
Abstract
The aim of this study is to compare the effect of magnesium and potassium on insulin resistance and blood sugar levels among insomniac patients with diabetes mellitus. A randomized controlled study was conducted on 320 subjects enrolled in placebo (T1), Magnesium (T2), Potassium (T3), and Magnesium + Potassium (T4) treatment groups. Pre- and post-trial blood sugar and insulin levels were analyzed through blood. Insulin resistance was calculated by the homeostatic model assessment for insulin resistance (HOMA-IR). Analysis was performed in IBM SPSS® version 25.0. HOMA-IR analysis showed that pretreatment mean of T4 (Magnesium + Potassium group) was 3.01 ± 0. 54, and post-treatment mean was 2.54 ± 0.29, showing a significant reduction (p = 0.001). There was a significant association among post-HOMA-IR scores of treatment groups (p = 0.001). Fasting blood sugar levels showed that all groups, except placebo, had significant differences in levels (p = 0.001). A comparison between treatment groups concluded that blood sugar levels were associated with significant differences (p = 0.001). The study suggests that magnesium alone and magnesium coupled with potassium supplementation assist insomniac diabetics more effectively to regulate insulin resistance and increased blood sugar levels.
Introduction
Diabetes mellitus (DM) is a metabolic illness known for consistent excessive concentration of glucose within the blood. It is one of the metabolic disorders that affects individuals worldwide. The most ordinary kind of DM is type-II. It is prevalent among 90% of the diabetic population. 1 In type-II DM, the response to insulin is decreased or completely vanishes. This is a condition known as insulin resistance or insulin insensitivity. This situation is dealt by the body through increased insulin secretion, but with the passage of time, insulin production decreases due to the diminished capacity of the cells of the pancreas to produce insulin. This results in type-II DM and occurs in people aged above 45 years. Currently, there is an increase in type-II DM cases among children, adolescents, and young adults due to an inclination toward a sedentary lifestyle, poor diet patterns, and obesity. 2
Magnesium plays a significant part in the control and cure of several illnesses. 3 Diseases that include Alzheimer, epilepsy, depression, decreased insulin sensitivity, type-II DM, high blood pressure, cardiovascular disease, strokes, migraine, hyperactivity, and attention deficit disorders in children are the most common disturbances that arise due to low serum magnesium levels. Considering neuronal functions, normal magnesium ion concentrations are imperative for the regulation of N-methyl-d-aspartate receptors’ anxiety. These receptors are critical for excitatory synapse transfer, neuronal plasticity, and excitotoxicity, which consequently play a critical role in developmental plasticity, learning, and memory. 4 Changes in magnesium levels are frequently associated with type-II DM. Individuals having type-II DM have also been found to have a higher frequency of magnesium deficiencies, particularly in people having inadequately managed blood sugar histories, prolonged illness durations, and an elevated incidence of persistent Micro-Vascular and Macro-Vascular problems. 5
Potential-dependent calcium and sodium pathways activate and depolarize as a result of the closing of ATP- sensitive potassium channels (KATP) brought on by a boost in Adenosine Triphosphate (and/or a reduction in Adenosine diphosphate) brought on by the breakdown of glucose. Insulin pellets are released as a consequence of the rise in calcium within cells. When the channels containing potassium, such as those in the potential and calcium-operated (KCa) potassium gate families, activate and the beta-cells repolarize, secretions come to an end. 6 As a result, the electrical signaling of the beta-cell directly impacts the quantity of insulin released. The options for therapy for illnesses associated with the equilibrium of glucose, such as diabetes, can be varied by modifying the many ionic gates included. The study aimed to identify the effect of magnesium and potassium supplementation on insulin resistance through serum electrolytes in insomnia patients suffering from diabetes. This study hypothesized that magnesium and potassium supplementation have an effect on insulin resistance.
In type 2 diabetes mellitus, the response to insulin is decreased or completely vanishes. This is a condition known as insulin resistance or insulin insensitivity.
This situation is dealt by the body through increased insulin secretion, but with the passage of time, insulin production decreases due to the diminished capacity of the cells of the pancreas to produce insulin.
The effect of magnesium and potassium on insulin resistance and blood sugar levels among insomniac patients with diabetes mellitus was investigated.
Magnesium alone and magnesium coupled with potassium supplementation assist insomniac diabetics more effectively to regulate insulin resistance and increased blood sugar levels.
