
Abstract
Endocrine disruptive chemicals (EDCs) are considered as the potential attributes for the increasing trend in obesity and metabolic syndrome (MS) through disruption of sex hormones, particularly in women. We evaluated the association of understudied EDC compounds with total testosterone (TT), sex hormone-binding globulin (SHBG), obesity, and MS. A population-based cross-sectional study was conducted using the National Health and Nutrition Examination Survey datasets collected during the years 2013–2016. Women of age ≥15 years with urinary measurements of nonpersistent EDCs, including bisphenol, triclosan, triclocarban, dichlorophenol, and paraben compounds were included in this study. Data were analyzed using the modified Poisson models to estimate the adjusted relative risk (RR) and 95% confidence interval (CI). The associations were also validated by considering TT and SHBG concentrations as the outcomes. The study included 1974 women with 11% high TT, 10.5% low SHBG, 40% obesity, and 46.2% MS. A medium to high exposure to bisphenol-A (RR = 1.64; 95% CI: 1.14, 2.35, p = 0.009), bisphenol-F (RR = 1.83; 95% CI: 1.35, 2.49, p < 0.001), bisphenol-S (RR = 1.83; 95% CI: 1.35, 2.49, p = 0.041) and 2, 4- dichlorophenol (RR = 1.61; 95% CI: 1.06, 2.45, p = 0.026) were associated with low SHBG but not with high TT. In addition, high exposure to triclosan was also inversely associated with SHBG concentrations (regression coefficient = −0.09; 95% CI: −0.15, −0.02, p = 0.013). However, these EDCs were found to be associated with SHBG, obesity, and MS according to menopausal status. High exposure to certain nonpersistent EDCs was associated with low SHBG, obesity, and MS according to menopausal status.
Introduction
The continuous rise in obesity and metabolic syndrome (MS) leading to adverse health outcomes has become a major health concern worldwide. 1 Recent studies postulated the possibility of environmental pollutants contributing to the global burden of obesity and MS.2–4 Several epidemiological and experimental studies in recent years have reported adverse health effects associated with environmental endocrine-disrupting chemicals (EDCs).4,5 EDCs are additives observed in personal care, cosmetic, and household products that influence the endocrine system. EDCs are associated with reproductive health, diabetes, obesity, neurodevelopmental disorders, and hormone-dependent cancers leading to substantial economic burden.5–7 EDCs are classified into persistent and nonpersistent chemicals. Persistent EDCs are organic pollutants that accumulate in the environment for a long time because of their long half-life. Although nonpersistent EDCs have a short half-life with reduced liposolubility, they can modify hormonal actions in the human body. Nonpersistent EDCs are more prevalent in the environment due to their widespread use in household products.8,9 The most common nonpersistent EDCs in the environment are phenols (including bisphenol, triclosan, triclocarban, dichlorophenol, and benzophenone-3), parabens, and phthalates. 9 A rapid increase in MS, especially in reproductive-aged females is noticed in a recent study indicating sex differences in health outcomes associated with differential levels of exposure to EDCs affecting sex hormones differently.10–12
EDC interactions with hormonal receptors may decrease the steroid-binding ability of sex hormone-binding globulin (SHBG), a hepatic protein that functions in the blood as a major transporter of sex hormones.13,14 Limited studies explored the association of nonpersistent EDCs with sex hormones and metabolic abnormalities among females yielding conflicting associations.6,15–17 The levels of sex hormones differ between pre- and postmenopausal women.18,19 Therefore, the aim of this study was to examine the association of exposure to understudied nonpersistent EDCs with sex hormones, obesity, and MS in females. We also sought to evaluate these associations according to their menopausal status.
Endocrine-disrupting chemicals (EDCs) are pervasive in the environment which adversely affects overall health by disrupting the sex hormones. The associations of some nonpersistent EDCs with sex hormones and metabolic abnormalities are unknown, particularly in women.
High exposure to bisphenol compounds and triclosan is associated with low SHBG and metabolic syndrome. In addition to bisphenol compounds, high triclocarban is also associated with obesity and metabolic syndrome.
Our study suggests that screening and mitigation of exposure to some EDCs are required among subjects with low SHBG or obese or metabolic syndrome.
Materials and methods
Study population
We conducted this cross-sectional study utilizing data from the National Health and Nutrition Examination Survey (NHANES), a program conducted by the Centers for Disease Control and Prevention (CDC) designed to assess the health and nutritional status of non-institutionalized adults and children in the United States, every year. We extracted data from NHANES for the years 2013 and 2016 to conduct this study as these two cycles of the NHANES database have the most recent data available to address our research questions. 6 All females aged 15 years or older were eligible for this study. A total of 1974 participants were included in the analysis after excluding females without EDCs (4146) and pregnancy status (31). Due to only one-third of individuals being surveyed for EDCs profiling in NHANES, a large proportion of female participants were excluded from this study. NHANES collects demographic, nutritional, behavioral, health, and biological data using standardized protocols after obtaining written informed consent from subjects and receiving approval from the National Center for Health Statistics Research Ethics Review Board of the CDC. We followed the Strengthening the Reporting of Observational Studies in Epidemiology reporting guidelines in this study. 20
Exposure assessment
Subject exposure to endocrine disruptors was measured through urine samples. Samples were processed according to the CDC protocols for urine profiling of EDCs. The CDC protocols followed for sample analysis, data processing, quality assessment, troubleshooting, and computational analysis for quality control and high standards have been reported in previous publications.6,21 EDCs were quantified using a high-performance liquid chromatography-electrospray ionization–tandem mass spectrometry method and measured in ng/mL. We included metabolites of 12 EDCs, including bisphenol-A (BPA), bisphenol-S (BPS), bisphenol-F (BPF), triclosan (TCA), triclocarban (TCC), 2,5-dichlorophenol (2,5-DCP), 2,4-dichlorophenol (2,4-DCP), benzophenone-3 (BP3), butylparaben (BP), ethylparaben (EP), methylparaben (MP), and propylparaben (PP). Given the non-Gaussian distribution of EDCs and the possibility of nonlinear associations with outcomes, we categorized EDC concentrations into tertiles for statistical analysis, with the lowest tertile considered as the reference category. The EDCs were categorized into tertiles to retain the maximum number of observations in each category.
