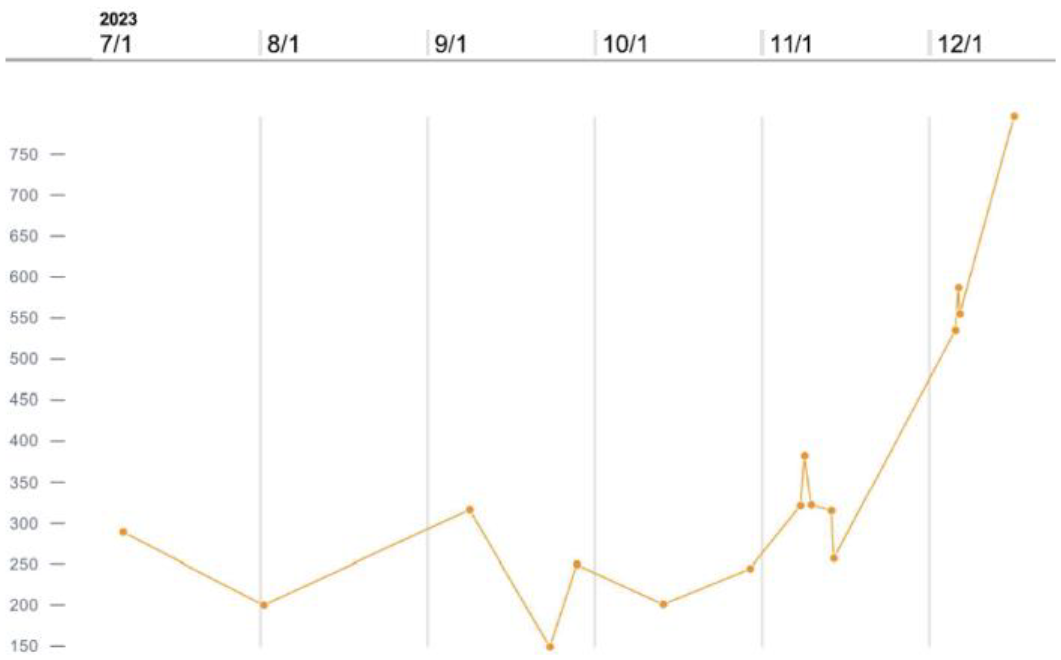
Methods Used: The most widely used hashtag associated with atrial fibrillation was identified as #afib. The top 100 videos were identified on December 3, 2023. Video titles, content creator credentials, posted date, number of views, number of likes, and number of comments were extracted. Descriptive analyses were conducted via TikTok Creator Center and Microsoft Excel 2024.
Summary of Results: Of the top 100 videos on #afib, a total of 50.8 million views were amassed with the earliest video shared in September 2019. The backgrounds of all creators were identified and the proportion of their videos were aggregated in Figure 1. Patients (35%) and Physicians (35%) were the two most popular backgrounds of creators. Among physicians, cardiologists shared the most content (57%) followed equally by anesthesiologists (15%) and internists (15%). Of shared content, 58% was educational, 29% was patient experiences with AF, and the remaining 13% was primarily satire/comedy about AF. The two most popular videos (36.6 million views) were recordings of cardioversions that were posted by paramedic TikTok users with educational commentary. Amongst educational videos, the topics most discussed included ECG analysis (31%) and medical treatments (26%). Of note, none of the top 100 videos had any references to medical literature either under the video description or within the video itself.
Conclusions: Despite the popularity of AF-related content on TikTok, there is a notable absence of evidence-based references among content creators. This absence raises concerns regarding the credibility and accuracy of the information disseminated, especially in a health context where misinformation can have serious consequences. Furthermore, while educational content comprises a significant portion of the discourse, the lack of citation to medical literature by physician content creators underscores the need for improved standards of information dissemination on social media platforms. Moving forward, efforts to promote collaboration between healthcare professionals and social media influencers could enhance the quality and reliability of health-related content on platforms like TikTok, ensuring that users have access to accurate and evidence-based information regarding atrial fibrillation and other medical conditions.
19. Prognostic Impact of Statins for Early-Stage Non-Small Cell Lung Cancer Patients following Image-Guided Radiofrequency Therapy
Anna L. Slingerland1, Ian Christie1, John Ryan2, Matthew Schuchert1, James Luketich1, Ryan Levy1, Arjun Pennathur1
1. Division of Thoracic and Foregut Surgery, Department of Cardiothoracic Surgery, University of Pittsburgh School of Medicine, the University of Pittsburgh Medical Center and UPMC Hillman Cancer Center, Pittsburgh, PA, United States.
2. Department of Cardiothoracic Surgery, University of Pittsburgh Medical Center, Pittsburgh, PA, United States.
Purpose of Study: Lung cancer is the leading cause of cancer-related mortality worldwide. NSCLC accounts for 85% of lung cancers. 25% of early-stage NSCLC patients are not candidates for surgery due to medical comorbidity. Image-guided RFA is a well-recognized option for these patients. There is an interest in the use of statins for their antitumor effects particularly in high-risk NSCLC patients. We investigated the impact of statin use with overall survival (OS), progression free survival (PFS), and response following RFA.
Methods Used: Patients with biopsy proven stage I NSCLC who underwent image-guided RFA from 2001-2018 were included. Primary outcomes were OS, PFS, and response at 3-6 months post-RFA (RECIST criteria). Statin use at surgery, 1-year postop, and any time 1-year preop to last follow-up was collected. Univariable analyses were performed by Wilcoxon rank sum tests for continuous variables, and Chi-square and Fisher’s exact tests for categorical variables. Unadjusted survival models were performed by the Kaplan-Meier method.
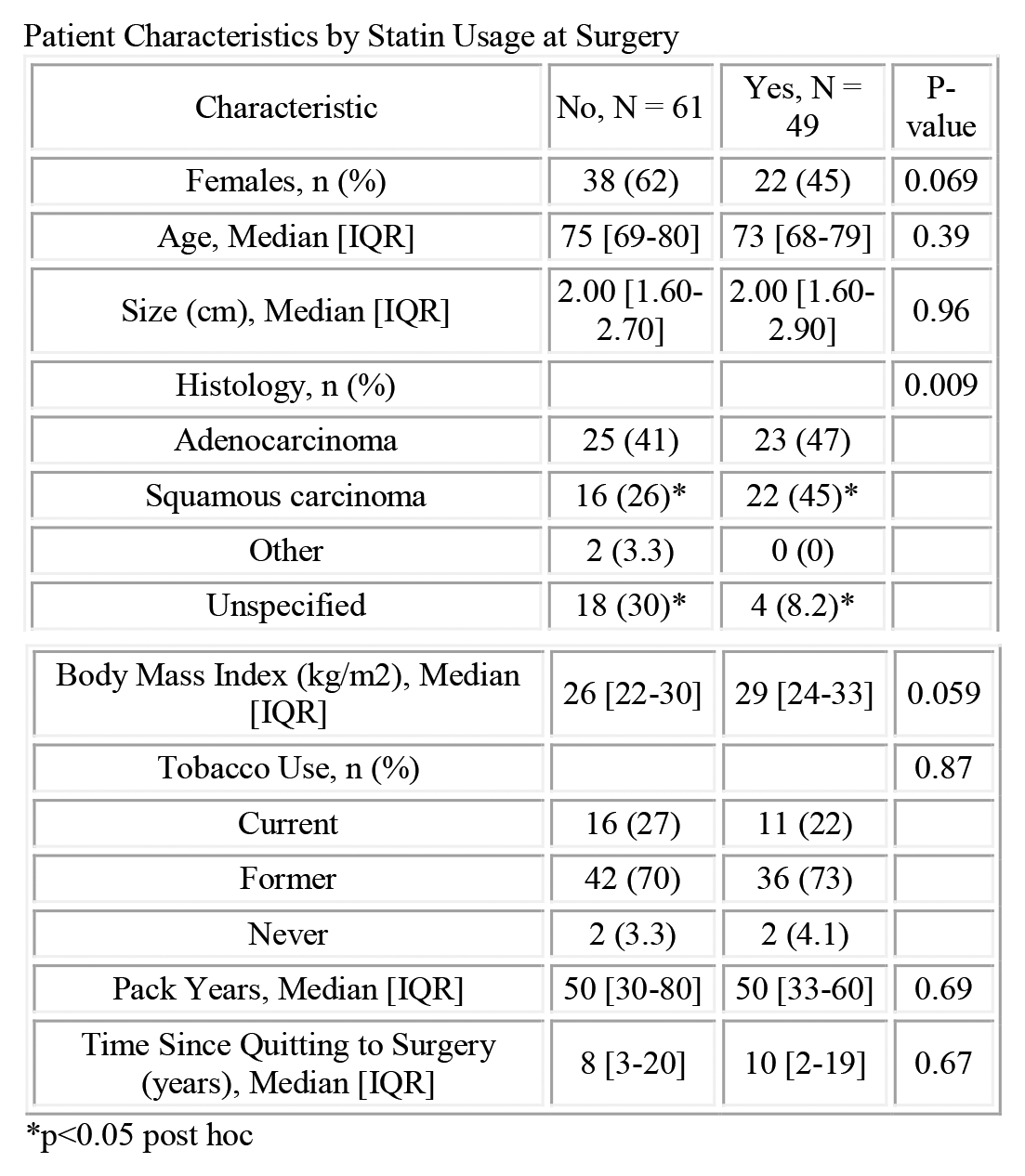
Summary of Results: A total of 111 patients (60 females; median age 74) underwent RFA for NSCLC. Medication data was unavailable at time of surgery for 1 (0.9%) patient and at 1-year follow-up for 30 (27%) patients. At surgery, 49 (44.5%) patients were on statins. Twenty-two (45%) of these patients had squamous cell carcinoma (SCC) compared to only 16 (26%) patients not on statins (p=0.009). Body mass index (BMI) was 29 kg/m2 (IQR:24-33) for patients on statins compared to 26 (IQR:22-30) for patients not on statins at surgery (p=0.059). Statins were not significantly associated with OS, PFS, or response rate. However, for patients who were on statins from anytime 1-year preop until last follow-up, there was a trend toward improvement in overall survival (p=0.093). Pack years at surgery was a significant predictor of OS (HR:1.01, CI: 1.00-1.01, p=0.015).
Conclusions: Statin usage was not significantly associated with outcomes after image-guided RFA for Stage 1 NSCLC. Patients on statins had significantly higher incidence of SCC tumors, which are associated with worse outcomes. Smoking history at surgery was associated with oncologic outcomes. Further investigation with a larger cohort and with propensity adjustment for confounding variables is planned.
Patient Characteristics by Statin Usage at Surgery
Time Since Quitting to Surgery (years), Median [IQR]
8 [3-20]
10 [2-19]
0.67
p<0.05 post hoc.
20. Amiodarone-associated Bone Marrow Granulomas: Review of Literature
Navneet Kaur1, Ravneet Kaur2
1. Internal Medicine, North Alabama Medical Center, Florence, AL, United States.
2. Government Medical College, Amritsar, Amritsar, India.
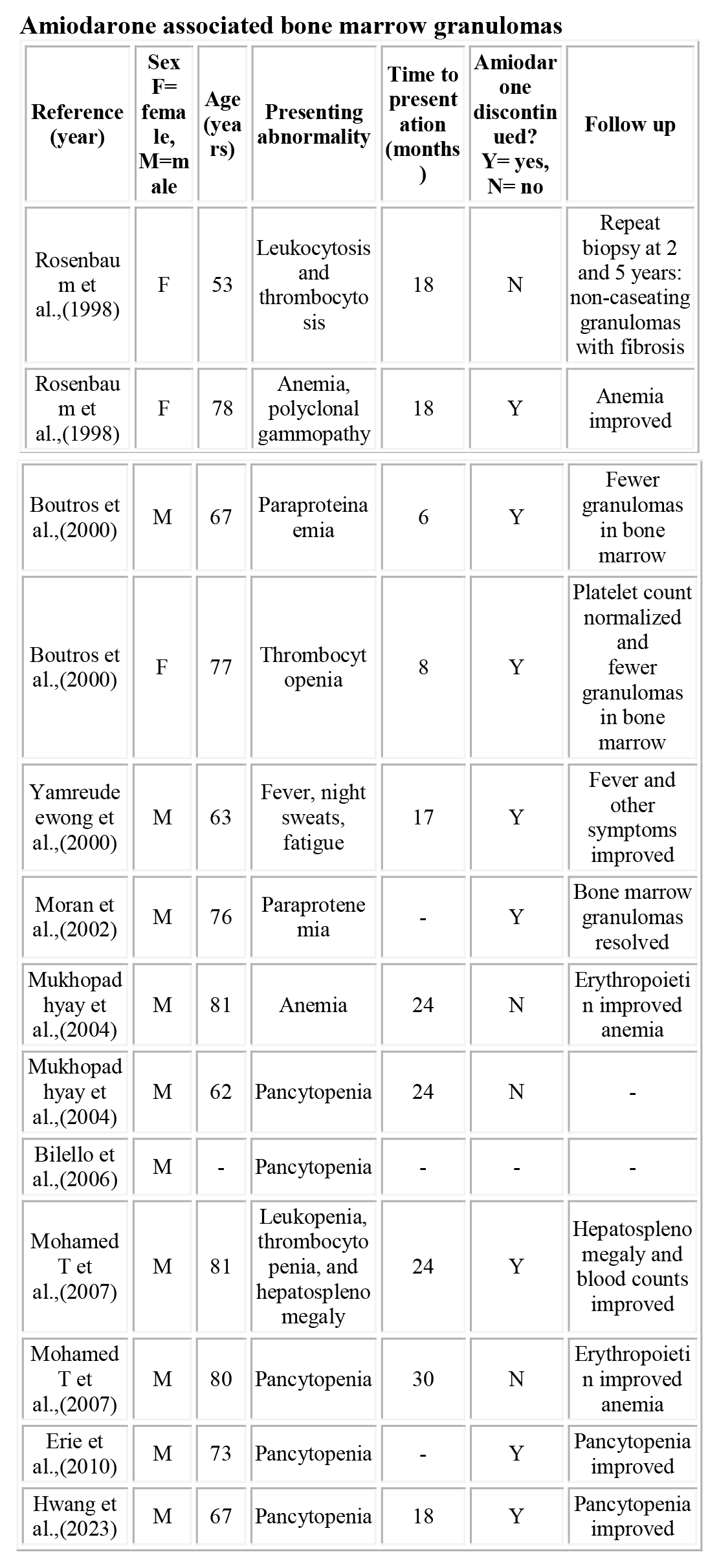
Purpose of Study: Amiodarone is a class III antiarrhythmic medication and comes with a handful of adverse effects. However, one particular hematological disorder is rather interesting. Although infrequent, there have been reports of amiodarone-associated bone marrow granulomas (BMGs). This abstract looks at all the reported cases of amiodarone-associated BMGs in literature, hematological oddities at presentation, and what to expect after discontinuing the drug.
Methods Used: We searched for related literature on Pubmed, Research Scholar, and Blood, using pre-specified terms “amiodarone” and “bone marrow granuloma". We identified all the case reports and conducted descriptive analysis.
Summary of Results: We identified 13 cases of BMGs associated with amiodarone reported to date. Male: female ratio was 10:3. The median age of patients was 74.5 years (range: 81-53). The median time to presentation was 18 months (range: 30-6) after starting amiodarone. The most common hematological abnormality was pancytopenia. Other presentations included leukopenia, thrombocytopenia, thrombocytosis, anemia, paraproteinemia, polyclonal gammopathy, and hepatosplenomegaly. Bone marrow biopsies were done in all the cases and revealed non-caseating granulomas. Amiodarone was stopped in 8 cases, with a resolution of symptoms. In two cases where it could not be discontinued, erythropoietin use improved anemia.
Conclusions: Clinicians should consider amiodarone as a potential cause of hematological abnormalities, especially pancytopenias. Discontinuing amiodarone reverses the granulomas and cytopenias and may reduce the need for transfusions. If stopping amiodarone is not an option, erythropoietin can be considered for anemia.
Amiodarone associated bone marrow granulomas
Reference (year)
Sex
F= female, M=male
Age (years)
Presenting abnormality
Time to presentation (months)
Amiodarone discontinued?
Y= yes, N= no
Follow up
Rosenbaum et al.,(1998)
F
53
Leukocytosis and thrombocytosis
18
N
Repeat biopsy at 2 and 5 years: non-caseating granulomas with fibrosis
Rosenbaum et al.,(1998)
F
78
Anemia, polyclonal gammopathy
18
Y
Anemia improved
Boutros et al.,(2000)
M
67
Paraproteinaemia
6
Y
Fewer granulomas in bone marrow
Boutros et al.,(2000)
F
77
Thrombocytopenia
8
Y
Platelet count normalized and
fewer granulomas in bone marrow
Yamreudeewong et al.,(2000)
M
63
Fever, night sweats, fatigue
17
Y
Fever and other symptoms improved
Moran et al.,(2002)
M
76
Paraprotenemia
-
Y
Bone marrow granulomas resolved
Mukhopadhyay et al.,(2004)
M
81
Anemia
24
N
Erythropoietin improved anemia
Mukhopadhyay et al.,(2004)
M
62
Pancytopenia
24
N
-
Bilello et al.,(2006)
M
-
Pancytopenia
-
-
-
Mohamed T et al.,(2007)
M
81
Leukopenia, thrombocytopenia, and hepatosplenomegaly
24
Y
Hepatosplenomegaly and blood counts improved
Mohamed T et al.,(2007)
M
80
Pancytopenia
30
N
Erythropoietin improved anemia
Erie et al.,(2010)
M
73
Pancytopenia
-
Y
Pancytopenia improved
Hwang et al.,(2023)
M
67
Pancytopenia
18
Y
Pancytopenia improved
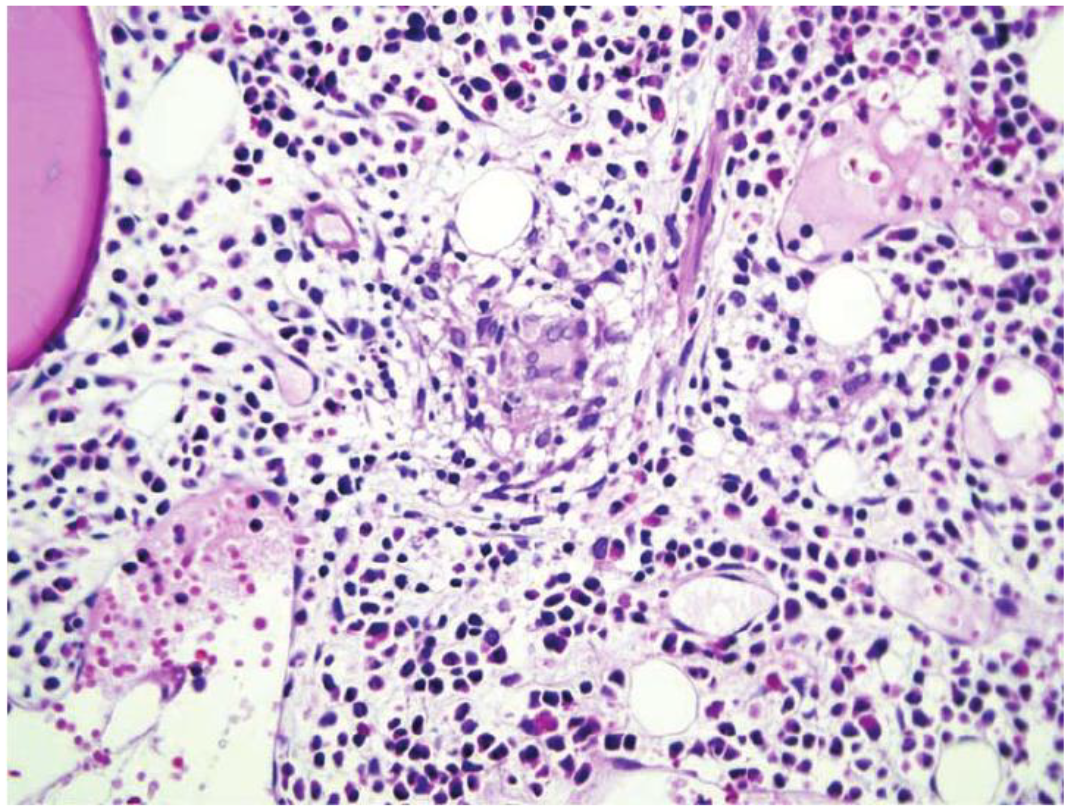
Non-caseating granulomas on bone marrow biopsy, benign appearing macrophages interspersed with small lymphocyte. (Miller et al., 2007)
21. Modeling Nilotinib in the Treatment of Alzheimer’s Disease in Cell Culture: Evaluation of a Repurposed Drug
Bi Zhang1, 2, Ankita Srivastava1, Heather A. Renna1, Maryann Johnson1, Katie M. Sheehan1, Aaron Pinkhasov3, Irving H. Gomolin1, Joshua De Leon1, Allison B. Reiss1
1. Departments of Medicine and Foundations of Medicine, NYU Grossman Long Island School of Medicine, Mineola, NY, United States.
2. New York Institute of Technology College of Osteopathic Medicine, Old Westbury, NY, United States.
3. Psychiatry, NYU Grossman Long Island School of Medicine, Mineola, NY, United States.
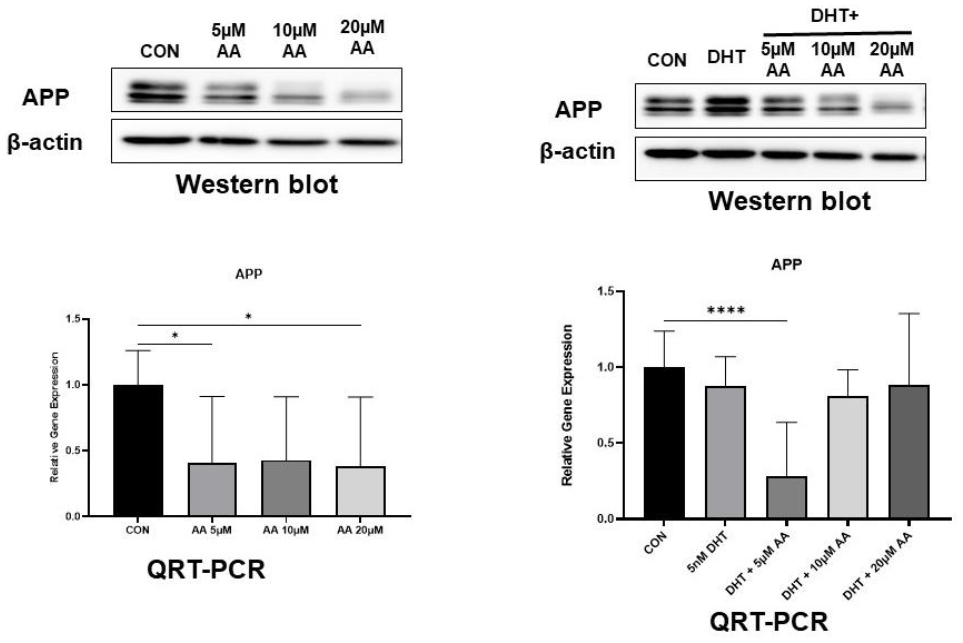
Purpose of Study: Alzheimer’s disease (AD) is a progressive neurodegenerative disorder that results in cognitive impairment, behavioral changes, and ultimately death. Pathological characteristics include deposition in the brain of misfolded proteins in the form of extracellular amyloid-β plaques, and intracellular neurofibrillary tangles (NFTs) of hyperphosphorylated tau. Nilotinib, a tyrosine kinase inhibitor that targets the c-Abl signaling pathway, is used to treat chronic myeloid leukemia positive for the Philadelphia chromosome. Increased expression of c-Abl is associated with both neuritic plaques and NFTs in the AD brain, prompting evaluation of this drug as an AD therapy. Nilotinib crosses the blood brain barrier and reduces c-Abl phosphorylation, amyloid-β levels, and dopaminergic neuron degeneration in an AD mouse model. Our study investigates the effects of nilotinib on amyloid processing and mitochondrial functioning in the SH-SY5Y human neuroblastoma cell line.
