
Abstract
Colorectal cancer (CRC) screening guidelines have prioritized age and clinically relevant family history, yet other clinically relevant parameters remain underutilized. Our study investigates the correlation between CRC-related manifestations and screening performance metrics—polyp detection rate (PDR) and adenoma detection rate (ADR). This cross-sectional retrospective study analyzed 235,781 colonoscopy procedures from eight medical centers in Israel conducted between 2016 and 2022. The dataset comprised the identification and classification of polyps, adenomas, and CRC, in conjunction with patient demographics, clinical background, and particular clinical-laboratory manifestations, including hematochezia, abdominal pain, family history of CRC, fecal occult blood results, and presence of anemia. Our study found significant variations in PDR and ADR based on symptom presence. Patients with hematochezia exhibited a PDR of 36.8% and an ADR of 12.1%, compared to 28.7% and 10.8% in those without it. Furthermore, individuals with occult blood in their feces had a PDR of 48.3% and an ADR of 21.5%, respectively, while those without had rates of 31.6% and 11.0%. In addition, having a family history of CRC is also related to a more significant increase in PDR and ADR of 37.7% and 13.8% compared to patients with no family history of CRC, who had PDR and ADR of 33.3% and 12.2%. Moreover, clinical combinations, including CRC family history with hematochezia or occult blood, had the highest PDR of 62.3% and 58.9%, and ADR of 15% and 20.6%, respectively. Incorporating hematochezia and fecal blood occult tests enhances the effectiveness of the CRC screening.
Keywords
Introduction
Around the world, colorectal cancer (CRC) is one of the most significant health issues.1–3 The survival rate for CRC depends on early diagnosis, which could save many lives.4,5 Despite available tools like Fecal Immunochemical Test (FIT) and colonoscopy, CRC screening uptake remains suboptimal, limiting early detection.6,7 Polyp detection rate (PDR) and adenoma detection rate (ADR) are standard indicators of screening quality, reflecting the success of identifying precancerous lesions. 8 These metrics reflect a program’s ability to identify conditions that could lead to cancer before it develops.9,10 This explains why they are often regarded as standards against which screening quality should be measured.9–11 A high ADR and PDR represent tremendous success in finding and removing precancerous lesions to prevent CRC development better through such initiatives. 11
Most current guidelines recommend colonoscopies based primarily on age and family history12–14; however, other manifestations such as hematochezia, abdominal pain, change in bowel habits, anemia, and/or a positive FIT might also be linked to the CRC location.15–20 Research has indicated that there exists a significant correlation between rectal bleeding and an elevated risk of CRC, 21 whereas more than 30% of individuals diagnosed with CRC concurrently experience anemia. 22 Nevertheless, there remains a paucity of investigation regarding the relationship between these clinical symptoms and the prevalence of polyps detected through colonoscopy, explicitly pertaining to advanced neoplasia (PDR and/or ADR). Understanding this relationship can improve screening practices by incorporating symptom-laboratory-based risk assessments into existing guidelines. Several studies have shown that including symptoms in screening protocols may result in early detection and improved outcomes.23,24 Given CRC’s varied presentation, 25 assessing symptom patterns in a large cohort could refine screening and diagnostic strategies. The current study explores the link between common clinical and lab findings in CRC and the detection of polyps and adenomas. We aim to determine whether these factors can serve as reliable indicators for CRC risk in a screened patient cohort.
Materials and methods
Study design and data source
This retrospective cross-sectional study looked at 235,781 colonoscopies performed from 2016 to 2022 in eight medical centers in Israel. We examined polyps, adenomas, patient demographic variables, including age and sex, as well as clinical histories encompassing prior diagnoses of cancer or inflammatory bowel disease; specific manifestations associated with CRC, such as hematochezia or fecal occult blood, were also evaluated in conjunction with other indicators such as abdominal pain and anemia. This comprehensive dataset was utilized to compute the ADR and the PDR. The Institutional Helsinki Ethics Board approved the study at Assuta Medical Center under protocol 0043-22-ASMC.
