
Abstract
Inflammatory bowel disease (IBD), including ulcerative colitis (UC) and Crohn’s disease (CD), is associated with high rates of anxiety and depression, which can significantly influence disease outcomes through the gut-brain axis. This study utilized the National Inpatient Sample (NIS) database (2018–2021) to assess the impact of these psychiatric comorbidities on hospitalization outcomes, including length of stay (LOS), total hospitalization costs (TOTCHG), and mortality. Among 24,584 UC hospitalizations, depression significantly increased LOS (+3.49 days, p < 0.001) and TOTCHG (+$41,480, p< 0.001), whereas anxiety was associated with lower hospitalization costs (−$14,766, p = 0.025) but had no impact on LOS. In 46,117 CD hospitalizations, moderate-to-severe depression (1.08%) led to longer hospital stays (6.92 vs 4.86 days, p < 0.001), higher costs ($68,169 vs $51,981, p = 0.001), and a fivefold increase in mortality risk (OR = 5.05, p = 0.002). Anxiety (2.08%) was associated with a slight increase in LOS (5.83 vs 4.86 days, p < 0.001) but did not significantly impact costs or mortality. In addition, racial and socioeconomic disparities were evident, with Black and Hispanic patients experiencing longer hospitalizations and higher costs, underscoring the need for equitable access to care. These findings highlight the significant burden of psychiatric comorbidities in IBD, particularly the substantial impact of depression on hospitalization outcomes and mortality risk in CD. Integrating mental health support into routine IBD care may improve patient outcomes and reduce healthcare burdens. Further research is needed to develop targeted interventions that address these disparities and optimize treatment strategies.
Keywords
Introduction
IBD, comprising CD and UC, is a chronic gastrointestinal condition that significantly impacts patients’ physical and psychological well-being. Both diseases present with debilitating symptoms such as abdominal pain, diarrhea, and weight loss, leading to substantial reductions in quality of life. In addition to these physical manifestations, psychiatric comorbidities—particularly anxiety and depression—are prevalent in up to 30%–40% of IBD patients. These mental health conditions have been increasingly recognized as contributors to poor disease outcomes, potentially exacerbating intestinal inflammation through the gut-brain axis, a bidirectional communication pathway linking the central nervous system and gastrointestinal tract.1,2
Despite growing awareness of the role of mental health in IBD, its specific impact on hospitalization outcomes—including LOS, TOTCHG, and mortality—remains incompletely understood. Prior studies suggest that anxiety and depression may disrupt disease management by reducing medication adherence, increasing the risk of stress-related flare-ups, and impairing timely decision-making. These challenges are particularly concerning given the unpredictable disease course of CD and UC, which often necessitate frequent hospitalizations and complex treatment regimens. In addition, emerging evidence suggests that psychiatric comorbidities may be linked to poorer clinical outcomes, including prolonged hospital stays, increased healthcare costs, and higher mortality rates, particularly in CD.3,4
This study aims to bridge this knowledge gap by analyzing the National Inpatient Sample (NIS) database from 2018 to 2021 to evaluate the effects of anxiety and depression on hospitalization outcomes in CD and UC. Specifically, it examines how these mental health conditions influence LOS, total hospitalization costs, and mortality in both diseases. By leveraging a large, diverse dataset, this study seeks to identify disease-specific patterns in hospitalization metrics associated with psychiatric comorbidities. These insights may inform strategies for integrating mental health management into routine IBD care, ultimately improving patient outcomes and reducing healthcare burdens.5,6
Methods
We conducted a retrospective analysis using data from the NIS between 2018 and 2021, identifying hospitalizations with a primary diagnosis of CD and UC based on ICD-10 codes. A total of 46,117 CD-related and 24,584 UC-related hospitalizations were included. Moderate-to-severe depression was defined using ICD-10 codes F321, F322, F323, F331, F332, F333, and F339, while Anxiety was identified with code F411 (Supplemental Table 1). These diagnoses were extracted from secondary diagnosis fields, and binary indicator variables were generated for both depression and anxiety. The primary outcomes evaluated were LOS, in days, TOTCHG, in U.S. dollars, and in-hospital mortality. Descriptive statistics were used to compare outcomes between patients with and without psychiatric comorbidities. Unadjusted linear regression models assessed the associations of depression and anxiety with LOS and TOTCHG, while logistic regression was used for in-hospital mortality. Fully adjusted models included covariates for age, sex, race, hospital division, and ZIP code income quartile to evaluate the independent effect of psychiatric comorbidities while accounting for demographic and socioeconomic confounders. All statistical analyses were conducted using Stata/BE version 18.5.