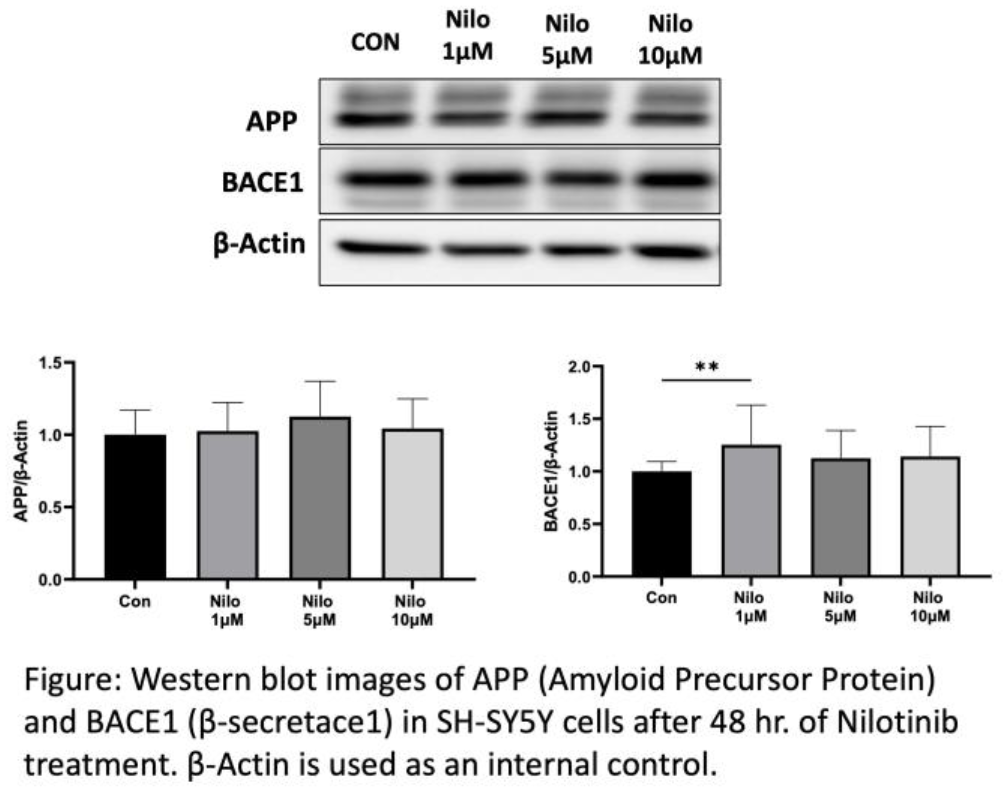
Methods Used: SH-SY5Y cells were exposed to 1, 5, and 10 µM of nilotinib. QRT-PCR was performed after 24 hr. of nilotinib treatment and data was analyzed using the 2ΔΔCt method with specific primers for the following markers: amyloid precursor protein (APP), β-secretase-1 (BACE1), mitochondrial transcription factor (TFAM) and Nuclear Respiratory Factor (NRF)1 with GAPDH as the housekeeping gene. Western blotting was performed after 48 hr. of nilotinib exposure using antibodies to the corresponding proteins. The immunoreactive proteins were detected using Electrochemiluminescence Western blotting detection reagents and the Bio-Rad ChemiDoc Touch Imaging System. Loading in each lane was validated using β-actin as an internal loading control. Quantification of Western blots were performed by using Image J software.
Summary of Results: APP and BACE1 are involved in amyloid-β formation while TFAM and NRF1 regulate mitochondrial fission-fusion balance. No significant difference in mRNA level of APP or BACE1 was observed with nilotinib treatment compared to vehicle control. In agreement with message level, there was no change in APP protein. However, BACE1 increased with 1 µM nilotinib (P=0.003). There was no difference in mRNA or protein level of TFAM or NRF1.
Conclusions: Our findings in a human neuronal cell model do not support efficacy of nilotinib treatment in AD. Neuroprotective effects were not found for the drug in 2 major hallmarks of AD pathogenesis: amyloid processing and mitochondrial functioning. Further investigation to determine possible mechanisms of neuroprotection with nilotinib using neurons derived from AD subjects is warranted as we await results of clinical trials.
22. Implementing a Patient Reported Outcomes Survey for Transgender and Gender Diverse Patients at a Gender Health Clinic in Birmingham, Alabama
Sunya Reddy1, Kelly W. Gagnon2, Brooke Penney3, Alfredo L. Guzman3, Brianna Patterson4, Baker Smith1, 5, Krishmita Siwakoti6, Olivia T. Van Gerwen2
1. Heersink School of Medicine, University of Alabama at Birmingham, Birmingham, AL, United States.
2. Division of Infectious Diseases, University of Alabama at Birmingham, Birmingham, AL, United States.
3. Research & Informatics Service Center, University of Alabama at Birmingham, Birmingham, AL, United States.
4. Department of Sociology, University of Alabama at Birmingham, Birmingham, AL, United States.
5. School of Public Health, University of Alabama at Birmingham, Birmingham, AL, United States.
6. Division of Endocrinology, Diabetes and Metabolism, University of Alabama at Birmingham, Birmingham, AL, United States.
Purpose of Study: Approximately 1.6 million Americans identify as transgender and gender diverse (TGD), yet health outcomes research focused on TGD patients is lacking. This gap persists despite significant health disparities experienced by TGD patients, including high rates of depression and suicidality. In clinical settings, patient-reported outcomes (PRO) surveys can pinpoint immediate clinical needs for individual patients while also generating health outcomes data. This study describes early outcomes and implementation of PROs for TGD patients being seen at the Gender Health Clinic at the University of Alabama at Birmingham.
Methods Used: We generated a REDCap-based PRO survey which included validated surveys to assess depression (the Patient Health Questionnaire-2 [PHQ-2], Patient Health Questionnaire-9 [PHQ-9] and gender dysphoria (Utrecht Gender Dysphoria Scale). Acceptability, appropriateness, and feasibility metrics were also collected. Patients completed the survey on iPads at triage.
Summary of Results: Between June and December 2023, 48 patients completed surveys during their clinic visit, including transwomen (n=21), transmen (n=20), nonbinary (n=9), genderqueer (n=3), and gender non-conforming (n=3) people. Approximately two-thirds of patients (n=30; 63%) had PHQ-2 scores of 0-1, indicating a positive depression screening among the remaining third (n=18; 37%). The average gender affirmation score was 18.13 (SD=2.25), indicating satisfaction with their self-identified gender. The average gender dysphoria score of 56.58 (SD=9.90) indicated significant distress due to the mismatch between their gender identity and sex assigned at birth. Patients found the survey highly acceptable (85%), appropriate (97.8%), and feasible (93.6%). Several challenges were encountered during implementations including REDCap technical issues, staffing and workflow complexities, and occasional patient difficulty with independent PRO completion.
Conclusions: This project reveals challenges in integrating novel screening strategies for monitoring the health of TGD patients in busy clinical settings. Despite thorough preparation, our team faced implementation barriers requiring continual adaptation. Preliminary insights highlight key aspects of trans health: gender affirmation, gender dysphoria, and depression. As data collection continues, we aim to better understand the interplay between depression and gender dysphoria while also collecting substance use data within this population. Overcoming implementation challenges will expand the PROs’ dissemination, better inform clinical decision-making and care planning, and serve as a valuable dataset for future research endeavors.
CASE REPORTS
C1. Paraphenylenediamine as the Causative Agent for Pathologic Cutaneous Reaction to a Permanent Multicolor Tattoo
Eliot Parascandolo1, Samuel Puglisi3, Gregory Puglisi2
1. NCH Healthcare System, Naples, FL, United States.
2. Mid-Island Allergy Group, Plainview, NY, United States.
3. University of Maryland, College Park, MD, United States.
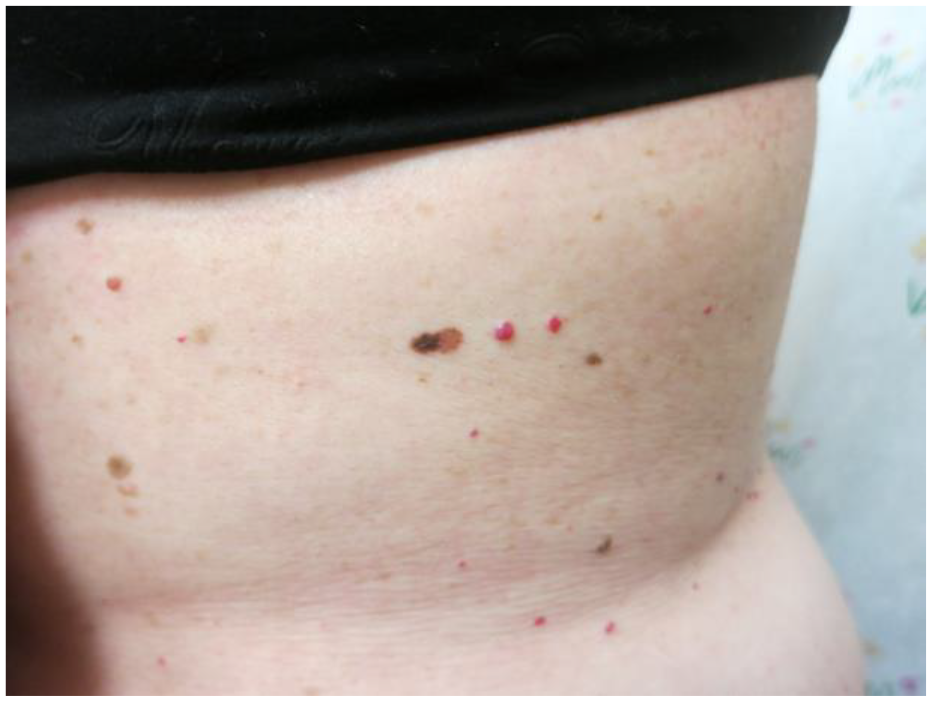
Rationale: Paraphenylenediamine (PPD) has been implicated in allergic contact dermatitis (ACD) in the literature. Although this has been described in temporary tattoos, the definite implication of PPD in permanent tattoos has not been described. We report a patient who developed severe ACD requiring skin grafting after receiving a permanent tattoo.
Methods: Smartpractice AC-core series was utilized for patch testing and the safety data sheets for each tattoo ink color were obtained.
Results: A 30-year-old female with a past history of atopic dermatitis and psoriasis presented with a cutaneous reaction to a recent tattoo that she obtained one week prior (Figure 1). The patient was previously identified on patch testing to have a PPD allergy after evaluation for irritation from hair dye. Following the tattoo placement, she applied soap and bacitracin cream which she had used several years prior on a similar tattoo. On presentation, she was found to have a deep ulcerated plaque with an indurated border encompassing the area of the tattoo. She was referred to the emergency department and admitted for treatment, ultimately requiring debridement and skin grafting. The patient obtained the safety data sheets for the tattoo inks which revealed PPD as an ingredient in every color.
Conclusion: We believe this is the first confirmed case of paraphenylenediamine being implicated as the causative agent for ACD to a permanent tattoo. Tattoo ink is unregulated and formulas are proprietary which makes safe practice difficult for patients with sensitivities. We advocate for consistent ingredient labeling, regulation, and transparency within the tattoo ink industry.
C2. Fertility-Preserving Strategies in Xanthogranulomatous Oophoritis: A Case Report on Surgical Decision-Making and Multimodal Treatments
Alisha K. Daroch1, 2, Michelle Greenman2, Aaron Nizam2, Jill Whyte2
1. CUNY School of Medicine, New York, NY, United States.
2. Northwell Health, New York, NY, United States.
History: A 22-year-old G0P0 female presented with a chief complaint of acute pelvic pain. No other symptoms were noted. She had a known prior history of an ovarian cyst for which she was previously offered minimally invasive surgical management but declined. Past medical and family histories were unremarkable.
Physical examination findings: Pelvic examination findings revealed a large fixed immobile mass palpable to the level of the umbilicus with fixed nodules at the rectovaginal septum, warranting further imaging.
Laboratory or Diagnostic imaging or Procedures: On ultrasound, an 11-centimeter complex adnexal mass was identified. The patient underwent a planned exploratory laparotomy, with the goal of ovarian cystectomy. However, intraoperatively, the adnexa and uterus were found to be indistinguishable from the mass, prompting concerns for malignancy. Procedure was aborted to avoid a premature total hysterectomy with bilateral salpingo-oophorectomy. Biopsy and culture specimen collections were sent for further evaluation.
Final Diagnosis and Further Interventions: Final pathology revealed xanthogranulomatous oophoritis. Following culture results, antibiotics were appropriately tailored to Klebsiella Pneumoniae. The patient underwent a cumulative 2 weeks of IV antibiotics with persistent pelvic drainage before improvement was noted. Oral antibiotics were continued for 4 weeks thereafter. The patient then returned 8 weeks after the initial encounter for an altered course of surgical treatment involving only a right salpingo-oophorectomy due to the decrease in mass size that resulted from the alternative interventions.
Discussion: Xanthogranulomatous Oophoritis is an uncommon form of chronic inflammation rarely found in the female genital tract. When present, it is typically restricted to the endometrium. Only a limited number of cases in the ovary have been reported. While oophorectomy still remains the standard choice of treatment for xanthogranulomatous oophoritis, aggressive antibiotic use and cautious surgical judgment should be implemented to limit invasive surgical intervention. Due to its resemblance to ovarian malignancy, preoperative diagnosis remains a challenge and must be addressed to avoid unnecessary invasive procedures that can impact fertility for females of reproductive age. As in the present case, suspicions of adnexal malignancies must be investigated with appropriate pathology review due to the possibility of a non-neoplastic etiology such as xanthogranulomatous oophoritis which could warrant alternative treatments. Implementing this multimodal approach, rather than a “one size fits all” strategy towards complex adnexal masses could allow for fertility preservation and thereby an improvement in quality of life for affected females of reproductive age.
C3. Recurrent Malignant Phyllodes of the Breast: A Case Report
Veronica M. Smith1, Emory B. Johnson2, Caroline Schreeder1
1. UABSOM, Birmingham, AL, United States.
2. UABSOM, Birmingham, AL, United States.
Introduction: Phyllodes tumors are rare and comprise only 0.3-0.9% of breast neoplasms, and among these, malignant types are even more scarce, accounting for 10-30% of phyllodes cases. The primary approach to treatment involves surgical resection with local recurrence rates being highest for malignant phyllodes at 23-30%. This case of recurrent malignant phyllodes offers unique insights into the complexities of this uncommon disease process.
Case Description: Mrs. B is a 62-year-old female who presented three months after her last normal mammogram due to an irregular lump in the outer quadrant of her right breast. Ultrasound revealed a suspicious mass, which led to a biopsy to confirm the diagnosis of borderline phyllodes with areas featuring malignant phyllodes characteristics. She underwent a partial mastectomy with final pathology showing a 5.5 cm mass with 1 cm clear margins.
At the patient’s six-month follow-up, she stated that 3 months ago she noticed a mass near her surgical scar that had progressively grown. The patient underwent a core biopsy of the mass that confirmed malignant phyllodes. She has no family history of breast or ovarian cancer and genetic testing was negative.
Mrs. B underwent a complete right mastectomy with immediate tissue expander reconstruction. The final pathology revealed a 7.5 cm malignant phyllodes tumor with a small 5 mm incidental focus of ductal carcinoma in situ (DCIS) that was estrogen receptor (ER) and progesterone receptor (PR) positive. She had positive margins with respect to the phyllodes tumor and underwent re-excision to achieve negative margins. 6 weeks later she started whole breast radiation therapy.
Discussion: A systematic review and meta analysis recorded that there was a 24% reduction of local recurrence of malignant phyllodes with surgical margins at or greater than 10 mm. NCCN guidelines report that no tumor on ink on pathologic analysis is sufficient. The average time to recurrence is 2 years. This patient noticed a breast mass within 3 months of initial excision. This begs the question about adjuvant radiation as part of the standard treatment algorithm. Current treatment of local recurrence includes re-excision with wide margins and or mastectomy with possible adjuvant radiation. This case highlights the importance of furthering our understanding of malignant phyllodes and various treatment strategies, including making radiation a part of the process.
C4. Mirror Syndrome: Unveiling Diagnostic Challenges and Therapeutic Strategies in a Rare Obstetric Phenomenon
2. CUNY School of Medicine, New York, NY, United States.
History: A 26 year old G1P0 female presented at 29 weeks gestation with progressively worsening bilateral lower extremity edema for the past two weeks. Symptoms had failed to resolve with elevation and compression stockings. A 60-lb weight gain was also noted, with 25-lbs gained in the previous month. All other aspects of the pregnancy were uncomplicated. No significant past medical history was reported. Family history was positive for a recent diagnosis of systemic lupus erythematosus (SLE) in her mother.
Physical Examination Findings: Vital signs were within normal limits. Further evaluation of the edema revealed 3+ bilateral pitting edema of the lower extremities.
Laboratory and Diagnostic Imaging: Laboratory findings were significant for anemia, proteinuria, and an elevated creatinine of 0.88 mg/dl. Ultrasound revealed fetal hydrops (fetal edema) with findings of scalp edema, significant abdominal ascites, and mild pulmonary and pericardial effusions.
Final Diagnosis and Further Interventions: Given the obscure maternal and fetal findings, a rare diagnosis of mirror syndrome was made. Following the diagnosis, a workup was conducted to explore possible etiologies. Fetal echocardiogram revealed no structural abnormalities and maternal evaluation for possible infectious etiologies was negative. Premature cesarean delivery was indicated to minimize life-threatening complications due to the absence of an identifiable cause. Following delivery, maternal improvement of symptoms was reported by postoperative day 4 with eventual recovery of the neonate following appropriate NICU intervention.
Discussion: Mirror syndrome is a rare phenomenon characterized by the simultaneous occurrence of fetal hydrops, maternal edema, and placentomegaly. Since its first classification in 1956, only 113 cases have been reported in the literature as of 2016. Previous studies have highlighted factors like rhesus isoimmunization, viral infections, placental tumors, and fetal malformations as potential triggers but the definitive cause remains elusive. For cases such as ours that lack a specific etiology, immediate delivery is often the recourse to alleviate symptoms. The diagnostic challenge lies in differentiating mirror syndrome from preeclampsia, a condition marked by maternal hypertension and proteinuria, accompanied by significant maternal edema. Misdiagnosis could be fatal, given that preeclampsia, particularly in its early stages, generally requires a less intensive treatment. The presence of fetal hydrops and placentomegaly, which are rarely observed in preeclampsia, may be indicative. Furthermore, mirror syndrome carries a higher risk for intrauterine fetal demise, emphasizing the critical need for early detection to potentially avert a premature birth. Establishing ultrasound as a standardized guideline for pregnant patients exhibiting significant edema may potentially facilitate the early identification of mirror syndrome, with improved maternal-fetal prognosis.
C5. Rock Solid Lungs? Pulmonary Cement Embolism after Kyphoplasty
Introduction/Background: Kyphoplasty and Vertebroplasty have become cornerstones in the management of vertebral compression fractures (VCFs), offering substantial pain relief and functional improvement for patients. However, despite its efficacy and safety profile, these procedures carry inherent risks, some of which may lead to unforeseen complications. We present a case report detailing a rare but potentially life-threatening complication following Kyphoplasty: cement embolism.
Description: The patient is a 47-year-old male with history of two thoracic vertebral compression fractures of unknown etiology who presents with a chief complaint of chest pain and dyspnea. Three days prior to admission, he underwent kyphoplasty with bone biopsy to determine the etiology of his compression fracture. On admission, his vital signs were significant for tachycardia and hypoxia and labs were within normal limits. His chest x-ray showed bilateral basilar opacities. CTA of the chest showed multiple hyperdense lesions in the right lower lobe pulmonary artery, right upper lobe pulmonary arteries, left lower lobe pulmonary artery branch that were concerning for barium cement emboli. Additionally, a low-density distal thrombus in the pulmonary artery supplying the right lower lobe was noted. Interventional Radiology performed a pulmonary angiogram which showed only a small foci of linear cement embolization that was not flow-limiting with a pulmonary artery pressure of 27 mmHg. Retrieval of cement emboli was deemed not necessary, and the patient was started on heparin for anticoagulation and closely monitored for changes in respiratory status. He was eventually discharged home with oral anticoagulation therapy.
Discussion and Conclusion: The exact incidence of cement embolisms (containing Poly Methyl Meth Acrylate, bone cement) following Kyphoplasty/Vertebroplasty procedures is not precisely defined. However, studies suggest that the occurrence of cement embolisms ranges from approximately 1% to 3%. Several factors contribute to the risk of cement embolism, including the volume of cement injected, the viscosity of the cement used, the technique employed during the procedure, and the underlying vascular anatomy of the patient. Additionally, the presence of pre-existing venous or pulmonary pathology may increase the likelihood of embolic events.
Healthcare providers should maintain a high index of suspicion for embolic events in patients presenting with sudden respiratory distress, chest pain, or neurological deficits following these procedures. Cement embolisms by themselves do not necessitate anticoagulation and are not associated with an increase in all-cause mortality. Providers may consider anticoagulation if there is an arterial clot present, as there was in our patient. Treatment is mostly conservative but can also include percutaneous or surgical removal of large cement emboli.
CXR on admission
CTA on admission
C6. Take my Breath Away: Hydropneumothorax as an initial Presentation of Malignancy
1. University of Florida College of Medicine Jacksonville, Jacksonville, FL, United States.
Introduction: We explore the case of an elderly male patient who presented with respiratory failure and was discovered to have a sizeable left hydropneumothorax. While hydropneumothoraces are often seen in the face of thoracic trauma, tuberculosis, or following thoracentesis, our patient had none of these risk factors. Further investigation into this patient led to a new diagnosis of an intrathoracic malignancy.