Moreover, a substantial connection was identified between the treatment groups for the post-treatment HOMA-IR scores and blood sugar levels, showing the overall efficiency of magnesium and magnesium-coupled potassium supplementation in lowering insulin resistance and blood sugar in contrast to placebo.
Clinical trial registration: Link to full application of trial: https://clinicaltrials.gov/study/NCT04642313?locStr=Pakistan&country=Pakistan&cond=Diabetes&term=potassium%20magnesium&rank=1
Materials and methods
A Randomized Controlled Trial (Single-blinded) was conducted by using a non-probability purposive sampling technique. The study spanned around 24 months from November 2020 to November 2022. The trial was registered at clinicaltrials.gov, and the trial number is NCT04642313. Ethical approval (IRB-UOL-FAHS/760/2020) was obtained from the Institutional Review Board (IRB) of the Faculty of Allied Health Sciences (FAHS), The University of Lahore. Written informed consents were obtained from the study participants. Diabetic patients of both genders aged between 19 and 65 years and with insomnia according to the Insomnia Severity Index (ISI) were included in the study; their pre- and post-trial blood was collected at the Diabetes Center of Akhuwat Health Services, Lahore, by a qualified phlebotomist in fasting conditions. Patients with hypomagnesemia, hypokalemia, and insomnia due to other psychological and systemic syndromes except diabetes were excluded. The sample size was calculated by the following formula:
Z 1−β is the desired power of study = 95%
Z 1−α/2 is the desired level of significance at 5%
μ1 is the mean in group 1 of insomnia severity (mean of Mg2+ intake group) = 14.14 7
μ2 is the mean in group 2 of insomnia severity (mean of the placebo group) = 15.77 7
σ1 is the standard deviation (SD) in group 1 of insomnia severity (SD of Mg2+ intake group) = 2.68 7
σ2 is the standard deviation (SD) in group 2 of insomnia severity (SD of the placebo group) = 1.92 7
Ratio (r) = 1
Alpha (α) = 0.05
Beta (β) = 0.2
n (expected sample size) = 66 in each group (×4)
The total sample size was 320, with 20% dropout. A total of 320 patients were selected and followed up, but after 2 months, 290 patients were followed up and completed the trial. Four treatment groups were made namely, T1(Placebo), T2(Magnesium), T3(Potassium), and T4(Magnesium + Potassium). The participants were divided randomly into the groups by the physician, and corresponding tablets were provided to the participants on a monthly basis for 2 months for monitoring of compliance. For Placebo tablets, starch (250 mg in each tablet) was used; for Mg2+, magnesium gluconate salt was used (each containing 414 mg magnesium gluconate as 250 mg elemental Mg2+); for K+, potassium chloride salt was used; and for combined tablets, both Mg2+ and K+ salts were used. Tablets were prepared according to the standard manufacturing process. Tablets were procured from Paragon Herbal Laboratories (Regd.), FORM-6 (according to the DRUG REGULATORY AUTHORITY OF PAKISTAN, Pakistan Act 1976) was taken from the manufacturer. Child-safe bottle packing (of 60 each) was used. Tablets were stored in a cool, dry place and were provided to patients on a monthly basis. Anthropometric measurements, insulin resistance values, and fasting blood sugar levels (>126 mg/dL = high blood sugar), and serum insulin levels (mg/dL) were taken at the beginning (0 day) and after 60 days of trial. A diet plan with magnesium and potassium under 75% RDA was provided to the patients with dietary guidelines, designed according to the Pakistan dietary guidelines. 8 Insulin resistance was calculated by HOMA-IR using the equation:
Glucose in molar units (mmol/L)
HOMA-IR = Glucose × Insulin/22.5
Glucose in mass units (mg/dL)
HOMA-IR=Glucose × Insulin/405
HOMA-IR stands for Homeostatic Model Assessment of Insulin Resistance. This calculation marks for both the presence and extent of any insulin resistance that you might currently express. 9 The following standard ranges were chosen: HOMA-IR < 2.60—normal, HOMA-IR 2.60 to 3.80—borderline high, and HOMA-IR > 3.80—high. Data were entered and analyzed using SPSS version 25.0. Numeric data, such as age and blood glucose level, were presented in the form of mean ± SD. Categorical data, such as gender, were presented in the form of percent frequencies. Comparison of pre- and post-serum insulin levels, blood sugar levels, and HOMA-IR scores within-group was conducted by paired sample t-test according to normality of data assessed by the Shapiro-Wilk test. The magnitude of change was quantified using Cohen’s d for paired samples. p-value ≤ 0.05 was considered significant. The CONSORT flow diagram for the trial is represented in Figure 1.
