
Abstract
While some studies have suggested better outcomes for critically ill patients with balanced solutions over normal saline, the best type of intravenous fluid to use for stroke patients remains unknown. Using a retrospective chart review of 2015–2019 Get with the Guidelines® data at a single academic medical center, this study sought to determine whether balanced solutions or normal saline are associated with risk of hemorrhagic transformation or 90-day disability in patients with acute ischemic stroke treated with intravenous thrombolysis. Exposure was the type of intravenous fluid and outcomes were modified Rankin scale (mRS) ≤2 at 90 days and hemorrhagic transformation. Multivariate analysis controlled for age, demographics, medical history, time to tissue plasminogen activator (tPA), and admission stroke scale. We identified 302 patients who received thrombolysis, of which 166 patients had mRS data at 90 days. In univariate analysis, exposure to any balanced solution was associated with increased 90-day disability (odds ratio (OR) 4.3, 95% confidence interval (CI) 3.8–4.9) and hemorrhagic transformation (OR 2.0, 95% CI 1.3–2.2). In multivariate analysis, exposure to a balanced solution at any time was associated with increased 90-day disability (OR 6.3, 95% CI 2.4–17.0, p < 0.01), but not hemorrhagic transformation. Thus, this observational trial demonstrated that exposure to balanced solutions is associated with an increased risk of disability at 90 days and possibly hemorrhagic transformation in patients with acute ischemic stroke treated with intravenous thrombolysis. This data would suggest that normal saline is a preferred solution in these patients, though larger future trials are needed.
Introduction
Acute ischemic stroke is a leading cause of death and disability. Intravenous fluids are one of the most common medications administered to hospitalized patients. Normal saline has historically been the fluid used for inpatients. In 2018, two large cluster randomized trials suggested that balanced solutions (e.g., Lactated Ringer’s, Plasma-lyte(B), Hartman’s Solution) lead to improved outcomes, particularly in terms of renal function in critically ill patients.1,2 Normal saline is not only slightly hypernatremic but it is very hyperchloremic and can lead to non-anion gap acidosis. This hyperchloremia is thought to damage the maculae densae of the kidneys, leading to renal dysfunction when used in large volumes. However, two more recent large, randomized trials have shown no benefit to balanced solutions compared to normal saline in critically ill patients.3,4
Patients with acute ischemic stroke, though, may represent a unique subset of patients. Many balanced solutions are hypo-osmolar and could theoretically lead to small shifts in osmolarity that place stroke patients at risk for cerebral damage and subsequent hemorrhage. Indeed, in studies examining colloids for traumatic brain injury, it appears osmolarity of the solution is the most important determinant in outcomes. 5 However, normal saline is known to cause endothelial damage and an inflammatory response, 6 which also could put patients at risk for hemorrhage, in a similar manner to the well-known increased risk for hemorrhage in patients with hyperglycemia. Given these hypotheses and the frequency with which inpatients receive intravenous fluids, we sought to determine whether exposure to balanced solutions vs normal saline increased the risk of hemorrhagic transformation or 90-day disability in acute ischemic stroke.
Materials and methods
This study was an Institutional Review Board-approved retrospective cohort study of 2015–2019 Get With the Guidelines® data of all patients who received thrombolysis at a single comprehensive stroke center. The outcomes were (1) a modified Rankin scale (mRS) at 90 days of 2 or less and (2) any classification of hemorrhagic transformation. Exposures were compared between balanced solution or normal saline exposure based on (1) whether a fluid type was received any time during the hospital stay, (2) which solution was received first (if received within 24 h of presentation), and (3) which solution was received during the majority of the hospitalization. The outcomes were included in the data set and fluid exposures were manually extracted by the author. Any infusion of 250 mL or greater of intravenous fluid was included, regardless of infusion rate. Carrier fluids for medications were not included. Multivariate analysis controlled for age, demographics, medical history, prior antiplatelet or anticoagulant use, time to tissue plasminogen activator (tPA) administration, and NIH stroke scale at admission. Patients who were lost to follow-up were excluded from 30-day analyses.
Univariate analysis was conducted using χ2 and odds ratios (ORs), and multivariate analysis was calculated using logistic regression, ORs, and Wald’s χ2. All analyses were performed in SAS Version 9.4® and Microsoft Excel®. Alpha was set at 0.05.
Results
There were 4926 patients in our Get With the Guidelines Data. We excluded 4264 patients (2056 who did not receive thrombolysis, 953 with intracerebral hemorrhage, 400 who received thrombolysis at an outside hospital, 470 with transient ischemic attack, and 385 with subarachnoid hemorrhage).