Result
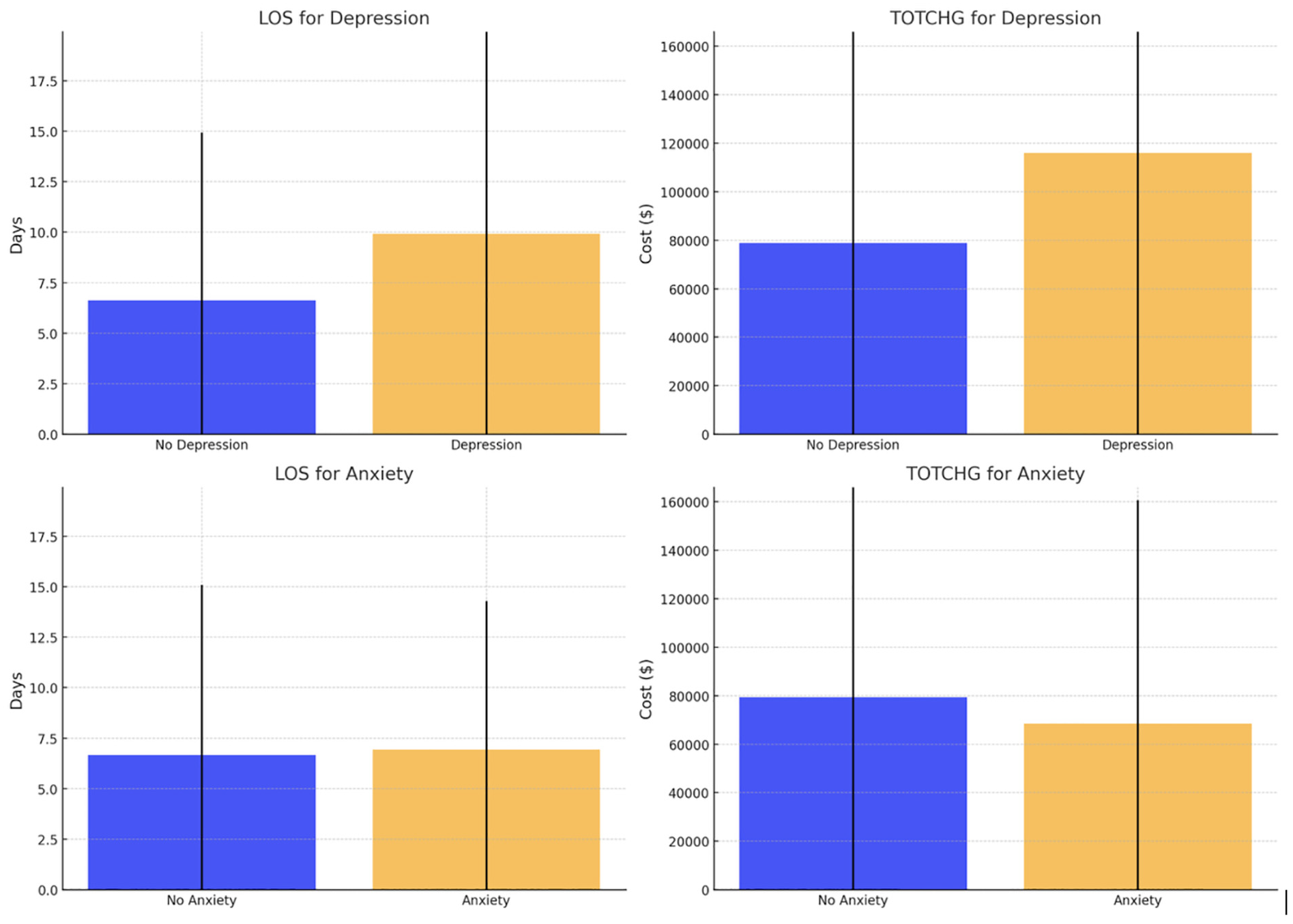
Patients with UC and depression had a significantly longer LOS (9.93 vs 6.63 days) and higher TOTCHG ($115,993 vs $78,795) compared to those without depression (Figure 1). In contrast, patients with anxiety had a slightly longer LOS (6.94 vs 6.66 days) but lower TOTCHG ($68,515 vs $79,415). Depression was associated with a significant increase in LOS (+3.31 days, p< 0.001) and TOTCHG (+$39,513, p < 0.001), while anxiety was linked to reduced TOTCHG (−$14,766, p = 0.025) without affecting LOS. After adjusting for age, sex, race, income, and hospital division, depression remained a significant predictor of increased LOS (+3.49 days, p < 0.001) and TOTCHG (+$41,480, p< 0.001), whereas anxiety showed no significant effects. Key covariates influencing outcomes included age, sex, and hospital division.