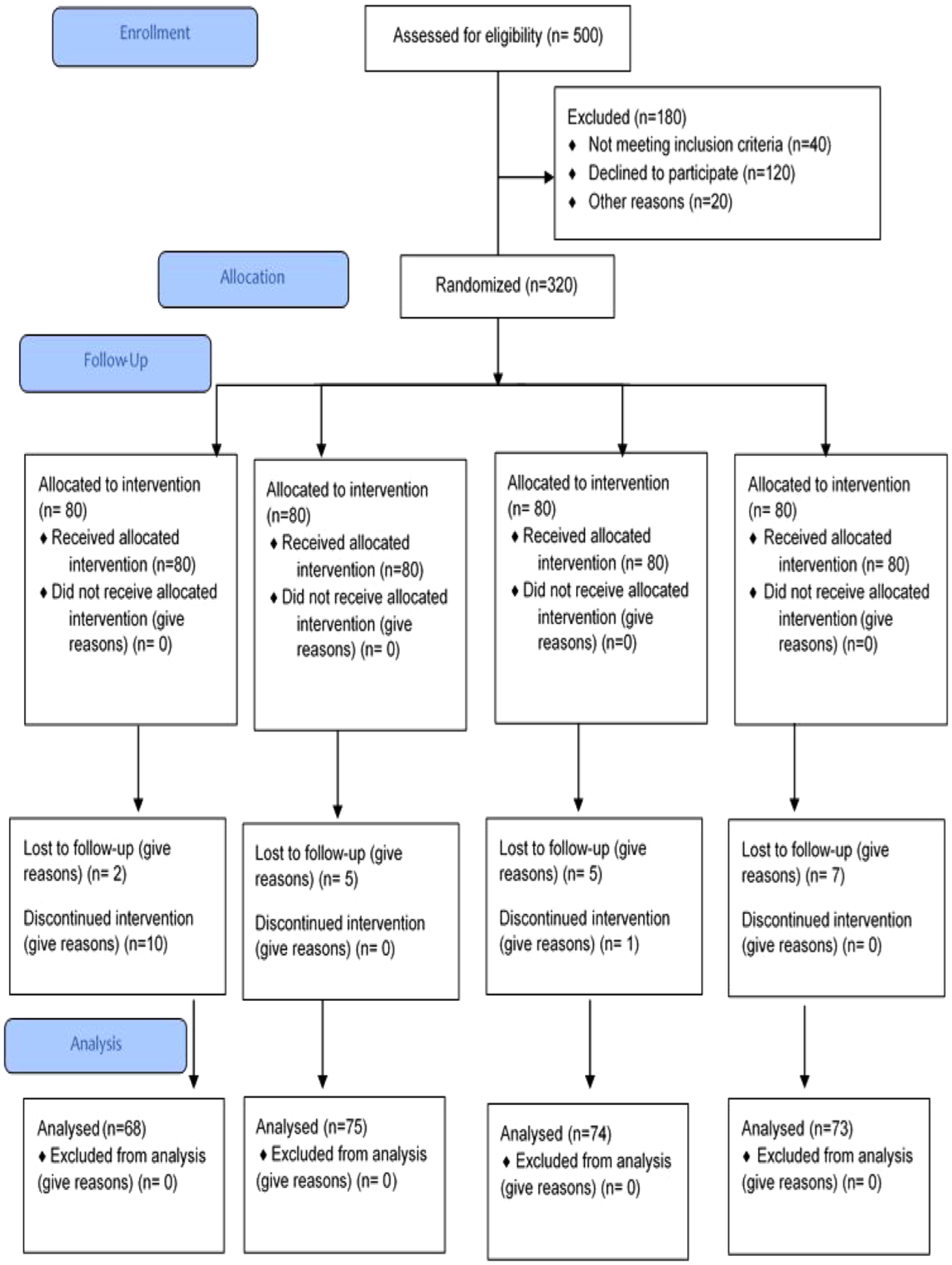
CONSORT flow diagram for the trial.
