
Abstract
This study aimed to evaluate the mediating role of depressive symptoms on asthma and the risk of mortality. We employed the distribution-of-product method to test whether depressive symptoms had a mediating effect on the association between asthma and risk of mortality. The 95% confidence interval (CI) of the distribution of the product was obtained. A weighted multivariable Cox regression model was used to analyze the correlation between asthma and all-cause mortality and verify the mediating impact of depressive symptoms on the association between asthma and risk of mortality. Odds ratio (OR), hazard ratio (HR), 95%CI, and percentage mediated were effect size. The mean follow-up time of all participants was 99.45 months. The percentage of subjects with depressive symptoms in the death group was 23.67%, and in the alive group was 16.65%. The risk of depressive symptoms was heightened in people with asthma (OR = 2.03, 95%CI: 1.82–2.27). Asthma was found to increase the risk of all-cause mortality (OR = 1.18, 95%CI: 1.06–1.31). The distribution of the product for the mediating effect of depressive symptoms on the relationship between asthma and all-cause mortality was 0.08 (95% CI: 0.01–0.16), with the 95% CI not including 0, indicating that depressive symptoms played a mediating role in this relationship. The indirect effect was 1.09(95%CI: 1.01–1.18), and the percentage of asthma’s impact on all-cause mortality mediated by depressive symptoms was 11.11%. Depressive symptoms mediated the association of asthma and all-cause mortality.
Introduction
Asthma is a common chronic noncommunicable disease characterized by inflammation of the airways, variable airflow obstruction, and bronchial hyperresponsiveness. 1 According to epidemiological data, asthma affects more than 3 billion people worldwide, resulting in increased medical expenditure and premature death. 2 The Global Burden of Disease (GBD) study reported that there were about 339 million individuals affected by asthma in 2016, and this may increase to 400 million by 2025, resulting in a high burden of disability.3,4 Evidence reported that about 10,000 people die from asthma each year in the USA, with a higher mortality rate in adults than in children, especially in those older than 65 years.5,6 Therefore, identifying more reliable markers to improve the prognosis for asthma patients is of great value.
Depression is the most common mental disorder, leading to an increased all-cause and cardiovascular disease (CVD)-related mortality risk.7–9 Former studies have demonstrated that depression is also common in asthma patients, with a significantly higher risk of depression compared to individuals without asthma.10,11 People with asthma are at a high susceptibility to emotional disorders, even in cases where their symptoms are effectively managed. 12 The prevalence of depression among asthma patients reached as high as 24.5%. 13 Previous studies suggested that inflammation might be an important mechanism linking asthma to depression.14,15 Asthma and/or its treatment might affect hippocampal chemistry and hippocampal metabolites, which were reported to be the potential mechanisms of depressive symptoms.16,17 Depression might lead to reduced bronchodilator use, asthma control, and quality of life in asthma patients.18–20 In addition, numerous studies have indicated that the mortality risk is significantly heightened for asthma patients with depression.21,22 Several researchers have explored how depression may mediate the correlation between chronic lung diseases and mortality, aiming to develop targeted interventions that effectively manage these diseases and prevent adverse outcomes.23,24 Therefore, we speculate that depression might mediate the association between asthma and mortality. However, no studies have specifically evaluated whether depression serves as a mediator in the relationship between asthma and mortality.
This study intended to assess the correlation among asthma, depressive symptoms, and the risk of mortality based on the National Health and Nutrition Examination Survey (NHANES). It also analyzed whether depressive symptoms had a potential mediating role in asthma and mortality risk.
The percentage of subjects with depressive symptoms in the death group was 23.85%, and in the alive group was 18.11%;
Asthma is a common chronic noncommunicable disease characterized by inflammation of the airways, variable airflow obstruction, and bronchial hyperresponsiveness;
The distribution of the product for the mediating effect of depressive symptoms on the relationship between asthma and all-cause mortality was 0.14, with the 95% CI not including 0, indicating that depressive symptoms played a mediating role in this relationship.
Our study’s findings may provide valuable guidance for future research aimed to elucidate the potential pathways linking asthma to mortality risk. The ultimate goal is to enhance asthma management and reduce mortality risk.
Materials and methods
Study design and population
The present cohort study assessed the data of 39,749 people aged ≥20 years from NHANES from 2005 to 2018. The NHANES is a population-based survey specifically designed to gather comprehensive information on the health and nutrition of the U.S. household population. Data were meticulously collected through structured interviews in participants’ homes, thorough physical examinations at mobile centers, and finally complemented with precise laboratory tests. This study was crafted utilizing a multistage probability sampling methodology. 25 In our study, we included participants aged ≥20 years who had assessed asthma and depressive symptoms within the NHANES database. Participants without key covariates or survival data were excluded.
