
Abstract
Immunotherapy with checkpoint inhibitors has improved the outcomes of patients with metastatic lung cancer in recent years. Despite improved prognosis, not all patients respond to treatment. Therapeutic interventions to build on the success of immune checkpoint inhibitors are needed. A retrospective review of patient records for patients who had received immune checkpoint inhibitors in a single cancer center over 4 years was undertaken. Demographic and disease characteristics of patients with metastatic non-small cell lung cancer were recorded. Data on other treatments including chemotherapy and radiation therapy were extracted, and survival outcomes were calculated. Most (81.8%) of the 77 metastatic lung cancer patients examined had received palliative radiation therapy within 3 months of starting immune checkpoint inhibitors. While the survival outcomes of these patients did not differ from patients who had not received radiotherapy, patients who had undergone hypofractionated radiotherapy (defined as one or more fractions of 700 cGy or higher) displayed a better overall survival (OS) than the rest of the cohort. Palliative radiation therapy administered in proximity with immune checkpoint inhibitors immunotherapy had no effect on the OS of metastatic lung cancer patients. However, patients receiving palliative radiotherapy with fractions above 700 cGy showed better OS. Further studies are needed to optimize a combination strategy.
Introduction
Immune checkpoint inhibitors are a new class of anticancer treatments introduced in the last decade and moved to the first-line treatment of some metastatic cancers as well as later-line treatment of several others. 1 These novel anticancer drugs are currently approved for the treatment of a broad array of cancers, and their indications are quickly expanding—they have even shown clinical benefit in the adjuvant or neoadjuvant setting in several types of cancers.2–4 Their effectiveness with or without chemotherapy has improved the outcomes of many cancers, such as metastatic melanoma and lung carcinomas, prolonging survival by several months.5–7 In other cancers, including cancers where chemotherapy has been minimally effective or ineffective, such as renal cell carcinoma, the introduction of immune checkpoint inhibitors has improved results for the first time in decades. 8 Most impressively, a significant minority of metastatic cancer patients treated with immune checkpoint inhibitors obtain long-term disease control, extending significantly their survival and suggesting that some patients may even be cured. 9 Locally advanced or metastatic non-small cell lung cancer patients treated with pembrolizumab had a 3 year survival of 26.4% (95% confidence interval: 14.3%–40.1%) in the first-line setting and a 3 year survival of 19% (95% confidence interval: 15%–23.4%) in later lines. 10 Nivolumab was more effective than chemotherapy with docetaxel in the second line setting of both metastatic adenocarcinomas and squamous non-small cell lung cancers.11,12 The immune checkpoint inhibitor prolonged the median overall survival (OS) of patients with non-squamous non-small cell lung cancer to 12.2 months from 9.2 months that was the median survival with docetaxel (hazard ratio 0.73, 95% confidence interval: 0.59–0.89, p = 0.002). 11 Similarly, patients with squamous lung cancers had a median OS of 9.2 months with nivolumab vs 6 months with docetaxel (hazard ratio 0.59, 95% confidence interval: 0.44–0.79, p < 0.001). 12
Several immune checkpoint inhibitors are currently approved for use in various cancer types and are all monoclonal antibodies targeting the inhibitory cell surface receptor CTLA-4 (Cytotoxic T Lymphocyte Antigen 4) or the PD-1 (Programmed cell Death 1)/PD-L1 (Programmed cell Death Ligand 1) pair of immune blockade molecules. Two CTLA-4 inhibitors, ipilimumab and tremelimumab, are currently in clinical use. Inhibitors of the PD-1/PD-L1 pair include pembrolizumab, nivolumab, durvalumab, atezolizumab, dostarlimab, avelumab, and cemiplimab. 13 From a mechanism perspective, immune checkpoint inhibitors invigorate the cytotoxic activity of immune cells (Cytotoxic T lymphocytes and NK cells) against tumor cells by neutralizing inhibitory immune interactions between ligands expressed by tumor cells and antigen-presenting cells and receptors expressed by cytotoxic cells. Interference with negative signals allows for positive signals derived from antigens presented in the context of Major Histocompatibility Complex (MHC) molecules, in conjunction with co-stimulatory signals, to activate the immune response. 14