Results
HOMA-IR
Statistical analysis of 290 subjects’ HOMA-IR score showed that there was a significant association between pre- and post-differential scores of treatment groups T2 and T4. Pretreatment mean ± SD of T1 (placebo group) was 3.176 ± 0.47, and post-treatment mean ± SD was 3.142 ± 0.45, showing an insignificant association within groups, as the p-value is 0.154. Pretreatment mean ± SD of T2 (Magnesium group) was 2.98 ± 0.48, and post-treatment mean ± SD was 2.49 ± 0.29, showing a significant association between pre- and post-treatment values, as the p-value is 0.001. Pretreatment mean ± SD of T3 (Potassium group) was 3.09 ± 0.60, and post-treatment mean ± SD was 2.93 ± 0.60, showing an insignificant association within groups, as the p-value is 0.10. Pretreatment mean ± SD of T4 (Magnesium + Potassium group) was 3.01 ± 0.54, and post-treatment mean ± SD was 2.54 ± 0.29, showing a significant association within groups as p-value is 0.001, as shown in Table 1.
Comparison of HOMA-IR score of diabetic patients with insomnia within treatment groups.
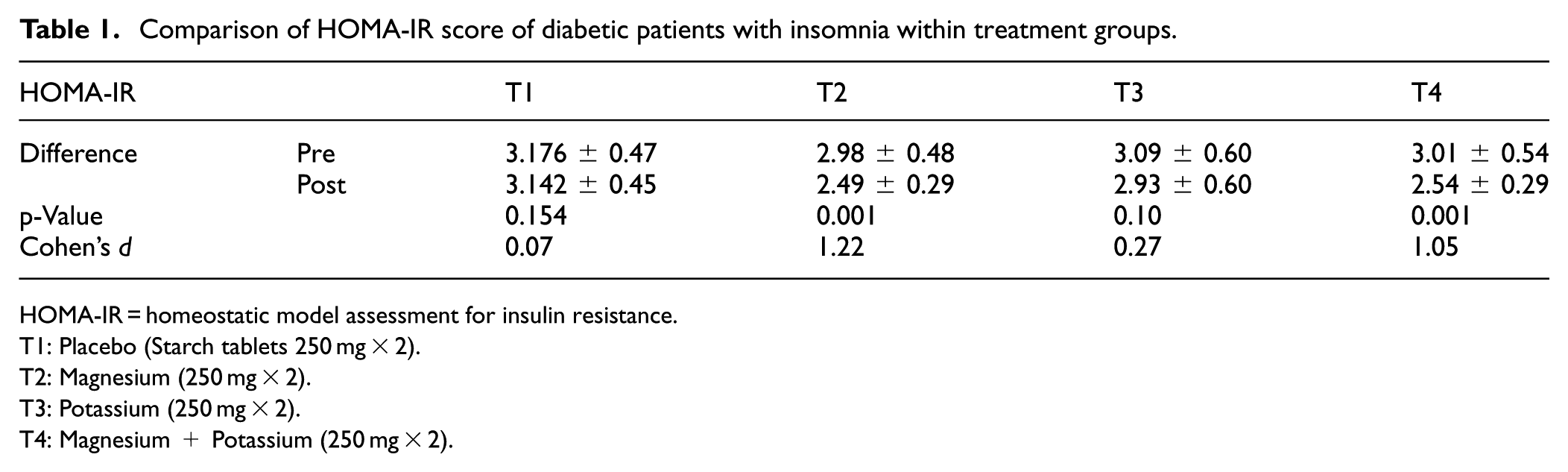
HOMA-IR = homeostatic model assessment for insulin resistance.
T1: Placebo (Starch tablets 250 mg × 2).
T2: Magnesium (250 mg × 2).
T3: Potassium (250 mg × 2).
T4: Magnesium + Potassium (250 mg × 2).
Blood sugar
Statistical analysis of blood sugar level (mg/dL) showed that there was a significant association between pre- and post-level differences within three of the treatment groups, excluding T1 (p = 0.650). Pretreatment mean of T2 (Magnesium group) was 238.28 ± 35.91, and post-treatment mean was 226.33 ± 37.69 (p = 0.001). Pretreatment mean ± SD of T3 was 218.26 ± 42.33, and post-treatment mean ± SD was 209.51 ± 4840 with a p-value of 0.001. Similarly, the differences of means in T4 were 223.75 ± 37.82 pre-trial and 209.04 ± 41.01 post-trial, showing a significant association within group with p-value 0.001 (Table 2).
Comparison of blood sugar level (mg/dL) of diabetic patients with insomnia within treatment groups.