Potential covariates and definitions
Age (years), marital status (married, never married, or others), education ( below high school, high school, college or above), gender (male or female), poverty-to-income ratio (PIR) (<1.0 or ≥1.0), race (non-Hispanic Black, non-Hispanic White, or others), smoke or not, drink or not, physical activity (<450 MET × min/week or ≥450 MET × min/week), complicated with diabetes, hypertension, dyslipidemia, CVD, chronic obstructive pulmonary disease (COPD), cancer, or chronic kidney disease (CKD) or not, receiving antipsychotics, or corticosteroids or not, body mass index (BMI, not obese <30 kg/m2 or obese ≥30 kg/m2), total energy (kcal), and the Mediterranean Diet (MED) score were potential covariates in this study.
Physical activity from the questionnaire in the database was utilized to estimate energy expenditure. Energy expenditure [metabolic equivalent (MET) × min] was calculated by multiplying the recommended MET value by the corresponding exercise duration (in minutes). This information could be further converted into weekly energy consumption. The definition of CVD was based on the response to the inquiry “Have you ever received a diagnosis of (congestive) heart failure, coronary heart disease, angina/angina pectoris, heart attack, or stroke?” Individuals with CVD included those who had any of these conditions or were taking medications for CVD. CKD was defined as urinary albumin-to-creatinine ratio >30 mg/g and/or estimated glomerular filtration rate (eGFR)<60 mL/ min/1.73 m2 according to the “KDIGO 2021 Guidelines.” 26 The MED score is determined by assigning values of “0,”“1,” or “2” to nine food categories, namely vegetables, legumes, fruits, nuts, fish, red and processed meats, alcohol, whole grains, and olive oil. Higher scores indicate a stronger adherence to the Mediterranean dietary pattern; the total score was 18.27,28
Main and outcome variables
Asthma and depressive symptoms were the main variables. Asthma was defined in line with the responses to questions “Ever been told you have asthma?” and “Still have asthma?” Individuals who answered both “yes” to these questions were considered to have been diagnosed with asthma by a physician.
Depressive symptoms were assessed using the Patient Health Questionnaire-9 (PHQ-9), which was conducted during the face-to-face Mobile Examination Center (MEC) interview. Participants were asked to rate their experiences over the past 2 weeks on a scale of 0 to 3 for the following symptoms: (1) anhedonia, (2) depressed mood, (3) sleep disturbances, (4) fatigue, (5) changes in appetite, (6) low self-esteem, (7) difficulties with concentration, (8) psychomotor disturbances, and (9) suicidal ideation. The total score was 27, and a score ≥10 indicates clinically depressive symptoms. 29
The outcome of the study was all-cause mortality, and the follow-up period concluded in December 2019.
Mediating analysis
The weighted univariable and multivariable logistic regression models were first established to assess the correlation between asthma and all-cause mortality, as well as to verify the mediating role of depressive symptoms in this correlation. Model 1 was the univariable logistic regression model, and Model 2 was the multivariable logistic regression model, if not stratified, adjusting for age, gender, race, education, PIR, smoking, drinking, diabetes, hypertension, dyslipidemia, CVD, CKD, cancer, corticosteroids, BMI obese, total energy, and MED score. Then the mediating effect of depressive symptoms on the correlation between asthma and mortality was evaluated via the distribution-of-product method. 30 The method provided a more accurate estimate of indirect effects, particularly with large sample sizes, and it was effective when the product of coefficients did not follow a normal distribution. The 95% confidence interval (CI) of the distribution-of-product, indirect effect, and percentage mediated could be obtained from the RMediation software package. If the CI of the distribution of the product did not contain 0, it indicated that the mediating effect was significant. The mediating role of depressive symptoms on the correlation between asthma and mortality was evaluated via the indirect effect and total effects.