Radiation therapy is often used in metastatic cancers to treat the disease in locations that threaten vital organs such as the spinal cord or to palliate intractable symptoms such as pain or bleeding. Radiation treatments used in the palliative/metastatic setting are frequently shorter than definitive or adjuvant treatments. Single fractionation treatments constitute an attractive option in the palliation of bone metastases due to their efficacy, convenience for the patient and the treatment unit, and cost-effectiveness.15,16 For painful skeletal metastases, single doses of 8 Gy are frequently used, based on their ability to provide prompt pain relief, higher response rates, and decrease in skeletal events such as pathologic fractures, compared with lower doses. 17 The utilization of single doses or reduced numbers of fractions has increased over the last several years, especially in academic centers and for older patients. 16
A putative synergy between radiation and the immune system has been postulated with the recognition of systemic effects of radiation. 18 Besides the local tumoricidal effect that occurs within the field applied, radiation therapy may have a systemic anticancer effect that affects metastatic cancer localizations outside the radiation field. This phenomenon is termed the abscopal (off-target) effect. 19 This systemic benefit is produced by stimulation of the systemic immune response to the tumor inflammatory microenvironment created by irradiated cells. 20 Besides a direct tumoricidal effect, radiation promotes the release of double-strand DNA (dsDNA) chains in the cytoplasm of irradiated cells. 21 dsDNA in the cytoplasm activates the enzyme cGAS (cGMP-AMP synthase), a protein that synthesizes cyclic GMP-AMP (cGAMP) dinucleotide. cGAS activation is dependent on the length of dsDNA but independent of the specific sequence. cGAMP and other dinucleotides activate the protein Stimulator of Interferon Response (STING), which then activates kinase TANK Binding Kinase 1(TBK1) in the Golgi apparatus. 22 The complex of STING and TBK1 recruits and phosphorylates transcription factor IRF3, leading to its activation. Activated IRF3, as well as activated NF-κB, induce the production of type I interferons (type I IFNs). 23 Interferon γ and NF-κB were both induced by ionizing irradiation in a model of fibrosarcoma cells, in contrast to another key immune regulating transcription factor, STAT1, which was not up-regulated by irradiation exposure in this model. 24 Type I IFNs act in an autocrine and paracrine manner to promote the inflammatory environment that may result in an antitumor response, provided that additional permissive conditions are fulfilled. These conditions include a functional tumor antigen presentation machinery in the cancer cells and the absence of inhibitory signals that would hamper incoming immune effectors’ cytotoxicity.25,26 Antigen presentation relies on the production of antigens by processing proteins in the immunoproteasome. The immunoproteasome is a specialized form of proteasome that utilizes dedicated alternative enzymatic units, different from the enzymatic units of the typical proteasomes, to produce peptide fragments appropriate for presentation in the context of MHC. 27 One of these sub-units, PSMB8, also called LMP7 or β5i, is induced by irradiation exposure in radiation-sensitive but not radiation-resistant cancer cells. 24
Given these considerations, the current study investigates the effect of palliative irradiation in patients with metastatic lung cancers treated with immune checkpoint inhibitors. It also explores radiation parameters as predictors of survival in this scenario.
Radiation therapy is often given for palliation of metastatic lung cancer patients.
Immunotherapy with immune checkpoint inhibitors has become one of the main treatment modalities for the disease.
Patients often receive these treatments concomitantly or in close proximity.
Delivery of palliative radiotherapy in patients receiving immune checkpoint inhibitors does not alter the Overall Survival of metastatic lung cancer patients.
The current retrospective analysis suggests that a systemic benefit of hypofractionated radiotherapy in combination with immune checkpoint inhibitors may be present in metastatic lung cancer patients.
The potential beneficial effect included the use of various PD-1 immune checkpoint inhibitors.
Future prospective studies with hypofractionated radiotherapy combined with immune checkpoint inhibitors are warranted.
Methods
A retrospective review of medical records to identify patients who had received immune checkpoint inhibitors with or without radiation for the treatment of metastatic cancers in a single cancer center over a 4-year period was performed. All patients with metastatic non-small cell lung cancers were included in the study and followed for survival. OS outcomes were extracted from records. Patients with cancers other than non-small cell lung cancer, patients with non-metastatic disease, or with incomplete data were excluded.
Demographic data (age, gender, smoking habits, and Eastern Co-operative Oncology Group Performance Status) and data on the histologic characteristics of tumors, stage, tumor markers, and molecular characteristics were captured from patient medical records. Data on radiation schedules, dose, number of sessions, and the organ irradiated were also extracted from the medical records. The timing of immune inhibitors in relation to radiation was also recorded.