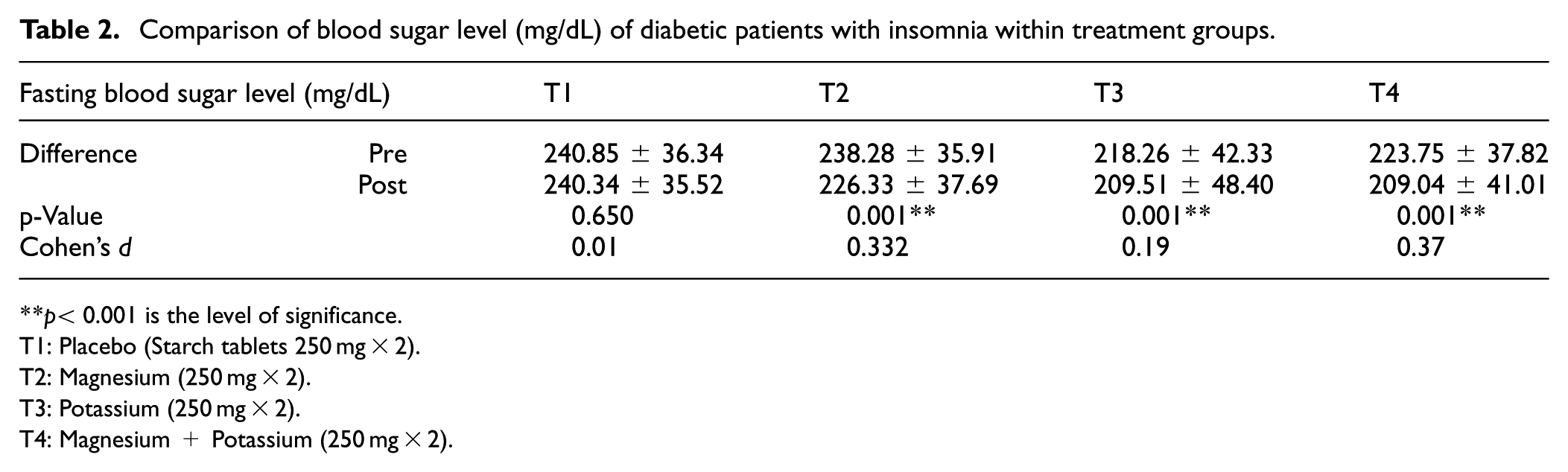
**p< 0.001 is the level of significance.T1: Placebo (Starch tablets 250 mg × 2).
T2: Magnesium (250 mg × 2).
T3: Potassium (250 mg × 2).
T4: Magnesium + Potassium (250 mg × 2).
Serum insulin
Statistical analysis of serum insulin (mg/dL) showed that there was a significant association between pre- and post-differences of the three treatment groups, excluding T1 (placebo). Pretreatment mean ± SD of T1 (placebo group) was 254.76 ± 56.74, and post-treatment mean ± SD was 282.84 ± 35.36, showing an insignificant association within groups, as the p-value is 0.509. Pretreatment mean ± SD of T2 (Magnesium group) was 257.36 ± 50.83, and post-treatment mean ± SD was 233.66 ± 42.56, showing a significant association within groups, as the p-value is 0.001. Pretreatment mean ± SD of T3 (Potassium group) was 267.64 ± 40.59, and post-treatment mean ± SD was 256.22 ± 38.49, showing a significant association within groups, as the p-value is 0.001. Pretreatment mean ± SD of T4 (Magnesium + Potassium group) was 259.38 ± 54.84, and post-treatment mean ± SD was 181.66 ± 17.66, showing a significant association within groups as p-value is 0.001, as shown in Table 3.
Comparison of serum insulin levels (mg/dL) of diabetic patients with insomnia within treatment groups.
