
Abstract

Inflammatory Bowel Disease (IBD), encompassing Crohn’s Disease (CD), and Ulcerative Colitis (UC), is characterized primarily by chronic, progressive inflammation of the gastrointestinal tract, affecting an estimated 4.9 million individuals globally. 1 Given its intricate and multifaceted etiopathogenesis, understanding extraintestinal manifestations remains elusive, hindering accurate prognosis and effective management. 2 The complex interaction of immune dysregulation in IBD triggers vicious cycles of inflammatory responses, culminating in extensive tissue destruction and increasing the risk of various cardiovascular diseases (CVD). 3 Factors such as altered collagen metabolism, myocardial atrophy, fibrosis, corticosteroid usage, and chronic inflammation are potentially implicated in precipitating heart failure (HF) in patients with IBD. 4 However, clinical evidence to establish a causal correlation between the two conditions remains contradictory.
The meta-analysis followed the PRISMA 2020 guidelines and was registered with PROSPERO (CRD42024557006). Two authors conducted an extensive and systematic search of the MEDLINE, EMBASE, and Cochrane Central databases to identify observational studies reporting the incidence of HF in IBD patients, covering the period from inception until August 2024. Predefined Medical Subject Headings (MeSH) terms and keywords, such as “Inflammatory Bowel Disease,”“Crohn’s Disease,”“Ulcerative Colitis,”“Heart Failure,” and “Cardiovascular Risk,” were used with Boolean operators “AND” and “OR.” Two authors independently extracted and reviewed the data. The Risk Ratio (RR) was pooled using a random-effects model, and heterogeneity among studies was assessed using the Higgins I2 model. Statistical analyses were performed using RevMan version 5.4.1. A p-value <0.05 was considered statistically significant.
Five observational studies5–9 that met the inclusion criteria were selected, encompassing 430,016 patients with IBD being observed for the occurrence of HF. The study design and baseline patient characteristics are presented in Table 1. The analysis revealed an increased risk of HF among patients with IBD, with a pooled RR of 1.28 (95% CI: 0.67–2.42, p = 0.45, I2 = 100%) (Figure 1(a)), although this finding was not statistically significant. When examining IBD subtypes, UC showed a numerically higher risk but did not reach statistical significance (RR = 1.43, 95% CI = 0.81–2.52, p = 0.21, I2 = 77%; Figure 1(b)). In contrast, CD was associated with a statistically significant risk of HF in our cohort (RR = 1.30, 95% CI = 1.15–1.46, p < 0.0001, I2 = 6%; Figure 1(c)).
Study design and baseline patient characteristics.

CD, crohn’s Disease; IBD, inflammatory bowel disease, UC, ulcerative colitis, NR, not reported.
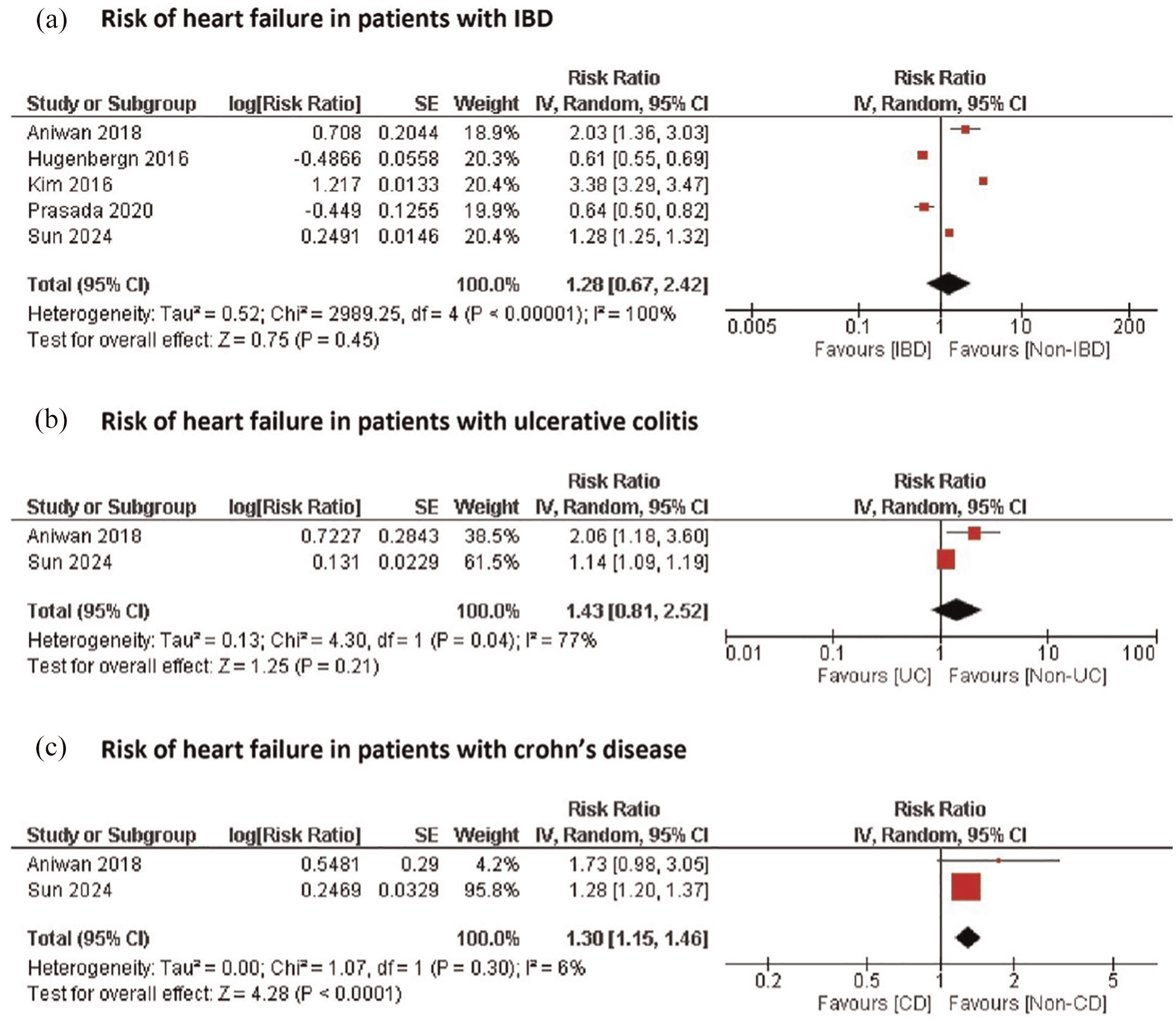
Forest plots showing the risk of heart failure in patients with (a) IBD, (b) Ulcerative colitis, and (c) Crohn's disease.