OS was defined as the interval from the start date of immunotherapy treatment to death. Survival plots of patients treated with combined radiation and immune checkpoint inhibitors and those who received only immunotherapy were constructed using the Kaplan–Meier method. OS of the groups was compared using the LogRank test. The χ2 test or Fisher’s exact test was used to evaluate differences in clinical and biologic characteristics of the groups. All resulting p-values were considered to be significant at the level of p < 0.05.
The protocol of this study was approved by the Ethics Institutional Review Board of the Sault Area Hospital, Sault Ste Marie, ON, Canada.
Results
A total of 173 patients with metastatic cancer who had received immune checkpoint inhibitors were identified. Among these, 77 patients had lung cancers and were included in the study, while the remaining 96 patients had other cancer diagnoses and were excluded. Lung cancer patients had a mean age of 67.3 years old (±10.8), 62.3% were older than 65 years old, and 50.6% were male (Table 1). Although most patients (67.5%) were not smokers at the time of their diagnosis, 89.6% were ex-smokers. Most patients (83.1%) had an Eastern Co-operative Group Performance Status (ECOG PS) of 0 or 1, and about two-thirds (66.2%) had significant cardiovascular (coronary artery disease, myocardial infarction, congestive heart failure, or peripheral vascular disease) or cerebrovascular (stroke) comorbidities. All patients with adenocarcinoma were negative for EGFR mutations, ROS1 rearrangements, and ALK rearrangements. Other common alterations, including KRAS, BRAF, and MET mutations, were not assayed as part of the genomic profiling. No patients in the cohort had received therapy with targeted inhibitors.
Characteristics of metastatic lung cancer patients of the cohort and according to whether they had received hypofractionated radiotherapy (RTx fractions ≥700 cGy). One patient who received pembrolizumab received also tremelimumab. The irradiated site refers to the location of the radiation treatment most close to the treatment with immunotherapy.

Fifty of the seventy-seven patients (64.9%) had received chemotherapy during the course of their metastatic disease. Sixty-three patients (81.8%) received radiation treatment within three months of the start of immunotherapy in various total doses, fractionations, and body locations, while 14 patients had not received radiation. OS was not significantly different in patients who had received radiotherapy compared with patients who had not received radiation (Log Rank p = 0.8, Figure 1). Thirty-four patients had received radiation within 30 days from the start of immunotherapy, and their OS did not differ from the OS of patients who were treated starting beyond 30 days from the start of immunotherapy (Log Rank p = 0.2).

Overall survival of patients with metastatic non-small cell lung cancer receiving immune checkpoint inhibitors according to whether they have received radiation therapy. The solid line curve represents the group without radiation therapy (n = 14) and the split line curve represents patients who had received radiation therapy (n = 63). Log Rank test p = 0.8.
Eight of the 63 patients who received radiation were treated with hypofractionated radiation consisting of fractions higher than 700 cGy. These patients did not differ significantly from the remaining 69 patients in the series regarding gender, age, smoking habits, tumor histology, ECOG PS, and cardiovascular or cerebrovascular comorbidities (Table 1). The most frequent target sites of hypofractionated radiotherapy were the lung in three patients, bones in two patients, and the brain, pleura, and intra-abdominal sites (adrenal) in one patient each (Table 2). Patients who received hypofractionated radiotherapy had more frequently received two lines of previous systemic therapies (37.5%) than patients in the group of non-hypofractionated radiotherapy or no radiotherapy (15.9%); however, this difference was not statistically significant (χ2 p = 0.24). The most frequently used immune checkpoint inhibitor in the cohort was pembrolizumab, followed by durvalumab, nivolumab, and atezolizumab. The OS of patients who received hypofractionated radiotherapy in combination with immunotherapy was better than that of the rest of the cohort who did not receive radiotherapy or received radiation with fractions lower than 700 cGy (Log Rank p = 0.04, Figure 2).
Characteristics and outcomes of the eight patients who received hypofractionated radiation therapy with immunotherapy.