Statistical analysis
Quantitative data were expressed as Mean (standard error) [Mean (SE)], and an independent sample t-test was employed for comparison of groups. Categorical data were presented as n (%) and the Rao-Scott chi-square test was used for comparison of groups. The missing values for variables were considered to be missing at random, as detailed in Supplementary Table 1. Variables including PIR, physical activity, and COPD had more than 5% missing values, and their missing values were categorized into the unknown group. Other variables with less than 5% missing data were dealt with using multiple interpolation methods via the miceforest package in Python. The imputation model included all variables relevant to the analysis, such as asthma, depression, mortality, age, gender, race, education, smoking, drinking, diabetes, hypertension, dyslipidemia, CVD, CKD, cancer, corticosteroids, BMI, total energy, and MED score. A sensitivity analysis was performed to compare the data before and after missing values imputation. No significant differences were found between the data sets pre- and post-imputation (Supplemental Table 2). Akaike’s information criterion (AIC) was implemented to identify the confounding factors correlated with all-cause mortality, using the stepwise Logit function in the R StepReg package and setting select= “AIC.” Finally, confounding factors including age, gender, race, education, PIR, smoking, drinking, diabetes, hypertension, dyslipidemia, CVD, CKD, cancer, corticosteroids, BMI obese, total energy, and MED score were identified and adjusted in the weighted multivariable logistic regression model. Odds ratio (OR), 95% CI, and percentage mediated were the effect size. The P*adjust () function of the R language was used for FDR correction, method=“BH.” FDR was calculated using the Benjamini-Hochberg (BH) method as follows: (1) Arrange all P-values in ascending order. The P-value is denoted as P, and the ordinal number of the P-value is denoted as rank(1,… .,i), and the total number of P-values is denoted m; (2) FDR(i) = P(i)*m/I; (3) According to the value of i from large to small, execute FDR(i)=. All statistical analysis was conducted using a two-sided test with α of 0.05 via SAS 9.4 (SAS Institute Inc., Cary, NC, USA). The mediating effects were analyzed and plotted using R 4.0.3 software.
Results
Comparisons of the data of participants alive or dead
In total, the data of 39749 participants ≥20 years old were collected. Among them, people without data on asthma (n = 2078), depressive symptoms (n = 4869), and survival information (n = 586) were excluded. Also, those without key covariates, including marital status (n = 19), BMI (n = 363), and cancer (n = 23) were not involved in. Finally, 31,811 individuals were involved. The flow chart of the participant’s screening is shown in Figure 1.
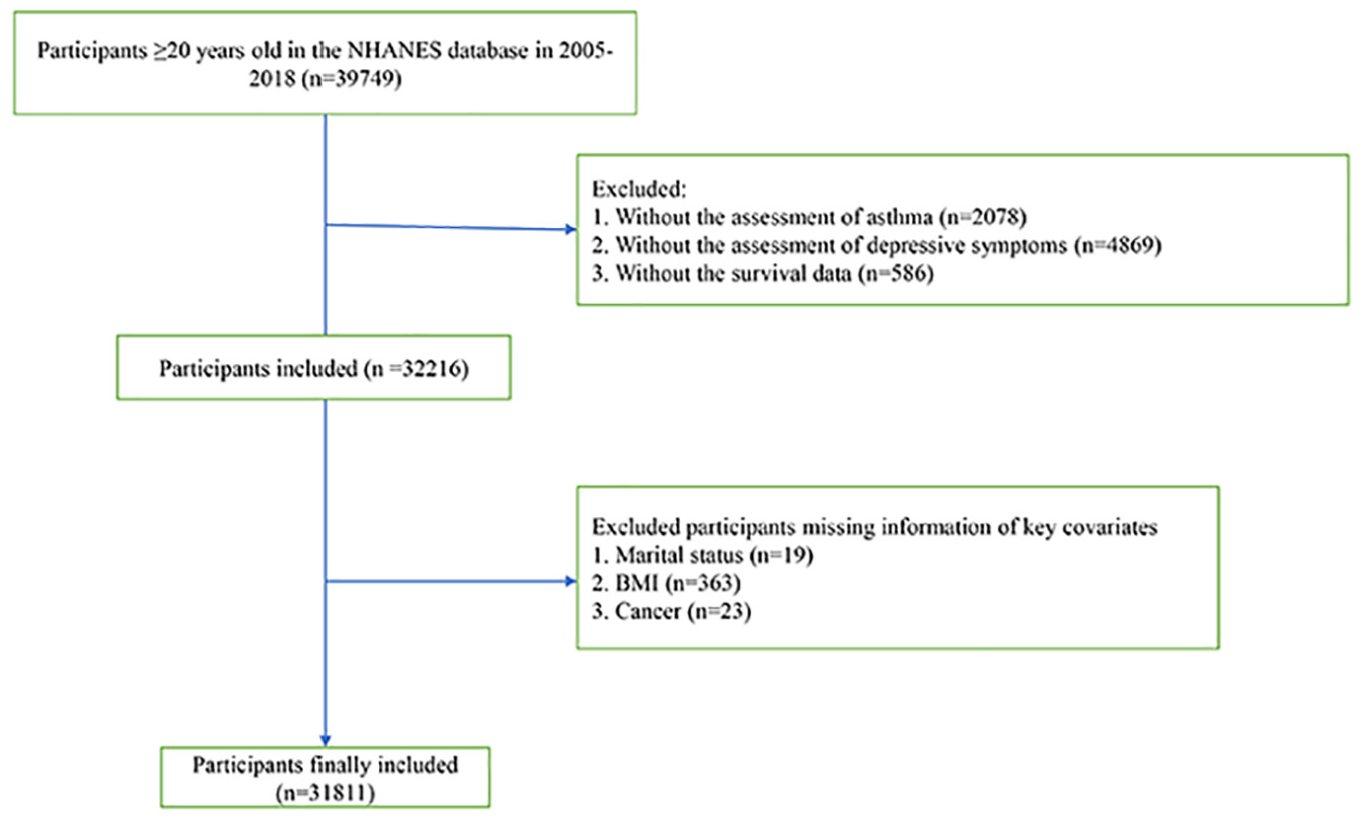
The screening process of the participants.