Outcomes: sex hormones assessment
The NHANES collected the serum samples along with urinary samples from the participants at the same time as other survey data collected using standardized protocols. Serum samples were used for defining sex hormones and MS in this study. The primary outcome measures were serum concentrations of SHBG and total testosterone (TT). The serum concentrations of SHBG were quantified by the electrochemiluminescence assay method while the serum concentrations of TT were quantified by the liquid chromatography-tandem mass spectrometry method. A SHBG level less than 30 nmol/L was used to define low SHBG. TT concentrations greater than 46 ng/dL (to convert to nanomoles per liter, multiply by 0.0347) for ages less than 50 years and a TT level greater than 32 ng/dL for ages 50 years or older were used to define high TT levels. These cutoffs were established and validated for female subjects in the NHANES database.6,18 We further validated findings by using log-transformed SHBG and TT concentrations in the analyses.
Outcomes: obesity and MS assessments
In NHANES, laboratory and physical measures are collected in mobile examination centers by trained staff using standardized methods. Obesity was calculated using the body mass index (BMI, kg/m2). A BMI of 30 or more was used to define obesity. The MS outcome was defined as per the National Cholesterol Education Program’s Adult Treatment Panel III. Accordingly, individuals with three or more abnormal levels of cardiometabolic symptoms including fasting glucose, blood pressure, cholesterol, high-density lipoprotein, and waist circumference were classified as having MS. 6
Covariates
We also recorded some covariates to adjust for confounding bias, such as age (years), race and ethnicity (Hispanic, Non-Hispanic Black, Non-Hispanic White, other [non-Hispanic Asian or other races, including multiracial]), and marital status (married or other [widowed, divorced, separated, never married, living with a partner, or unknown]). Educational level was classified into lower than or equal to a high school diploma or greater than a high school diploma. Annual household income was divided into categories <$45,000, $45,000–$99 999, ≥$100,000, or unknown. Self-reported behavioral characteristics included physical activity (low or moderate/vigorous), drinking status (yes or no), and smoking status (yes or no). Urinary creatinine (mg/dL) was also recorded for the adjustment purpose in this study.6,22