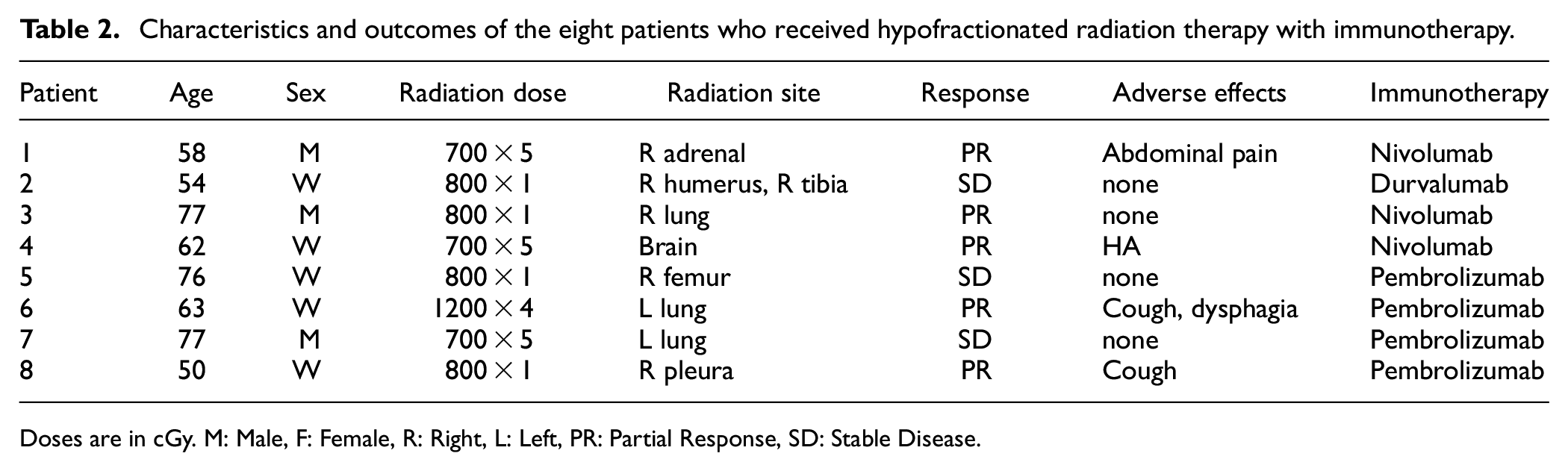
Doses are in cGy. M: Male, F: Female, R: Right, L: Left, PR: Partial Response, SD: Stable Disease.

Overall survival of patients with metastatic non-small cell lung cancer receiving immune checkpoint inhibitors according to whether they have received hypofractionated radiation therapy. The solid line curve represents the group without radiation therapy or with non-hypofractionated radiation therapy (n = 69) and the split line curve represents patients who had received hypofractionated radiation therapy (n = 8). Log Rank test p = 0.04.
Discussion
During the last several years, the introduction of immunotherapy in the form of monoclonal antibodies blocking inhibitory immune receptors has revolutionized cancer therapy and the field of clinical oncology. 28 These drugs activate the immune system to attack cancer cells. 28 The strategy of using the patient’s own immune system to combat the tumor has provided remarkable results in certain cancers, although it has been less successful in others.2–5 In non-small cell lung cancer, immunotherapy has become a standard treatment in the adjuvant setting for both adenocarcinomas and cancers with squamous histology. 29 Similarly, in the metastatic setting, immune checkpoint inhibitors are commonly included in the treatment of lung cancer patients either alone or in combination with chemotherapy. 29 On the other hand, radiation therapy is also frequently used for the palliative treatment of metastatic lung cancer lesions that are either symptomatic or refractory to systemic therapy. Thus, a significant percentage of metastatic lung cancer patients receive both immune checkpoint inhibitors and palliative radiation, often in close time proximity to each other.
The systemic antineoplastic effect of radiation treatment for tumor locations that have not been irradiated, termed the abscopal effect, suggests that exposure of a patient to radiation may have a salutary effect for controlling cancers beyond the benefit of local control.20,30 This systemic effect has been proposed to be mediated by local modulation of the immune system by radiation through the activation of immune cells, which then travel to other tumor locations and contribute to tumor control in these locations that have not been irradiated. 20 The sum of the antitumor effect in several locations may translate to control of cancer progression in some metastatic patients and to improved survival.