Our analysis showed a trend toward an increased risk of HF in patients with IBD; however, this association did not reach statistical significance. On subgroup analysis, however, patients with UC were found to have an increased risk of HF. The exact mechanisms underlying the relationship between IBD and HF remain unclear, but persistent systemic inflammation and alterations in the microbiota have been implicated.10,11 This inflammation, characterized by elevated levels of pro-inflammatory cytokines (such as interleukin-1, interleukin-6, and tumor necrosis factor-α) and lipopolysaccharides derived from altered microbiota, promotes endothelial dysfunction. This dysfunction impairs signaling pathways that regulate myocardial hypertrophy, relaxation, and stiffness.12,13 The resulting hemodynamic strain may lead to diastolic dysfunction and adverse left ventricular remodeling, ultimately contributing to HF. 4 In addition, patients with IBD are at a higher risk of acute arterial events and arrhythmias due to the atherosclerotic and arrhythmogenic effects of lipopolysaccharides and pro-inflammatory cytokines, which may further exacerbate HF.14,15 Although systemic inflammation is a well-recognized contributor to HF, reductionist approaches that focus on a single or limited set of inflammatory pathways may fail to capture the diverse inflammatory pathophysiologies underlying HF. 16
The substantial risk seen in CD patients emphasizes the necessity of specific cardiovascular risk assessment and management techniques in this population. First, to identify high-risk groups at an early stage, healthcare providers and patients should be aware of the potential long-term increase in the risk of HF in patients with IBD, particularly those with concurrent cardiovascular comorbidities. Second, regular cardiovascular monitoring and early intervention strategies could be particularly beneficial in mitigating the elevated risk of HF in patients with CD. Third, careful assessment and judicious use of anti-inflammatory therapy for IBD management and remission is warranted, with a focus on drugs with minimal cardiovascular complications. This is especially important when providing drugs with cardiovascular risks (such as steroids and tofacitinib) to IBD patients who have classic HF risk factors.17,18 Finally, our results, together with previous evidence on the effect of IBD on CVD, could be used to develop new guidelines for the assessment and management of CVD, specifically the risk of HF in patients with IBD.
This study has several limitations. First, only five observational studies were included due to insufficient data exploring this association, which may limit the generalizability of our findings. Moreover, the insignificant results could be attributed to the underpowered nature of the outcomes. Second, observational studies are inherently prone to confounding bias. Third, the included studies did not address lifestyle factors, such as diet, physical activity, and smoking, nor did they report the medications patients were taking, all of which could impact the risk and outcomes of HF.
In conclusion, our study demonstrated a trend toward an increased risk of HF in patients with IBD; however, no statistical significance was reached. On subgroup analysis, an increased risk of HF in patients with CD was noted.
Footnotes
Acknowledgements
The authors have no acknowledgments to declare.
Author contributions
All authors reviewed, contributed to, and approved the final version of the manuscript for submission.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
No ethical approval was required for this study design, as all data were obtained from publicly available sources.