Statistical analysis
We used survey weight-adjusted analyses to account for the complex survey design used for data collection in the NHANES study. The distribution of EDC concentrations was described using various quantiles (including median and interquartile range[IQR]), whereas the distribution of all categorical variables was summarized with weighted frequency and percentages. In the primary analysis, we used a survey generalized linear model (GLM) with a Poisson family distribution and log link to determine the adjusted association of each categorized EDC with high TT, low SHBG, obesity, and MS after adjusting for all considered covariates. A joint test was used to determine the overall association of each categorized EDC with each categorized outcome. The adjusted association of each EDC with each outcome was also evaluated with survey GLM models using a Poisson distribution and log link separately for pre- and postmenopausal women. Based on multiple studies, we classified women with age below 50 years as a premenopausal group whereas age ≥50 as a postmenopausal group.
6
The combined exposure of each EDC is determined by the sum of substances based on their parent compounds.
Results
The average age of participants was 46.9 (SD: 18.5) years with majority non-Hispanic whites (62.8%; Table 1). In total, we observed 10.9% high TT, 10.5% low SHBG, 46.2% MS, and 40.1% obesity (Supplemental Table 1). The median concentrations were highest for MP (78.1; IQR: 23, 245.9) followed by BP3 (23.5; IQR: 6.3, 117.0), PP (13.5, IQR: 2.7, 57.5), and TCA (4.5, IQR: 1.2, 23.2; Supplemental Table 2).
Subject characteristics, NHANES (2013–2016).
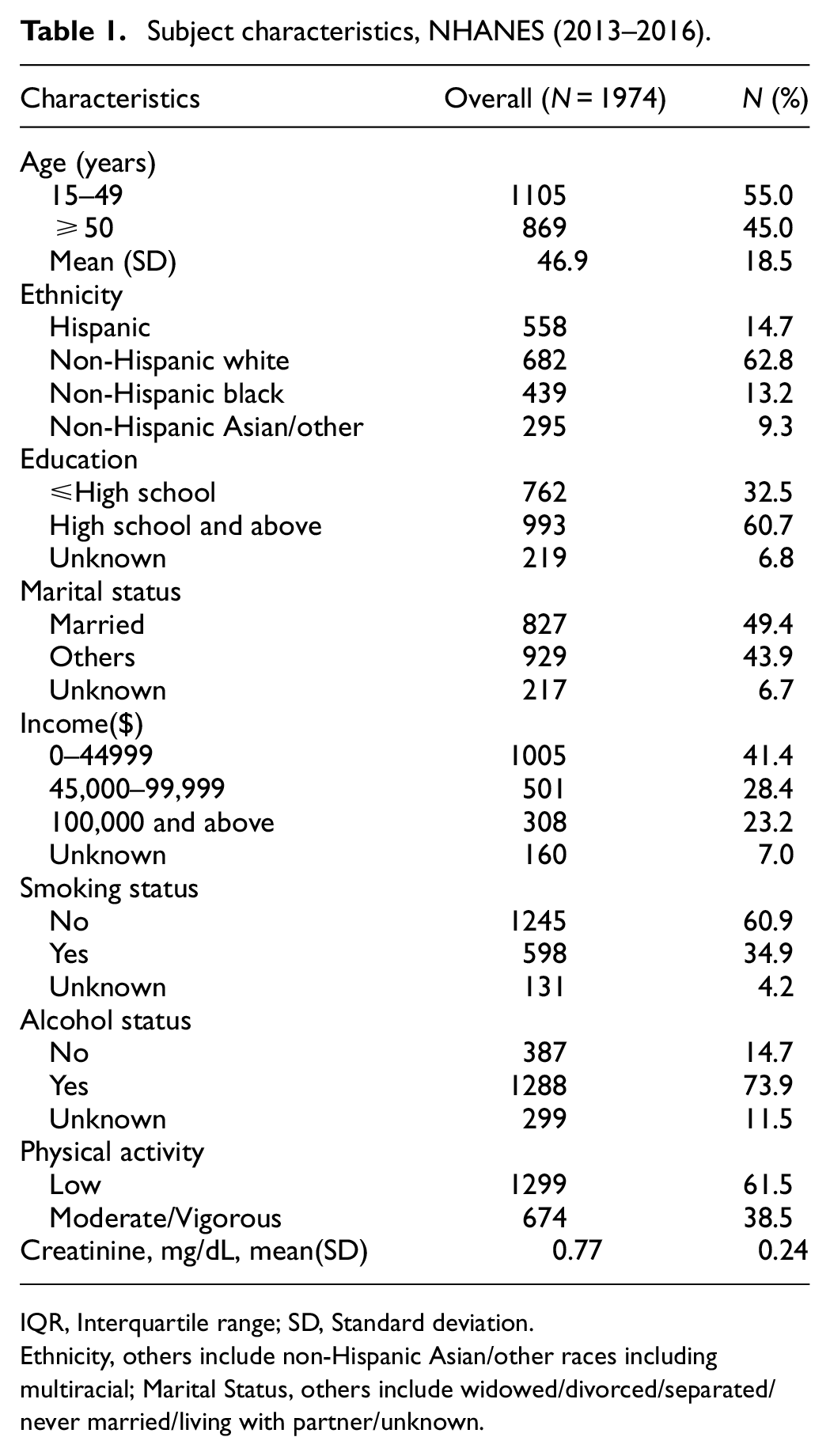
IQR, Interquartile range; SD, Standard deviation.
Ethnicity, others include non-Hispanic Asian/other races including multiracial; Marital Status, others include widowed/divorced/separated/never married/living with partner/unknown.
None of the EDCs was positively associated with high TT in the overall sample or in pre- or postmenopausal groups (Table 2). Only BP-3 levels were positively associated with TT concentrations in premenopausal women (Supplemental Table 3). In contrast, high tertile of BPA (RR = 1.64; 95% CI: 1.14, 2.35) and BPF (1.83; 95% CI: 1.35, 2.49) and middle tertile of BPS (1.83; 95% CI: 1.35, 2.49) and 2,4-DCP (1.61; 95% CI: 1.06, 2.45) were significantly