Statistical analysis
IBM SPSS Statistics (Version 25.0; IBM Corp., Armonk, NY, USA) and GraphPad Prism 9.0 (GraphPad Software, La Jolla, CA, USA) were used for statistical analysis. Categorical variables between groups were compared using the chi-square test. A p < 0.05 was considered statistically significant.
SIGNIFICANCE STATEMENT
WHAT IS ALREADY KNOWN?
Colorectal cancer’s (CRC) current screening guidelines primarily rely on age and family history as the main criteria for colonoscopy recommendations.
Several studies have suggested that symptoms such as rectal bleeding (hematochezia), anemia, and a positive Fecal Immunochemical Test (FIT) are associated with CRC risk. Still, the role of these symptoms in improving risk stratification for CRC screening remains underexplored, and current guidelines do not fully integrate symptom-based risk assessment.
WHAT DOES THIS STUDY ADD?
This study provides large-scale, multicenter, realworld evidence from 235,781 colonoscopies demonstrating that hematochezia, positive FIT, and family history significantly increase polyp detection rate (PDR) and adenoma detection rate (ADR).
The study quantifies the increased PDR and ADR when these symptoms are present, highlighting their predictive value.
The combination of risk factors dramatically increases detection rates, emphasizing the importance of a symptom-based screening approach.
HOW MIGHT THIS STUDY AFFECT RESEARCH, PRACTICE, OR POLICY?
Findings support integrating symptom-based criteria (hematochezia, positive FIT) into CRC screening protocols rather than relying solely on age and family history.
Healthcare providers can use these findings to prioritize high-risk individuals for early colonoscopy screening, improving CRC detection rates.
Screening guidelines may need revisions to incorporate symptom-based stratification.
Results
Demographics and scope of the study population
Our survey consisted of 235,781 colonoscopy records gathered from 2016 to 2022 of 123,241 males (52.3%) and 112,540 females (47.7%) with a mean age of 59.51 years (median: 59.19 years, range: 45.00–74.99 years; Figure 1(a)). CRC presents with a broad spectrum of clinical manifestations, ranging from asymptomatic cases detected through screening to advanced disease with significant symptoms. Our survey reveals excellent variations in the proportion of people with CRC-related symptoms across different patient populations. For instance, hematochezia was observed in 7.5% of patients, while fecal occult blood (patients with a positive FIT) appeared in 9.3%. Abdominal pain was reported in 10.8% of patients, while anemia was diagnosed in 5.7% (Figure 1(b)). In addition, 14.5% showed a family history of CRC.