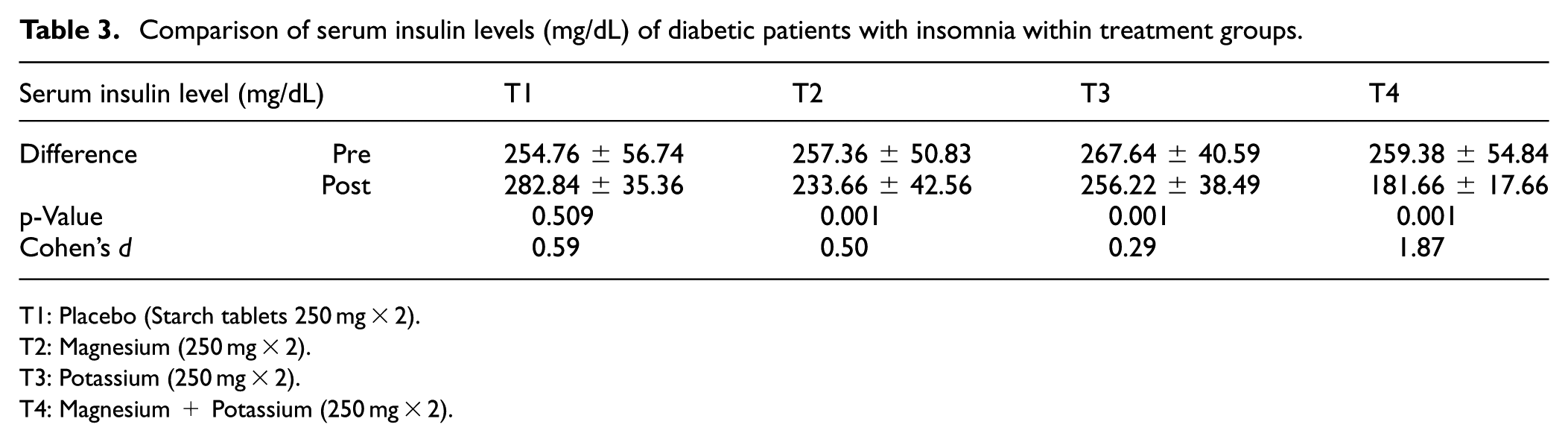
T1: Placebo (Starch tablets 250 mg × 2).
T2: Magnesium (250 mg × 2).
T3: Potassium (250 mg × 2).
T4: Magnesium + Potassium (250 mg × 2).
Discussion
Current research was carried out to show the effect of Mg2+ and K+ on insulin resistance and blood sugar levels. Mg2+ intake has been shown in several metabolic processes investigations to have a beneficial effect on how insulin works and the absorption of glucose.10,11 An excessively inadequate potassium amount can cause the organism to produce fewer hormones, such as insulin.
In the current study, for groups T2 (magnesium) and T4 (magnesium + potassium), the analysis shows substantial correlations between pre- and post-treatment variations in HOMA-IR scores, showing the effectiveness of these therapies in reducing insulin resistance. With lower HOMA-IR values after therapy than before, groups T2 and T4 demonstrated significant connections within the groups. On the other hand, neither the potassium group (T3) nor the placebo group (T1) showed any appreciable improvements. Moreover, a noteworthy correlation was seen between the treatment groups in the HOMA-IR scores after the intervention, underscoring the therapies’ overall efficacy in mitigating insulin resistance in contrast to the placebo. Increased intake of magnesium, potassium, and vitamin D is linked to optimum HOMA-IR values in individuals with pre-diabetes and normoglycemia. 12
We also investigated the effects of magnesium and potassium supplementation on insomnia and sleep hormones in same patients with diabetes mellitus in our previous study. We used an Insomnia Severity Index (ISI) for the assessment of severity and duration of insomnia among T1, T2, T3 and T4 groups. Sleep hormones (melatonin and cortisol) were measured from serum samples using an enzyme-linked immunosorbent assay (ELISA). The findings demonstrated that magnesium, potassium separately as well as combined had a significant effect on serum cortisol and melatonin levels. Hence, the addition of supplementation was suggested to decrease the severity of insomnia in patients with diabetes. 13 During the same trial, we also investigated the comparative efficacy of magnesium and potassium towards cholesterol and quality of life in type-II DM patients. It was observed that there was an improvement in hyperlipidemia and quality of life after magnesium and potassium supplementation. 14 Similarly, an association of cholesterol with hepatorenal markers were also explored during the same trial. However, no association was observed in this regard. 15
A comprehensive analysis by Yokota et al. reported that the effects of supplementing with magnesium were not statistically noteworthy on plasma glucose (p = 0.119). However, a subgroup analysis comparing the periods of magnesium supplementation—less than 4 months against more than 4 months—showed a significant difference in the concentrations of glucose during fasting (p < 0.001). 16 Furthermore, 24-week research using 500 mg of magnesium oxide daily found no difference in fasting blood glucose levels or HbA1c. Whang et al. reported that supplementing with Mg using a lake’s natural solution negatively impacted HOMA-IR but not FBG or HbA1c. 17 Similar results were observed by Veronese and colleagues in 2016. According to their study, after a two-hour oral glucose tolerance test, magnesium supplementation dramatically reduced plasma glucose levels and seemed to decrease HOMA-IR levels as well. They reported that supplementing with magnesium seems to be advantageous and improves insulin-sensitivity parameters in those at high risk of developing diabetes, as well as glucose metrics in those who already have the disease. 18 Findings of Simental-Mendia et al., who conducted a study on diabetic and nondiabetic patients, are also in accordance with current findings. According to them, in both diabetic and nondiabetic participants, there was a significant impact of magnesium supplementation on the HOMA-IR index (p = 0.013) and fasting glucose. 