associated with low SHBG. Some of these associations were statistically significant after adjusting for multiple testing. High tertile of BPS (RR = 1.73; 95% CI: 1.01, 2.98), BPF (RR = 1.99; 95% CI: 1.30, 3.05), and 2,4-DCP (RR = 1.75; 95% CI: 1.04, 2.94) were found to be significantly associated with low SHBG only in premenopausal women while high tertile of BPA (RR = 2.25; 95% CI: 1.24, 4.08), TCA (RR = 2.59; 95% CI: 1.17, 5.72), and BP (RR = 1.88; 95% CI: 1.11, 3.19) were associated with low SHBG in postmenopausal women (Table 3). High levels of BPA and BPF remained significantly associated with lower SHBG concentrations in pre- and postmenopausal women, respectively. In addition, middle and high tertiles of TCA were also inversely associated with SHBG concentrations in postmenopausal women. However, a high tertile of BP-3 and EP was associated with higher concentrations of SHBG in premenopausal women while a high tertile of MP was associated with higher concentrations of SHBG in postmenopausal women (Supplemental Table 4).
Adjusted association of each EDC with high TT in all subjects and by menopausal status, NHANES (2013-16).
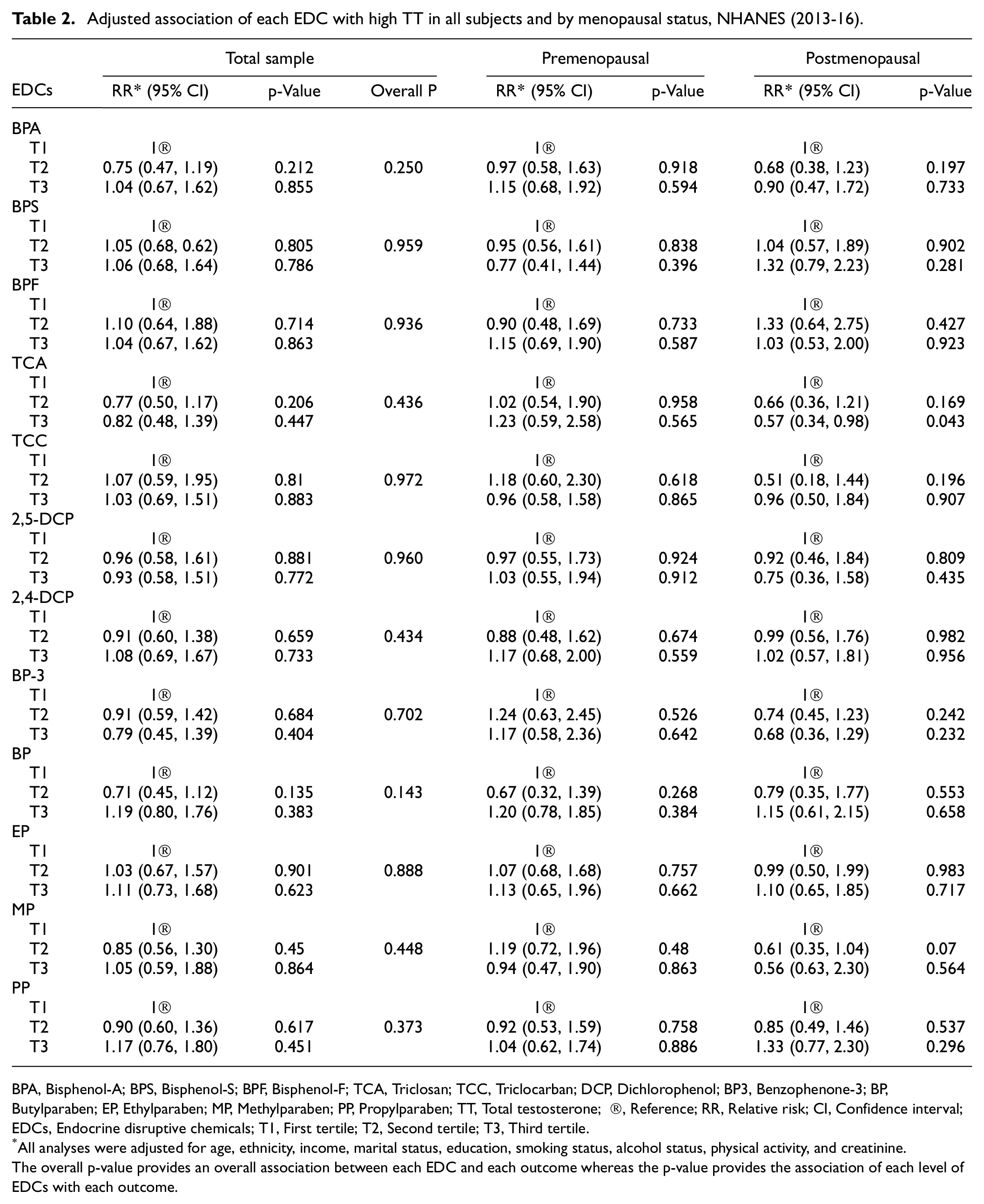
BPA, Bisphenol-A; BPS, Bisphenol-S; BPF, Bisphenol-F; TCA, Triclosan; TCC, Triclocarban; DCP, Dichlorophenol; BP3, Benzophenone-3; BP, Butylparaben; EP, Ethylparaben; MP, Methylparaben; PP, Propylparaben; TT, Total testosterone; ®, Reference; RR, Relative risk; CI, Confidence interval; EDCs, Endocrine disruptive chemicals; T1, First tertile; T2, Second tertile; T3, Third tertile.
All analyses were adjusted for age, ethnicity, income, marital status, education, smoking status, alcohol status, physical activity, and creatinine.
The overall p-value provides an overall association between each EDC and each outcome whereas the p-value provides the association of each level of EDCs with each outcome.
Adjusted association of each EDC with low SHBG in all subjects and by menopausal status, NHANES (2013–2016).
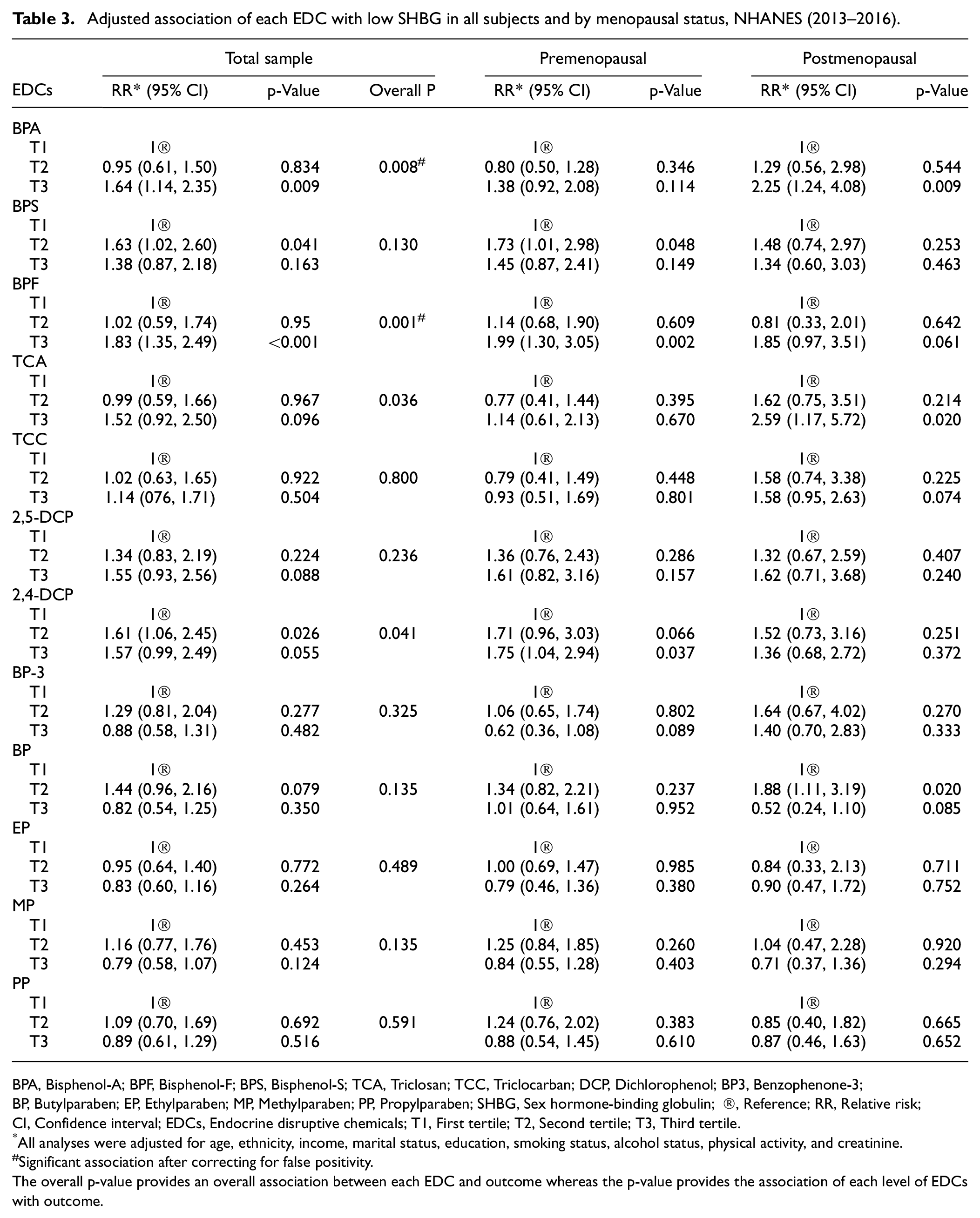
BPA, Bisphenol-A; BPF, Bisphenol-F; BPS, Bisphenol-S; TCA, Triclosan; TCC, Triclocarban; DCP, Dichlorophenol; BP3, Benzophenone-3;BP, Butylparaben; EP, Ethylparaben; MP, Methylparaben; PP, Propylparaben; SHBG, Sex hormone-binding globulin; ®, Reference; RR, Relative risk;CI, Confidence interval; EDCs, Endocrine disruptive chemicals; T1, First tertile; T2, Second tertile; T3, Third tertile.