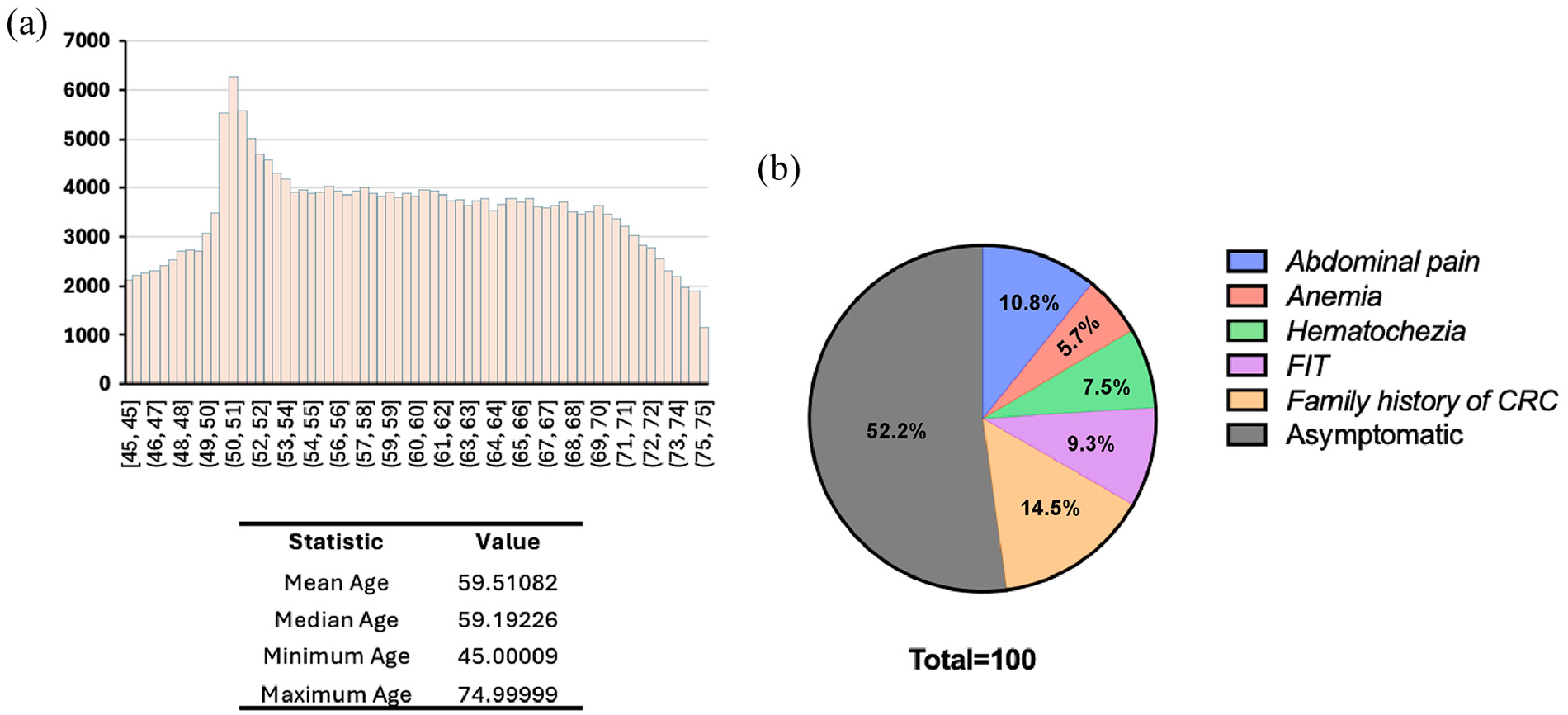
Demographics and scope of the study population. (a) Age distribution of the study population: the histogram represents the number of patients across different age groups who underwent colonoscopy between 2016 and 2022. The mean age is 59.51 years (median: 59.19 years), with an age range of 45.00–74.99 years. (b) The prevalence of clinical parameters related to CRC, presented in the pie chart, illustrates the distribution of FIT-positive patients, abdominal pain, anemia, hematochezia, and a family history of CRC. The study population’s total prevalence of these parameters was 47.8%, and the rest (50.2%) of the patients were asymptomatic.
Hematochezia, occult blood, and a family history of CRC are the strongest predictors of ADR and PDR in CRC screening
Subsequently, we correlated this data with PDR and ADR by stratifying patients into cohorts. Thereafter, we explored PDR and ADR in relation to these cohorts by juxtaposing the outcomes of individuals exhibiting these manifestations against those devoid of them (Tables 1 and 2). Remission colonoscopy effectiveness depends heavily on bowel preparation.8–11 Studies show higher PDR and ADR in patients with adequate prep, while poor cleansing obscures lesions and often requires repeat procedures.8–11 In our research, Picosalax was the most commonly used bowel preparation, administered to 89.6% of patients, with Moviprep (5.8%), Meroken new (4.4%), and Spodex being the least popular (0.2%), as shown in Figure 2(a). The quality of bowel preparation significantly impacts the accuracy of polyp detection and overall procedure success. Of the studied patients, 75.9% received a good grade, 16.9% moderate, and 7% poor (Figure 2(b)). The high percentage of adequate bowel preparation (good/moderate: 92.8%) suggests adequate patient adherence to preparation protocols, which is crucial for minimizing missed lesions and reducing the need for repeat procedures.
PDR in relation to CRC-related manifestations.