Case Presentation: A 78-year-old male with tobacco use disorder presented with progressively worsening shortness of breath. An initial chest radiograph showed significant left-sided lung collapse by a large volume of intrapleural air, with an associated dense fluid level in the left pleural space, suggestive of a left hydropneumothorax. A pigtail pleural catheter was inserted, revealing serosanguinous, exudative fluid. The cytology of this fluid was noted to be benign. A computed tomography (CT) angiogram of the pulmonary vasculature showed numerous pulmonary nodules and masses bilaterally, the largest being 5.3 x 3.4 x 5.8 cm in the right upper lobe with evidence of cavitation) and right upper lobe pulmonary thromboembolism, raising the suspicion of an underlying malignancy. A detailed history revealed an unintentional fifty-pound weight loss over the past few months and a persistent non-productive cough over the past year. CT of the head, abdomen, and pelvis showed no findings of malignancy outside the thoracic cavity. Subsequent bronchoscopy with ultrasound-guided endobronchial biopsies of the left lung revealed a CK7 and CK20 positive malignancy, suggestive of lung adenocarcinoma versus gastrointestinal malignancy. On further discussion with the patient regarding investigations for the primary tumor and chemotherapy, the patient opted for hospice care.
Discussion: There is a paucity in the literature on the mechanism behind hydropneumothorax in lung malignancy. Intrathoracic malignancies are well known to impair both the lymphatic drainage of pleural fluid and increase fluid drainage into the pleural space. Furthermore, rupture of necrotic neoplastic tissue in or near the pleural cavity can lead to a spontaneous pneumothorax with an associated accumulation of fluid in the pleural space. Worldwide, tuberculosis remains the most common condition associated with hydropneumothorax, with iatrogenic introduction of air during thoracentesis also being standard. Our case describes a rarely described phenomenon of a hydropneumothorax as the initial presentation of an intrathoracic malignancy. We hope that clinicians being aware of this phenomenon can lead to earlier diagnosis of lung malignancy, which remains the leading cause of cancer-related death worldwide.
Chest radiograph shows air (red arrow) and fluid (blue arrow) in pleural space. The green arrow shows a pulmonary nodule, likely related to malignancy
A chest CT with contrast shows air (red arrow) and fluid (blue arrow) in the pleural space. The green arrow shows a pulmonary nodule, likely related to malignancy
1. North Alabama Medical Center, Florence, AL, United States.
2. Clearview Cancer Institute, Florence, AL, United States.
History: A hexagenarian female with a past medical history of myelofibrosis, status post failed stem cell transplantation 2 years ago, visited the emergency department due to worsening right lower quadrant abdominal pain over the last 2-3 months following a colonoscopy. The colonoscopy was noted to be unremarkable. She denied fever, nausea, vomiting, changes in bowel habits, or weight loss.
Physical Examination Findings: Upon physical examination, the patient displayed tenderness in the right lower quadrant without rebound tenderness or guarding. Bowel sounds were normal, and vital signs were within the normal range.
Laboratory or Diagnostic Imaging Findings: Routine laboratory results were unremarkable except for moderate anemia, with a hemoglobin level of 8.1g/dL, and thrombocytopenia, with a platelet count of 29×109/L. A recent abdominal CT scan performed a few days ago at another facility showed a large necrotic mass originating from the cecum, measuring 7.3 x 7.7 x 8.2 cm. Given the unremarkable recent colonoscopy results and undetectable carcinoembryonic antigen, the patient was started on broad-spectrum antibiotics-Vancomycin, levofloxacin, and metronidazole-for suspected abscess.
Despite antibiotic treatment, the patient’s abdominal tenderness persisted. A subsequent CT scan revealed that the necrotic cecal mass remained unchanged in size but extended into the right iliopsoas muscle and encircled the mid-right ureter and the right common iliac artery bifurcation, raising concerns about malignancy.
Final diagnosis: The repeated colonoscopy revealed a large infiltrative and ulcerated mass in the ascending colon, which had not been detected 2-3 months earlier. A biopsy of the mass confirmed high-grade B-cell lymphoma. Subsequently, the patient was referred to hematology/oncology and initiated chemotherapy with R-CVP (Rituximab, Cyclophosphamide, Vincristine, and Prednisolone).
Discussion: Lymphoma has multiple risk factors, including immunodeficiency. Hematopoietic stem cell transplantation (HSCT) recipients, in particular, face an increased risk of developing a lymphoproliferative disorder known as post-transplantation lymphoproliferative disorder (PTLD), with an incidence of 1~2%.
The patient is also diagnosed with PTLD by definition. However, this report describes diagnostic challenges as the rapid progression of cancer within a short timeframe of 2-3 months is highly uncommon. Additionally, the patient did not manifest any classical symptoms typically associated with malignancy, such as weight loss, night fever, or changes in bowel habits. This case underscores the potential for PTLD to develop rapidly with very nonspecific symptoms. Therefore, physicians should maintain a high level of suspicion for malignancy, especially when a patient with a history of transplantation presents with an atypical clinical presentation, as described in this case.
Abdominal/pelvis CT showing the mass measuring approximately 9.5 x 7.9 cm in greatest axial dimension and effacing the mid right ureter and right iliac artery bifurcation.
The picture of biopsy from the mass showing polymorphoneuclear cells with a high grade nucleus:cytoplasm ratio, consistent with malignancy.
C8. A Rare Case of Paraneoplastic Seronegative Neuromyelitis Optica Spectrum Disorder
1. North Alabama Medical Center, Florence, AL, United States.
2. Clearview Cancer Institute, Florence, AL, United States.
History: A female in her fifties with a past medical history of a left breast mass with lymph node involvement noticed one month before admission visited the emergency department due to blurred vision in her right eye, accompanied by ataxia and weakness in her right upper limb over the last 2-3 weeks.
Physical examination findings: Upon physical examination, the patient exhibited decreased vision in the right eye, reduced motor power (Grade 4/5), and impaired sensation in the right upper limb. Vital signs were within normal limits.
Laboratory or diagnostic imaging findings: Routine laboratory results were unremarkable. Brain MRI findings were also unremarkable and negative for demyelination or tumor. However, cervical MRI revealed uniform enhancement from C1 to C5. Optic nerve MRI showed bilateral enhancement of the optic nerves.
Final diagnosis: Taking into account the patient’s symptoms and imaging findings, she was tentatively diagnosed with neuromyelitis optica spectrum disorder (NMOSD). Treatment was initiated with high-dose steroids and plasmapheresis. Although a serology test for aquaporin-4 IgG (AQP4-IgG) returned to be negative, the treatment plan remained unchanged due to the consistency between the symptoms and MRI findings with NMOSD.
Following the treatments, the patient experienced partial improvements in visual disturbance and weakness. She was discharged with a follow-up appointment with neurology and hematology/oncology. Subsequent biopsy of the left breast mass revealed human epidermal growth factor receptor-positive breast cancer, leading to the initiation of chemotherapy.
Despite receiving oral steroids, the patient continued to experience waxing and waning neurological deficits. The patient’s NMOSD was suspected to be related to her breast cancer, based on the coexistence of both conditions and the observed treatment response. Consequently, she was diagnosed with paraneoplastic seronegative NMOSD.
Discussion: NMOSD is a rare autoimmune disease with an incidence of 1-10 per 1,000,000. Diagnostic criteria for NMOSD require at least one core clinical symptom (e.g., optic neuritis or acute myelitis) and positive serum AQP-IgG autoantibody. However, patients with a strong clinical suspicion of NMOSD rarely do not have the autoantibody, referred to as seronegative NMOSD. Diagnosis of seronegative NMOSD requires a minimum of two core presentations with concordant MRI imaging findings disseminated in space, as described in this case.
NMOSD also can rarely be associated with cancer. The patient, in this case, exhibited a temporal relationship between NMOSD and breast cancer, as evidenced by their coexistence. Additionally, her partial response to appropriate therapy suggested a secondary etiology of her NMOSD. These facts underscore the clinical connection between her cancer and NMOSD, supporting the diagnosis of paraneoplastic NMOSD. Improvement in her neurological symptoms can be expected with the treatment of the breast cancer.
Optic nerve MRI showing pronounced enhancement of the left optic nerve with enhancement of the right optic nerve primarily at the orbital apex
Cervical MRI demonstrating increased T2 signal with edematous changes to the spinal cord extending superiorly to the level of the C1 vertebral body through the mid C5 vertebral body
C9. A Complex Presentation of Bartonella Henselae Endocarditis
Santul Bapat1, Ronald G. Washburn2
1. Internal Medicine, Atrium Health Wake Forest Baptist, Winston-Salem, NC, United States.
2. Section of Infectious Disease, Atrium Health Wake Forest Baptist, Winston-Salem, NC, United States.
Background: Infective endocarditis is an important complication of bioprosthetic heart valves. Most cases are associated with bacteremia. Culture negative endocarditis is a less common and frequently missed diagnosis. Implicated pathogens include Mycobacteria, Bartonella henselae, Brucella, and Coxiella burnetii. We present a case of a patient with B. henselae endocarditis of a bioprosthetic valve complicated by central nervous system emboli.
Case: A 70-year-old male with history of bioprosthetic aortic valve replacement was evaluated for several months of intermittent fever, dyspnea, ataxia, and episodes of altered mental status. Over the course of six months, he had several ED visits and admissions, during which, blood cultures were consistently negative. Trans-thoracic echocardiogram was initially negative for any vegetation on his prosthetic aortic valve. MRI of the brain demonstrated multifocal subacute infarcts concerning for an embolic source. Due to persistent symptoms, trans-esophageal echocardiogram was obtained which showed a vegetation on the prosthetic aortic valve concerning for subacute endocarditis.
He was followed in infectious disease clinic and had extensive blood testing which was positive for Coxiella IgM titer of 1:512 as well as for Bartonella IgG titer of 1:2560. He was treated for presumed Q-fever endocarditis with doxycycline and hydroxychloroquine. His symptoms persisted on this regimen. Due to persistent symptoms, he had surgical replacement of his aortic valve and aortic root. Excised tissue was sent for pathological examination and broad range PCR was positive for B. henselae. At follow up with infectious disease, his antibiotic regimen was changed to doxycycline and rifampin. He had resolution of symptoms on this regimen.
Discussion: This patient had multiple risk factors for organisms known to cause culture negative endocarditis. He traveled abroad while in the military and had a farm where he raised animals known to harbor pathogens associated with culture negative endocarditis. In addition, he had kept cats as pets for years. His blood tests were significant for positive Q-fever IgM and B. henselae IgG. It was initially felt that Q-fever was causing his endocarditis and that B. henselae was positive due to chronic exposure to cats. Ultimately, broad spectrum PCR of his excised vegetation showed B. henselae as the causative organism. Given the lack of recurrence of altered mental status and ataxia after surgery and antibiotics, we concluded that previous septic emboli were driving his episodes of altered mentation.
Conclusion: Culture negative endocarditis is a potential cause of recurrent infectious symptoms. Any patient with recurrent infectious symptoms, particularly with a bioprosthetic valve, should undergo workup for endocarditis. Blood tests can help to narrow the differential but, as in this case, the gold standard for diagnosis is pathological examination of surgically excised tissue.
Trans-esophageal echocardiogram image demonstrating calciifed vegetation on the aortic valve.
MRI of the brain with multifocal hyperintensities suggestive of embolic strokes.
C10. Septic Emboli: A Unique Complication of Clostridium Septicum Induced Myonecrosis
1. College of Medicine, California Northstate University, Elk Grove, CA, United States.
2. Internal Medicine, Oroville Hospital, Oroville, CA, United States.
Introduction: Spontaneous clostridial myonecrosis is a life-threatening infection leading to rapid muscle destruction due to direct bacterial inoculation. Non-traumatic clostridial myonecrosis infections are predominantly caused by Clostridium septicum. These patients may have an underlying gastrointestinal malignancy, diabetes, and/or are immunocompromised. This case presents a rare association of nontraumatic spontaneous clostridial myonecrosis of the left arm preceding cerebral septic emboli with underlying invasive colorectal adenocarcinoma.
Case Presentation: A 60-year-old male with a history of hypertension and poorly controlled diabetes presented to the emergency department with left-sided chest pain radiating into his left shoulder, worsening since that morning. Workup in the ER revealed elevated D-dimer, troponin, CRP, WBC, and CPK. However, ultrasound of the left upper extremity (LUE) and CTA of the chest, abdomen, and pelvis revealed no significant findings.
In the ER, the patient decompensated requiring intubation and was treated for empiric sepsis. CT of the chest, LUE, and neck revealed innumerable soft tissue gas collections along the posterior aspect of the LUE.
Incision and drainage of the left triceps for myositis and possible necrotizing infection. Unexpectedly, the muscle was healthy-appearing with patches of ecchymosis. No purulence, necrosis, or visible gas were noted. A muscle biopsy was obtained, revealing myonecrosis. Exploration and deep excisional debridement was subsequently performed removing a 5x3 cm segment of tissue. Intraoperative muscle swab was positive for Clostridium septicum.
Postoperatively, the patient was transferred to the ICU where he required pressor support. In the subsequent days, the patient required several trips to the operating room for further debridement of the LUE. During this time, the patient’s status continued to deteriorate, developing rhabdomyolysis, AKI, and DIC. On day six, patient exhibited left-sided paralysis and brain CT revealed innumerable white matter infarcts indicative of septic emboli. TTE was negative for endocarditis. In the months following, the patient made slow neurologic recovery and underwent a colonoscopy, revealing cecal adenocarcinoma. Right hemicolectomy and loop ileostomy was successfully performed and the patient recovered in a skilled nursing facility.
Discussion: Mortality rates associated with C. septicum have been reported to be as high as 70%. Furthermore, studies report as many as half of all patients with C. septicum to have an associated colorectal malignancy. As such, it is imperative that every patient with confirmed C. septicum infection undergo appropriate screening. Furthermore, to our knowledge, this is the first case reported of septic emboli secondary to spontaneous myonecrosis with Clostridium septicum, highlighting a unique burden of emboli-induced neurological deficits. Early intervention is, thus, crucial to potentially mitigate the spread of infection.
C11. Posterior Reversible Encephalopathy Syndrome Leading to Diagnosis of Acute Post-Infectious Glomerulonephritis in a Pediatric Patient: A Case Report
Samuel Hayworth1, Desalyn L. Johnson1, Erinn O. Schmit2
1. University of Alabama at Birmingham Heersink School of Medicine, Birmingham, AL, United States.
2. Department of Pediatrics, University of Alabama at Birmingham Heersink School of Medicine, Birmingham, AL, United States.
History: An 8-year-old previously healthy female initially presented to the pediatric intensive care unit after new-onset seizure activity. 3 days prior, she began experiencing progressively severe headaches and rash over the left lower extremity. She continued to have headaches and soon after experienced several episodes of non-bilious, non-bloody emesis. The morning of presentation, she was found unresponsive, exhibiting right gaze deviation and clenched jaw. Further history revealed a recent Group A Strep pharyngitis infection, which was treated with a 10-day regimen of amoxicillin. During this time, her mother reported her daughter to have decreased oral intake but normal urinary output, without dysuria or hematuria.
Physical Examination: Vital signs were notable for temperature of 101.7 degrees Fahrenheit, heart rate of 100 beats per minute, blood pressure of 167/97, respiratory rate of 28, and oxygen saturation of 96% on room air.
At this time, the patient was drowsy but arousable. The neck was supple with no evidence of meningismus. The head, ears, eyes, nose, and throat exams were unremarkable. Cardiac auscultation showed regular rate and rhythm with normal S1 and S2. A skin exam revealed an erythematous, crusting rash, resembling poison ivy on the left lower extremity below the knee. A neurological exam revealed a Glasgow Coma Scale (GCS) of 14, with an eye sub-score of 4, verbal sub-score of 4, and motor sub-score of 6. The patient was somnolent but oriented to self and able to follow simple commands. Cranial nerves II – XII were intact bilaterally. Sensory, motor, and coordination were unremarkable.
Laboratory, Imaging, & Procedures: Laboratory findings included leukocytosis, microscopic hematuria, decreased C3 and C4 levels, and positive titers of anti-streptolysin O antibody. Lumbar puncture was conducted with unremarkable CSF findings. Imaging revealed hypoattenuation in the occipital lobes on CT venogram and hyperintensities in bilateral occipital lobes on MRI T2-FLAIR sequences, consistent with PRES.
Final Diagnosis: PRES secondary to post-infectious glomerulonephritis
Discussion: PRES in pediatric patients has been associated with a variety of conditions including hypertension (idiopathic or secondary), renal disorders, autoimmune disorders, and hematologic or oncologic conditions. Based on our literature review, reports of PIGN-induced PRES are limited. Consideration of the abnormal UA led to obtaining complement levels, and further history elucidated helped to narrow the differential to post-infectious glomerulonephritis due to streptococcal infection with confirmation of positive ASO antibody titer.
C12. New-onset Jaundice in 13-day Old Baby with Trisomy 21
Shane Clark1, Annette Roberts2, Paul Suhocki3, Samrat Das1
1. Department of Pediatrics, Duke University School of Medicine, Durham, NC, United States.
2. Department of Pediatrics, Division of Pediatric Gastroenterology, Hepatology, and Nutrition, Duke University School of Medicine, Durham, NC, United States.
3. Department of Interventional Radiology, Duke University School of Medicine, Durham, NC, United States.
Case Presentation: A 13-day old term female infant with trisomy 21 who previously had normal transcutaneous bilirubin screenings in the first few days of life develops jaundice overnight. She has been hospitalized since birth due requirement of low flow nasal cannula support (0.1 to 0.3 L/hr) for suspected pulmonary edema secondary to a moderately sized atrial septal defect and a large patent ductus arteriosus. For the last 3 days, the patient has had poor feeding intake.
Physical Examination: She is 5% below birth weight. Other than her O2 requirement, her vital signs are stable. Her physical exam this morning shows an active infant with conjunctival icterus and jaundice of the face and body. The lungs are clear to auscultation with no audible murmurs. A soft liver tip is palpated at the right costal margin.
Labs/Imaging/Procedures: Total serum bilirubin level is 15.6 mg/dL (conjugated bilirubin 8.5 mg/dL and unconjugated bilirubin 7.1 mg/dL). Additional labs show an elevated AST of 446 U/L, ALT of 436 U/L, and alkaline phosphatase of 607 U/L. Liver doppler ultrasound showed a dilated left portal vein with increased velocity involving its connection with the hepatic vein. Follow up, Computed Tomography (CT) confirms diagnosis. Transhepatic portal venography, obtained prior to IR procedure, demonstrated two small portosystemic shunts and a dominant shunt between the left portal vein and the hepatic vein (Figure 1). The dominant shunt was occluded with a 7 mm diameter Amplatzer Plug (Abbott, Chicago, Illinois) on day of life (DOL) 24 (Figure 2). The two smaller shunts were left untreated. Our patient was discharged home on DOL 33 and was doing well on follow up.
Final Diagnosis: The patient was diagnosed with a rare condition called a congenital portosystemic shunt (CPSS). CPSS is thought to occur in 1 out of 50,000 births and can be associated with genetic syndromes, most commonly trisomy 21. CPSS is caused by an abnormal connection between portal and systemic veins that forms due to a failure of involution of specific primordial vessels. This results in complete or partial diversion of portal blood flow away from the liver to the systemic venous system. CPSS can lead to cholestasis and complications such as end stage liver disease, portopulmonary hypertension, and pulmonary arteriovenous shunts.
Discussion: This case highlights the extremely rare diagnosis of CPSS. Imaging, particularly liver ultrasound with doppler, is crucial for diagnosis due to nonspecific clinical findings. Follow up CT or MRI are used to confirm the diagnosis. Intrahepatic shunts often close spontaneously within the first year of life, so interventions are typically reserved for patients over one year old or those with complications such as poor fetal hemodynamics, growth restriction, respiratory distress, and hepatic inflammation. Most patients show improvement post-shunt closure, with heart and liver complications usually resolving within months afterward.
Portal venography with iodinated contrast demonstrates tip of transhepatic catheter (open arrows) in an enlarged left portal vein. A large branch of the left portal vein (arrowheads) communicates directly with the left hepatic vein (curved arrow) via a large congenital portal-systemic shunt (bracket). Two smaller portal-systemic shunts (arrows) are also present.
Post embolization portal venography demonstrates the tip of a vascular sheath (arrowheads) in the left portal vein branch that previously communicated with the left hepatic vein. The portal vein branch is now occluded by an Amplatzer Plug (open arrowheads) and the hepatic vein no longer fills with contrast. Two smaller portal-systemic shunts (arrows) remain patent.
C13. Bowel Perforation: A Rare Complication of Trichobezoar
Clara El Nakib1, Lauren Thomas1, Rheu Cristine Candava2
1. Pediatrics, SUNY Upstate Medical University, Syracuse, NY, United States.
2. Pediatric Gastroenterology, SUNY Upstate Medical University, Syracuse, NY, United States.
Background: Trichobezoars are the most common type of bezoars, encompassing mostly human hair, most commonly seen in females with trichotillomania or trichophagia. Rapunzel syndrome is a rare complication of trichobezoars in which the hair extends to the small intestine. One of the very uncommon complications of Trichobezoars is bowel perforation which we describe in two patients below.
Cases: An 11-year-old girl with anxiety, trichotillomania and constipation presented to the emergency department (ED) with epigastric pain, vomiting, weight loss and a palpable right upper quadrant mass. CT abdomen (CTA) showed hair casts in the gastric body extending to the duodenum. Endoscopic removal was unsuccessful; so she underwent laparotomy with successful removal and no immediate complications, and was started on proton pump inhibitor for ulcers in the stomach and duodenum. She was discharged home in stable condition after upper GI series confirmed the absence of gastric leak. A week later, she had worsening abdominal pain and suffered cardiac arrest at home. She was resuscitated and abdominal Xray (AXR) showed free intraperitoneal air necessitating urgent surgical exploration during which a perforation in the distal ileum was noted with marked purulent fluid through her abdomen. Her small bowel was partially resected, but she continued to be hemodynamically unstable and ultimately passed away.
A 10-year-old girl with autism, chronic constipation and trichotillomania presented to the ED with abdominal pain and vomiting. AXR revealed dilated loops of bowel with significant stool burden. Nasogastric cleanout failed to improve symptoms and upper endoscopy revealed a trichobezoar in the gastric body and prepyloric portions of the stomach. Endoscopic removal was unsuccessful (Image 1), and she was started on TPN awaiting surgery. Within a week, she began passing balls of hair per rectum and CTA revealed trichobezoar extending towards the distal ileum and rectum. Exploratory laparotomy showed full thickness necrosis along the mesenteric border of the small bowel and perforation necessitating resection of 80 cm of small bowel (Image 2). She had a stable post-operative course necessitating nutritional optimization and she was discharged home in stable condition.