We included 302 patients with acute ischemic stroke who received thrombolysis at our center. Of these strokes, 23.2% (n = 70) were cardioembolic, 22.5% (n = 68) were cryptogenic, 20.9% (n = 63) had no etiology documented, 18.5% (n = 56) were caused by large artery atherosclerosis, 11.9% (n = 36) were caused by small vessel disease, and 3.0% (n = 9) were caused by other etiologies. There were 169 males (56.0%), and the vast majority were white (n = 286, 94.7%). Of the 302 patients, 166 (55.0%) had mRS data recorded at 90 days. At any point during their hospital stay, 271 (89.7%) patients had normal saline exposure, and 85 (28.1%) were exposed to a balanced solution. The vast majority of the patients with balanced solutions used (89.4%, 76/85) were exposed to Lactated Ringer’s. Thirty-nine patients (12.9%) suffered hemorrhagic transformation, 25 with hemorrhagic infarction and 14 with parenchymal hemorrhage.
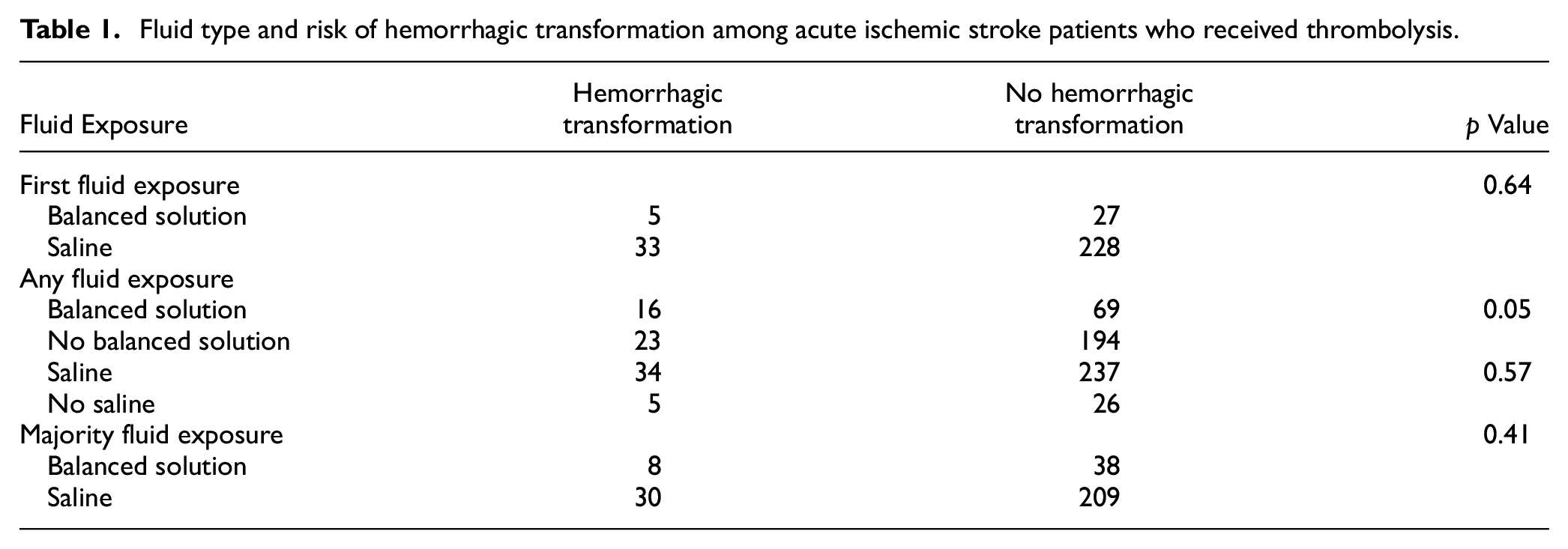
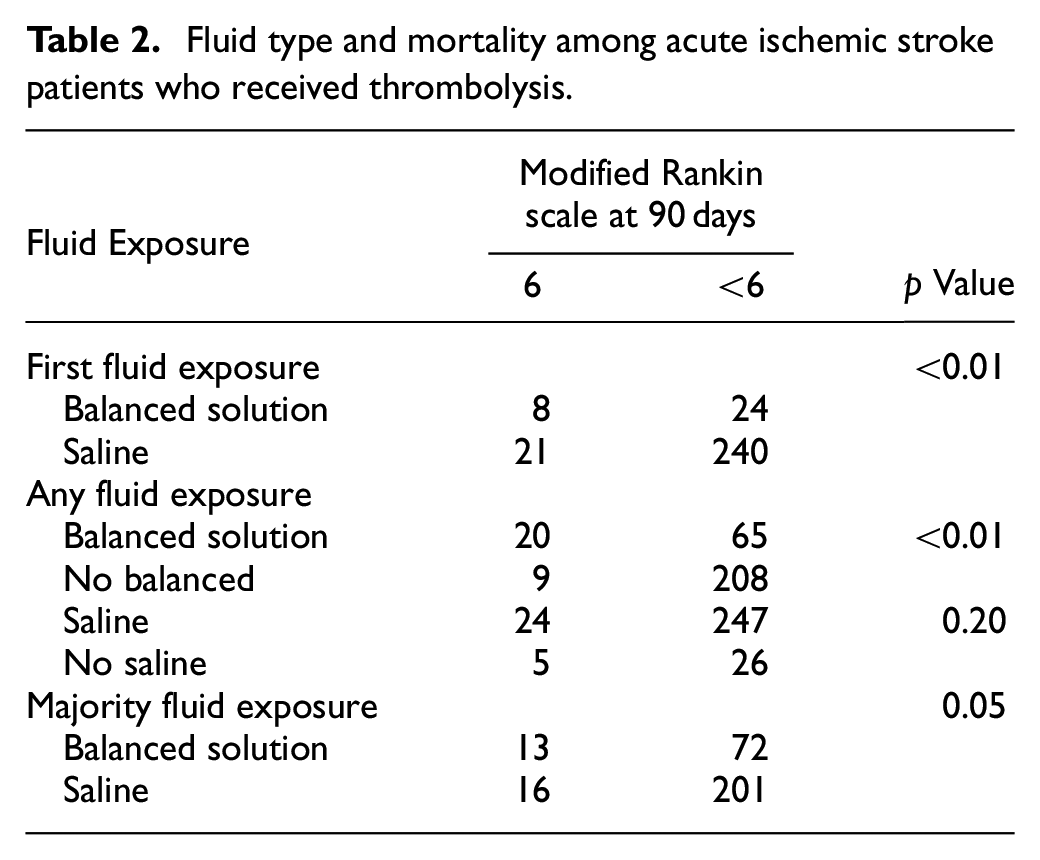
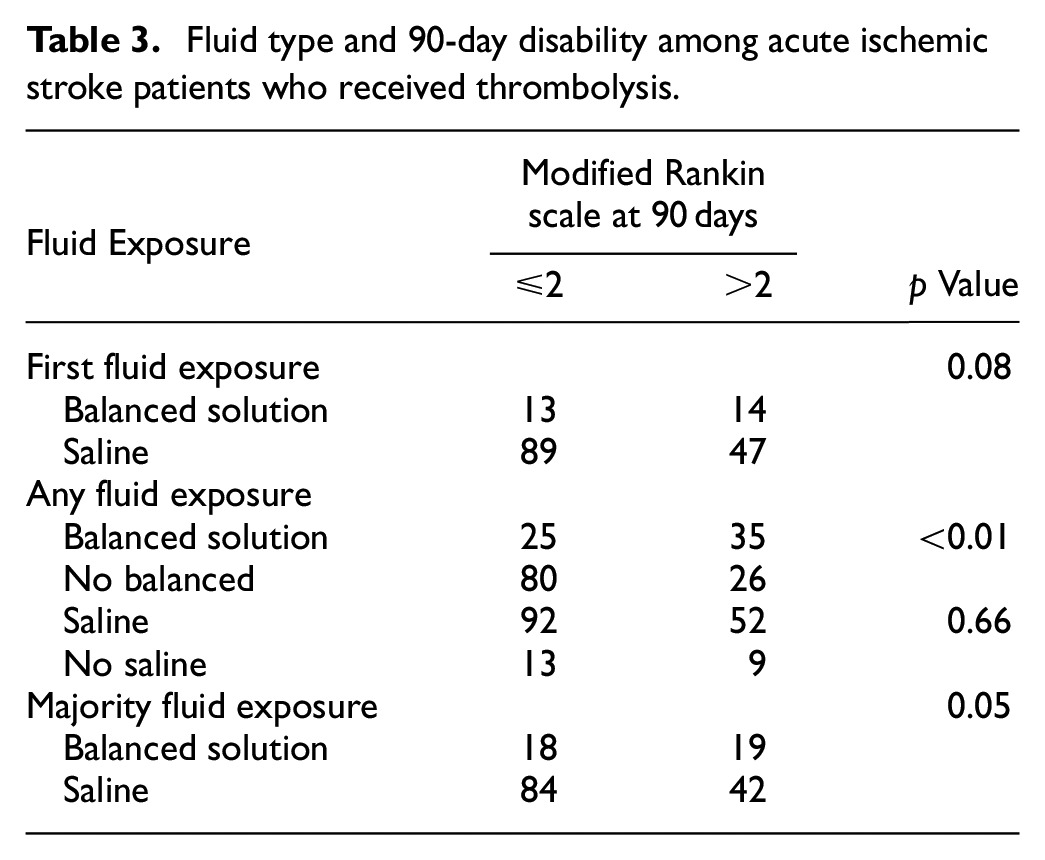
In univariate analysis, exposure to balanced solution at any time during hospital stay was associated with increased disability, that is, mRS >2 at 90 days (OR 4.3, 95% confidence interval (CI) 3.8–4.9, χ2 = 18.8, p < 0.01, Table 1), increased risk for mortality (OR 3.8, 95% CI 1.5–9.5, χ2 = 9.2, p < 0.01, Table 2), and increased risk of hemorrhagic transformation (OR 2.0, 95% CI 1.3–2.2, χ2 = 3.7, p = 0.05, Table 3). Both types of hemorrhagic transformation were higher in those exposed to balanced solutions, with parenchymal hemorrhage (8.1% vs 3.2%, p = 0.06) more so than hemorrhagic infarction (10.3% vs 7.4%, p = 0.36). There was no association between the first type of solution used or the solution used during the majority of hospitalization for hemorrhagic transformation. Exposure to a balanced solution during the majority of the hospitalization was associated with increased disability at 90 days (OR 1.5, 95% CI 1.2–1.8, χ2 = 4.0, p = 0.05) and increased risk for mortality (OR 2.2, 95% CI 1.0–4.9, χ2 = 4.4, p = 0.04).