After adjusting for age, sex, race, income, and hospital division, depression significantly increased LOS (+3.49 days, p < 0.001) and TOTCHG (+$41,480, p < 0.001), while anxiety showed no significant effects. Age, sex, and hospital division were statistically significant covariates influencing the outcomes in the adjusted models.
Among patients with CD, those with depression had a significantly longer mean LOS (6.92 vs 4.86 days; SD = 11.47 vs 5.52) and higher TOTCHG ($68,169 vs $51,981; SD = $138,429 vs $75,067) compared to patients without depression. The mortality rate was also significantly higher among patients with depression (0.8% (4/500)) than those without (0.2% (92/45,515)). Patients with anxiety had a modestly increased LOS (5.83 vs 4.86 days; SD = 6.68 vs 5.60) and slightly higher TOTCHG ($55,383 vs. $52,089; SD = $71,703 vs $76,150), but no deaths were reported among them.
Adjusted regression analyses confirmed that depression significantly increased LOS (Coefficient = 1.85, p< 0.001), while anxiety also contributed to a moderate yet significant LOS increase (Coefficient = 0.80, p< 0.001). Key factors associated with longer LOS included older age (Coefficient = 0.008, p < 0.001) and race, with Black (Coefficient = 0.43, p < 0.001) and Hispanic (Coefficient = 0.30, p = 0.006) patients experiencing prolonged hospital stays. Regarding total charges, depression was significantly associated with higher costs (Coefficient = $11,389.82, p = 0.001), whereas anxiety had no significant impact (Coefficient =$3,288.48, p = 0.186). Higher charges were also observed among Hispanic patients (Coefficient= $11,532.87, p < 0.001) and those treated in the Pacific region (Coefficient = $36,910.87, p < 0.001).
Mortality analyses revealed that depression significantly increased the odds of death (OR = 5.05, p = 0.002) (Figure 2). Anxiety perfectly predicted survival, leading to its exclusion from the model. Other key predictors of mortality included older age (OR = 1.08, p < 0.001) and income level, with patients in the third income quartile having lower odds of mortality (OR = 0.53, p = 0.041). No significant mortality differences were found across hospital divisions after adjustment.
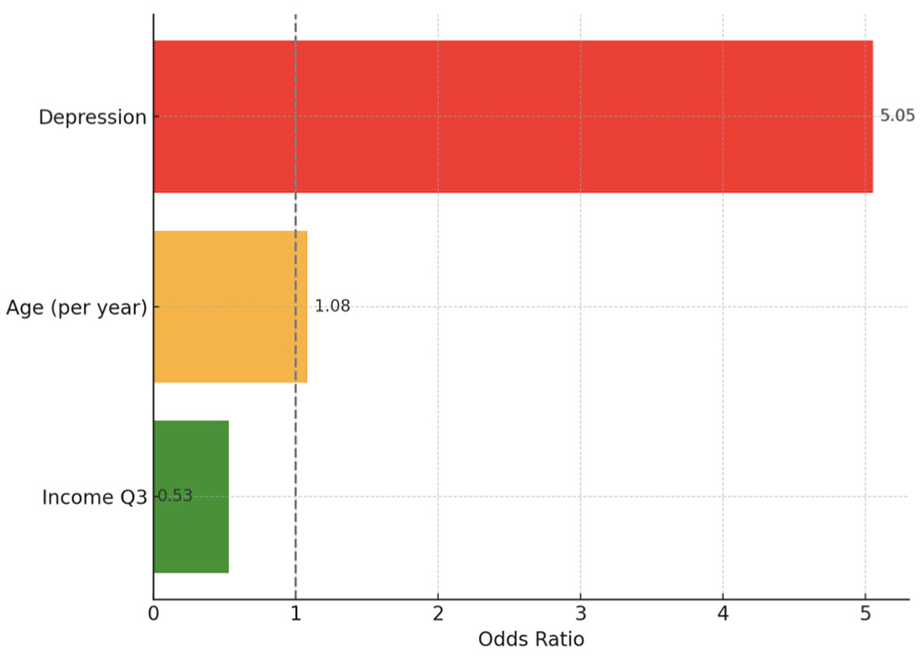
Mortality analyses revealed that depression significantly increased the odds of death (OR = 5.05, p = 0.002).