Discussion: The mechanism of bowel perforation in Trichobezoars is unclear but is likely multifactorial including bowel injury, ischemia, and delayed healing process possibly due to decreased blood flow, protein-losing enteropathy, and loss of elasticity. The bezoar hair body has potential to break down, with satellite hairs lodging within the gastrointestinal tract after bezoar removal and potentially damaging the intestines further. Given the increased morbidity and mortality in such cases, further studies are needed to evaluate the need for post-operative follow up imaging, and whether it should be conducted in all patients or on a case-by-case basis
Visualized trichobezoars from the gastric body to the small bowel via endoscopy.
Resected small intestine segment, 40 cm long, found to have serosal tears with full-thickness perforations within close proximity to one another.
POSTERS
P1. Diagnostic Challenge: Drug Reaction with Eosinophilia and Systemic Symptoms Presenting as Acute Encephalopathy
Sunpil Hwang1
1. North Alabama Medical Center, Florence, AL, United States.
History: A septuagenarian male presented to the emergency department after an episode of a seizure-like movement followed by a loss of consciousness. He had been receiving ceftazidime for osteomyelitis of the left third toe, which was switched one week before from vancomycin due to the development of skin rashes.
Physical Examination Findings: Physical examination revealed generalized maculopapular erythematous rashes, including on the palms and soles. The site of osteomyelitis was well-dressed and showed no signs of inflammation or infection. The patient was intubated to maintain the airway.
Laboratory or Diagnostic Imaging Findings: Routine labs showed leukocytosis with eosinophilia counts of 1,600/µL. Brain CT and MRI were unremarkable. EEG showed no evidence of epileptic activity. A lumbar puncture was only noted for elevated total CSF protein of 77. Broad-spectrum antibiotics were initiated to cover undiagnosed infections. IV methylprednisolone was also added for suspected drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome. An extensive work-up for infectious diseases, including tick-borne disease, fungal disease, hepatitis, and HIV, yielded negative results. Viral meningitis and encephalitis PCR panel were negative. ANA and rheumatoid factor were unremarkable. Subsequently, antibiotics were discontinued as there was no evidence of infection.
Final diagnosis: After ruling out other potential causes, the Registry of Severe Cutaneous Adverse Reaction (RegiSCAR) score was utilized and indicated probable DRESS syndrome with a score of 5. Treatment with IV prednisolone resolved the patient’s encephalopathy. The patient was subsequently extubated, and his skin lesions showed gradual improvements. Given the treatment response, RegiSCAR score, and exclusion of alternative causes, the patient was diagnosed with DRESS syndrome.
Discussion: DRESS syndrome is a severe drug reaction characterized by extensive skin rashes and involvement of internal organs. The presentation of the disease can vary, and symptoms may arise two to eight weeks after the exposure, making the diagnosis of DRESS syndrome very challenging for medical providers.
In this case, the patient developed skin rashes and encephalopathy following treatment with vancomycin, the well-known causative medication for DRESS syndrome. The diagnosis was challenging due to unusual neurologic manifestations and the absence of classical features, such as lymphadenopathy or hepatic involvement. Therefore, diagnosing DRESS syndrome necessitates a high level of suspicion, particularly in patients with recent medication exposure, skin lesions, and eosinophilia, given its potential for varied symptom presentations. The RegiSCAR score can serve as a valuable tool for the diagnosis. However, it is crucial to rule out other potential causes, such as autoimmune diseases or infections, which can mimic DRESS syndrome, as described in this case.
P2. An Case of Overlap Syndrome presenting with life-threatening Multiple Organ Dysfunction Syndrome
Ryan T. Brummond1, 2, Ankita Vayalapalli3, Michelle Patel3, Renuka Mehta4
1. Pediatrics, Medical College of Georgia, Augusta, GA, United States.
2. Medical Detachment, Rhode Island Army National Guard, Providence, RI, United States.
3. Medical College of Georgia, Augusta, GA, United States.
4. Pediatric Critical Care, Medical College of Georgia, Augusta, GA, United States.
Case Report: Overlap Syndrome (OS) is a rare rheumatologic disease in which patients present with multiple immune diseases or aspects of immune diseases evidenced through serologic workup. The most common diseases involved in OS are Rheumatoid Arthritis, Scleroderma, Lupus, and Myositis. OS commonly presents as progressive and chronic illness and is not easily diagnosed as its presentation overlaps several of Immune mediated illnesses.
We report an atypical presentation of OS in a 15-year-old female admitted to the Pediatric ICU with Multiple Organ Dysfunction Syndrome (MODS). The objective is to highlight a possibility of life-threatening presentation of this case report due to complex presentation and delay in diagnosis.
The patient is a 15-year-old Caucasian female with a 3-month history of Immune Thrombocytopenic Purpura (ITP) (treated with apixaban) and Iron Deficiency Anemia who presented with a 1-week history of nausea and vomiting. She initially responded to fluid resuscitation but subsequently progressed to acute respiratory distress and chest pain requiring sepsis workup, multiple fluid resuscitations, ionotropic support, intubation, and mechanical ventilation (MV). She was then started on high-dose steroids for possible autoimmune disease. The patient continues to have worsening hypoxemia requiring increase in MV support and initiation of inhaled nitric oxide. Chest x-ray showed interstitial lung disease consistent with OS. She was started on methotrexate and azithromycin, but subsequently developed MODS requiring Venovenous Extracorporeal Membrane Oxygenation (VV-ECMO). She remained on VV-ECMO for 4 days and MV support for 2 weeks. Based on her characteristic appearance of petechiae on the lower extremities and positive rheumatologic workup for +ANA, +anticentromere Ab and +anticardiolipin Ab, a diagnosis of OS was made.
High-dose steroids and methotrexate were successful in treating this acute exacerbation of OS. The patient was discharged home after two weeks on apixaban, trimethoprim/sulfamethoxazole, enoxaparin, hydroxychloroquine, leuprolide, and lisinopril. This clinical case highlights the importance of awareness of atypical presentations of OS and early interventions to mitigate more serious sequelae that occur secondary to disease progression. In this case, early diagnosis and intervention with steroids could have avoided the development of MODS and subsequent need for ECMO.
P3. Severe Hyperphosphatemia Following Sodium Phosphate Enema in a Medically Complex Pediatric Patient
Clara El Nakib1, Mohammed Doklaijah1, Rachel Clarke2, Kimberly Rush2
1. Pediatrics, SUNY Upstate Medical University, Syracuse, NY, United States.
2. Pediatric Intensive Care, SUNY Upstate Medical University, Syracuse, NY, United States.
Introduction: Hyperphosphatemia can lead to serious complications including hypocalcemia, seizures, coma, renal failure and cardiac arrest. Critical hyperphosphatemia due to exogenous sources is relatively rare. Sodium phosphate enemas are commonly used preparations for constipation and well tolerated with a low side effect profile, however, the main ingredient, sodium phosphate, can lead to phosphorous toxicity in complex patients with inappropriate administration.
Case: A 3-year-old female with a history of prematurity, caudal regression syndrome, neurogenic bladder, renal dysplasia, and chronic constipation was admitted to the pediatric intensive care unit in hypovolemic shock after receiving 240 ml of sodium phosphate enema at home via appendicostomy. Within 1 hour of administration, she developed stiffness, listlessness, and emesis prompting presentation to the Emergency Department. Laboratory evaluation was significant for hyperphosphatemia >26mg/dL, metabolic acidosis with anion gap >62mmol/L, bicarbonate < 6mmol/L and ionized calcium 0.67 mmol/L. Due to tetany, she was treated with calcium carbonate, calcium gluconate, lactated ringers, and bicarbonate with improvement. Abdominal computed tomography showed severe stool burden and she was manually disimpacted and started on a Golightly bowel cleanout which she completed successfully. She received hemodialysis for persistent hyperphosphatemia and her electrolytes improved markedly. She subsequently made a full recovery and was discharged home in a stable condition.
Discussion: In patients with obstipation and slow colonic transit, solution retention of sodium phosphate enemas may lead to electrolyte derangement and intravascular hypovolemia through osmotic effects. Attention to dosing is vital, as the recommended dose in pediatrics varies by age despite standard over-the-counter preparations. Hypocalcemia and hypomagnesemia can result from a rapid increase in serum phosphate and excessive fluid movement into the bowel lumen. Sodium phosphate enema induced hyperphosphatemia in children is a rare but serious complication that can occur with inappropriate use. Healthcare providers should be aware of this risk and educate patients and caregivers on proper use of sodium phosphate enemas. Prompt recognition and treatment of hyperphosphatemia is critical to prevent serious complications and ensure a favorable outcome for affected children.
P4. Fixed Drug Eruption, Raynaud’s, Lupus, or None of the Above? A Puzzling Dermatological Case in a Resource-Limited Rural Pakistani Village
Azeem Rathore1, Hamza Ajmal2, Jahanzaib Ekram3, Sharif Hussein1, Rafik Jacob1
1. Internal Medicine, University of Florida Health Science Center, Jacksonville, FL, United States.
2. Rocky Vista University College of Osteopathic Medicine, Greenwood Village, CO, United States.
3. H. Lee Moffitt Cancer Center and Research Institute, University of South Florida, Tampa, FL, United States.
Background: Diagnosing dermatological conditions in resource-poor settings presents complex and difficult challenges. We present an unusual case of a self-limiting and spontaneously painful unilateral cutaneous wrist discoloration in an otherwise healthy individual.
History: A 30-year-old male with a medical history of nephrolithiasis residing in rural Pakistan presents to a PCP with recurrent left wrist pain. He states his left wrist first developed discoloration one year prior during the winter. His occupation involves computer-related tasks, but denies that keyboard typing is a trigger. He tried both acetaminophen and NSAIDs with minimal relief of his symptoms. Last year he was able to purchase topical corticosteroids but they also proved ineffective. There is no significant family medical history, and he denies allergies to medications. He further states his symptoms typically self-resolve over several days to weeks. On physical examination, a pruritic, violaceous lesion at the base of the 1st digit on the left hand was present (see Image 1). The lesion is tender to touch with restriction to the range of motion in the first digit of the left hand. Laboratory data was overall unremarkable, including autoimmune tests which included a negative ANA. The patient was lost to follow-up.
Discussion: In rural and third-world country settings, diagnosing dermatological conditions presents unique challenges, particularly when performing invasive procedures like biopsies may not be practical or accessible. In these resource-limited environments, clinicians must rely heavily on clinical judgment, history-taking, and physical examination skills to formulate diagnoses. In the given case, the patient’s presentation of a self-limiting and spontaneously painful unilateral cutaneous wrist discoloration, recurrence occurring during the winter months, and lack of response to topical corticosteroids, help formulate a few differential diagnoses to consider. We believe the patient suffered from perniosis, or chilblains which is a seasonal inflammatory disorder that is triggered by prolonged exposure to cold. It is a form of inflammation of the small blood vessels (vasculitis) that is characterized by painful, itchy, and tender skin lesions. Other differentials we considered included an atypical presentation of Achenbach’s syndrome, characterized by painful, violaceous lesions, may be considered, although it almost always affects fingers not wrists. Cutaneous lupus erythematosus cannot be ruled out entirely, especially considering the discoloration’s tender nature and the absence of a positive ANA test should not exclude diagnosis given its low specificity. Follow-up with a detailed physical examination, emphasizing skin lesion characteristics and systemic signs and Labwork, including CBC, ESR, CRP, and additional autoimmune markers, as well as skin biopsy would help further definitively arrive at a diagnosis.
The patient’s left wrist with a violaceous lesion at the base of the 1st digit on the left hand was present.
P5. Two Cases of Melanoma In Situ Presenting with Two Distinct Growth Patterns and “Figure of 8” Shape Configurations
Mathew Trandafirescu1, Shane Meehan3, Elizabeth Bentsianov2, Chapman Wei4, Stefan Bradu5
1. Vanderbilt University, Nashville, TN, United States.
2. Union College, Schenectady, NY, United States.
3. Dermatopathology, New York University Langone Health, New York, NY, United States.
4. Internal Medicine, Staten Island University Hospitals- Northwell Health, New York, NY, United States.
5. Internal Medicine- Division of Dermatology, Staten Island University Hospitals- Northwell Health, New York, NY, United States.
Case Report: The recognition and diagnosis of early melanoma are essential tactics in decreasing the mortality of this aggressive form of skin cancer. Specific geometric patterns of growth and pigmentation can supplement the traditional ABCDE criteria used to detect skin lesions with an increased risk of melanoma. We report two cases of melanoma in situ presenting with two distinct growth patterns and pigment configurations resembling the “figure of 8”.
The first case is a 55-year-old Caucasian female with a history of treated basal cell carcinoma who presented to the Dermatology clinic complaining of a skin lesion on the left flank that she noticed for one year. The patient denied lesion changes and symptoms. Visual examination of the lesion revealed a hyperpigmented 8 x 3 mm flat papule showing a “figure of 8” shape configuration with the anterior oval half darker than the posterior oval hyperpigmented half (Figure 1). Histopathologic examination of the shave skin biopsy showed findings consistent with a melanoma in situ evolving in an atypical junctional melanocytic nevus.
The second case is a 59-year-old Caucasian male with a noncontributory medical history presenting to the Dermatology clinic with a dark skin lesion on the right posterior shoulder. The patient was only aware that he had multiple asymptomatic dark lesions on the back for years. A hyperpigmented flat lesion 12 x 5 mm with “figure of 8” shape configuration was noted during visual examination on the right posterior shoulder (Figure 2). The lesion did not appear to be darker compared to the surrounding lesions, but dermoscopy showed pigmentary unevenness throughout the lesion and border irregularity in the inferior part of the lesion. Histopathologic examination of the shave skin biopsy showed findings consistent with a melanoma in situ arising in association with a compound melanocytic nevus.
We report that melanoma in situ can present clinically with two distinct “figure of 8” pigmentation patterns which can be easily recognized visually by both clinicians and non-clinicians. Depending on the expertise of the examiner and understanding of the ABCDE criteria used during melanoma detection, certain types of geometric growth patterns of melanoma in situ including “figure of 8” configurations can introduce difficulties in evaluating the asymmetry, border, and color variegation features of pigmented lesions. Certain “figure of 8” pigmentation patterns of melanoma might not always be easy to differentiate clinically from collisions of other pigmented skin lesions. Specific geometric patterns of pigmentation are most useful for the early recognition of melanoma before other disorganized growth patterns of advanced melanoma cells occur and may be important components of melanoma detection education which are currently overlooked. Further studies are needed to determine the incidence and etiology of the specific pigmentation patterns observed in early melanomas.
P6. Peripheral Pigmentation as a Macroscopic Visual Sign of Amelanotic/Hypomelanotic Melanoma In Situ
Mathew Trandafirescu1, Elizabeth Bentsianov2, Michael Miller3, Chapman Wei4, Stefan Bradu5
1. Vanderbilt University, Nashville, TN, United States.
2. Union College, Schenectady, NY, United States.
3. Dermpath Diagnostics, White Plains, NY, United States.
4. Internal Medicine, Staten Island University Hospitals- Northwell Health, New York, NY, United States.
5. Internal Medicine- Division of Dermatology, Staten Island University Hospitals- Northwell Health, New York, NY, United States.
Case Report: Amelanotic/hypomelanotic melanoma (AHM) is defined as a subtype of cutaneous melanoma which presents clinically with little or no pigment. Approximately 2-8% of all melanomas were reported to be AHMs. AHMs often lack obvious features of pigmented melanomas such as the ABCD criteria, likely contributing to their higher risk of delayed diagnosis and significantly lower 5-year melanoma-specific survival compared to pigmented melanomas. The scarcity of publications about in situ AHMs limits our knowledge regarding the macroscopic visual features of in situ AHMs. We present the case of a patient with peripheral brown-gray pigmentation in a pink-red macule whose pathology was consistent with an in situ AHM with regression.
A 63-year-old female with noncontributory medical history came to the dermatologist complaining of an itchy skin lesion, enlarging for a year on the left dorsal forearm. Physical examination showed an oval, scaly, pink-red macule with a faint brown- gray peripheral pigmented area, on a background of chronic actinic damage. The lesion was frozen with liquid nitrogen as treatment for a possible actinic keratosis. After 5 weeks, the lesion persisted as a 1.1 cm oval pink- red macule with a 4 mm brown-gray area of peripheral pigmentation (Figure 1). Dermoscopic examination showed mild vascular polymorphism, subtle shades of milky pink-red, and a brown-gray structureless peripheral area.
Due to the atypical features, a shave biopsy was done. The possible differential diagnosis included pigmented actinic keratosis, pigmented squamous cell carcinoma, lichen planus like- keratosis, pigmented basal cell carcinoma, and AHM. Microscopic examination after H&E staining showed a proliferation of atypical melanocytes present as nests and solitary units at all levels of the epidermis in a haphazard manner. The underlying dermis was fibrotic with foci of dense mononuclear inflammatory cell infiltrate. The atypical melanocytes were highlighted with Melan-A and SOX-10 stains (Figure 2). These findings were consistent with a melanoma which was at least in situ, inflamed, with regression, extending to the margins. A month later, pathologic examination of the subsequent excision revealed no residual atypical melanocytic lesion.
The paucity of published in situ AHM images can limit the ability of clinicians and non-clinicians to recognize early AHMs. A few studies have reported that subtle peripheral light brown or gray areas are not uncommon in macular and thin nodular AHMs. Our patient presented with an AHM in situ showing peripheral light brown-gray pigmentation, further emphasizing the potential role of this subtle macroscopic feature of melanomas to aid in the naked eye visual detection of early AHMs by both clinicians and non-clinicians. The presence of color unevenness in a pink-red skin lesion with peripheral brown-grey pigmentation should prompt immediate referral for further evaluation with dermoscopy and possible biopsy.
P7. Cocaine-induced Leukocytoclastic Vasculitis
Michael C. Swindell1, Pamela Obi1
1. Floyd Family Medicine Residency, Rome, GA, United States.
Presenting Symptoms: 27-year-old male with past medical history of polysubstance abuse presented with painful cellulitic changes to his bilateral lower extremities. These had started 3 months prior to his presentation and began his only pain and swelling to his lower extremities. It then progressed to bruising, and then to bleeding and open wounds. He had initially been treated at 2 other outside hospitals for this and had been through multiple courses of antibiotics without any improvement. Blood cultures from both of those admissions were all negative. Of note, he had an extensive history of drug abuse, most notably cocaine; to which he admitted to using 2 g/day last 6 months. He also endorsed use of in the past peds, marijuana, ketamine, and alcohol. 2 days prior to his presentation he quit all of these "cold turkey" and was already showing signs and symptoms of withdrawal at the time of presentation. Most notably increased upper respiratory secretions.
Labs
AlkPhos 179
ALT 84
AST 144
GGT 104
Iron 16
TIBC 178
Transferrin 9
Ferritin 694
Lactic acid 2.0
CRP 25.3
ESR 81
WBC 21.55
Hgb 9.5
Hct 31
Plt 990
UDS positive for Benzos, cocaine, THC
C-ANCA titer 1:80
p-ANCA titer <1:20
Complement >60
Anti-MPO Ab <0.2
Anti-PR-3 Ab > 8.0
ANA neg
Skin Biopsy of Right Lower Extremity lesion: Several vessels with luminal thrombi. Neutrophils around and infiltrating the vessel wall. Extravasated RBCs in the dermis and superficial necrosis.
Clinical Course: Bilateral leg swelling and ulceration 2/2 c-ANCA leukocytoclastic vasculitis
On admission he was treated with wound care and autoimmune labs were obtained. Venous ultrasound bilaterally was obtained to rule out DVT and an ABI was obtained to rule out arterial insufficiency. He was found to be positive for C ANCA, and a high-resolution CT chest was obtained which was consistent with vasculitic disease. A punch biopsy was performed of a purpura like lesion of the right lower leg. This was read as consistent with leukocytoclastic vasculitis. He was also found to be positive for antiproteinase 3 antibody. He was given a one-time dose of Solu-Medrol 125 on 4/5. On 4/6 he was discharged home with a presumptive diagnosis of drug-induced c-ANCA leukocytoclastic vasculitis. On discharge he was given a 6-week steroid taper and advised to establish care with a primary care doctor for further evaluation.
History of polysubstance abuse: He endorsed a history of benzodiazepine, cocaine, ketamine, THC abuse. He began doing drugs at age 19 and endorsed increased use in the past 6 months. 2 days prior to admission his friends had an intervention with him, and he decided to quit all drugs cold turkey. He was monitored with withdrawal precautions. He had heavy nasopharyngeal secretions. On 4/5 the secretions resolved. He endorsed a strong motivation to quit all drugs and said that on discharge he would find a Narcotics Anonymous group to become involved with.
P8. Pseudo-Thrombotic Microangiopathy (TMA) in Vitamin B12 Deficiency: Navigating the Diagnostic Challenges
Benjamin M Easow1, Tijin Mathew1, Lydia George1, Greeshma Thomas1, Sri Laxmi Valasareddi2
1. Internal Medicine, Southeast Health, Dothan, AL, United States.
2. Hematology and Oncology, Southeast Health, Dothan, AL, United States.
History: A 52-year-old African American male with a past medical history of hypertension and coronary artery disease presented to the emergency department for complaints of dizziness and fatigue for over one month. He had been experiencing dizziness, resulting in multiple falls in the past few days. The patient denied any history of head trauma or loss of consciousness. He acknowledged poor appetite for several months, leading to an 18-pound weight loss in the last 6 months. The patient denied any family history of malignancy or bleeding disorders and reported a smoking history of half a pack of cigarettes daily for the last 18 years. There was no history of alcohol consumption.
Physical Exam: Upon examination, vital signs were normal except for tachycardia with a heart rate of 108. Physical examination was unremarkable.
Labs: Complete blood count (CBC) revealed hemoglobin 6.4 g/dL, hematocrit 18.8%, mean corpuscular volume (MCV) 111.2 fL, and platelet count 75 x 10-3/uL. Hepatic panel showed unconjugated hyperbilirubinemia of 1.4 mg/dL (total bilirubin 1.6 mg/dL). Further laboratory workup was remarkable for Vitamin B12 107, elevated LDH of 3,895 U/L, haptoglobin less than 30 mg/dL, and a negative direct antiglobulin test. Iron studies and folate levels were within normal limits. Furthermore, the Reticulocyte Production Index (RPI) was observed to be low at 0.66, indicating a hypoproliferative bone marrow. Peripheral smear showed rare schistocytes and hypersegmented neutrophils.
Diagnosis and management: On admission, he received two units of packed red blood cell transfusion. Hematologist suspected pseudo TMA due to B12 deficiency and recommended B12 replacement parenterally, 1000 mcg IM daily for 7 days, weekly for 4 weeks, then monthly. After a 2-day hospital course, as the patient showed symptomatic improvement with stable hemoglobin and hematocrit, with no further drop in values post-transfusion, he was discharged with recommendations to continue IM Vitamin B12 daily. At four week follow-up, his laboratory workup showed complete resolution of pseudo-TMA with hemoglobin of 11.5 g/dL, hematocrit of 37.1%, MCV of 87.6 fL, platelet count of 263 x 10-3/uL, total bilirubin 0.8 mg/dL and LDH of 149.