Fluid type and risk of hemorrhagic transformation among acute ischemic stroke patients who received thrombolysis.
Fluid type and mortality among acute ischemic stroke patients who received thrombolysis.
Fluid type and 90-day disability among acute ischemic stroke patients who received thrombolysis.
Multivariate analysis showed that exposure to a balanced solution at any time during hospitalization was associated with mRS >2 at 90 days (OR 6.3, 95% CI 2.4–17.0, p < 0.01) but not hemorrhagic conversion.
Discussion
This observational study showed that, among acute ischemic stroke patients who received thrombolysis, exposure to a balanced intravenous solution was associated with an increased risk of disability at 90 days and possibly an increased risk of hemorrhagic conversion. This may be related to the osmolarity of the fluids leading to subclinical shifts in free water accumulation in brain tissue. Indeed, in one of the recent randomized trials, the PLUS trial, 3 a subgroup analysis suggested that patients with traumatic brain injury have decreased mortality when saline is used. Another analysis of the SMART trial also suggested saline was associated with improved disability and decreased mortality in patients with subarachnoid hemorrhage. 7
Limitations
Our study has several important limitations. The data presented in our study are limited by its sample size and the fact that it is observational. Our study was completed at a single American academic medical center and may not be generalizable to other populations. Furthermore, the exact amount of each fluid and exposure to “carrier” fluids for medications were not included in our analysis. Not all potential confounders were included in our multivariate analysis; for example, inpatient hypertension control is known to be