All analyses were adjusted for age, ethnicity, income, marital status, education, smoking status, alcohol status, physical activity, and creatinine.
Significant association after correcting for false positivity.
The overall p-value provides an overall association between each EDC and outcome whereas the p-value provides the association of each level of EDCs with outcome.
High tertile of BPA (RR = 1.40; 95% CI: 1.12, 1.76), BPF (RR = 1.27; 95% CI: 1.12, 1.44), and TCC (RR = 1.24; 95% CI: 1.05, 1.46) was associated with obesity. In addition, middle (RR = 1.29; 95% CI: 1.05, 1.59) and high (RR = 1.37; 95% CI: 1.12, 1.67) tertiles of BPS were also associated with obesity in adjusted analyses. In contrast, high tertile of EP (RR = 0.68; 95% CI: 0.56, 0.82) and MP (RR = 0.81; 95% CI: 0.72, 0.91) was inversely associated with obesity. All these associations were statistically significant after adjusting for false positivity (Table 4). In the stratified analysis, the higher levels of BPS (RR = 1.76; 95% CI: 1.41, 2.20) and BP-3 (RR = 1.20; 95% CI: 1.01, 1.42) were associated with obesity in premenopausal women while the high tertile of BPF (RR = 1.45; 95% CI: 1.10, 1.89) and TCC (RR = 1.29; 95% CI: 1.07, 1.56) was positively associated with obesity in postmenopausal women. A high tertile of BPA was associated with obesity in both pre- (RR = 1.46; 95% CI: 1.09, 1.96) and postmenopausal (RR = 1.41; 95% CI: 1.07, 1.86) groups (Table 4). A higher tertile of BPA (RR = 1.15; 95% CI: 1.00, 1.33) and TCC (RR = 1.16 (1.01, 1.33) was positively associated with MS whereas EP and MP were inversely associated with MS in adjusted analyses. However, these associations except for EP did not reach a statistical significance level after adjusting for multiple comparisons (Table 5).
Adjusted association of each EDC with obesity in all subjects and by menopausal status, NHANES (2013–2016).
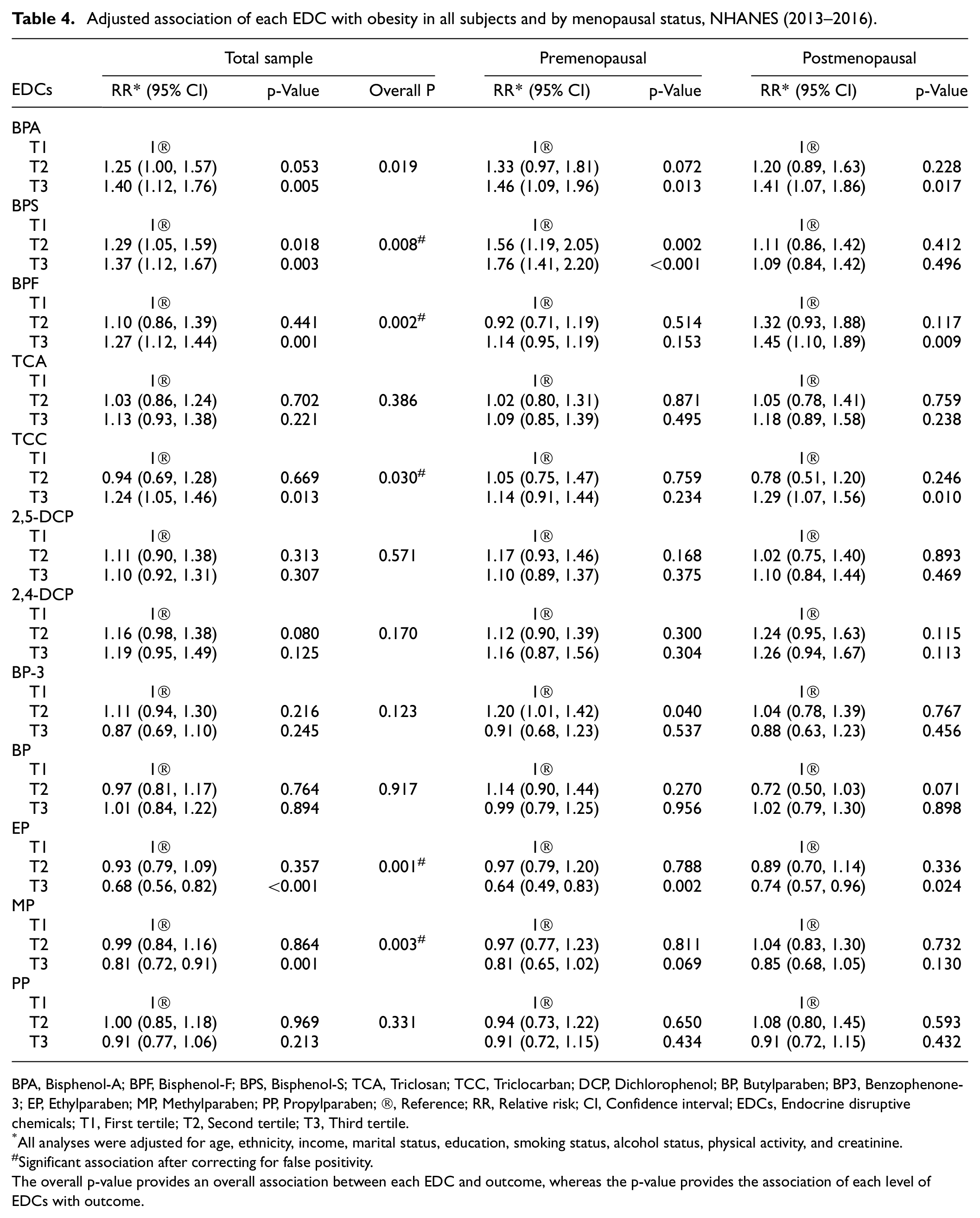
BPA, Bisphenol-A; BPF, Bisphenol-F; BPS, Bisphenol-S; TCA, Triclosan; TCC, Triclocarban; DCP, Dichlorophenol; BP, Butylparaben; BP3, Benzophenone-3; EP, Ethylparaben; MP, Methylparaben; PP, Propylparaben; ®, Reference; RR, Relative risk; CI, Confidence interval; EDCs, Endocrine disruptive chemicals; T1, First tertile; T2, Second tertile; T3, Third tertile.