Expression of the PD-1 inhibitory immune receptor may interfere with the development of the abscopal effect. 31 This possibility was examined in a preclinical experimental model in mice bearing tumors in two different and remote from each other locations. One of the tumors was irradiated with a single dose of 15 Gy, while the second tumor served as control. An abscopal effect was evident in the non-irradiated tumors and was more prominent in mice receiving an anti-PD-1 antibody or in PD-1 receptor knockout mice, compared with control mice. Moreover, interfering with the PD-1 receptor function, either through genetic knockout or pharmacologically with the anti-PD-1 antibody, improved responses in the primary irradiated tumor. In contrast, no difference was observed in experiments where the non-irradiated tumors consisted of a different cell line from the one at the irradiated site. 31 Therefore, combinations of the two treatment modalities, radiation therapy, and immune checkpoint inhibitors, present an opportunity for synergy. Radiation in a distant body location would induce activation of immune cells by producing a cytokine-inflamed systemic environment which would boost further the effect of immune checkpoint inhibitors in immune cell activation. A clinical confirmation of this hypothesis was provided by data from a secondary analysis of a phase 1 trial of pembrolizumab in 98 patients with locally advanced or metastatic non-small cell lung cancer. 32 Forty-two of ninety-seven patients (one patient was lost to follow-up) had received radiation therapy at any time before starting pembrolizumab treatment. About two-thirds (27 patients) had received palliative radiation treatment and the remaining 15 patients had received previous definitive radiotherapy or a combination of definitive and palliative radiotherapy. Patients who had received radiotherapy before pembrolizumab had better Progression Free Survival (PFS) (median PFS of 4.4 months) compared with patients who had not received previous radiation therapy (median PFS: 2.1 months, hazard ratio: 0.56, 95% confidence interval: 0.34–0.91, p = 0.019). Similarly, the OS of patients who received prior radiation was better than the OS of their counterparts who had not received prior radiation (median OS: 10.7 months vs 5.3 months, hazard ratio: 0.58, 95% confidence interval: 0.36–0.94, p = 0.026). The benefit of previous radiation was also evident when only patients who had received extracranial radiotherapy were considered in the analysis. 32 Interestingly, in this cohort the median time between radiotherapy and subsequent pembrolizumab treatment was 9.5 months with a range of 1 month to 106 months. This suggests that the salutary effect of radiation in potentiating the immune checkpoint inhibitor efficacy may be more long-lasting.
In the current investigation, the putative effect on OS of palliative radiation in metastatic lung cancer patients who had been treated with immune checkpoint inhibitors was examined. Overall, the addition of palliative radiation in these patients did not influence significantly their survival. However, in the smaller subset of patients (10.4%) in the cohort who received one or few high-dose radiation fractions, defined as one or more fractions of at least 700 cGy, a positive treatment effect of prolonged OS was discerned.
Besides immune activation, radiation therapy has been observed in experimental systems to have immune suppressive effects through the activation of TGFβ, IL4, and IL-10 signaling. 33 Apoptotic cells in irradiated fields attract M2 macrophages, N2 neutrophils, and regulatory CD25+ T lymphocytes (Tregs), which contain the inflammation induced by the dying cells. 34 TGFβ is a cytokine, which in addition to being crucial for cancer cell motility and metastasis, provides inhibitory signals to the immune system. 35 A TGFβ signature has been associated with a lack of response in urothelial cancer patients treated with the PD-L1 inhibitor atezolizumab. 36 Cytotoxic CD8+ T lymphocytes were excluded from the tumor parenchyma and were restricted to the peripheral tumor stroma. Moreover, a combination of PD-L1 blockade with TGFβ blockade in a mouse model led to the restoration of CD8+ lymphocyte penetration and tumor regression. 36 A similar synergistic effect of PD-L1 and TGFβ blockade was also observed in a mouse model of colorectal cancer metastases, whence increased tumor lymphocyte infiltration as a result of reduced TGFβ signaling potentiated the antitumor immune effect of PD-L1 blockade. 37 A phase Ib/ II clinical study of the small molecule TGFβ inhibitor galunisertib in combination with the PD-1 inhibitor nivolumab disclosed an acceptable toxicity profile and a response rate of 24% in metastatic lung cancer patients who had previously received chemotherapy but were immunotherapy naive. 38 The median OS was 12 months. Specific attributes of radiation therapy, such as fraction and field size, organ irradiated, type of targeted cancer, and the temporal relationship between radiation and immunotherapy, may be of importance for obtaining a synergistic effect if these attributes have different effects in TGFβ as well as other immune system cascades.