19 Findings of Lopez-Ridaura et al. indicated a strong negative relationship between the risk of diabetes and magnesium consumption, which supports these findings. Their study backed up the dietary advice to eat more whole grains, nuts, and green leafy vegetables—some of the main food sources of magnesium. 20 According to Chatterjee et al., hypothesis, supplementing with potassium chloride (KCl) should lead to improvements in metabolomic indicators, which are linked to a lower risk of diabetes and cardiovascular disease. 21 Whang and Sims presented a similar hypothesis. As there was frequent deficiency of magnesium and potassium in diabetic patients, they stated that Mg2+ and K+ supplementation can prevent the effects of vascular diabetic disease. 22 Similarly, according to Sun et al., the patients with no central obesity, hypertriglyceridemia, low HDL-C, or increased fasting plasma glucose levels, had lower blood potassium levels when age and sex were taken into account. 23 Although magnesium is a necessary auxiliary component for metabolic enzymes of glucose and insulin, Chu et al. found no correlation between magnesium and parameters that are reliant on glucose, which is contrary to the current study findings. 24
Conclusion
The study examined how potassium (K+) and magnesium (Mg2+) supplementation affected blood sugar levels and insulin resistance in insomniac diabetics. Both magnesium alone (T2) and magnesium coupled with potassium (T4) groups reduced insulin resistance. Neither the potassium-alone (T3) nor the placebo (T1) group improved. Blood sugar levels also dropped upon magnesium, potassium, and their combined supplementation, along with significant relationships between pre- and post-treatment groups. Moreover, a substantial connection was identified between the treatment groups for the post-treatment HOMA-IR scores and blood sugar levels, showing the overall efficiency of magnesium and magnesium-coupled potassium supplementation in lowering insulin resistance and blood sugar in contrast to placebo. The study suggests that magnesium alone and magnesium coupled with potassium supplementation assist insomniac diabetics more effectively to regulate insulin resistance and increased blood sugar levels.
Footnotes
Acknowledgements
The authors extend their appreciation to Umm Al-Qura University, Saudi Arabia, for funding this research work through grant number: 25UQU4330924GSSR02.
Author contributions
Conceptualization: Sidra Khalid, Shahid Bashir; Riffat Mehboob, Data curation: Humaira Waseem; Sidra Khalid, Formal analysis: Imran Shahid, Humaira Waseem; Investigation and interpretation: Shatha Alharazy; Abdullah R. Alzahrani; Methodology: Sidra Khalid, Shahid Bashir; Project administration: Sidra Khalid, Zergham Mazhar; Riffat Mehboob, Supervision: Shahid Bashir Validation: Abdullah R. Alzahrani; Imran Shahid Funding Acquisition: Imran Shahid; Abdullah R. Alzahrani, Writing-original draft: Sidra Khalid, Humaira Waseem, Riffat Mehboob, Shahid Bashir; Writing-review and editing: Imran Shahid, Zergham Mazhar, Abdullah R. Alzahrani, Shatha Alharazy.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research work was funded by Umm Al-Qura University, Saudi Arabia, under grant number: 25UQU4330924GSSR02.
Ethical approval and consent to participate
The study was approved by the University of Lahore, Lahore, Pakistan (Ethical Clearance Reference Number: (IRB-UOL-FAHS/760/2020) on September 15, 2020, and Lahore Medical Research Center, Lahore, Pakistan (Ethical Clearance Reference Number: LMRC/01/2021/02/RCT02) on Apr. 20th, 2021.
Consent for publication
All participants provided written informed consent prior to participating. Participants also provided consent for publication.
Data availability statement
Data will be available upon reasonable request to the corresponding authors.