All analyses were adjusted for age, ethnicity, income, marital status, education, smoking status, alcohol status, physical activity, and creatinine.
Significant association after correcting for false positivity.The overall p-value provides an overall association between each EDC and outcome, whereas the p-value provides the association of each level of EDCs with outcome.
Adjusted association of each EDC with MS in all subjects and by menopausal status, NHANES (2013–2016).
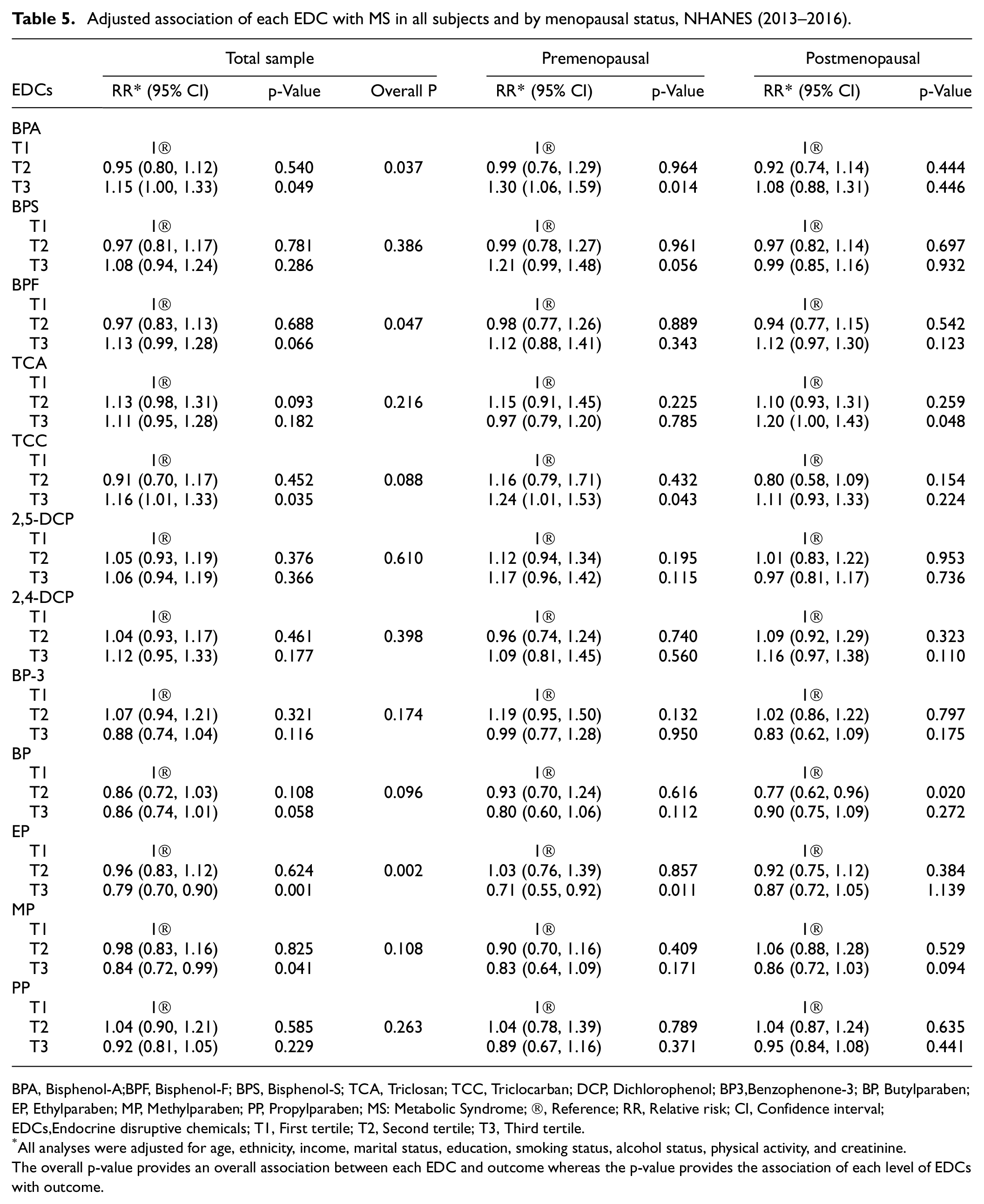
BPA, Bisphenol-A;BPF, Bisphenol-F; BPS, Bisphenol-S; TCA, Triclosan; TCC, Triclocarban; DCP, Dichlorophenol; BP3,Benzophenone-3; BP, Butylparaben; EP, Ethylparaben; MP, Methylparaben; PP, Propylparaben; MS: Metabolic Syndrome; ®, Reference; RR, Relative risk; CI, Confidence interval; EDCs,Endocrine disruptive chemicals; T1, First tertile; T2, Second tertile; T3, Third tertile.