The total energy in the dead group was lower than the alive group (2023.78 kcal vs 2195.94 kcal). The percentage of asthma people in the death group was higher than in the alive group (21.57% vs 15.51%). The percentage of depressive symptoms among people in the death group was higher than in the alive group (23.67% vs 16.65%) (Table 1).
Comparisons of the characteristics of participants alive or dead.

S. E, standard error; PIR, poverty-to-income ratio; CVD, cardiovascular disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; BMI, body mass index.
The association between asthma and depressive symptoms
According to Table 2, confounding factors including age, gender, race, education, PIR, smoking, drinking, diabetes, hypertension, dyslipidemia, CVD, CKD, cancer, corticosteroids, BMI obesity, total energy, and MED score were identified. In the crude model, asthma might be related to elevated depressive symptoms risk (OR = 2.74, 95%CI: 2.48–3.02). The risk of depressive symptoms was elevated in people with asthma after adjusting for confounding factors (OR = 2.03, 95%CI: 1.82–2.27). Subgroup analysis revealed that in subjects aged ≥45 years (OR = 2.28, 95%CI: 2.02–2.57), or aged <45 years (OR = 1.67 95%CI: 1.38–2.03), with BMI ≥30 kg/m2 (OR = 2.07, 95%CI: 1.78–2.40), or BMI <30 kg/m2 (OR = 2.01, 95%CI: 1.74–2.33), asthma was correlated with a higher likelihood of experiencing depressive symptoms (Table 3).
AIC identifying potential covariates.

AIC, Akaike’s information criterion; Ref, reference; OR, odds ratio; CI, confidence interval; PIR, poverty-to-income ratio; CVD, cardiovascular disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; BMI, body mass index.
The association between asthma and depressive symptoms.
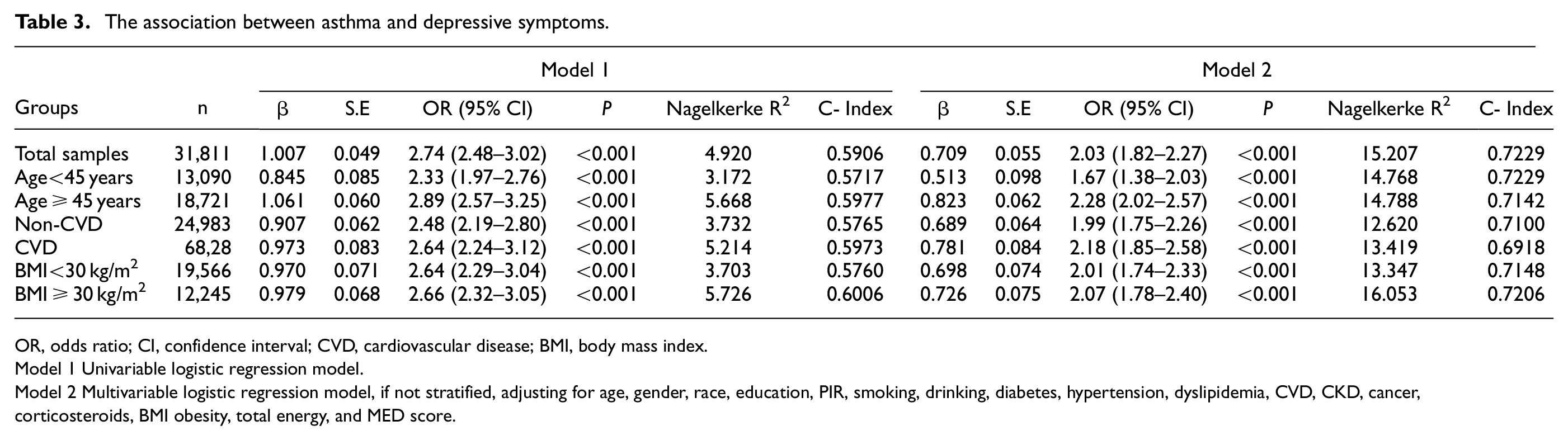
OR, odds ratio; CI, confidence interval; CVD, cardiovascular disease; BMI, body mass index.