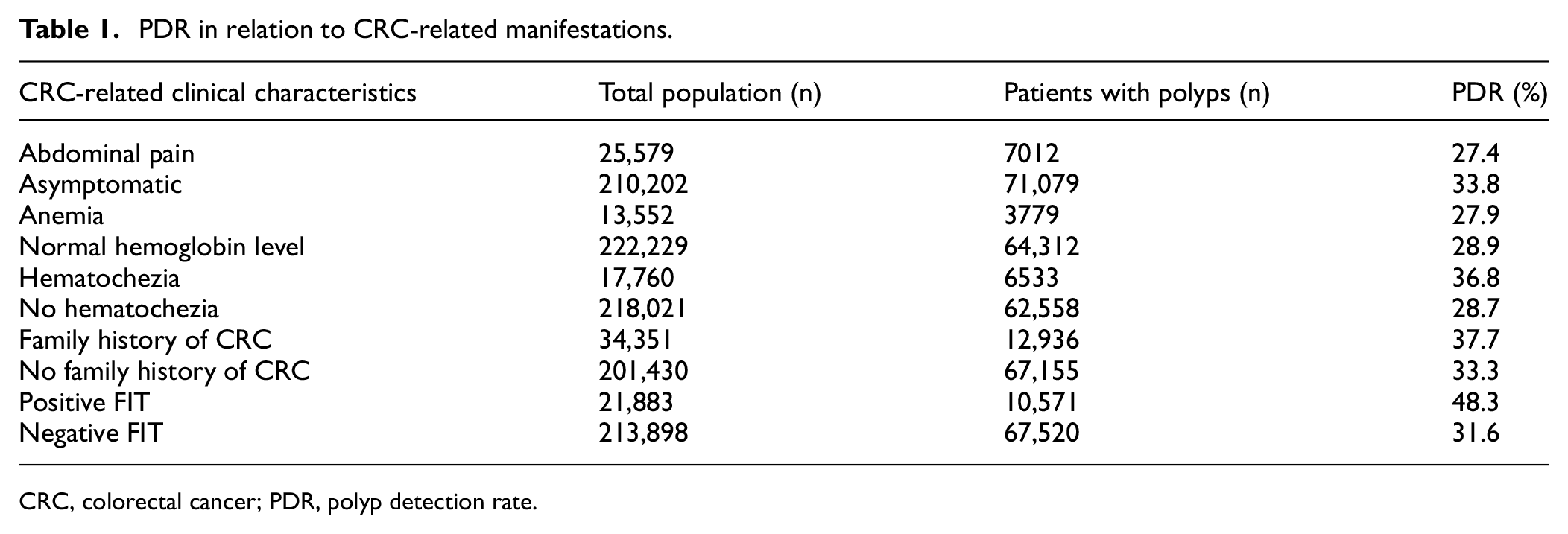
CRC, colorectal cancer; PDR, polyp detection rate.
ADR in relation to CRC-related manifestations.
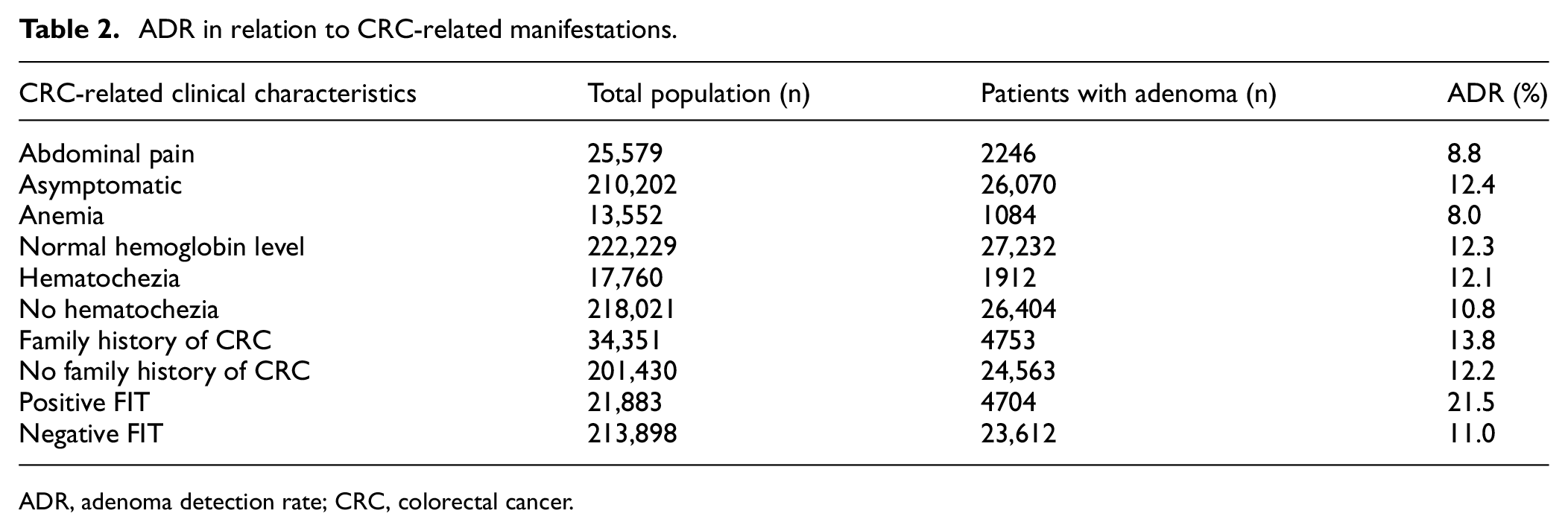
ADR, adenoma detection rate; CRC, colorectal cancer.