All analyses were adjusted for age, ethnicity, income, marital status, education, smoking status, alcohol status, physical activity, and creatinine.
The overall p-value provides an overall association between each EDC and outcome whereas the p-value provides the association of each level of EDCs with outcome.
In the composite analysis of EDCs, none of the EDCs was associated with high TT (Figure 1A) or TT concentrations (Table S5). However, higher bisphenol concentrations (RR = 1.22; 95% CI: 1.03, 1.46) were associated with low SHBG in premenopausal women while higher concentrations of TCA/TCC (RR = 1.16; 95% CI: 1.04, 1.30) and dichlorophenol (RR = 1.13; 95% CI: 1.00, 1.29) concentrations were associated with low SHBG in postmenopausal women (Figure 1(a)). Total bisphenol and TCA/TCC concentrations were also inversely associated with SHBG concentrations in postmenopausal women (Supplemental Table 5). Higher bisphenol concentrations were associated with obesity in both pre- (RR = 1.15; 95% CI: 1.05, 1.25) and postmenopausal (RR = 1.12; 95% CI: 1.02, 1.24) women. Total TCA/TCC concentrations were only associated with MS (RR = 1.05; 95% CI: 1.01, 1.09) in postmenopausal women (Figure 1(b)).
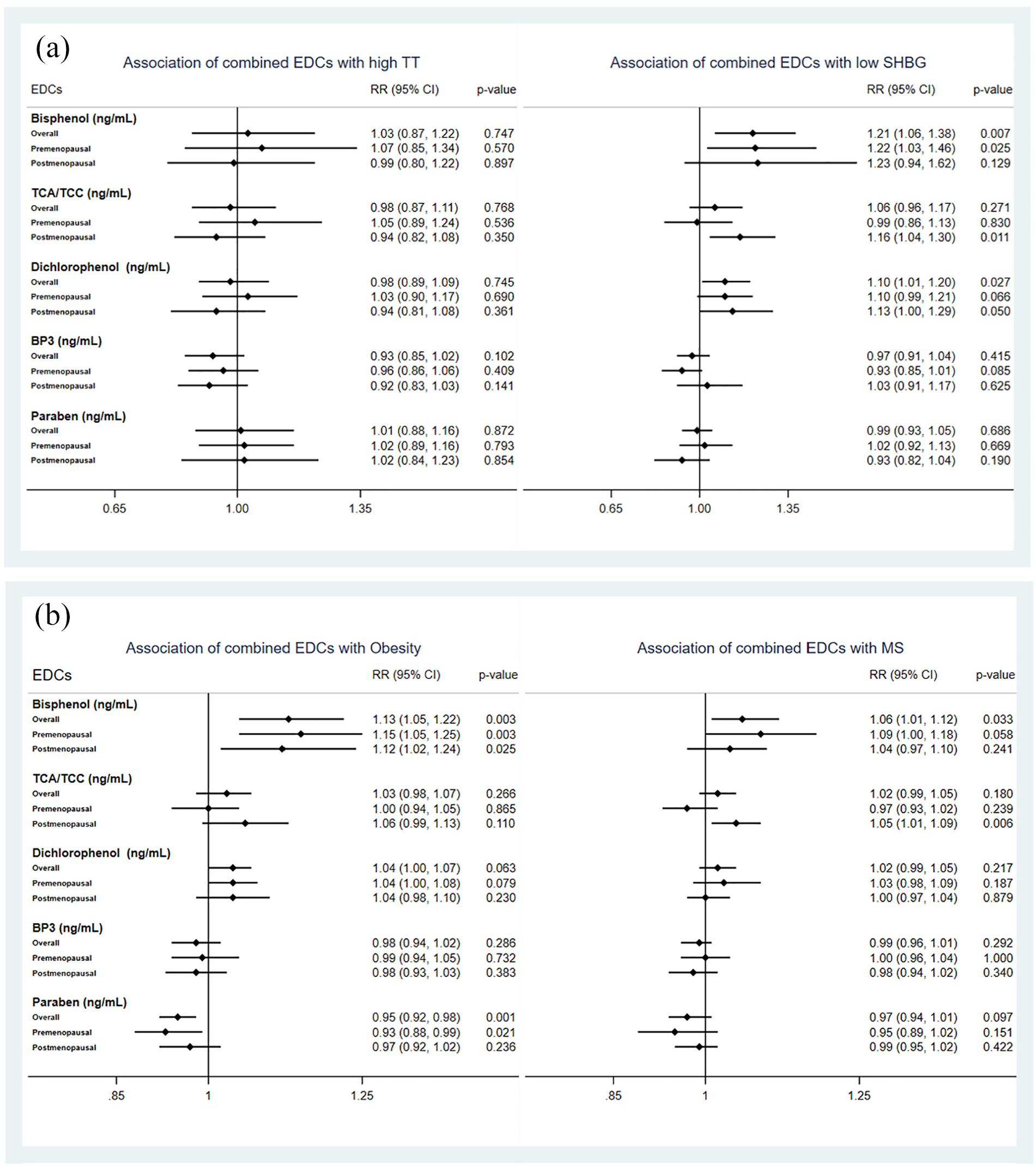
(a) Adjusted associations of combined EDCs with high TT and low SHBG. (b) Adjusted associations of combined EDCs with obesity and MS, NHANES (2013-16).