Discussion: Given the remarkably similar presentations of pseudo-thrombotic microangiopathy (TMA) and TMA, each requiring distinct treatments, we highlight three subtle yet pivotal differences in laboratory findings between the two. (See Figure 1)
References: 1. Hassouneh, R., Shen, S., Lee, O., Hart, R., Rhea, L., & Fadden, P. (2021). Severe Vitamin B12 Deficiency Mimicking Microangiopathic Hemolytic Anemia. Journal Of Hematology, 10(4), 202-205.
2. Walter K, Vaughn J, Martin D. Therapeutic dilemma in the management of a patient with the clinical picture of TTP and severe B12 deficiency. BMC Hematol. 2015 Dec 1;15:16. doi: 10.1186/s12878-015-0036-2. PMID: 26634125; PMCID: PMC4667528.
The three subtle yet pivotal differences in laboratory findings between Pseudo-TMA and TMA.
P9. The Numbers CAN Lie: Highlighting the Phenomena of Spurious Hyperphosphatemia and Pseudohyponatremia in Multiple Myeloma
1. University of Florida College of Medicine Jacksonville, JACKSONVILLE, FL, United States.
Introduction: Clinicians, especially ones early in their training, may be eager to correct a patient’s electrolyte abnormalities without considering the bigger clinical context. Not all electrolyte abnormalities should be taken at face value. In this case, a patient with newly diagnosed multiple myeloma had laboratory work that showed hyperphosphatemia and hyponatremia when, in reality, was hypernatremic and hypophosphatemic.
Case Presentation: A 70-year-old male from a skilled nursing facility presented to evaluate coffee-ground emesis that began a few days before the presentation. He had a pertinent history of substance use disorder and a recent ischemic stroke. Incidentally, his initial labs revealed a significant gamma gap of 9 g/dl. Further investigation revealed an M spike of 5.66 on serum protein electrophoresis. Immunofixation studies showed IgG monoclonal paraprotein gammopathy. A bone marrow biopsy showed a plasma cell neoplasm involving 75% of marrow cellular elements, and flow cytometry showed monoclonal plasma cells. His beta-2 microglobulin was elevated to 5.8mg/L. Throughout his hospitalization, his lab work was significant for several electrolyte derangements, namely hyponatremia as low as 129 mmol/L and hyperphosphatemia as high as 6.3 mg/dL. The profound paraproteinemia from myeloma meant he was, in reality, hypernatremic and hypophosphatemic. With hypophosphatemia, an increased risk of hemolysis and respiratory depression exists. Fortunately, his lactate dehydrogenase and haptoglobin were within normal limits, which suggested no active hemolysis. Medications that promoted respiratory depression, such as opioids, were avoided. With this knowledge, no individual efforts were made to correct these laboratory abnormalities. The decision was made to start the patient on chemotherapy with bortezomib and dexamethasone. He tolerated this chemotherapy well, and eventually, his pseudohyponatremia and spurious hyperphosphatemia resolved. He was discharged back to a skilled nursing facility with plans to continue chemotherapy as an outpatient.
Discussion: With multiple myeloma, a large amount of paraproteins are present in the serum. These paraproteins can cause false elevations in serum phosphate because the ultraviolet light absorbance commonly used detects proteins as phosphate. Due to multiple myeloma’s effect on bone, patients are actually commonly hypophosphatemic. In the case of sodium, the paraproteins displace water molecules, leading to falsely low concentrations of sodium and other electrolytes in indirect electrode measurements. Recognizing these laboratory phenomena and obtaining appropriate confirmatory testing is critical to prevent unnecessary therapeutic interventions with detrimental outcomes.
P10. Extensive Stage Small Cell Lung Cancer with Cerebellar Metastasis: 5 Years Survival
1. Appalachian Regional Healthcare, Whitesburg, KY, United States.
Case Report: Small cell lung cancer (SCLC) or oat cell cancer is the second most common cancer in the world and it constitutes of about 20% of all lung cancers. SCLC is highly aggressive disease and is strongly associated with smoking. SCLC with brain metastasis is stage 4 carcinoma and it confers poor prognosis with median survival of three to four months. Brain metastasis is usually treated with whole brain radiation vs surgical resection. Here we present a very rare case of long-term survivor with cerebellar metastasis in a SCLC patient.
A 63-year-old male with history of forty-pack year smoking, COPD, small cell lung cancer, hypertension presented with headache, weight loss. He was on carboplatin+etoposide and atezolizumab for SCLC. On physical examination, he appeared visibly fatigue. A magnetic resonance imaging (MRI) brain demonstrated a cerebellar mass without vasogenic edema obstructing the fourth ventricle and causing non-communicating hydrocephalus. Metastatic SCLC diagnosis made. A ventriculoperitoneal shunt placed to relieve the obstruction. Pre-treatment MRI brain (Fig 1). Then patient had whole brain radiation for metastasis. Atezolizumab withheld for extreme fatigue and poor appetite. He received dronabinol and appetite, fatigue improved. Then restarted on atezolizumab after four months. Later patient admitted for neutropenia, mastoiditis and treated with in-patient antibiotics. Patient received three cycles of carboplatin+etoposide, atezolizumab and two cycles of maintenance atezolizumab. Repeat MRI brain after three years of metastatic SCLC did not demonstrate any cerebellar mass (Fig 2).
SCLC is a disease known for its aggressive nature. It confers very poor prognosis with brain metastasis. Our case is rare because the patient is metastasis free and been doing well for past three years since diagnosis of cerebellar metastasis.
Pretreatment magnetic resonance imaging demonstrating left cerebellar mass.
Post treatment magnetic resonance imaging at 60 months with no evidence of recurrence.
P11. Epidural Hematoma with Cord Compression in a Pediatric Patient with Immune Thrombocytopenia and Concurrent Histoplasmosis
Mohammed Doklaijah1, Clara El Nakib1, Jody Sima1
1. Pediatrics, Suny Upstate, Syracuse, NY, United States.
Case Report: Introduction: The incidence of pediatric epidural hematomas is 0.02 per 100000 children per year, with the majority attributed to traumatic causes. The incidence of immune thrombocytopenic purpura (ITP) varies, with a reported prevalence of 4.6 to 5.3 cases per 100000 children per year, mostly aged 2 to 5 years. ITP is characterized by decreased platelet counts and altered platelet function, which could contribute to bleeding complications, especially in the presence of trauma or minor injuries.
Case: The patient is a 9-year-old girl with no medical history and pertinent family history of ITP who presented after a fall with acute onset neck pain that progressed to quadriparesis. She had a low platelet count of 2 platelets per unit. A CT spine showed no evidence of fracture but raised concern for a compressive lesion from C3-C6. MRI of the spine showed an extensive dorsal epidural collection from C2-3 through L1-2, resulting in severe narrowing at the C4-5 and C5-C6 levels, along with T2 signal change in the cervical spine extending rostrally to the brainstem; consistent with an epidural hematoma with significant cord compression. She received steroids, IVIG and emergent splenectomy, with spleen biopsy suggesting histoplasmosis infection and histoplasma antibodies positive. She then underwent laminoplasties at C3-6 and T4-6 with evacuation of the cervicothoracic epidural hematoma with benign post-op course. Platelet counts increased gradually. Post op MRI spine showed interval improvement. She regained her strength and reflexes and was discharged in a stable condition.
Discussion: The relationship between ITP and the development of epidural hematomas, especially in the presence of histoplasmosis, remains an area of ongoing investigation. The association of histoplasmosis with immune thrombocytopenia adds a layer of diagnostic challenge, as thrombocytopenia can be multifactorial in such cases. This underscores the need for a multidisciplinary approach, involving hematology, neurosurgery, infectious diseases, and other relevant experts, to ensure optimal patient care and outcomes.
P12. Step-wise Treatment of Portal Vein Thrombosis in a Healthy, 27-Year-Old Professional Athlete
Nicole Mamprejew1, Zackary Anderson1, Anna Juncadella2, Alimer Gonzalez1
1. Graduate Medical Education, NCH Healthcare System, Naples, FL, United States.
2. Gastroenterology, NCH Healthcare System, Naples, FL, United States.
Introduction: Portal vein thrombosis (PVT) is rare with unclear incidence in those without cirrhosis (1-2). A lack of research has resulted in limited treatment guidelines, which include anticoagulation (AC), thrombolysis, thrombectomy, and transjugular intrahepatic portosystemic shunt system procedure (1-4). This case details the step-wise treatment of a young, healthy patient with recent PVT.
Case Presentation: A 27-year-old professional male athlete with no medical history presented with 12-hours of intractable epigastric pain. He was diagnosed with PVT on contrasted computed tomography of the abdomen and pelvis. Labs revealed normal hepatic function. Initial work-up of etiology evidenced no malignancy or inflammatory disease. Preliminary work-up of thrombophilia was negative for antithrombin deficiency, anticardiolipin antibody, beta-2 glycoprotein antibodies, lupus anticoagulant antibodies, and JAK2 tyrosine kinase mutation. Paroxysmal nocturnal hematuria was also ruled out. The patient had full resolution of epigastric pain after heparinization. He was transitioned to rivaroxaban on discharge. At one-week follow-up in an outpatient resident clinic, he was found to have recurrence of intractable abdominal pain. Through interdisciplinary discussions with interventional radiology and gastroenterology, it was determined the patient was appropriate for readmission to undergo in-situ thrombolysis. Intraprocedural venogram revealed filling defects in the mesenteric vein and portal vein with involvement of its branches. With a transhepatic puncture approach into the portal vein, alteplase was delivered into the thrombosed vessels, and a catheter was maintained at the portal vein through which alteplase was administered for 24 hours. Post-intervention venogram revealed decreased clot burden with some persistent filling defects, indicating chronic thrombus. Immediately post-procedure, the patient had full remission of pain and prior to discharge was reinitiated on rivaroxaban. The patient awaits genetic counseling to pursue Factor V Leiden work-up. He has returned to the tennis court pain-free.
Discussion: PVT poses significant morbidity in young patients, as it may lead to hepatic ischemia and dysfunction early in life. This case presents a staged treatment plan with escalation of treatment based on symptoms. Although guidelines for treatment of PVT with cirrhosis remain limited, direct-acting oral anticoagulants (DOACs) are increasingly popular in the treatment of PVT (3-4). DOACs represent an initial non-invasive treatment and have excellent utility for young patients given their simple dosing regimens and lack of lab monitoring (3-4). The next treatment step, in-situ thrombolysis, represents an escalation to a minimally invasive, catheter-based procedure (4-6). Most patients experience partial to full recanalization, however the risks and benefits of pharmacologic treatment versus in-situ thrombolysis are still being explored (4-6).
P13. Severe Aortic Insufficiency Requiring ECMO Support Revealed After Cholecystectomy in a Patient with Repaired Taussig-Bing Anomaly
Henna Awan1, Mobin Kheirkhahan1, Ervin Fox1
1. University of Mississippi Medical Center, Jackson, MS, United States.
Introduction: Patients with congenital cardiac defects require extensive monitoring in specialized clinics especially once they reach adulthood. We present a unique case of a young adult female with Taussig-Bing anomaly intervened on in infancy who required extracorporeal membrane oxygenation (ECMO) due to severe aortic insufficiency revealed after a routine cholecystectomy.
Case Presentation: A 21-year-old female with a medical history significant for a double outlet right ventricle (Taussig-Bing anomaly) corrected with arterial switch operation (ASO), ventricular septal defect (VSD) patch closure, and aortic arch augmentation, patch arterioplasty of right coronary ostium,and left ventricular outflow tract obstruction resection with aortic root replacement presented to the cardiology clinic with complaints of atrial tachycardia and weight loss. She was directly admitted to the hospital for further workup and was found to have symptomatic acalculous cholecystitis. She underwent a laparoscopic cholecystectomy that was complicated by a bradycardic and hypotensive cardiac arrest requiring ACLS. ROSC was achieved but patient required high amounts of vasopressors and was ultimately cannulated for ECMO. On ECMO, her hemodynamics improved, and she was subsequently decannulated after 4 days. Unfortunately, shortly after decannulation, she exhibited anterior ST depressions on EKG as well as labile hemodynamics. She was recannulated again 5 days later. Interventional and congenital cardiology teams assisted with evaluation and determined that patient had ostial RCA disease that was a large contributor to her hemodynamic compromise. She underwent percutaneous coronary intervention (PCI) and had some improvement in systolic function. Multiple attempts were made to wean patient off of ECMO but she did not tolerate it and instead experienced a decrease in systolic function (and eventual hypotension) with decreasing ECMO flow. Transthoracic echocardiogram (TTE) performed during her hospitalization showed worsened aortic insufficiency. With the assistance of multidisciplinary meetings, a transcatheter aortic valve replacement (TAVR) was decided as the next step. She successfully underwent this procedure and was able to be weaned from ECMO 23 days into her admission. Patient was discharged after spending 49 days in the hospital with close follow up with the adult congenital cardiology clinic.
Conclusion: Neo-aortic dysfunction is a known complication in patients that have been surgically treated for Taussig-Bing anomaly. However, knowing such outcomes require specialists who have been trained in identifying them. In the case of our patient, she was well-established with a congenital cardiology team that was following her healthcare in her adulthood. Given that our patient had been followed by both pediatric and adult physicians, she was able to benefit from a team familiar with the complications that can arise in adulthood in patients with congenital cardiac defects.
P14. Endoscopic Third Ventriculostomy as a Treatment for Persistent Obstructive Hydrocephalus following Surgical Resection of Pilocytic Astrocytoma
Ryan T. Brummond1, 2, Michelle Patel3, Ankita Vayalapalli3, Renuka Mehta4
1. Pediatrics, Medical College of Georgia, Augusta, GA, GA, United States.
2. Medical Detachment, Rhode Island Army National Guard, Providence, RI, United States.
3. Medical College of Georgia, Augusta, GA, United States.
4. Pediatric Critical Care, Medical College of Georgia, Augusta, GA, United States.
Case Report: Pilocytic Astrocytoma (PA) is a common childhood brain tumor which can present with brainstem compression and Obstructive Hydrocephalus (OH). Hydrocephalus is typically resolved after total resection of PA but can occasionally persists due to inflammation, blood clots and/or residual tumor, therefore requiring placement of a Ventriculoperitoneal Shunt (VPS). Won et al., found post-operative OH in 37.5% of pediatric patients following PA resection, all of whom were subsequently treated with VPS. However, shunt-related complications commonly arise following placement and can be avoided using Endoscopic Third Ventriculostomy (ETV) as an alternative treatment (Won et al., 2020). We herein describe a rare case in which resolution of persistent OH following resection of PA was achieved using ETV.
The patient is a 3-year-old male with no significant past medical history who presented with altered mental status and neck stiffness/pain for 1 week. Urgent Head CT scan of head revealed a 4.1 x 3.8 x 5.2 cm mass at the midline cerebellar vermis with impending upward trans tentorial herniation secondary to surrounding vasogenic edema and OH. Patient was promptly admitted to the Pediatric Intensive Care Unit (PICU) and emergent placement of an External Ventricular Drain (EVD) was performed at the bedside. Patient underwent suboccipital craniotomy for resection of the PA the following day. Post-operative T2 FLAIR MRI revealed a hyperintense mass-like lesion in the region of superior medullary velum with persistent OH, and patient continued to have elevated intracranial pressure (ICP) with high cerebrospinal fluid drainage.
ETV was performed 10 days following the PA resection, ultimately leading to successful resolution of elevated ICP and OH. Patient was discharged home 25 days following the ETV. This clinical case demonstrates that ETV can be used as a successful intervention in the management of persistent OH, thereby preventing the development of VPS-related complications.
References: Won, SY., Dubinski, D., Behmanesh, B. et al. Management of hydrocephalus after resection of posterior fossa lesions in pediatric and adult patients—predictors for development of hydrocephalus. Neurosurg Rev 43, 1143–1150 (2020). https://doi.org/10.1007/s10143-019-01139-8
P15. “Switching Beats”: A Case Report Highlighting the Extravascular Implantable Cardioverter-Defibrillator
Nicole Mamprejew1, Sankalp Patel2, Luis Rechani2, Samantha Sublette2
1. Graduate Medical Education, NCH Healthcare System, Naples, FL, United States.
2. Rooney Heart Institute, NCH Healthcare System, Naples, FL, United States.
Introduction: Effective defibrillation capability in patients with poor vasculature and elevated infection risk was thought to be resolved with the standard subcutaneous implantable cardioverter-defibrillator (SICD). Lead placement on the sternal body mandates elevated energy and lacks anti-tachycardia pacing (ATP) and pause prevention, standard in most transvenous implantable cardioverter-defibrillators (TICDs). The extravascular implantable cardioverter-defibrillator (EICD) circumvents the limitations of most TICDs and SICDs, with reduction in defibrillation energy, ATP and pause prevention capability, and accessibility in poor vasculature. This case demonstrates the optimal scenario for an EICD, comparing it to the SICD and TICD.
Case Description: A 77 year old male with history of ischemic cardiomyopathy with baseline ejection fraction (EF) of 25%, TICD complicated by Staphylococcus Aureus bacteremia with device extraction and replacement with SICD, peripheral vascular disease, and coronary disease managed with 7 stents presented with chest pain, flushing, and syncopal spell. On arrival, he was in monomorphic ventricular tachycardia (VT). His SICD was inattentive to the arrhythmia given a response rate set above 200 beats per minute due to prior inappropriate therapy delivery. The patient chemically converted into sinus rhythm with an amiodarone bolus, resulting in resolution of symptoms. A transthoracic echocardiogram showed unchanged EF at 25% and no new valvulopathies. Left heart catheterization revealed in-stent restenosis within the left anterior descending artery (LAD), successfully treated with 2 overlapping drug-eluting stents. Next, an electrophysiology study (EPS) unveiled inducible VT in the territory of the LAD lesion. This area was successfully ablated in routine fashion with confirmation of no further VT induction. Though re-installment of a TICD was considered, given the patient’s bacteremia history and poor peripheral access, he underwent EICD placement, and removal of prior SICD system.
Discussion: We highlight a patient with monomorphic VT from ischemic substrate and prior scar, in need of reliable ICD therapy. The patient demonstrated SICD failure to deliver therapy and intolerance to TICD systems, meeting indication for an EICD system. The EICD has the multimodal treatment benefits of a TICD, by providing defibrillating energy, ATP, and pause-preventing pacing, with the benefits of the SICD, including lower rates of infection, bacteremia, endocarditis, cardiac perforation, lead failure, pneumothorax, and vascular injury. ICD selection requires careful consideration of unique patient characteristics for the most appropriate device to balance the benefits of treatment and risks of complications.
P16. Misleading High-Sensitive Cardiac Troponin T Elevation in Poorly Controlled Polymyositis: A Case Report
Azeem Rathore1, Jahanzaib Ekram4, Jeremy Williams1, Cristine Arcilla2, Ikwinder Preet Kaur2, Dinesh Kadariya3, Mint Thway2, Gurjit Kaeley2
1. Internal Medicine, University of Florida Health Science Center, Jacksonville, FL, United States.
2. Internal Medicine, Division of Rheumatology, University of Florida Health Science Center, Jacksonville, FL, United States.
3. Medicine, Division of Cardiology, University of Florida Health Science Center, Jacksonville, FL, United States.
4. Morsani College of Medicine, University of South Florida, Tampa, FL, United States.
Background: Elevations in cardiac enzyme levels are commonly understood as markers for myocardial ischemia. However, these elevations may stem from diverse conditions, such as inflammatory myopathies. Indeed, the presence of cardiac involvement in myopathies is linked to elevated mortality rates. However, false-positive outcomes can occur due to cross-reactivity in the Troponin T assay, triggered by different cardiac troponin forms. We present a case of recurrent and elevated high-sensitive cardiac troponin T levels in the setting of polymyositis.
Case: A 50-year-old female with a medical history of poorly controlled polymyositis to the emergency department complaining of pleuritic chest pain. She stated her chest pain was intermittent and located on her left lower rib. She was recently discharged for a previous myositis flare-up and admits to poor compliance with her tapered prednisone regimen. Initial vitals were unremarkable and physical examination was significant for diffuse joint and muscle pains. Laboratory investigations revealed elevated high-sensitive cardiac troponin T levels (normal < 14ng/L) that were uptrending (535-528-566-587) along with elevated C-reactive protein and creatinine kinase levels. Chest CTA revealed a small right lower lobe consolidation, but no right heart strain or pulmonary embolism. ECG did not show signs of pericarditis or ischemia. Previous cardiac work-up included a TTE with normal ventricular size and function, MPI without any inducible ischemia, and cardiac MRI without perfusion defects or myocardial abnormalities.
Decision-making: To determine whether the rise in cardiac enzymes is attributable to inflammatory myositis or myocardial injury, Troponin T should be measured by confirmatory Troponin I to screen patients for subclinical cardiac disease or low-grade skeletal muscle disease activity. Cardiac troponin levels continued to increase (796-737) and cardiology was consulted. A repeat TTE was performed which was stable. With recurring elevated troponin levels over seven months (see Figure 1) and a recent hospitalization of similar chest pain with elevated troponins (314-330-363), a heart catheterization was recommended but the patient declined. The patient was discharged on Day 5 with a tapered prednisone and methotrexate regimen.
Conclusion: Troponin I is specific for cardiac muscle whereas Troponin T is expressed by skeletal muscle, including regenerating skeletal muscle tissue. By assessing Troponin I levels, we can ascertain whether patients with myositis require additional cardiac evaluation or if the enzyme elevation is linked to their underlying disease. The detection of specific antibodies, like the SRP antibody, further elevates suspicion of cardiac involvement, despite its absence in our patient’s case. Clinicians need to be aware of the possibility that noncardiac increases in Troponin T may occur and lead to a possible false-positive diagnosis of cardiac injury when skeletal muscle pathology is present.
High-Sensitive Troponin T Zero Hour measurements during eleven healthcare encounters, including emergency room visits and hospitalizations.
P17. It’s a Heartache: A Case of Chlamydial Myocarditis
Abigail Zane2, Aesha Patel1, Kelsey Ivey1
1. Internal Medicine, University of Alabama Birmingham School of Medicine Huntsville Campus, Huntsville, AL, United States.
2. University of Alabama School of Medicine, Huntsville, AL, United States.
Case Report: Myocarditis is an inflammatory disease of the myocardium that can be due to infectious or noninfectious origins, and clinical manifestations can be highly variable. We present a patient with a rare etiology of myocarditis.