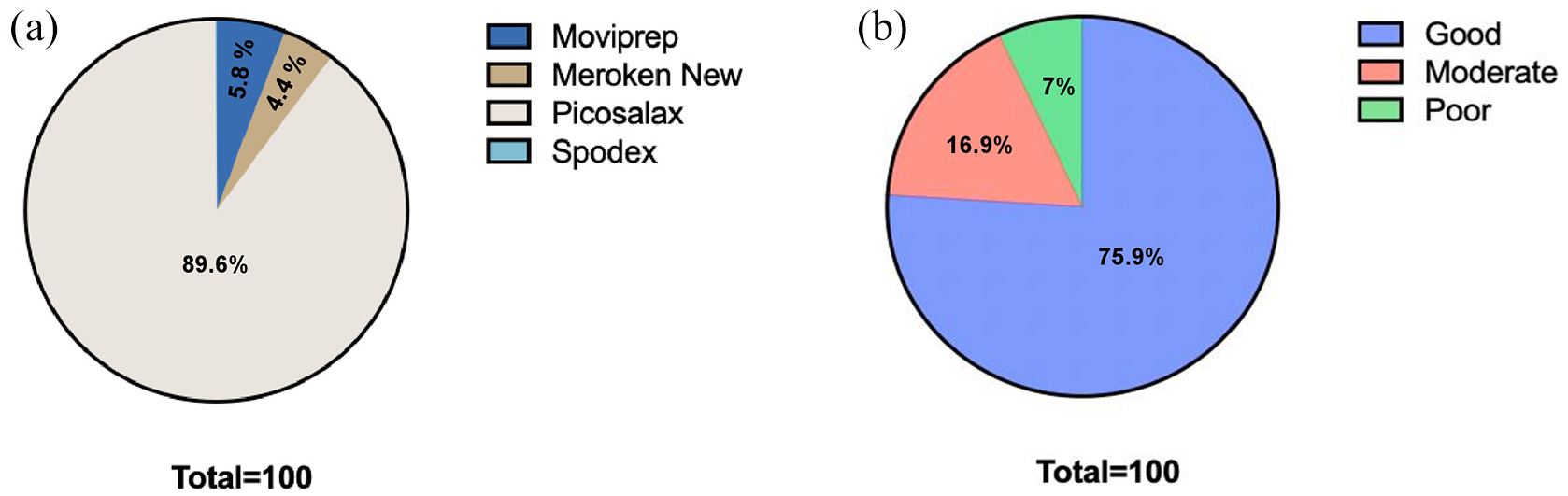
Distribution of (a) bowel preparation types and (b) quality in the study population.