Model 1 Univariable logistic regression model.
Model 2 Multivariable logistic regression model, if not stratified, adjusting for age, gender, race, education, PIR, smoking, drinking, diabetes, hypertension, dyslipidemia, CVD, CKD, cancer, corticosteroids, BMI obesity, total energy, and MED score.
Depressive symptoms mediating on the correlation between asthma and all-cause mortality
According to Table 4, asthma was related to elevated all-cause mortality risk (OR = 1.18, 95%CI: 1.06–1.31). The increased odds of all-cause mortality were also observed in people with asthma aged ≥45 years (OR = 1.26, 95%CI: 1.12–1.42), complicated with CVD (OR = 1.23, 95%CI: 1.05–1.45), and with BMI <30 kg/m2 (OR = 1.24, 95%CI: 1.06–1.45).
The mediating role of depressive symptoms on the association between asthma and all-cause mortality.
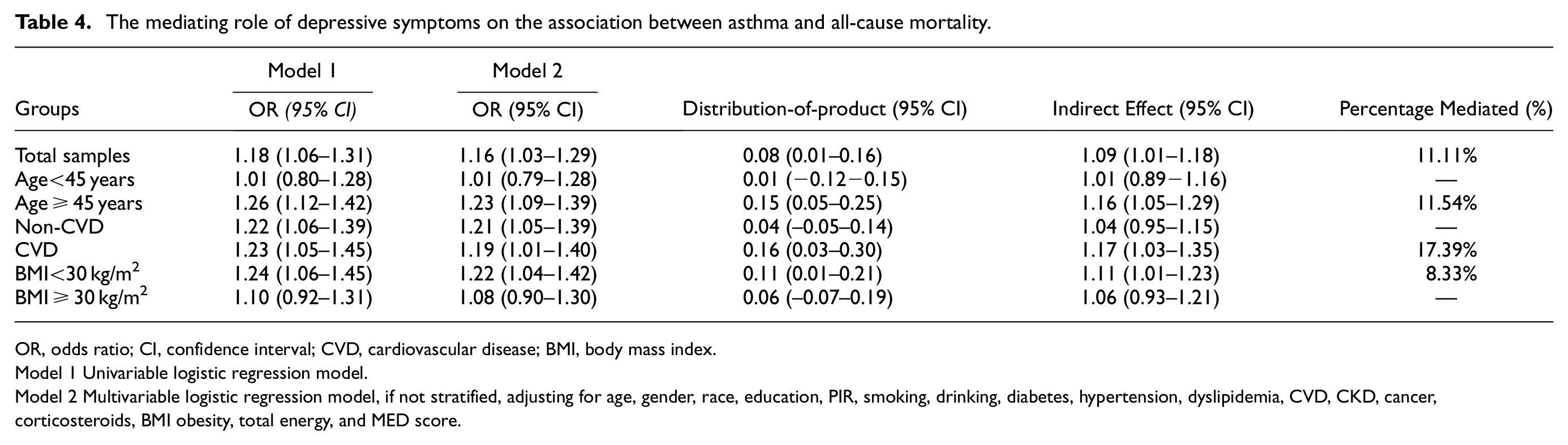
OR, odds ratio; CI, confidence interval; CVD, cardiovascular disease; BMI, body mass index.
Model 1 Univariable logistic regression model.
Model 2 Multivariable logistic regression model, if not stratified, adjusting for age, gender, race, education, PIR, smoking, drinking, diabetes, hypertension, dyslipidemia, CVD, CKD, cancer, corticosteroids, BMI obesity, total energy, and MED score.
As exhibited in Supplementary Table 3, there was no interaction effect between asthma and depressive symptoms on all-cause mortality. The analysis indicated that the mediating role of depressive symptoms in the correlation between asthma and all-cause mortality had a distribution product of 0.08 (95%CI: 0.01–0.16), and the 95%CI did not include 0, verifying depressive symptoms played a mediating role in the association between asthma and all-cause mortality. The indirect effect was 1.09 (95%CI: 1.01–1.18), and the percentage of the effect of asthma on all-cause mortality mediated by depressive symptoms was 11.11%.