Discussion
Our study highlights the significant impact of mental health comorbidities, particularly depression and anxiety, on hospitalization outcomes in patients with IBD. We observed that in both UC and CD, moderate-to-severe depression was associated with longer LOS and higher TOTCHG. Notably, in CD patients, depression was linked to a fivefold increase in inpatient mortality risk. Conversely, while anxiety was associated with prolonged LOS in both UC and CD, it did not significantly impact total charges in CD and was unexpectedly linked to lower hospitalization costs in UC.
The observed increase in LOS and TOTCHG in patients with depression aligns with existing literature indicating that depression exacerbates disease activity, reduces medication adherence, and increases healthcare utilization in IBD patients.7,8 The bidirectional relationship between inflammation and mental health may explain these findings, as depression contributes to systemic inflammation via dysregulation of the hypothalamic-pituitary-adrenal axis and increased pro-inflammatory cytokine release, potentially worsening disease severity and hospitalization outcomes.9,10 The substantial increase in mortality risk in CD patients with depression further emphasizes the critical need for early psychiatric intervention in this population. 11
Interestingly, while anxiety was expected to follow a similar trend as depression, our results suggest different mechanisms influencing hospitalization outcomes. In UC patients, anxiety was linked to a slight increase in LOS but unexpectedly lower hospitalization costs. One possible explanation is that patients with anxiety may engage more proactively with outpatient care, reducing the need for costly inpatient interventions.12,13 In CD, while anxiety was associated with prolonged LOS, it did not significantly impact total hospital charges or mortality, suggesting a more nuanced relationship between anxiety and disease burden. 14
Our study also identified racial and socioeconomic disparities in hospitalization outcomes, particularly among CD patients. Black and Hispanic patients experienced significantly longer LOS, while Hispanic patients also incurred higher total charges. Prior studies suggest that minority patients often face diagnostic delays, reduced access to advanced therapies, and worse disease outcomes, which may contribute to these findings.15,16 Furthermore, patients from higher-income ZIP code quartiles incurred greater hospitalization costs, potentially reflecting increased access to specialized care, differences in insurance coverage, or hospital billing variations. 17 Addressing these disparities through equitable access to care and early intervention is crucial for improving outcomes in IBD patients.
Geographic variations in hospitalization outcomes were also observed. In CD, hospitals in the Mountain region were associated with shorter LOS, while those in the Pacific region had the highest total charges, emphasizing the influence of regional healthcare infrastructure and clinical practice patterns on IBD management.18,19
Given the significant impact of mental health on hospitalization outcomes, integrating psychiatric care into IBD management is essential. Targeted psychosocial interventions, early mental health screening, and multidisciplinary care models incorporating gastroenterologists, mental health professionals, and IBD specialists may improve both psychological well-being and disease outcomes.20,21
Limitations of our study include its retrospective design and reliance on administrative coding, which may introduce misclassification biases. In addition, disease severity, treatment regimens, and outpatient care access were not fully accounted for. Future prospective studies incorporating disease activity indices and patient-reported outcomes could provide a more comprehensive understanding of these associations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Ethical approval was not required for this study as it utilized de-identified patient data from the NIS, a publicly available database that adheres to strict privacy and confidentiality guidelines. As this dataset does not include direct patient identifiers, institutional review board approval and informed consent were not necessary.
Informed Consent
Not required. Data obtained from de-identified publicly available database.