The overall ADR and PDR for the study population were 26% and 32%, respectively. Upon examination of the dataset in relation to the presence of symptoms in Tables 1 and 2, it was observed that patients presenting with hematochezia exhibited an ADR of 12.1% and a PDR of 36.8%, in contrast to non-bleeding patients whose corresponding rates were 10.8% and 28.7%, respectively. Furthermore, patients with a positive FIT had an ADR of 21.5% and a PDR of 48.3%, compared to the alternative cohort, which reported rates of 11% and 31.6%, respectively. Aligned with these results, patients with a family history of CRC had an ADR of 13.8% in addition to a PDR of 37.7% compared to the alternative cohort of 12% and 33.3%, respectively. However, in the context of anemic patients, their respective ADR was documented at 8%, while their PDR was noted at 27.9%, contrasting with non-anemic subjects who exhibited rates of 12.3% and 28.9%. These results were likely to patients complaining about abdominal pain, with ADR of 8%, and PDR recorded at 27.4%; this is juxtaposed with those individuals who did not report abdominal pain, whose rates were evaluated accordingly. The statistical significance of the data is provided in Tables 1 and 2 in the Supplementary Material. The findings suggest that specific manifestations such as hematochezia, positive FIT, and a family history of CRC are associated with a higher probability of ADR and PDR, indicating greater chances of finding adenomas and polyps during colonoscopy and highlighting the integration of clinically based risk assessment into prevailing CRC screening guidelines.
Predictive value of symptom combinations in CRC detection
Further, the PDR and ADR distribution on various combinations of CRC-related manifestations was studied. Our findings in Table 3 suggest that the highest PDR (62.3%) was recorded in patients with a positive family history of CRC and those presenting with hematochezia, which strongly indicates risk for CRC. This was followed by combinations involving FIT, anemia, and abdominal pain reported by patients who had PDRs of 58.9%, 56.2%, and 50.9%, respectively. Thus, it can be stated that these specific symptom clusters are characterized by high levels of cancer detection rates among colonoscopy participants with a familial history of colorectal carcinoma, thus further supporting their role as essential indicators for suggesting early colonoscopic screening practices. Out of all occult blood combinations, a positive FIT plus anemia combination had the highest PDR value of 42.5%, followed by positive FIT with abdominal pain with a PDR of 37.6%. Some other relationships between abdominal pain and anemia (PDR 24.0%), as well as between hematochezia and anemia (PDR 31.1%), had lower values, which in turn resulted from their weaker predictive utility for colon cancer. The statistical significance of the data is provided in Table 3 in the Supplementary Material. Our results emphasize the necessity of integrating clinical risk factors, particularly hematochezia, positive FIT, and family history of CRC, into screening guidelines to enhance early detection and optimize CRC prevention strategies.
PDR by combination of clinical manifestations of CRC.
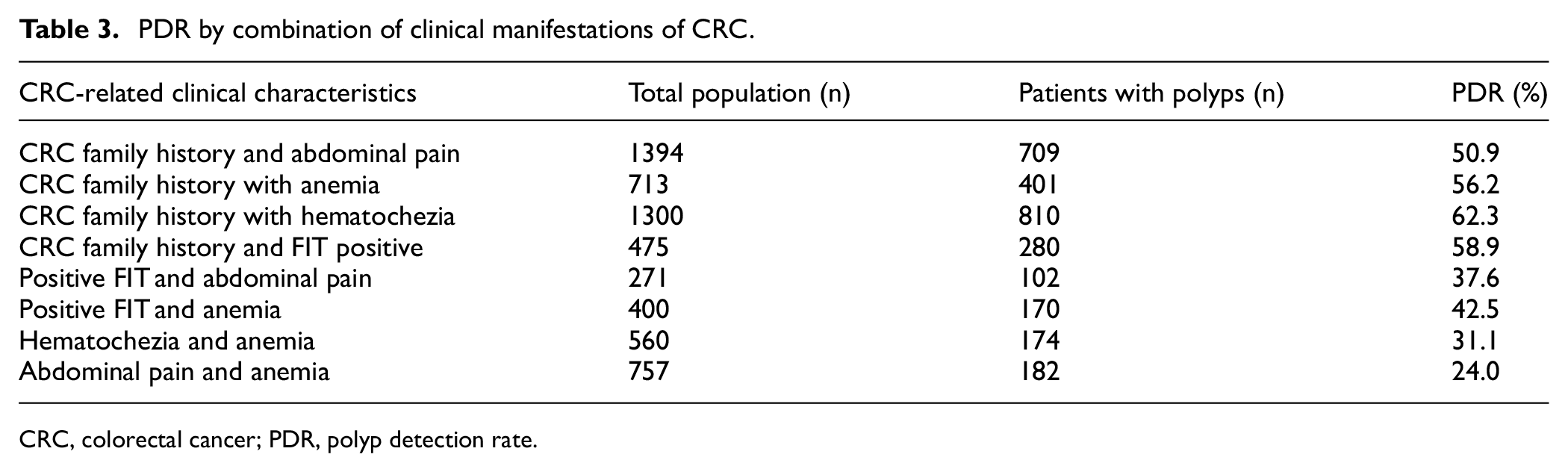
CRC, colorectal cancer; PDR, polyp detection rate.