A 20-year-old male presented with three days of acute crushing, pleuritic chest pain associated with an episode of vomiting. On physical examination, the pain was reproducible with sternal palpation and slightly improved by leaning forward. The patient was hemodynamically stable. Laboratory results were significant for an elevated troponin of 603 ng/L, creatine phosphokinase of 579 EnzU/L, white blood cell count of 22.03x10^3/µL and C-reactive protein of 4.6 mg/dL. An electrocardiogram showed sinus arrhythmia. Echocardiogram and coronary computed tomography were remarkable for mild left ventricular hypertrophy with no pericardial effusion. Cardiac magnetic resonance imaging (MRI) showed basal and inferolateral wall myocardial edema, hyperemia, and nonischemic mid-wall enhancement consistent with myocarditis. The patient’s troponin reached a peak of 1,426 ng/L and began trending down. An extensive infectious and autoimmune laboratory workup, including COVID PCR, respiratory viral panel, HIV, Hepatitis panel, ANA, etc. was negative, other than a positive urine PCR for Chlamydia trachomatis. Of note, the patient denied any genitourinary symptoms during his hospital stay. He reported no recent medications and or vaccinations. The patient was discharged after four days and received doxycycline for 21 days. On cardiology follow-up one month post discharge, he was doing well.
Discussion: C. trachomatis is a gram-negative bacterium responsible for the majority of sexually transmitted infections in the United States. Genitourinary infections are commonly asymptomatic, as in our patient, but can cause dysuria, polyuria, discharge, bleeding, and dyspareunia. Because chlamydial infection may present with complications of infection rather than the expected genitourinary presentation, this case exhibits the importance of including sexual history as part of the history-taking process on all patients. Antibody formation to various chlamydiae species, including C. pneumoniae, C. psittaci, and C. trachomatis, has been linked to myocarditis in mice and there have been rare case reports in humans as well. Through molecular mimicry, Chlamydial proteins trigger an autoimmune response toward myocardial tissue. Due to the infrequency of myocarditis, a presumptive diagnosis is often made by clinical presentation to avoid the risk associated with a more definitive diagnosis with biopsy. Diagnosis can also be further supported by cardiac MRI with high specificity in detecting edematous changes correlating with histologic and immunohistologic criteria. In our patient, cardiac MRI was the only imaging study that demonstrated findings consistent with myocarditis, which resolved with treatment of the presumed causative Chlamydial infection with doxycycline.
P18. Hemolytic Uremic Syndrome: Not Just a Pediatric Disease
Varshini Venkatesan1
1. Internal Medicine, Brookwood Baptist Health Residency Program, Birmingham, AL, United States.
Case Report: History: 35-year-old male without significant past medical history presented with 1 week of worsening right sided abdominal pain and 2 episodes of hematemesis. 1 week prior, he was seen at an Urgent Care for diarrhea and prescribed Levofloxacin for possible colitis. His diarrhea resolved, but abdominal pain worsened. He had also developed 3-4 episodes of bilious emesis daily, and eventually, hematemesis on day of admission. Associated symptoms included chills, fatigue, loss of appetite, and dark urine. He denied fever, diarrhea, hematochezia, dizziness, confusion, recent travel, known sick contact. Family history of father with Crohn disease.
Physical Exam: Vitals: Temp 99.7F, HR 110, BP 150/88, RR 18, SpO2 99% on RA, BMI 29.1.
Patient appeared stated age and in no obvious distress. PERRL, EOMI with pale conjunctiva and icteric sclera. Lungs clear to auscultation bilaterally. Abdomen soft, nondistended, but tender to palpation of right lower quadrant and suprapubic region with guarding, no rebound tenderness. Alert and oriented, without focal neurological deficits. No evidence of skin changes including cyanosis, bruises, or petechiae.
Labs: Hgb 8.9, Hct 24.9, Platelet 13, Retic Ct 4.4%, Cr 2.6, Total bili 5.2, Direct bili 0.6, Fibrinogen 344, haptoglobin 7.8, LDH 2015, ADAMST13 75%, Coombs negative, Peripheral blood smear: multiple shistocytes, few platelets, RBC fragments. Stool culture – e.coli with STx 1.
Final diagnosis: Hemolytic Uremic Syndrome
Discussion: Hemolytic uremic syndrome (HUS) is a microvascular occlusive disease characterized clinically by the classic triad of thrombocytopenia, microangiopathic hemolytic anemia, and acute renal failure (or any signs of end organ damage). Typical HUS is a rare occurrence in healthy adults as it is predominantly a pediatric disease. It is mainly associated with STEC (Shiga toxin producing E. coli) or SP (Streptococcus pneumoniae). Known risk factors include undercooked beef and dairy products, contaminated water, and recent viral illness. Pathogenesis involves fecal oral transmission of the shiga toxin that enters the systemic circulation to target endothelial cells with G3b receptors, causing detachment and apoptosis, resulting in hemolytic anemia and mass platelet consumption. Diagnosis is confirmed with stool culture, PCR, and serologic testing (anti-O157 Ab titer), but late stool collection and antibiotic use can result in a false negative. Mainstay of treatment for typical HUS is supportive care with adequate hydration, anti-emetics, and blood transfusions if needed. Although it is the treatment for atypical HUS, Eculizumab can be used for severe neurological complications in typical HUS. Our patient presented with severe thrombocytopenia after diarrheal illness, raising high concern for HUS. Due to its similarity to TTP, ADAMTS13 level was needed to confirm diagnosis. Supportive measures were in place and patient recovered within 48 hours.
P19. Saved by Sepsis? Type B Aortic Dissection Complicated by Clonidine Withdrawal Masked by MRSA Bacteremia
Henna Awan1, Mobin Kheirkhahan1, Ervin Fox1
1. Medicine, University of Mississippi Medical Center, Jackson, MS, United States.
Introduction: “Impulse control” is a well-known strategy for medically managing aortic dissection, aimed at halting its progression, organ damage, and managing pain. In this case, we discuss the application of this strategy in a critical condition that made achieving impulse control very challenging.
Case Presentation: A 36-year-old woman with end-stage renal disease (ESRD) on hemodialysis (HD) via a tunneled dialysis catheter (TDC), resistant hypertension, heart failure with reduced ejection fracture (HFrEF), and a mechanical mitral valve on warfarin, presented to the hospital with a two-day history of nausea, vomiting, poor intake, severe weakness, and orthostatic lightheadedness. In the ED, she was noted to be hypotensive and tachycardic. Physical exam was remarkable for diffused abdominal tenderness and ascites. Initial labs showed a leukocytosis, elevated proBNP, and supra-therapeutic INR (7.73). She received IV fluids, blood cultures were drawn, and vancomycin and cefepime were started. Cultures grew gram positive cocci (later identified as MRSA). Transthoracic echocardiography showed a mobile mass at the tip of TDC in her right atrium; however, TDC removal nor paracentesis could be performed due her INR. A CT chest/abdomen was obtained because of worsened abdominal pain which showed a type B aortic dissection extending to the internal iliac arteries. As part of impulse control, we aimed to maintain her systolic blood pressure <120 mmHg, and heart rate ideally <60 but practically <100. However, because of ongoing sepsis, bacteremia, and clonidine withdrawal, we could not strictly adhere to these parameters. To control the infectious source more rapidly, vitamin K was given. With improvement in her INR, the TDC was removed, and paracentesis performed. Subsequent blood cultures showed no growth. With improvement of her infection, impulse control was pursued more aggressively by starting guideline directed medical therapy. After 48 hours without growth in blood cultures, the TDC was replaced, HD was resumed, and her home clonidine was permanently discontinued.
Conclusion: First, impulse control is the cornerstone of medical management of aortic dissection, but other clinical conditions with competing hemodynamic goals might be present. It is of utmost importance to monitor patients closely and ensure that while we are controlling their heart rate, we are not pushing them towards decompensated shock. Second, rapid source control in severe sepsis is essential in improving patient outcomes. Finally, clonidine with its short half-life and risk of rebound tachycardia and withdrawal is not an appropriate agent for aortic dissection and other oral antihypertensives should be pursued and maximized before considering this for blood pressure control.
P20. A Case of Coccidiomycosis Confounding a Systemic Lupus Erythematosus Diagnosis
1. Internal Medicine, LSUHSC, New Orleans, LA, United States.
Intro: Systemic Lupus Erythematosis is a rare autoimmune disease with prevalence of 20-150 cases per 100,000 in the United States. Despite increased awareness among physicians and improvements in serologic testing, the time to diagnosis from onset of symptoms is still delayed, with one study estimating average time to diagnosis of 6 years. One significant cause of delay is due to the heterogeneity in the disease presentation, with symptoms that can present similarly to many other autoimmune, infectious, or hematologic diseases. Many of the nonspecific symptoms of SLE, such as night sweats, weight loss, symmetric arthralgias, and rash, are very similar to symptoms of cocciodiodomycosis infection. While there are an estimated 150,000 cases of coccidiodal infections in the U.S annually, 60% of patients are asymptomatic. Those who are symptomatic, experience those listed above, which can obfuscate and further delay an already difficult to diagnose rare disease, as evidenced in this case.
Presentation: A 33-year-old Hispanic male with no significant past medical history presented with a 3-week history of cough, hemoptysis, fevers, fatigue, myalgias, and loss of appetite. He had recently traveled to Arizona where his symptoms began, and was given a course of antibiotics without improvement. During his admission, patient tested positive for Coccidioides Ab IgM, Coccidioides titer of <1:2, and Coccidioides immitis Ab <1:2. Respiratory sputum culture grew 2 colonies of Coccidioides immitis/posadasii. While at the time, patient was positive for anti-dsDNA 94, anti-RNP, anti-SM, anti-smRNP, and anti-chromatin, the positivity was attributed to acute infection rather than SLE. He was discharged on a 3-month course of fluconazole and outpatient follow-up.
Patient was subsequently lost to follow-up, presenting 9 months later with worsening dyspnea, cough, rash and weight loss. Given the patient’s history, there was high concern for recurrent or disseminated Coccidioidosis. Patient underwent full workup including imaging, lab studies (hepatitis, HIV, fungal, bacterial) and biopsies (renal, lymph nodes, bone marrow, skin, gastrointestinal). After ruling out infections and malignancy, attention turned to SLE with patient being positive again for SLE markers and positive dsDNA Crithidia (1:160). Patient was started on steroids and hydroxychloroquine with symptom improvement.
In this case of a patient with concomitant Coccidioides and SLE, it is still difficult to delineate if the patient’s already existing SLE resulted in an immunocompromised state that allowed the Coccidioides infection to become symptomatic, or if it was the infection that triggered or unmasked an underlying SLE. Because of the non-specific presentation and inconsistent follow-up, the patient’s final diagnosis was not reached until over 1 year after symptom onset and potentially longer given the uncertainty of when symptoms actually began.
Patient with facial and lip edema as well as a faint malar rash.
Chest with new circular diffuse rash with central clearing. Skin punch biopsy revealed mild lichenoid lymphocytic infiltrate and dermal mucinosis with interface dermatitis, pattern that could be seen in dermatomyositis and mixed connective tissue disease.
P21. Augmentin’ a DILI-emma
Javier K. Nishikawa1, Hunter Johnson1, Alan Baggett1
1. UAB Heersink School of Medicine, Huntsville, AL, United States.
Case Report: A 35 year-old-male with a past medical history of splenectomy and abdominal hernia presented to the emergency room with several days of worsening left upper quadrant pain. The pain radiated diffusely across the upper abdomen and was associated with nausea without vomiting. The patient reported no inciting or exacerbating factors and was recently treated with 10 days of amoxicillin-clavulanate, steroids, and an inhaler for a sinus infection. Social history was non-contributing. Initial lab results showed elevated AST of 305 EnzU/L and ALT of 136 EnzU/L, elevated total and direct bilirubin at 3.1mg/dL and 1.4mg/dL, respectively, and elevated alkaline phosphatase (ALP) at 343 EnzU/L. White blood cell count was elevated at 19.81 cells/mL and platelets of 439 cells/mL with coagulation studies and electrolytes within normal range. The patient was hemodynamically stable. Imaging included an ultrasound of the abdomen and gallbladder, a CT of the chest and abdomen, and an MRI MRCP. These studies collectively showed mild gallbladder wall thickening with no gallstones or biliary ductal dilation, a midline hernia defect, and vague heterogenous attenuation of the liver with minimal abdominal ascites. A HIDA scan suggested acalculous cholecystitis, and a cholecystectomy with ventral hernia repair was performed. Despite this, the patient continued to have transaminitis and total bilirubin increased to 9.1mg/dL. This worsening prompted a liver biopsy that showed bland lobular cholestasis consistent with drug induced liver injury (DILI). Amoxicillin-clavulanate had been discontinued at admission, and supportive care continued until the patient was ready for discharge.
DILI can be acute or chronic and follows a hepatic, cholestatic, or mixed pattern of injury. Diagnosis is made via biopsy. Treatment begins with immediate discontinuation of the offending agent and initiation of supportive care. An R ratio determines the category of injury and is calculated as shown in Equation 1
(1)R=(ALTValue/ALTULN)/(ALPValue/ALPULN)
where a value greater than 5 is hepatocellular, less than 2 is cholestatic and in between is mixed. The pathophysiology of DILI can be intrinsic, as with acetaminophen, where a certain drug causes reproducible damage in a dose-dependent manner, or can be idiosyncratic which is unpredictable and independent of dose. Idiosyncratic DILI usually occurs 7-14 days following ingestion and the mechanism is unknown but thought to be multifactorial combining host, drug, and environmental factors. Amoxicillin-clavunate (Augmentin) is the most common antibiotic cause of idiosyncratic DILI, usually presenting in men with mixed hepatocellular-cholestatic injury. Combined amoxicillin-clavunate causes more DILI than amoxicillin alone. This case demonstrates the importance of taking a thorough history including all recent medication changes, and the presentation of a rare adverse effect of a commonly prescribed antibiotic.
P22. A Unique Case of Primary Pulmonary Cryptococcosis Presenting with Bilateral Lung Nodules
Soumyadeep Bag1, Farrah Ibrahim1, Ali Hachem1, Zohra Chaudhry2
1. Internal Medicine, Huntsville Regional Campus, UAB Heersink School of Medicine, Huntsville, AL, United States.
2. Infectious Diseases, Alabama Infectious Disease Center, Huntsville, AL, United States.
Case Report: Mr. H is a 77-year-old male who presented to the emergency department with fatigue and poor oral intake. Past medical history is significant for Type II Diabetes mellitus, severe protein-calorie malnutrition, peripheral neuropathy, stage IV CKD, hypertension and remote history of bladder cancer treated with right nephrectomy and cystectomy with urostomy.
He had several hospitalizations within the past year for similar symptoms, most recently a month ago. A chest CT during that admission showed bilateral lung infiltrates suggestive of multifocal pneumonia. A PET scan 2 weeks later showed multiple pulmonary nodules in the right upper, right middle and bilateral lower lobes with increased FDG uptake suspicious for metastasis.
On presentation, he looked chronically ill with bitemporal wasting and significant weight loss. His urostomy was patent. His vitals were grossly unremarkable. His chest x-ray was concerning for progression of metastatic disease and possible development of overlying pneumonia. He subsequently underwent CT-guided biopsy of one of the right-sided lung nodules along with PEG tube placement to help with feeding/malnutrition.
The lung biopsy showed benign alveolar tissue with vague granulomatous inflammation, negative for malignancy. Acid-fast stain was negative for mycobacteria, but GMS stain was positive for abundant fungal yeast forms. PAS fungal stain was positive, making Histoplasma unlikely and Alcian blue and mucicarmine stains were negative, making Cryptococcus unlikely. Fungal serologies, including Histoplasma, Coccidioides, Blastomyces, aspergillus antigen, rapid candida panel and (1-3)-β-d-glucan were negative. However, his serum cryptococcal antigen (CrAg) was positive with a titer of 1:40, which later worsened to 1:160. He underwent a lumbar puncture which was negative for any CNS infection, and blood cultures remained negative. Mr. H was initially started empirically on Isavuconazole. Once work-up was positive for pulmonary cryptococcosis, he was switched to high-dose IV Fluconazole(12mg/kg/day). Eventually, his serum CrAg started downtrending, and he was discharged on oral fluconazole 800mg daily for 12 weeks with plans to trend serum CrAg outpatient.
Discussion: Although Cryptococcus mainly causes CNS infections, primary lung infections such as multifocal pneumonia should be considered, especially in the immunocompromised. The clinical picture may mimic lung metastasis or other fungal infections such as Histoplasma or Aspergillus. Although fungal stains for mucin can help establish a diagnosis, they are often negative, as was the case for our patient. So, treatment should be started based on serum antigen detection while awaiting culture/PCR. Also of note: although Isavuconazole has comprehensive coverage against several fungi, high-dose fluconazole remains the drug of choice for non-CNS cryptococcosis. Patients often require an extended course, sometimes up to 6-12 months.
P23. Devastating Effects of Untreated Acute Bacterial Sinusitis Causing Pott’s Puffy Tumor in an 11-Year-Old Child: A Case Report
Alfredo J. Pacheco Aponte1, Taylor Smith1, Fatma Levent1
1. Adventhealth, Orlando, FL, United States.
Introduction: Sinusitis is a common condition in children and does not normally lead to significant complications, however in some cases, the inflammation and tissue disruption associated with sinusitis allows for the invasion of normal nasopharyngeal flora, causing infection and abscess. Most cases of Pott’s Puffy Tumor are associated with frontal sinusitis, and adolescents have a higher risk. The infection is often polymicrobial including nasal flora. A recent case series showed the association between Streptococcus intermedius and brain abscesses causing life-threatening intracranial infections. The case series also highlights the increase in the incidence of intracranial infections caused by Streptococcus intermedius after the COVID-19 pandemic.
Case Description: We introduce the case of a previously healthy 11-year-old male presenting with nine days of cough, congestion, fevers, and headache. Physical examination was significant for bilateral periorbital edema and erythema with frontal scalp swelling and tenderness. Labs revealed leukocytosis and significantly elevated inflammatory markers. Computed tomography of the sella and orbits revealed findings suggestive of acute sinusitis complicated by a periosteal abscess (i.e. Pott’s Puffy Tumor) in the left frontal subcutaneous region, orbit, and maxillary sinus. Additionally, suggestive findings of left myositis of the medial rectus and inferior rectus along with hypoattenuation in the frontal region of the brain. Magnetic resonance imaging of the brain and magnetic resonance venous imaging revealed no thrombosis or intracranial extension along with prior findings. The patient was initially started on intravenous ampicillin and sulbactam, which was switched to ceftriaxone and metronidazole empirically. On day 2 of admission, the patient underwent sinus drainage of the left maxillary, frontal ethmoid, and orbital subperiosteal abscess. Drainage cultures were collected at the time of surgery and were positive for Streptococcus intermedius. The patient completed five days of intravenous antibiotic therapy with significant improvement in clinical presentation and was transitioned to a prolonged course of oral amoxicillin-clavulanate to complete four weeks of therapy.
Discussion: Acute bacterial sinusitis is a common condition found in many children, however, in some cases, it can progress to a more severe form of infection such as Pott’s Puffy Tumor, a life-threatening condition that requires prompt IV antibiotics and surgical drainage. There appears to be a relation between Streptococcus intermedius and the formation of brain abscesses, seen most frequently since the beginning of the COVID-19 pandemic. More research should be done in the future to study the true relationship between Streptococcus intermedius and brain abscess, however, empirical therapy should include coverage of this microorganism as it seems to be found commonly as a cause of Pott’s Puffy Tumor.
P24. Longitudinal Analysis of Bacterial Species Composition among Women with Incident Bacterial Vaginosis Illuminated through Peptide Nucleic Acid Fluorescence in situ Hybridization
Sheridan D. George1, Chaoling Dong1, Kristal J. Aaron1, Alex Sherman1, Olivia T. Van Gerwen1, Ashutosh Tamhane2, 3, Christopher M. Taylor4, Lúcia G. Sousa5, Carina Almeida6, 7, Nuno Cerca5, Christina A. Muzny1
1. Division of Infectious Diseases, University of Alabama at Birmingham, Birmingham, AL, United States.
2. Division of Nephrology, University of Alabama at Birmingham, Birmingham, AL, United States.
3. Center for Clinical and Translational Sciences, University of Alabama at Birmingham, Birmingham, AL, United States.
4. Department of Microbiology, Immunology, and Parasitology, Louisiana State University Health Sciences Center, New Orleans, LA, United States.
5. Laboratory of Research in Biofilms Rosário Oliveira, Centre of Biological Engineering, University of Minho, Braga, Portugal.
6. Laboratory for Process Engineering, Environment, Biotechnology, and Energy, University of Porto, Porto, Portugal.
7. Associate Laboratory in Chemical Engineering, University of Porto, Porto, Portugal.
Purpose of Study: Bacterial vaginosis (BV) is characterized by depletion of Lactobacillus species and overgrowth of anaerobic bacteria. However, its etiology remains unknown. Key BV-associated bacteria (BVAB) that may be important in incident BV (iBV) pathogenesis are Gardnerella species and Prevotella bivia. We aimed to quantify the amount of these bacterial species in clue cell biofilms in specimens prior to iBV (cases) and controls using peptide nucleic acid fluorescence in situ hybridization (PNA-FISH).
Methods Used: Women ages 18-45 years with normal vaginal microbiota were enrolled to self-collect twice daily vaginal specimens for 60 days. iBV was defined as a Nugent score of 7-10 on ≥4 consecutive specimens. For women who developed iBV (cases), twice daily specimens for 14 days prior to iBV, day of iBV (day 0), and days post-iBV (days 1-3) were selected. Specimens from women with normal vaginal microbiota (controls), comparable by age, race, contraceptive use, and menstrual cycle, were selected. Fluorescent PNA probes were used to quantify the amount of Gardnerella spp. and P. bivia in clue cell biofilms; Alexa Fluor 594 and 488 were conjugated for targeting Gardnerella spp. and P. bivia, respectively. DAPI was used for counterstaining of bacterial DNA. Six epi-fluorescent microscopic images were captured per specimen using the EVOS M5000 Imaging System. Bacterial counts were determined using the auto or manual count tools of the imaging system.
Summary of Results: As of 1/22/24, 103 women were enrolled and 9 (9.3%) developed iBV; 9 controls were selected. There were no meaningful differences in characteristics between groups. PNA-FISH has been completed for 5 cases (168 specimens) and 2 controls (56 specimens). The pooled Gardnerella spp. counts for both cases and controls varied over time but there were notable spikes on certain days prior to iBV and after. There was an increase on days -5.5 to -3.5 (median Gardnerella spp. counts 179.0, 103.5, 155.5, 86.5, and 31.5). In contrast, the median Gardnerella spp. counts for pooled controls during this time was 1.0, 4.5, 1.0, 1.5, and 3.0. Interestingly, as pooled cases approached the day of iBV, Gardnerella spp. counts decreased but spiked again on days 1-3 post iBV (median Gardnerella spp. counts 38.0, 170.0, 218.5, 146.5, 237.5, 236.0, and 123.0). In contrast, median Gardnerella spp. counts for pooled controls on days 1-3 were 16.5, 5.5, 4.5, 6.0, 5.5, 26.0, and 7.0. Pooled P. bivia counts for both cases and controls also varied over time. Counts for pooled cases followed a similar pattern to Gardnerella spp., but more subtle due to smaller ranges of the count data.
Conclusions: P. bivia was detected in clue cell biofilms, although in smaller amounts than Gardnerella spp. Spikes in Gardnerella spp.counts at specific times suggest when key events in iBV pathogenesis may be occurring.