associated with the risk of hemorrhagic conversion. The mRS, the measure of disability used in our study, is a somewhat subjective measure with interobserver variability. This study was done while thrombolysis was performed with alteplase, and many centers have switched to tenecteplase as the thrombolytic used for acute stroke. Tenecteplase theoretically has a lower risk of hemorrhage overall, and the results may not apply to patients receiving tenecteplase as a thrombolytic. Finally, given the use of intravenous fluid in inpatients is very common, it is possible that small, clinically important differences would not be detected in a study of this size. Future larger randomized studies should be directed at acute ischemic stroke patients to determine which type of intravenous fluid leads to the best outcomes.
Conclusion
Our observational study showed that exposure to balanced solutions is associated with worse outcomes in patients with acute ischemic stroke treated with intravenous thrombolysis. The data would suggest that normal saline is a preferred solution in these patients, though future prospective randomized trials are needed to confirm this finding.
Footnotes
Acknowledgements
To the best of my knowledge, I have no conflicts of interest, financial or other, to declare regarding this manuscript and no competing interests. This work represents the author’s independent analysis of local or multicenter data gathered using the AHA Get With The Guidelines® (GWTG) Patient Management Tool/IQVIA Registry Platform but is not an analysis of the national GWTG dataset and does not represent findings from the AHA GWTG National Program. Portions of this data have been presented at the American College of Emergency Physicians Scientific Assembly in October 2022.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study received approval from the Institutional Review Board of Penn State Milton S. Hershey Medical Center.