Identifying potential predictors for CRC is critical in evaluating the ADR associated with the various symptom combinations pertinent to CRC (Table 4). Our findings indicated that the ADR reached its peak (20.6%) in instances where a familial history of CRC was present alongside positive occult blood tests, followed by familial cancer history and the presence of hematochezia, with an ADR of 15%. Another significant finding was seen when a positive FIT result was associated with abdominal pain, leading to an ADR score of 12.2%, and anemia, leading to an ADR score of 11.5%. Similarly, in patients with hematochezia with anemia, the ADR was 11.1%. In contrast, other combinations, such as familial history of CRC alongside anemia (7.7%) and experiencing abdominal pain in conjunction with anemia (7.4%), were correlated with diminished detection rates, thereby indicating a comparatively decreased probability of recognizing adenomatous polyps. Table 4 in the Supplementary Material illustrates the key aspects of the results’ statistical value. The data emphasize the need to integrate crucial symptom clusters such as family history, occult blood positivity, and hematochezia into the guidelines for CRC screening to improve early adenoma detection and increase preventive measures.
ADR by combination of clinical manifestations of CRC.
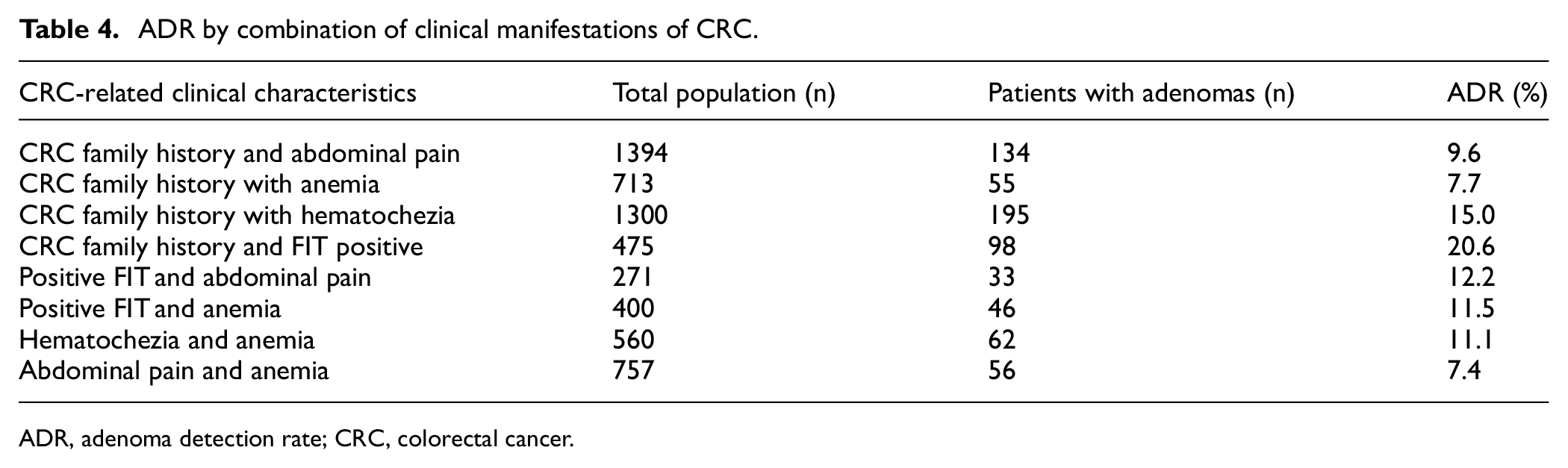
ADR, adenoma detection rate; CRC, colorectal cancer.