P25. Evaluating the Risk of Skin Infections in End-Stage Renal Disease Patients with Comorbid Porphyria Cutanea Tarda
Edwine Coulanges1, Resean Wallace1, Jennifer Waller1, Stephanie Baer1, Wendy Bollag1
1. Medical College of Georgia, Augusta University, Augusta, GA, United States.
Purpose of Study: Porphyria cutanea tarda (PCT) is one of many metabolic conditions characterized by increased photosensitivity, manifesting as blistering skin lesions on areas exposed to the sun. Due to the increased photosensitivity and skin fragility, PCT patients are more susceptible to skin infections. End-stage renal disease (ESRD) is a potential complication of PCT, and individuals with ESRD also exhibit an increased risk of infection.
Methods Used: Therefore, a retrospective cohort study using the United States Renal Data System database from 2005-2019 was conducted to determine if PCT is an independent risk factor for certain infections in the ESRD population using International Classification of Disease (ICD)-9 and ICD-10 codes. A diagnosis of PCT was determined in 1,019 out of a total of 1,398,765 ESRD patients who met the inclusion and exclusion criteria, with bacterial infections, cellulitis, blisters, abscesses, and bacteremia queried as outcomes.
Summary of Results: Logistic regression analysis determined the impact of PCT on the risk of each infection after controlling for demographic and clinical factors. PCT was associated with a significantly decreased risk for 3 out of the 5 queried infections: bacterial infections (adjusted odds ratio: 0.50; 95% confidence interval: 0.43-0.58), cellulitis (0.61; 0.53-0.71), and bacteremia (0.44; 0.38-0.52). No significant positive or negative association was found between PCT and blisters or abscesses.
Conclusions: These results indicate that ESRD patients with PCT are actually at a decreased risk of some infections compared with ESRD patients without. The reason is unclear but could be related to either the disease process or its clinical management.
P26. Association of Pemphigus Vulgaris and Mortality in End Stage Renal Disease Patients
Nadia N. Talebi1, Sara Attari1, Jennifer Waller1, Stephanie Baer1, 3, Wendy Bollag2, 3
1. Medical College of Georgia, Augusta, GA, United States.
2. Augusta University, Augusta, GA, United States.
3. Charlie Norwood VA, Augusta, GA, United States.
Purpose of Study: Pemphigus vulgaris is an autoimmune disease characterized by flaccid bullae on mucosal and cutaneous surfaces. Pemphigus vulgaris is a life-threatening disease with a mortality rate three times higher than that of the general population. However, little is known regarding the impact of pemphigus vulgaris as a comorbid condition. This study aimed to determine if patients with end-stage renal disease (ESRD) and a comorbid diagnosis of pemphigus vulgaris may be at an increased risk of mortality
Methods Used: A retrospective cohort analysis of ESRD patients in the United States Renal Data System from 2005-2019 was conducted to determine if a diagnosis of pemphigus vulgaris was associated with a significantly increased risk for mortality. International Classification of Disease (ICD)-9 and ICD-10 codes were used to determine a diagnosis of pemphigus vulgaris and various comorbid conditions that were controlled for including alcohol dependence, tobacco use, and the Charlsoncomorbidity index (CCI). The relationship between pemphigus vulgaris diagnosis and one-year mortality was examined using Kaplan-Meier survival curves and Cox proportional hazards (CPH) modeling.
Summary of Results: Of the 1,413,746 individuals included for analysis, a total of 654 individuals with pemphigus vulgaris were identified. Increasing age [adjusted odds ratio (OR)=1.02; 95% confidence interval (CI)=1.01-1.03], using tobacco (OR=1.28; CI=1.09-1.51), and increasing CCI (OR=1.15; CI=1.13-1.17) were associated with an increased risk of pemphigus vulgaris. Pemphigus vulgaris was not significantly associated with mortality within one-year in either the simple model nor final multivariable model (OR=0.98; CI=0.82-1.17).
Conclusions: Other covariates found to be significantly associated with increased risk of mortality within one-year included increasing age, hemodialysis (versus peritoneal dialysis), catheter access or graft access compared to arteriovenous fistula access, and alcohol use. While female sex, black race, Hispanic ethnicity, and tobacco use were associated with a decreased risk of mortality within 1 year. These results suggest that a diagnosis of pemphigus vulgaris is not a significant risk factor for mortality in ESRD patients.
P27. A case of Membranous Nephropathy with Light Chain Restricted Deposit
Raghunandan Konda1, Jared Cook1, Deepak Chandramohan1
1. Nephrology, University of Alabama at Birmingham, Birmingham, AL, United States.
Case Report: A 36-year-old African American woman with a history of hypertension and type II diabetes mellitus for 18 years was referred for evaluation of progressive chronic kidney disease and worsening proteinuria. Her diabetes mellitus was well controlled, and she had no diabetic retinopathy and no history of nephrotic syndrome. She had a significant family history of kidney disease with a maternal aunt on intermittent hemodialysis. The diagnostic workup revealed a creatinine of 2.7 mg/dl corresponding to creatinine estimated glomerular filtration rate (eGFR) of 23 (confirmed by Cystatin C eGFR), a urine protein creatinine ratio of 10 g/g, a urine albumin creatinine ratio of 5.9 g/g, and a serum albumin of 3.1 g/dl. Further evaluation of the nephrotic range proteinuria was negative for infectious etiologies like hepatitis B, hepatitis C and human immunodeficiency virus. Autoimmune workup was negative for systemic lupus erythematosus, anti-neutrophil cytoplasmic autoantibody (ANCA)-associated vasculitis, cryoglobulinemia, and normal complement levels. Serum levels of Thrombospondin Type-1 Domain-Containing 7A Antibodies and anti–Phospholipase A2 receptor (PLA2R) antibody levels were negative. Malignancy workup revealed no M spike or monoclonal antibodies on serum and urine protein electrophoresis and immunofixation electrophoresis, serum free light chain ratio of 1.36, normal corrected calcium level and a hemoglobin of 9 g/dl. A renal biopsy was performed which revealed lambda-restricted Membraneous Nephropathy (MN), PLA2R stain was negative, no evidence of proliferative glomerular lesions, immunofluorescence showed capillary loop staining for IgG and lambda and moderate chronicity changes. Due to the presence of light chain restriction, she was referred to hematology. The lymphoproliferative disorder workup revealed peripheral blood flow cytometry a small lambda light chain restriction B cell population. Bone marrow biopsy revealed 5-10% plasma cells, positive for CD 138 but negative for clonal cells. She was diagnosed with MN with lambda- restricted light chains, after discussion with the tumor board, she began treatment with Daratumab, bortezomib, cyclophosphamide, and dexamethasone for 4-6 cycles.
Discussion: Membranous nephropathy is not an uncommon cause of nephrotic syndrome but MN with monoclonal gammopathy is rare. The natural history and clinical features have not yet been determined. We present a case of MN with lambda- restricted light chains.
This case highlights the need to evaluate progressive proteinuria in patients with diabetes mellitus and the need for renal biopsy for alternate etiologies. Primary MN is characterized by subepithelial immune complex deposits which are typically polytypic. Monotypic deposition in MN is rare and when present, should provoke suspicion of a lymphoproliferative disorder. Atypical features such as focal proliferation, absence of PLA2R positivity, and positive
P28. A Rare Case of Systemic Sclerosis with Membranous Nephropathy and Focal Segmental Glomerulosclerosis
1. Kern Medical Center, Bakerfield, CA, United States.
Introduction: Systemic sclerosis is a chronic multisystem disease characterized by widespread vascular dysfunction and progressive fibrosis of the skin and internal organs. The most common renal manifestation of systemic sclerosis is the sclerodermal renal crisis, a life-threatening emergency. Some individuals of systemic sclerosis are initially asymptomatic or show only mild proteinuria, microscopic hematuria, and occasional casts. These patients follow an indolent course until hypertension and progressive deterioration of kidney function develop. We present a patient with a very rare manifestation of systemic sclerosis.
Case Presentation: 34-year-old female presented with generalized swelling of legs, arms and face for 1 month. Swelling of legs persisted even after supportive measures and later developed more generalized swelling. She denied any urinary symptoms. On examination, vitals were stable. Physical examintaion showed bilateral pitting edema of upper and lower extremities as well as edema of the face. Urinalysis showed proteinuria and albumin-creatinine ratio was significantly elevated to 7,685. A renal biopsy was done which showed membranous nephropathy, PLA2R negative and THSD7A negative with secondary focal segmental glomerulosclerosis. Further infectious and cancer work-up was negative. ANA was found to be positive with centromere pattern, and the titer was elevated to 1:320. Anticentromere antibody was positive (3.9). Patient was treated with Losartan 50 mg daily and the urine albumin-creatinine ratio markedly decreased to 360 over a period of six months and to 91.2 over a period of 1 year. Patient did not have any other clinical manifestations of systemic sclerosis. The patient is also being followed up to monitor for any progression of proteinuria and development of other clinical features of systemic sclerosis.
Discussion: Very few cases of membranous nephropathy have been reported in patients with systemic sclerosis. In most cases, they were related to the use of D-pencillamine, but in a few patients, no cause of scleroderma was identified. Subepithelial deposits were seen on electron microscopy of these patients, suggesting that autoantibodies directed against Scl-70, centromere or polymerase III may cause formation of in-situ immune complexes. Even after thorough review of literature, we could not find any cases of FSGS in patients with systemic sclerosis.
This case highlights a rare renal manifestation of systemic sclerosis with no other clinical features illustrating the need for prompt treatment and close follow up.
References: 1 Moroni G, Ponticelli C. Secondary membranous nephropathy. Frontiers in Medicine. 2020 Dec 3;7:611317.
2 Bruni C, Cuomo G, Kidney involvement in systemic sclerosis Journal of Scleroderma and Related Disorders. 2018 Feb;3(1):43-52.
P29. A 53-Year-Old Male with Weight Loss, who Develops Joint Pain, Skin Ulcerations, and a Violaceous Rash
Soma Agrawal1, Rashmi Dixit2
1. University of California Davis, Davis, CA, United States.
2. University of California San Francisco, San Francisco, CA, United States.
Case Report: Patient is a 53-year-old male who one year prior to presenting to our clinic developed persistent joint pain in his hands. He subsequently developed weight loss, normocytic anemia, and Vitamin D deficiency. In a baseline healthcare evaluation to rule out malignancy, a chest X-ray was notable for interstitial changes, and a CT of the abdomen/pelvis with contrast revealed only increased interstitial markings at the lung bases. An upper endoscopy revealed esophagitis, and a biopsy of the second portion of the duodenum was taken showing moderate villous blunting with increased intraepithelial lymphocytes. A colonoscopy was unrevealing. Laboratory testing was remarkable for a strikingly positive tTG-IgA greater than 100 U/mL (normal 0-3 U/mL), confirming celiac disease. The patient started on a gluten-free diet and began regaining weight.
In the months prior to presentation to our rheumatology clinic, despite improvement in his gastrointestinal symptoms, his joint pain began to increase and he visited the ER on three different occasions. Patient self-referred himself to our rheumatology clinic for further evaluation of his hand joint pain. He had no weakness, cough, or dyspnea on exertion. Family history was unremarkable. Patient had a distant history of smoking a fifth of a pack per day for 10 years, was not using any alcohol or drugs, and taking no medications. On exam the patient was afebrile, BP was 127/89, and pulse 111, and respiratory rate was normal. There was mild erythema on the back in a “shawl” distribution and fine bibasilar rales. Examination of the hands revealed periungual erythema, tenderness of wrists, tender violaceous rash on bilateral palms and fingers, and ulcerated Gottron’s papules on the bilateral 2nd MCPs (see figures 1a and 1b). Motor strength exam of the upper and lower extremities, proximal and distal, was 5/5.
Clinical assessment was that his presentation and examination was very suggestive of dermatomyositis sine myositis, specifically anti-MDA5 (anti-melanoma differentiation-associated protein 5) dermatomyositis. These patients can be predisposed to rapidly progressing interstitial lung disease. Laboratory testing revealed CBC with mild stable anemia with hemoglobin of 12.2, normal CMP, ANA IFA negative, rheumatoid factor negative, CCP negative, CRP of 5, ESR of 37, HBsAg negative, Hepatitis C negative, aldolase normal, CPK 85, and T spot TB test negative. A MyoMarker 3 Plus profile confirmed MDA-5 antibodies 36 (nl<20).
Prednisone 40 mg was started, and an HRCT of the lungs and urgent referral to pulmonology was ordered. At two-week follow up, the patient’s hands had improved significantly, and CellCept 500 mg BID was initiated. Post-pulmonology workup, JAK inhibitors may be considered.
P30. What a Pain: Immune-Mediated Necrotizing Myopathy with Statin Use
1. NCH Healthcare System, Naples, FL, United States.
Introduction: Immune-mediated necrotizing myopathy (IMNM) also known as necrotizing autoimmune myopathy is classified as a rare cause of severe proximal muscle weakness. The incidence rate is about 8.3 million cases per year with a prevalence rate of 1.85 per 100,000 people.The median age afflicted is 64 with no gender specific correlation. The primary risk factors for IMNM include statin use (34%), malignancy (9.5%), connective tissue disorders, with greater than 50% being idiopathic in nature. The diagnostic gold standard is biopsy including nonspecific findings consistent with prominent necrosis and regeneration of muscle fibers without inflammatory infiltrates.
Case Presentation: Presented is a 47-year-old female, who presented with nausea, right arm pain, and blurry vision. Imaging, including magnetic resonance imaging (MRI) of the brain was consistent with 3 cerebellar lesions with locations in the right and left hemisphere, and left cerebral tonsil. Subsequently the patient was initiated on on aspirin and statin therapy with Atorvastatin 80 mg. Prior to discharge, the patient had noted myalgias but was encouraged to continue statin due to her recent ischemic event and was discharged to a rehabilitation facility. Only 5 days later, the patient returned and was found to have a progressing moderate subacute infarct, now involving the left cerebellum. The patient was closely monitored and reinitiated on statin therapy. The patient followed up in the outpatient clinic, where hypercoagulable work-up was found to be unremarkable. Additionally, repeat labs were performed showing elevated liver enzymes, and now the patient was also endorsing worsening myopathy and new muscle weakness. Due to the elevated transaminase levels and myopathy, statin therapy was continued due to her recurrent strokes, though at a lowered dose. Despite a decreased dose of statin, the patient continued to have transaminitis, and further worsening myopathy. Subsequently, the patient was referred to gastroenterology and found to have evidence of fatty liver on right upper quadrant ultrasound. Despite discontinuation of the statin therapy for a month, the patient still endorsed myopathy-like symptoms. In that setting, she was referred to Rheumatology who opted to perform a muscle biopsy was consistent with IMNM. The patient was started on glucocorticoid treatment and continued follow up in the clinic with improvement in her myopathy.
Discussion: This case represents a rare case of IMNM in which it was diagnosed after excluding other more common causes. Suspicion is often raised incidentally when statin-induced myalgia is ruled out. As clinicians, we often overestimate statin-induced myalgias despite lack of clinical evidence. In a recent randomized trial, greater than 90% of muscle related symptoms were not related to underlying statin utilization. Thus, when patients report myalgias with statins, it often indicates a different acute process warranting further investigation.
P31. Novel SPAST Deletion Mutation in an American Family with Hereditary Spastic Paraplegia: A Case Report
Sydney B. Bhopatkar2, Juebin Huang1
1. Department of Neurology, University of Mississippi Medical Center, Jackson, MS, United States.
2. School of Medicine, University of Mississippi Medical Center, Jackson, MS, United States.
Background: The diverse group of neurodegenerative disorders known as Hereditary Spastic Paraplegia (HSP) is characterized by spasticity and weakness of the bilateral lower extremity due to degeneration of the corticospinal tract. The most common subtype of HSP is HSP type 4 (HSP-SPG4), a result of mutations in the SPAST gene (Chr 2p22.3) that leads to impaired activity of the microtubule-severing protein spastin. Typically presenting as an uncomplicated, autosomal dominant (AD) form of the disease, HSP-SPG4 has been documented worldwide with vast genomic variance across the SPAST gene.
History: A 66-year-old man with a prior diagnosis of ankylosing spondylitis was referred to the neurology clinic with a chief complaint of jerking movements in both legs. The patient described difficulties with walking and coordination since childhood, resulting in him being wheelchair-bound for 20 years. Family history was significant for similar lower extremity weakness and walking difficulties in his father (deceased), son, daughter, and affected daughter’s son.
Upon neurological examination, his mental status, cranial nerves, and sensory exam were grossly normal. Motor exam revealed muscle strengths were 5/5 in bilateral upper extremities and 3/5 in bilateral lower extremities. Muscle tone was normal in bilateral upper extremities, but severe spasticity was noted in bilateral lower extremities. Deep tendon reflexes were 2+ in bilateral upper extremities. Patellar reflex was 4+ bilaterally, and ankle reflex was 2+ bilaterally. There was persistent bilateral ankle clonus. Babinski signs were positive bilaterally. Myoclonic jerking movement was noted in bilateral lower extremities upon standing with assistance. Given the significant family history of similar presentations, HSP was suspected.
Genetic Testing: A Hereditary Spastic Paraplegia Comprehensive genetic analysis panel obtained for the patient and his daughter reported a heterozygous 26.1 kb deletion within the SPAST gene, which was believed to be pathogenic. This deletion includes exon 4 to 7, with breakpoints in introns 3 and 7. Combined with the significant family history, the patient and his daughter were subsequently diagnosed with pure, AD HSP-SPG4.
Discussion: We report a novel pathogenic deletion mutation of SPAST gene in a family with AD HSP-SPG4 phenotype. Although single and multiple exon deletions of SPAST gene are a well-known cause of HSP-SPG4, to our knowledge, this exact 26.1 kb deletion has never been reported in the literature. Our case had a prolonged history of lower extremity weakness and spasticity with a strong family history of similar presentation across four generations. However, he went undiagnosed until age 66 with severe disability. Such a delay can likely be attributed to lack of access to healthcare and lack of awareness of rare hereditary diseases such as HSP in general health care providers.
P32. Effective Management of Toxic Metabolic Encephalopathy Induced by Pembrolizumab (Keytruda): A Successful Intervention with Dexamethasone (Case Report)
1. Osteopathic Medicine, Nova Southeastern University Dr. Kiran C Patel College of Osteopathic Medicine, Davie, FL, United States.
2. Internal Medicine Residency, Naples Comprehensive Healthcare, Naples, FL, United States.
Pembrolizumab, an immune checkpoint inhibitor (ICI) and Anti-PD-1 Monoclonal Antibody, has revolutionized the management of non-small cell lung cancer (NSCLC). Although it has a significant improvement in cancer prognosis, it is associated with widespread immune mediated adverse effects (imAE). Here we present a rare case of encephalitis, after Pembrolizumab treatment with successful treatment with high-dose steroids in the face of unpublished guidelines.
Case Report: 65-year-old woman with metastatic NSCLC on Pembrolizumab and chronic hyponatremia, presented to the hospital due to worsening hyponatremia (Na127mmol/L), at oncologist’s request. On admission she was asymptomatic. Clinical presentation was consistent with euvolemic hyponatremia. Initial testing supported SIADH. The night after admission she experienced a 102.9F fever. In the morning the patient was noted to be confused, oriented only to person. CT and MRI of brain were unremarkable, drawing suspicion of infection. Broad spectrum antibiotics were initiated, but the patient continued to decline. Day two the patient was unable to follow commands, had mixed aphasia, and was highly agitated. Serum sodium levels continued to decrease (Na124mmol/L). Due to abnormally low electrolyte levels and large urine output, we suspected pituitary axis dysfunction and started dexamethasone pending testing. After starting steroids, we observed significant improvement in mentation and her sodium improved to 132mmol/L. By day three, the patient was capable of communicating and following commands. The rapid improvement in mentation after dexamethasone raised suspicion for encephalitis/hypophysitis due to Pembrolizumab treatment and less likely due to hyponatremia.
Discussion: This patient’s toxic metabolic encephalopathy with acute cerebral dysfunction was likely due to her metabolic disturbance induced by Pembrolizumab. Despite extensive interventions to address her encephalopathy and hyponatremia, the patient continued to decline rapidly. Only after a dose of dexamethasone did the patient show significant improvement. CNS related imAEs with ICIs, especially with widely used Pembrolizumab, is exceedingly rare. Without a high suspicion for pembrolizumab-induced encephalopathy leading to AMS, a potential treatment pathway may be overlooked. To our knowledge, successful treatment of AMS in Pembrolizumab-induced encephalopathy with high dose steroids has only been reported once in literature. Other cases have shown that delay in care has resulted in irreversible complications and even death. This case highlights the significance of having imAE as part of the differential diagnosis of encephalopathy in patients that are being treated with Pembrolizumab and other ICIs. Furthermore the success in our treatment regimen is a valuable contribution in how to approach ICIs and Pembrolizumab related encephalopathies, opening the doors for further research in creating appropriate treatment guidelines.
P33. The Weight Loss Enigma: Balancing New Drugs with Mental Health Risks
Bryan Mortimer1, Tarak Vasavada1, 2, 3
1. UAB Heersink School of Medicine, Birmingham, AL, United States.
2. Psychiatry, Huntsville Hospital, Huntsville, AL, United States.
3. President, Indo-American Psychiatric Association, Huntsville, AL, United States.
Case Presentation: A 68-year-old female patient presented to the ER with sudden onset SI and depression. She had a history of MDD, anxiety, HTN, DM type 2, and insomnia. Four weeks prior to admission, the patient stated that she started experiencing sudden onset in extreme feelings of helplessness, hopelessness, and anxiety. She said that “this is the most depressed I have ever been, more so than when my husband died two years ago”. She rated her depression as a 9/10. The only recent change in the patient’s life was a medication dose change about four weeks ago. Her weekly subcutaneous Ozempic dose had been doubled from 0.5mg to 1mg. The patient stated that this increase was because of her desire to lose weight. Patient has had no prior psychiatric admissions or suicide attempts. Her psychiatric conditions have been well-controlled for years on Cymbalta, Buspar, and PRN Restoril. Patient has good social support between her neighborhood community and children. She has no new stressors in her life. Within her four-day psychiatric hospitalization, the patient reported complete resolution of SI and symptoms. On discharge, we advised the patient to continue taking her weekly 1 mg Ozempic but to follow up with her prescribing physician to address potentially backing down on the dosage.
Discussion: Suicide was the 12th overall cause of death for the year 2020 in the US. Most mental disorders and symptoms such as helplessness, depression, and impulsivity can predict ideation. It is important to also assess for other factors such as new stressors or changes in medications. GLP-1 agonists like semaglutide (Wegovy and Ozempic) are rising in popularity not only for treatment of diabetes mellitus but also to induce weight loss. Depression is highly comorbid with obesity. Currently, suicidal behavior and ideation are listed as the last “precaution” only for Wegovy and not for Ozempic. History of depression or other mental health disorders are not currently listed as precautions or contraindications to starting these widely popular GLP-1 agonists.