In people aged ≥45 years, depressive symptoms mediated about 11.54% of the correlation between asthma and all-cause mortality. In people complicated with CVD, depressive symptoms mediated about 17.39% of the correlation. In people with BMI<30 kg/m2, depressive symptoms are mediated about 8.33% of the correlation (Figure 2).
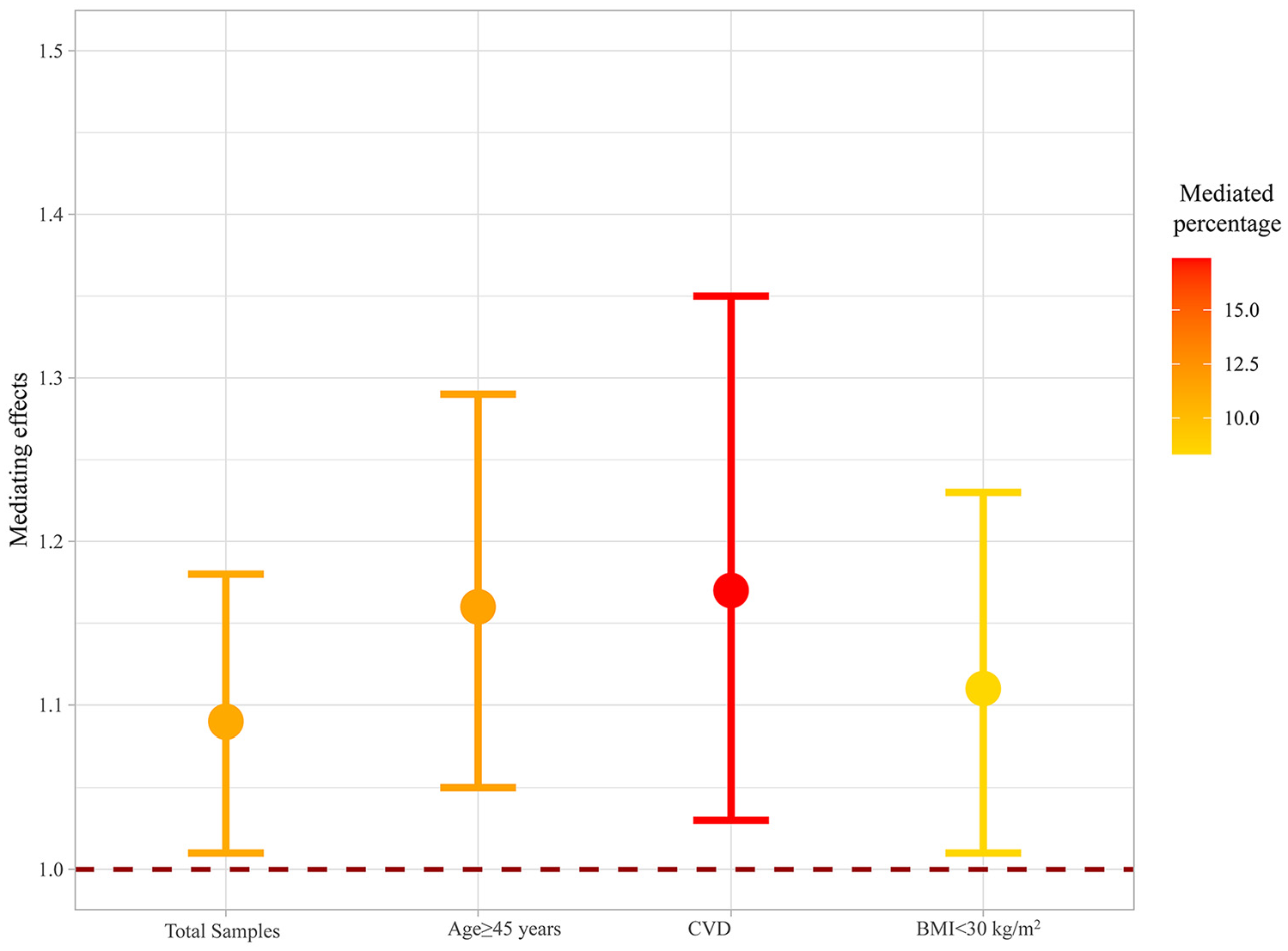
The mediating role of depressive symptoms on the association between asthma and all-cause mortality in subgroups.
Discussion
The present study analyzed the correlation between asthma, depressive symptoms, and the risk of mortality, and the mediating role of depressive symptoms on the correlation of asthma and the risk of mortality was also analyzed. The results indicated that asthma was related to an increased risk of depressive symptoms and all-cause mortality. Depressive symptoms mediated the association of asthma and all-cause mortality. Our study’s findings may provide valuable guidance for future research aimed to elucidate the potential pathways linking asthma to mortality risk. The ultimate goal is to enhance asthma management and reduce mortality risk.