Discussion
Our study evaluated the link between specific CRC-related symptoms and screening effectiveness via PDR and ADR. We found that hematochezia, positive FIT, anemia, abdominal pain, and family history of CRC were associated with higher PDR and ADR, suggesting their value in targeted CRC screening. Notably, hematochezia and FIT positivity showed significantly higher detection rates, supporting prior studies identifying them as key CRC predictors.14–19 The significantly higher PDR observed in patients with a positive FIT and hematochezia compared to those without it underscores the potential utility of integrating this model risk assessment into existing screening protocols. In addition, we have pointed out the family history, which is crucial in assessing the CRC risk. CRC family history patients have increased PDR and ADR, in particular when these are combined with fecal occult blood and also with hematochezia. This supports existing guidelines that recommend earlier and more frequent screening for individuals with a family history of CRC. The current study suggests that incorporating other parameters, besides those family profiles, into CRC screening guidelines could improve patient outcomes. A symptom-based approach would allow clinicians to offer screening to high-risk individuals who do not meet the standard age criteria. Most importantly, the enormous decline in both PDR and ADR that is associated with the other symptoms and signs, including abdominal pain and anemia, is primarily due to the absence of additional high-risk factors, which would suggest that these signs in question can be of poor CRC prognostic value when considered in isolation. Notwithstanding these considerations, these factors should not be overlooked because they could indicate other gastrointestinal pathologies that need more evaluation.
In addition, this analysis stresses the role of combining various symptoms in CRC gastroenterological screening and illustrates the essence of considering clinical risk determinants in screening protocols. The study shows that a family history of CRC with hematochezia and a positive FIT score has the highest PDR and ADR, which indicates that it is the strongest predictor of CRC. This is in support of the other reports that have found that CRC-predisposed individuals with a field of rectal bleeding should be screened with a colonoscope at an earlier age. Our results argue the case for incorporating hematochezia, a positive FIT, and a family history of CRC into CRC screening guidelines to promote early diagnosis and better preventive measures. One of the strengths of this study is the illustrative sample, which includes many patients of different backgrounds, which has broader implications for the results. The dataset is also robust because it is multicentered and multiyear, making it helpful in examining multiple factors and their correlation with CRC epidemiology. Although many factors contribute to CRC detection rates, the ADR may be lower due to incomplete data in many cases where the results of adenoma findings are absent. When results are lacking, it confounds the overall data, making the prevalence rate of CRC detection appear less than it is.
Our analysis underscores the importance of thorough CRC risk assessment, including factors such as family history, hematochezia, and occult blood. Lab-based parameters should be integrated into screening protocols to support early diagnosis and better care. Further research is needed to refine the model and assess its impact on screening outcomes and mortality.
Supplemental Material
sj-docx-1-imj-10.1177_10815589251346964 – Supplemental material for Beyond age and family history: Symptoms as predictors in colorectal cancer screening
Supplemental material, sj-docx-1-imj-10.1177_10815589251346964 for Beyond age and family history: Symptoms as predictors in colorectal cancer screening by Majd Khader, Rimon Artoul, Jorge-Shmuel Delgado, Moshe Ben Artzi and Abu-Freha Naim in Journal of Investigative Medicine
Footnotes
Acknowledgements
Not applicable.
Author contributions
MK and RA: supervise, conceptualize, conduct formal analysis, and write the original draft. J-SD: software, validation. MBA and NA-F: visualization and curation. All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This study was conducted in accordance with the principles outlined in the Declaration of Helsinki and approved by Assuta Medical Center’s Helsinki Ethics Board (approval number: 0043-22-ASMC). The requirement for informed consent was waived by the IRB due to the retrospective design of the study and the use of de-identified data in compliance with national regulations and the Declaration of Helsinki.
Declaration of generative AI and AI-assisted technologies in the writing process
During the preparation of this work, the author(s) used Grammarly as a sophisticated artificial intelligence system built to analyze and improve sentences written in English.
Availability of data and materials
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.