The dose of radiation treatment is critical for the observed genomic response of cancer cells, and different doses ranging from 0.2 Gy to 10 Gy produce a different genomic signature of immune-related genes in diverse cancer cell line experiments. 39 Different genomic signatures were observed after irradiation to the same total dose but using different fractionations of radiation. In addition, the dose of radiation has been previously proposed to be of potential importance in the production or lack of abscopal effect associated with immune checkpoint inhibitors. Experiments in mice showed that radiation treatment at a dose of 8 Gy when given together with an anti-mouse CTLA4 monoclonal antibody was effective in producing an abscopal effect. 40 In contrast, a dose of 20 Gy was ineffective in inducing a synergistic effect between the two therapy modalities. The differential effectiveness of the two radiation doses was found to be related to the activity of DNA exonuclease Three prime Repair Exonuclease 1 (TREX1). TREX1 activation is induced by the higher radiation dose, but not by the 8 Gy dose. Activated exonuclease TREX1, prevents cGAS activation by cleaving dsDNA that has leaked to the cytoplasm following cell irradiation. Lack of activation of the cGAS/ STING cascade in cells with TREX1 activation by the higher radiation dose precludes induction of type I IFNs response, as described above. A single dose of 12 to 15 Gy or above was shown to induce TREX1 in different cell lines, and a decrease in dsDNA production post-irradiation was observed in parallel. 40 Fractions of 6–8 Gy also led to an optimal production of interferon gamma by tumor-associated CD8+ T cells. 41 Whether similar fractionation of irradiation is optimal for synergistic systemic effect in combination with immunotherapy in other types of primary cancers, besides lung cancer, remains an important clinical question. This could be answered with studies similar to the current study, as the clinical use of immune checkpoint inhibitors expands. In this regard, exploration of the radiation dose in preclinical models suggests that the response to different fractionations of radiation is also relevant for the survival and proliferation of breast cancer cells. 42 Moreover, the genomic landscape of individual tumors and the presence of alterations in the DNA damage response machinery are critical for determining the response to different doses of radiation and the ability of cancer cells to repair sub-lethal radiation doses. 43 The most frequently mutated tumor suppressor gene across cancers, p53 participates in the DNA damage response and its mutations alter the sensitivity of cancer cells to split doses of radiation therapy. In another preclinical study, the use of even moderate hypofractionation of radiation (daily doses of 2.75 Gy) produced divergent levels of proliferation arrest in lung cancer cell lines and fibroblasts. 44 Immune checkpoint inhibitors targeting other immune receptors, besides CTLA-4 and the PD-L1/ PD-1 pair which are in advanced clinical development could also modulate radiation effects, and their synergy with radiation will need to be explored.
In addition to radiation fractionation, the irradiated tumor volume may also be of importance in the systemic effect of radiation treatment and the ability of irradiated cells-derived circulating factors to prime a T cell immune response. 45 With the improvement of imaging and radiation delivery techniques allowing enhanced volume targeting accuracy, the effect of combining hypofractionated radiotherapy with immunotherapy in patients with oligometastatic disease to obtain synergistic and possibly more durable effects is also worth investigating.46,47
Our study has limitations. The retrospective design is prone to bias stemming from potential confounding factors. OS is the most robust survival outcome and has the smallest probability to be affected by the retrospective non-randomized, non-blinded design of the study and was chosen as the primary outcome of interest to mitigate some of the outcomes bias associated with retrospectively ascertaining PFS or Disease-Specific Survival. Moreover, the small number of included patients reduces the confidence in the observed results. The patients included in the study had received one to four previous lines of systemic therapy at the time of radiotherapy, a fact that could affect the efficacy of subsequent therapies and survival outcomes. Although all patients had metastatic disease, the burden of the disease and the number of organs involved varied and could also have influenced survival outcomes. No data on key pathologic predictors of immunotherapy response, including PD-L1 expression and microsatellite instability status were available. However, microsatellite instability is rare in lung cancers and therefore it would be unlikely that it plays a significant role in the observed results.
Conclusion
The current retrospective data suggest a systemic benefit of hypofractionated radiotherapy in combination with immune checkpoint inhibitors in metastatic lung cancer patients. Although these data are only hypothesis generating and require prospective validation, hypofractionated radiation should be the preferred mode of treatment in metastatic lung cancer patients who require palliative radiation and receive concomitant immunotherapy.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was partially funded by a grant by the Sault Ste Marie Academic Medical Association (to I.A.V.)
Ethics declaration
Research was contacted in accordance with the declaration of Helsinki.
Consent to participate declaration
As this was a retrospective study involving only review of medical records the ethics committee has waived requirement for individual patient consent.