Discussion
Our study suggests that higher levels of some analogs of bisphenol are associated with low SHBG, obesity, and MS but not with high TT according to menopausal status. In addition, higher levels of TCA and 2,4-DCP were also associated with low SHBG, whereas high TCC exposure was only associated with obesity and MS. Low SHBG is considered a significant marker for adverse cardiometabolic health including hyperandrogenism and polycystic ovary syndrome among women 18 and is strongly associated with phthalate metabolites and aldehyde in women.6,23 Most of the considered nonpersistent EDCs and their derivatives have a structural binding affinity with human SHBG along with strong concordance with androgen receptor indicating that medium to high exposure to these EDCs can affect SHBG functions and subsequently exert adverse health outcomes.13,24,25 Contrary to our study and another study, 16 several small-sized studies reported either no association or positive association between BPA levels and SHBG concentrations among adult women.26,27
All considered analogs of bisphenol and TCC were found to be associated with obesity and MS according to menopausal status in our study. Except for a few, 28 several studies supported our findings that higher exposure to BPA is associated with obesity and metabolic components in women.29,30 Consistent with our study, a review noticed that BPS is more obesogenic than BPA with a different mechanism. 31 Several reviews highlighted the influence of bisphenol analytes on C-reactive protein, oxidative stress, and inflammatory markers linking the potential relationship between bisphenols and MS, including obesity.32,33 Although we did not observe an association between TCA and obesity, two studies reported conflicting associations based on NHANES datasets.34,35 In contrast, several US studies identified that TCC but not TCA is associated with an increased risk of diabetes attesting to the significance of TCC in metabolic abnormalities.36,37 Like our study, multiple cross-sectional studies reported an inverse association of BP3 and all parabens with obesity, metabolic abnormalities, and diabetes among adults,38,39 particularly in women. 40 Some studies suggested that some nonpersistent EDCs, including parabens and BP3 are highly lipophilic and they accumulate more in adipose fat tissues than the concentrations observed in urine. Therefore, individuals with higher body fat may store more parabens and BP3 in their adipose fat tissues and excrete less amounts in urine. This phenomenon was observed more among women than men owing to more adipose tissues among females.41,42 Kolatorova et al. used plasma as a matrix for paraben analysis during the menstrual cycle and identified a positive association between total parabens and obesity. 43
Similar to our study, a few studies reported a nonsignificant association between EDCs and TT in men or women.6,27,44,45 Although there is no study directly associating BPS, BPF, TCA, TCC, or DCP with SHBG or TT, and MS among pre- or postmenopausal women, emerging evidence suggests these EDCs may influence reproductive and endocrine health, particularly in women.31,46,47 Since premenopausal women are more susceptible to EDC exposure than postmenopausal women, most EDCs are likely to affect SHBG, obesity, and MS during reproductive age. 12 However, adverse cardiometabolic health associated with changes in the hormonal profile is often observed among menopausal women. 19 Due to a significant decline in antioxidant capacity and increased oxidative stress in postmenopausal women, 48 some EDCs may profoundly affect SHBG levels and obesity in postmenopausal women.16,33,49 In addition, it is likely that some EDCs may take a longer duration of exposure to show their effects. Furthermore, some EDCs may yield low doses and non-monotonic effects according to menopausal status. 50
The underlying mechanism between EDCs and metabolic abnormalities is not fully understood as EDCs can target multiple pathways by binding with nuclear receptors and aryl hydrocarbon receptors and may act as antagonists or agonists.46,51 Therefore, EDCs can affect hormone actions, metabolism, and biosynthesis. 52 Our study findings suggest two possible mechanisms are likely to occur with exposure of considered EDCs on metabolic abnormalities. Firstly, the influence of EDCs on the downregulation of SHBG levels affects the distribution and circulation of steroid hormones to target tissues and cells.13,24 The influence of EDCs on SHBG functions through disruption of the hypothalamic-pituitary-adrenal (HPA), -gonadal (HPG), and -thyroid (HPT) axes, potentially may lead to obesity, MS, and other reproductive health effects.11,46 The second mechanism could be the impact of considered EDCs on nuclear receptors, particularly estrogen receptor, androgen receptor, peroxisome proliferator-activated receptors, and retinoid X receptor affecting SHBG functions leading to energy balance, inflammation, and glucose homeostasis, obesity, and MS.5,53
Due to cross-sectional analysis, the associations of EDCs with sex hormones and metabolic health obtained in this study cannot be causally linked. Moreover, a single-point assessment of exposure to EDCs did not allow us to evaluate variability in the assessment of EDCs and their associations with sex hormones, obesity, and MS. Although the urinary measure of EDCs mostly detects exposure to nonpersistent EDCs, the collection, and analysis of other matrices such as serum or blood along with urine matrix on repeated measurements may provide more insights for the associations. The assessment of EDCs among one-third of the survey participants may further limit the generalizability of our findings. Despite these limitations, our study comprehensively evaluated the associations of most understudied nonpersistent EDCs with sex hormones including SHBG, obesity, and MS utilizing the recent cycle of the NHANES database. Our comprehensive analysis including stratified analysis by menopausal status, adjusting for weighting structure of data and most critical covariates in the analysis, and individual and composite analysis of EDC compounds increased the reliability and usefulness of our study findings.
In conclusion, higher levels of the considered EDCs were associated with low SHBG, obesity, and MS except for parabens. However, these associations varied according to menopausal status. Our study suggests that screening of bisphenol compounds and TCA/TCC may be required among low SHBG or obese subjects. Healthcare providers are required to spread community awareness to avoid products containing toxic EDCs during clinic visits and monitor harmful EDCs among at-risk individuals. Interventional and mechanistic studies are required to understand potential strategies for monitoring, screening, and early management of exposure to EDCs to avoid their adverse consequences among women.
Supplemental Material
sj-docx-1-imj-10.1177_10815589241297724 – Supplemental material for Association of exposure to nonpersistent endocrine disruptors with sex hormones and metabolic health in US females
Supplemental material, sj-docx-1-imj-10.1177_10815589241297724 for Association of exposure to nonpersistent endocrine disruptors with sex hormones and metabolic health in US females by Pallavi Dubey, Sireesha Y. Reddy, Chinthana Thangavel, Ghislain Hardy and Alok Kumar Dwivedi in Journal of Investigative Medicine
Footnotes
Acknowledgements
We appreciate the efforts of researchers and participants involved in the NHANES studies and the CDC. We also thank the biostatistics and epidemiology consulting lab members and postdocs for preliminary data analyses.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data availability
Supplemental material
The supplementary file includes tables reporting all additional results.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.