Conclusion: GLP-1 receptors are present all over the body and the production of GLP-1 happens even within the brain (the nucleus tractus solitarius) and are released as neurotransmitters. These receptors are thought to be participating in processes such as addiction and reward circuitry. Mouse studies revealed that several GLP-1 agonists can cross the blood brain barrier (BBB) from systemic circulation. More work needs to be done to elucidate the extent to which all GLP-1 agonists are interacting with the CNS. This is even more important due to the rise in the usage of Wegovy and Ozempic for not only diabetes treatment but for everyday weight loss.
P34. An Orange a Day May Keep the Doctor Away
Elisabeth Holbert1, Chloe Carroll1, Jayci Avery1, Kelli R. Stringer1
1. The UAB Heersink School of Medicine, Birmingham, AL, United States.
Introduction: Scurvy, pathologic deficiency of Vitamin C, leads to impaired collagen synthesis. This connective tissue damage may appear as gingivitis, petechiae, poor wound healing, follicular hyperkeratosis, “corkscrew” hairs, fatigue, and lethargy. Due to its perception as a historical diagnosis, delay can exist from time of symptom onset to diagnosis.
History: A 7 year old male with a medical history of nonverbal autism presented for 6 week history of non weight bearing on bilateral lower extremities and unexplained weight loss. The patient fell 5 weeks prior to presentation, no other trauma was noted. Sedated MRI revealed multifocal metaphyseal marrow signal abnormalities in both lower extremities with areas of adjacent myositis, consistent with scurvy or other infiltrative diseases.
Physical Exam and Labs: After imaging, bleeding of the patient’s oral mucosal was noted, as well as lower and upper extremity petechiae, gingival hyperplasia of maxillary and mandibular gum lines and a left lateral ankle ecchymosis. Patient was hemodynamically stable with mild tachycardia. Range of motion was limited due to significant leg pain. Patient was noted to have AKI with initial creatinine of 0.7, up from his baseline of 0.3 as well as an anion gap acidosis with an anion gap of 19, likely due to dehydration. He was mildly anemic with a Hgb of 10.5 and MCV of 76.8; CBC was otherwise unremarkable. Further investigation revealed the patient’s diet consisted of 5 foods including peanut butter sandwiches, graham crackers, breakfast sausage, strawberry granola bars, chocolate cookies and water. Hematology was consulted and eventually ruled out malignancy, the primary pediatrics team focused on pain management, fluid and nutritional supplementation, including 100 mg vitamin C IV for 7 days. Physical therapy worked to encourage ambulation. Clinically, the patient improved. His creatinine improved to 0.2.
Final Diagnosis: Vitamin C level resulted <0.1 μmol/L which confirmed the diagnosis of scurvy. Patient was discharged on 100 mg oral ascorbic acid three times daily, as well as Vitamin D, iron polysaccharide, and plan for close follow with outpatient physical therapy.
Discussion: Scurvy persists in vulnerable populations, including children with autism spectrum disorder (ASD) who often have strong food sensitivities. Familiarity with presentation of scurvy may avoid time consuming or painful testing prior to establishing diagnosis. In our patient, hematologic and malignant conditions were considered due to radiologic findings. Bone marrow biopsy was considered but was ultimately not conducted. In one systematic review 50% of children with eventual scurvy diagnoses received 3 or more imaging procedures and in 21%, bone marrow biopsy was conducted. In the case of our patient, MRI established his diagnosis due to characteristic findings, though a conclusion may have been drawn at initial presentation due to clinical findings and history of restrictive diet secondary to ASD.
P35. Inhibition of Androgen Synthesis Affects Gene Expression Profile in a Human Male Neuronal Cell Line: Potential Mechanism for Cognitive Deficits with Prostate Cancer Therapy
Allison B. Reiss1, Samantha E. Vasalani1, Ankita Srivastava1, Heather A. Renna1, Aaron E. Katz1
1. NYU Grossman Long Island School of Medicine, Mineola, NY, United States.
Purpose of Study: Lowering testosterone levels is a mainstay treatment for metastatic prostate cancer (PCa), improving progression-free survival. However, inhibiting androgen synthesis has numerous adverse effects, including an impact on cognitive function that can interfere with occupational pursuits and quality of life. Some PCa patients may avoid this treatment due to intolerable neurocognitive symptoms. Abiraterone acetate (AA) is an oral agent that reduces androgen production by blocking the enzyme cytochrome P450 17-α-hydroxylase. This study uses a human male neuroblastoma cell model to document AA-induced alterations in gene expression profile as a possible mechanism of anti-androgen-related cognitive decline.
Methods Used: BE(2)M17 neuroblastoma cells in 10% charcoal stripped fetal bovine serum to avoid extraneous hormones ± dihydrotestosterone pretreatment (DHT, 5nM, 12hr.) were exposed to 0, 5, 10 and 20uM AA (24hr.). RNA and protein were isolated for Real-Time PCR (n=9) and Western blotting (n=3-5) to quantify select genes involved in neuronal health or damage and mitochondrial (Mt) function. Key genes for neuronal function included BDNF (brain-derived neurotrophic factor), important for neuronal plasticity, and amyloid precursor protein (APP), cleaved to form excess amyloid-β in Alzheimer’s disease. Mt genes included Mt transcription factor A (TFAM), a binding protein critical for genome maintenance and low density lipoprotein receptor-related protein 1 (LRP1), which regulates amyloid-β peptide clearance and maintains brain homeostasis.
Summary of Results: Real-Time PCR showed a significant reduction in BDNF mRNA in BE(2)M17 cells exposed to AA alone (P=0.0001 at 5uM, P<0.0001 at 10uM and 20 uM) and in these cells when exposed to both AA + DHT (P=0.0003 at 5uM, P=0.0396 at 10uM, P=0.0001 at 20uM). APP mRNA was significantly reduced when cells were exposed to AA alone (P=0.0451 at 5uM, P=0.0295 at 20uM) and in cells exposed to both AA + DHT (P<0.0001 5uM). Western blot revealed a significant reduction in APP protein in cells exposed to AA alone (P<0.0001 at 10uM and 20uM) or to AA + DHT (P= 0.0067 at 20uM) [See figure]. BE(2)M17 cells showed a significant decrease in TFAM mRNA when incubated with either AA alone (P= 0.0003 at 5uM, P=0.0002 at 10uM, P<0.0001 at 20uM) or AA + DHT (P<0.0001 at 5uM, P<0.0001 at 10uM and 20uM). BE(2)M17 cells showed significantly reduced LRP1 mRNA with either AA alone (P=0.0055 at 20uM) or with AA + DHT (P=0.0002 at 5uM).
Conclusions: These experiments suggest that AA, whether alone or in the presence of DHT, adversely affects expression of BDNF, TFAM, APP, and LRP1, 4 genes vital for neuronal health and Mt function. Taken together, our results reveal that AA could induce cognitive impairment by influencing neuronal and Mt health.
P36. Association between Diabetes and Patient Awareness of Impaired Fecundity in the United States: Insights from NHANES
Caitriona M. Greene1, Lora Kasselman3, Allison B. Reiss2
1. Public Health, University of Rochester, Rochester, NY, United States.
2. Internal Medicine, NYU Grossman School of Medicine, Mineola, NY, United States.
3. Medical Sciences, Hackensack Meridian School of Medicine, Nutley, NJ, United States.
Purpose of Study: It is well-established that diabetes (DM) causes increased likelihood of reproductive health complications, but patients with pre-pregnancy DM may not be informed of these risks. This cross-sectional analysis determines the correlation between patient awareness of impaired fecundity and DM in the USA in order to assess the need for education as a risk reduction strategy.
Methods Used: Data from the National Health and Nutrition Examination Survey (NHANES) from 2017 to 2020 was extracted on a subset of 2,692 respondents out of 15,556. Logistic regression analyses were performed to find the odds ratio (OR) of participants with DM based on self-reporting and available glycohemoglobin (HbA1c) levels answering yes to “Have you ever attempted to become pregnant for at least a year without becoming pregnant?” or “Have you ever been to a doctor or other medical provider because you have been unable to become pregnant?”. Confounding variables considered include race and ethnicity, education level, family income-to-poverty ratio, body mass index, and hip-to-waist ratio, with age below 44 years.
Summary of Results: Patients self-reporting a DM diagnosis had a significantly increased risk of visiting a medical practitioner for impaired fecundity (OR=2.595, 95% CI: [1.028, 6.548], p = 0.045) and showed a trend for impaired fecundity (OR=1.969, 95% CI: [0.857, 4.523], p = 0.093). Patients at pre-clinical risk of DM based on their HbA1c also showed a trend for impaired fecundity and seeing a medical practitioner for impaired fecundity (OR = 1.916, 95% CI: [0.846, 4.341], p = 0.10 and OR = 1.554, 95% CI: 0.897, 2.690], p = 0.10, respectively). There was no association with visiting a physician for impaired fecundity among patients at clinical risk of DM based on HbA1c.
Conclusions: Self-reported DM is associated with self-reporting seeing a medical practitioner for impaired fecundity, and trends towards increased risk for self-reporting fertility issues. This may indicate that patients aware of their DM are also aware of associated fertility problems and the importance of seeking help for DM-related reproductive issues. Pre-clinical DM based on HbA1c also trends towards an increased risk for self-reporting fertility issues and self-reporting seeing a medical practitioner for impaired fecundity. This group may contain both respondents with medically managed DM and those who have not progressed to DM. A relationship exists between self-report of having DM and knowing that DM may compromise fertility. Among those who do not self-report DM but have unmanaged HbA1c indicating clinical risk for DM, there is a lack of supporting evidence of reporting on the fertility issues associated with DM. Considering DM often progresses during pregnancy, expanding DM education to pre-clinical patients and patients with high HbA1c is important in people of child-bearing age.
Self-reported diagnosis of diabetes is associated with significant increase in likelihood of seeing a medical professional for impaired fecundity
P37. Two Decades of Untreated Rheumatoid Arthritis: A Case Report Revealing Long-Term Complications
Azeem Rathore1, Victoria Cuello2, Nadim Qadir1, Ikwinder Preet Kaur3, Mint Thway3
1. Internal Medicine, University of Florida Health Science Center, Jacksonville, FL, United States.
2. University of Texas Rio Grande Valley School of Medicine, Edinburg, TX, United States.
3. Rheumatology, University of Florida Health Science Center, Jacksonville, FL, United States.
Background: Rheumatoid arthritis (RA) is an autoimmune condition defined by joint inflammation, predominantly afflicting women and peaking in middle age. RA patients confront an elevated risk of complications, including interstitial lung disease (ILD), coronary artery disease, heart failure, vasculitis, carpal tunnel syndrome, lymphomas, and cervical spine instability such as fractures. Early initiation of disease-modifying antirheumatic drugs (DMARDs) is pivotal for optimizing long-term outcomes and decreasing such complications.
Case Presentation: A sixty-year-old woman with a medical history of longstanding seropositive RA, ILD, a 45-pack-year tobacco history, and a period of homelessness, presented to the hospital with worsening dyspnea and worsening joint pains for the past few days. She was recently discharged from another hospital for respiratory distress suspected secondary due to untreated ILD. She has previously declined steroids, hydroxychloroquine, methotrexate, or antifibrotic therapy for her ILD, citing varied concerns about side effects. Further, she also was previously treated with TNF-α inhibitors (etanercept and adalimumab) from 2012 to 2015 but declined further infusions due to worsening symptoms. Instead, she relies exclusively on NSAIDs and narcotics for pain relief. Over the last six months, she experienced unintentional weight loss and was advised to undergo a leukemia workup, which she also neglected. Laboratory findings included elevated CRP and ESR with leukocytosis. Imaging included a C-spine MRI that revealed extensive erosion of the odontoid process with severe erosion at the right atlantooccipital joint and a high-resolution Chest CT (HRCT) demonstrating further progression of her ILD with a usual interstitial pneumonia (UIP) pattern (Figure 1). Despite a single dose of methylprednisolone, she refused further steroid therapy. Echocardiogram findings also revealed septal flattening suggestive of right ventricular volume overload, a right ventricular thrombus, and an ejection fraction of 40-45%. Diuretics were initiated, however, despite patient education, she refused continued therapy, only accepting supplemental oxygen. Palliative care was consulted for placement to a rehabilitation center and further palliative care coordination.
Conclusion: Untreated RA poses significant morbidity and mortality risks. Our patient’s case underscores the dangers associated with untreated RA, compounded by socioeconomic and psychological factors. Her medication refusal emphasizes the necessity of patient education and involvement in treatment decisions as the patient developed fixed delusions of certain medication side effects. Early recognition and treatment of RA are pivotal in mitigating its multi-systemic impact such as musculoskeletal, pulmonary, and cardiac impairments. Healthcare providers must adeptly communicate treatment benefits, considering patients’ unique circumstances and concerns.
(left) C-spine MRI: Severe erosion of the odontoid process, severe erosion and remodeling along the right atlantooccipital joint, and soft tissue thickening compatible with pannus; (right) HRCT: bilateral subpleural honeycombing and reticulation consistent with UIP pattern
P38. Help, I Can’t Breathe: A Rare Case of Isolated Cricoarytenoid Joint Stenosis in Rheumatoid Arthritis
Kollin Kahler1, Dr. Hanan Ibrahim2
1. Internal Medicine, University of Mississippi Medical Center, Jackson, MS, United States.
2. Rheumatology, University of Mississippi Medical Center, Jackson, MS, United States.
Introduction: Rheumatoid arthritis (RA) is a systemic inflammatory disease that affects joints lined by a synovial membrane. The cricoarytenoid (CA) joint, which controls the vocal cords, is diarthrodial and lined by a synovial membrane. RA of the CA joints is found in a minority of patients. In the acute phase, patients can complain of hoarseness, dysphonia, or dysphagia. Chronic RA of the CA joints can lead to their fixation. A review of 218 cases with immobility of both vocal folds revealed CA fixation secondary to RA in 6.3% of the cases. Direct visualization through laryngoscopy is needed. We present a rare case of isolated fused CA joints in a patient with newly diagnosed RA.
History and Clinical Course: An 82-year-old male with a history of bilateral neck adenopathy was referred to Rheumatology by Otolaryngology (ENT) due to recurrent supraglottic edema (status post tracheostomy tube) with concerns for an autoimmune etiology. Prior to the tracheostomy, the patient reported worsening dysphagia, voice changes, and progressive stridor. He denied a personal or family history of rheumatological pathologies. Initial lab work-up at the time was unremarkable- Antinuclear Antibody, Ribonucleoprotein Ab, and anti-dsDNA Ab negative. Chitotriosidase levels were mildly elevated (keeping sarcoidosis on the differential). Chest and hand X-rays were unremarkable. On repeat laryngoscopy with ENT, newly identified fixed cricoarytenoid joints were visualized. With concerns for RA, new labs revealed a positive Rheumatoid Factor (31.8). A supraglottic tissue biopsy was also obtained which revealed chronic inflammation without any granulomas or cancerous findings. IL-6 inhibition with Sarilumab was initiated and resulted in minimal improvement, thus the patient transitioned to tumor necrosis factor (TNF) blockade with Adalimumab. Since transitioning, the patient reports improvement in overall symptoms- improved fatigue, less laryngeal secretions, and improvement with voice. A follow-up with ENT is scheduled for evaluation of tracheostomy tube removal.
Physical Exam Pertinent Findings: HEENT: tracheostomy tube in place, soft tissue swelling around the neck
Respiratory: coarse upper airway sounds
Musculoskeletal: Heberden and Bouchard nodes on the right hand
Discussion: This rare RA case of isolated CA fixation emphasizes the importance of a multidisciplinary approach when treating patients with complex autoimmune conditions. Initially, elevated Chitotriosidase levels suggested sarcoidosis. Subsequent lab and pathology results ruled out sarcoidosis as a cause. The elevated RF levels alone are not an exclusive enough finding to diagnose RA, but this highlights the importance of the direct visualization by ENT of the fixed CA joints. This case spotlights that isolated CA joint fusion, although exceptionally rare, can be the sole presentation of RA. With symptom improvement on TNF blockade, tracheostomy tube removal is a possibility.
Initial Laryngoscopy
P39. Acid-Secreting Inlet Patch: An Atypical Cause of Esophageal Strictures
Amira Elgogary1, William Provance1
1. NCH Healthcare System, Naples, FL, United States.
Case Presentation: A 78-year-old female presented to the emergency department with a chief complaint of a foreign body sensation in her throat. She was having a salad the night before which became impacted. She tried to relieve her symptoms by drinking but regurgitated. She experienced similar episodes previously. This has only occurred with solids and never with liquids. She denied odynophagia, hematochezia, melena, early satiety, and weight loss. She has a history of osteoporosis and a family history of lung cancer. She reported occasional alcohol use but denied tobacco use. Vital signs were stable. Physical examination was unremarkable, without abdominal tenderness. Laboratory data, including a complete blood count and metabolic panel, was normal. Upper endoscopy was performed, food content was not identified in the esophagus; however, a circumferential salmon-colored mucosa was detected in the upper esophagus at 16-18 cm from the incisors in addition to a benign-appearing, intrinsic moderate stricture found at 18cm. The stricture measured 1.2cm (inner diameter) x less than one cm (in length) (Figure 1). The remainder of the esophagus appeared normal; no masses or pouching were identified. Cold forceps biopsies for histology were obtained. Gentle stricture dilation was performed to 51 Fr. with a Savary dilator with evidence of mucosal disruption after dilation (Figure 2). After endoscopy, proton pump inhibitor therapy was initiated. The pathology report was consistent with a gastric inlet patch, revealing gastric heterotopia adjacent to the normal esophageal mucosa. There was no intestinal dysplasia and no evidence of eosinophilic esophagitis. Gastric antral biopsies were negative for Helicobacter pylori infection. On follow-up evaluation, the patient denied recurrence of her symptoms.
Discussion: Gastric inlet patches are ectopic gastric tissue found in the upper third of the esophagus. Although typically asymptomatic, they have been implicated in various complications, including esophageal strictures and webs. The genesis of these complications is thought to be due to acid secretion from ectopic parietal cells present within the aberrant mucosa. Under conventional white light endoscopy, they appear as salmon-hued, velvety mucosal regions adjacent to the esophagus’s red squamous epithelium. This subtle contrast contributes to their frequent oversight; their detection might be further compromised by the tendency of endoscopists not to thoroughly inspect the cervical esophagus during the scope withdrawal. Currently, there are no standardized protocols for the management and follow-up of esophageal inlet patches, mainly due to their underdiagnosis and varying presentations resulting in the lack of substantial clinical data and comprehensive statistical analyses. This case underscores the pressing need for dedicated research aimed at enhancing the endoscopic detection of inlet patches to mitigate the risk of unfavorable potential complications.
Upper third of the esophagus: Gastric inlet patch and stricture.
Upper third of the esophagus: Mucosal disruption after dilation.
P40. Diagnostic Modalities for Early Anastomotic Leak Detection After Colorectal Surgery
Halley Yung1, Alisha K. Daroch1, Rooshi Parikh1, Dharam Mathur1, Ide Kafexhiu1, Elliot Goodman1
1. CUNY School of Medicine, New York, NY, United States.
Purpose of Study: Anastomotic leak remains a severe complication following colorectal surgery, leading to increased morbidity and mortality, particularly in cases of delayed diagnosis. Existing diagnostic methods, including CT scans, contrast enemas, endoscopic examinations, and reoperations can confirm anastomotic leak but lack strong predictive value. Early detection is crucial for improving patient outcomes, yet a definitive and reliable predictive test, or “gold standard,” is still lacking.
Methods Used: A comprehensive PubMed review was focused on CT imaging, serum levels of C-reactive protein (CRP), and procalcitonin (PCT) to assess their predictive utility in detecting anastomotic leak after colorectal resection. Three independent reviewers evaluated eligibility, extracted data, and assessed the methodological quality of the studies. A total of 21 studies aligned with the inclusion criteria (10 prospective observational, 8 retrospective analyses, 3 meta-analysis) that investigate CRP as a biomarker in the detection of AL. Similarly, a total of 12 studies were selected to examine the relationship between PCT and AL occurrence (9 prospective observational, 2 meta-analyses, and 1 retrospective analysis).
Summary of Results: The reported cut-off values for CRP ranged from 77 to 180 mg/L from post-operative days (PODs) 3 to 6. The area under the receiver operating curve (AUROC) ranged from 0.709 to 0.956, with the highest AUROC on POD 4. For PCT, cut-off values ranged from 0.0065 ng/mL to 4.93 ng/mL from POD 3 to 9. AUROC values ranged from 0.61 to 0.947 with the highest value being reported on POD 3. Our analysis revealed the effectiveness of both CRP and PCT in anastomotic leak detection during the early postoperative period. CT imaging, capable of identifying fluid collection, pneumoperitoneum, extraluminal contrast extravasation, abscess formation, and other early signs of leak, also proved valuable.
Conclusions: Considering the variability in findings and statistics across these modalities, our study suggests a personalized, multimodal approach to predicting anastomotic leak. Integrating CRP and PCT assessments with the diagnostic capabilities of CT imaging provides a nuanced, patient-specific strategy that significantly enhances early detection and management. By tailoring interventions based on individual clinical characteristics, surgeons can optimize patient outcomes, reduce morbidity, and mitigate the consequences associated with anastomotic leak after colorectal surgery. This approach emphasizes the importance of personalized medicine in surgical care, paving the way for improved patient health outcomes.
American Federation for Medical Research 2024 Southeastern Award Recipients
Frank Adusei Poku
Meharry Medical College, Nashville, TN
Adult-onset Kawasaki Disease: An Updated Review of the English-Language Literature from 1980 through 2023
Mohammed Ahsan
NCH Healthcare System, Naples, FL
Is Computer-aided Detection Technology Effective in Mitigating Physician Fatigue Among Experienced Endoscopists in the Community Setting?
Kabeer Ali
University of Florida College of Medicine Jacksonville, Jacksonville, FL
Take My Breath Away: Hydropneumothorax as an Initial Presentation of Malignancy
Shane Clark
Duke University School of Medicine, Durham, NC
New-onset Jaundice in 13-Day OldBaby with Trisomy 21
Christopher Fiechter
University of Central Florida, Orlando, FL
Exploring the Neurologic Impact of Licorice-induced Hypertensive Encephalopathy: Emphasizing the Critical Role of Timely Intervention
Kylie Krohmaly
The George Washington University, Washington, DC
Bacterial Small RNAs May Mediate Immune Response Differences Seen in Respiratory Syncytial Virus versus Rhinovirus Bronchiolitis
Azeem Rathore
University of Florida Health Science Center, Jacksonville, FL
Evaluating Atrial Fibrillation-Related Content on TikTok: A Social Media Analysis
Bi Zhang
NYU Grossman Long Island School of Medicine, Mineola, NY
Modeling Nilotinib in the Treatment of Alzheimer’s Disease in Cell Culture: Evaluation of a Repurposed Drug