Growing numbers of studies have stated that patients with asthma are at a higher risk of depression. The prevalence of anxiety was observed in 54.3% of asthma patients, while depression was identified in 50.6%, indicating that over half of asthmatic patients experience comorbid anxiety and depression. 31 The results of a previous study utilizing Beck’s Depression Inventory (BDI) as well as the State-Trait Anxiety Inventory (STAI) indicated that individuals with asthma exhibited significantly higher state anxiety scores compared to healthy controls. 12 The study conducted by Choi et al. revealed a significantly elevated hazard ratio (HR) for depressive disorders in patients with asthma compared to those without asthma. 11 These findings gave support to our study, which showed that asthma patients were at a higher risk for depressive symptoms. Previous studies have analyzed potential reasons for this connection. Hou et al. showed that severe asthma patients were related to elevated levels of anxiety and depression, and suggested that inflammatory responses might be an underlying factor contributing to this comorbid condition. 32 Asthma and its comorbid conditions often share common risk factors, and there is some evidence suggesting that they involve shared inflammatory pathways that exacerbate asthma symptoms. Inflammation plays a crucial part in the initiation and development of various comorbidities. 33 And inflammatory response may be an important mechanism connecting asthma and depression.10,11 A growing body of evidence indicates potential shared dysfunctions in the immunologic, endocrine, and peripheral nervous systems between depression and asthma.34,35 Asthma phenotypes exhibit heightened proinflammatory states at baseline, in response to noxious stimuli, and during exacerbations. 36 Treatment with proinflammatory cytokines has been documented to be associated with the onset of depressive symptoms in humans. 37 Systemic and inhaled glucocorticoids for asthma may exert direct modulatory effects on the hypothalamic-pituitary-adrenal (HPA) axis. Genetic abnormalities of the HPA axis have been linked to steroid-resistant asthma. In addition, dysregulation of the HPA axis has also been observed in animal models of major depressive disorder (MDD) and stress-induced depression.35,38
Despite the finding of the association between asthma and depressive symptoms, another notable finding in our study was that depressive symptoms mediated the correlation between asthma and all-cause mortality. The previous evidence has indicated a high prevalence of anxiety and depression among patients with asthma, which is associated with an increased frequency of exacerbations, heightened utilization of healthcare resources, and suboptimal control over asthma symptoms. 39 In addition, asthma patients with depression generally report a lower quality of life related to their respiratory health. They experience more disease-related symptoms and have poorer asthma control compared to those without depression. 40 A study by Lin et al. demonstrated that depressive disorder was common in asthma patients, and depression in asthma patients was related to an increased mortality rate. 22 This might be due to depression leading to decreased use of bronchodilators, poorer asthma control, and a diminished quality of life.18–20 Hams et al. also discovered that anxiety symptoms were significantly related to poorer asthma control, greater impairment in quality of life, and severe insomnia symptoms. In addition, adolescents with probable anxiety disorders exhibited increased odds of persistent uncontrolled asthma and higher utilization of emergency department services. 41 Asthma patients exhibiting depressive symptoms were found to have poorer asthma control and experience more frequent asthma exacerbations, 42 which further increased the risk of mortality in these patients. The presence of depressive disorder might also influence forced expiratory volume in 1 second (FEV1) responses in patients with occupational asthma. 43 The pathogenesis of neurodegeneration and neurofunction, such as inflammation in patients with depressive symptoms, might increase the risk of mortality in asthma patients.14,17,44,45 There was evidence showing that asthma had an impact on heart rate variability, and another study also indicated that stress disorder might be associated with changes in heart rate.46,47
The findings might suggest the importance of early screening of depressive symptoms in asthma patients, and timely interventions, such as drug interventions, should be applied for asthma patients with depressive symptoms. It is crucial to develop interventions that specifically target the molecular pathways linked to neuropsychiatric conditions in asthma patients with depressive symptoms. The inclusion of inquiries regarding psychiatric symptoms should be taken into consideration by clinicians as an integral component of routine asthma management. Collaborating with a mental health specialist in a multidisciplinary approach is essential for enhancing the quality of life and improving both somatic and psychiatric outcomes in patients with asthma who exhibit depressive symptoms.
This study evaluated the association between asthma, depressive symptoms, and the risk of mortality, as well as the mediating role of depressive symptoms on the correlation between asthma and mortality. The study samples were from NHANES, which were large and representative. In research, many categorical mediating and outcome variables were most accurately analyzed using survival analysis methods. Methods based on the distribution of the product and resampling methods, such as the bootstrap, yield the most accurate confidence intervals for the mediated effect and tests of hypothesis regarding the mediated effect for categorical data analysis. In our study, the mediating role of depressive symptoms on the correlation of asthma and the risk of mortality was analyzed via the distribution of the product, which provides more accurate confidence limits and statistical tests, as demonstrated in several statistical simulation studies. 48 The findings suggested the importance of monitoring the signs of depressive symptoms in asthma patients, and interventions should be performed early for these patients, which might help improve the management of asthma patients. The missing variables were dealt and a sensitivity analysis was performed, which showed no significant differences between the data before and after interpolation. The manipulation of missing values ensured the sample size and might help reduce the selection bias and strengthen the study’s robustness. There were several limitations in this study. First, although possible confounding factors, including diet, lifestyle, and complications, were considered, other potential confounding factors, such as changes in behaviors and treatments during the follow-up period, which might affect the results, were not reported. Behavior changes aimed at managing asthma could serve as effective self-care interventions. 49 Also, there was evidence indicating that well-controlled asthma and allergic sensitization decreased the likelihood of anxiety. 31 The severity of asthma and other chronic conditions was not reported in the database, and their absence from the analysis could affect our study’s results. Second, asthma was obtained through self-reporting and might be subject to reporting bias, recall bias, or measurement bias compared to other tools such as spirometry. These might lead to over- or under-estimation of the associations among asthma, depressive symptoms, and the risk of mortality. Some participants were excluded due to unmeasured variables, which might have selection bias. Although PHQ-9 is a valid scale for assessing depressive symptoms based on the Diagnostic Statistical Manual of Mental Disorders (DSM)-V, there might be recall bias. Third, the present study uses the absence of sensitivity analyses to examine whether the observed mediation effects persist under alternative model specifications. Future research should explore this aspect to strengthen the robustness and generalizability of the findings. Lastly, this was a cohort study; only the association between asthma and depressive symptoms was obtained, and the causality between asthma and depressive symptoms, asthma, and all-cause mortality could not be identified. Further studies are necessary to focus on the causal link among asthma, depressive symptoms, and all-cause mortality, and more interventions are required to improve the outcomes of asthma patients.
Conclusions
The mediating role of depressive symptoms on the correlation between asthma and mortality was evaluated in this study, which depicted that depressive symptoms mediated the association of asthma and all-cause mortality. It potentially serves as a modifiable risk factor for asthma patients and helps improve their prognosis.
Supplemental Material
sj-docx-1-imj-10.1177_10815589251352474 – Supplemental material for The mediating role of depressive symptoms between asthma and risk of all-cause mortality
Supplemental material, sj-docx-1-imj-10.1177_10815589251352474 for The mediating role of depressive symptoms between asthma and risk of all-cause mortality by Chenyi Zhang and Ziqing Ye in Journal of Investigative Medicine
Supplemental Material
sj-docx-2-imj-10.1177_10815589251352474 – Supplemental material for The mediating role of depressive symptoms between asthma and risk of all-cause mortality
Supplemental material, sj-docx-2-imj-10.1177_10815589251352474 for The mediating role of depressive symptoms between asthma and risk of all-cause mortality by Chenyi Zhang and Ziqing Ye in Journal of Investigative Medicine
Supplemental Material
sj-docx-3-imj-10.1177_10815589251352474 – Supplemental material for The mediating role of depressive symptoms between asthma and risk of all-cause mortality
Supplemental material, sj-docx-3-imj-10.1177_10815589251352474 for The mediating role of depressive symptoms between asthma and risk of all-cause mortality by Chenyi Zhang and Ziqing Ye in Journal of Investigative Medicine
Footnotes
Acknowledgements
None.
Authors’ Contributions
(1),Chenyi Zhang and Ziqing Ye conceiving and designing the study;
(2),Chenyi Zhang collecting the data;
(3),Chenyi Zhang analyzing and interpreting the data;
(4),Chenyi Zhang writing the manuscript;
(5),Ziqing Ye providing critical revisions that are important for the intellectual content;
(6),All authors approving the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
Not applicable, because NHANES belongs to public databases, the patients involved in the database have obtained ethical approval, users can download relevant data for free for research and publish relevant articles, and our study is based on open-source data, and the Zhejiang Hospital does not require research using publicly available data to be submitted for review to their ethics committee, so there are no ethical issues and other conflicts of interest.
Consent for publication
Not applicable, because this paper did not reveal any personal information of patients.
Availability of data and materials
The datasets used and/or analyzed during the current study were publicly available from the NHANES database
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.