
Abstract
The role of early endoscopy in patients with nonvariceal upper gastrointestinal bleeding (UGIB) is controversial; in addition, the timing of endoscopy in patients with variceal hemorrhage has been poorly studied. We aimed to determine the effect of time to endoscopy on clinical outcomes in nonvariceal and variceal UGIB. We identified patients with acute UGIB admitted from the emergency room in an academic medical center. Patients were stratified by risk (low and high) and source of bleeding (variceal or nonvariceal). We examined time to endoscopy (within 3, >3–6, >6–12, and >12–24 h) and assessed the following outcomes: stigmata of bleeding, transfusions, rebleeding, surgery, mortality, ICU admission, readmission (within 42 days), weekday versus weekend admission, and length of stay (LOS). We identified 987 patients with nonvariceal UGIB and 288 patients with variceal UGIB. Clinical outcomes, including transfusions, rebleeding, surgery, mortality, ICU admission or readmission, did not vary as a function of the time to endoscopy. However, a shorter time to endoscopy was an independent predictor of identifying stigmata of bleeding (p < 0.001) and increases in time to endoscopy reduced the likelihood of identifying stigmata of bleeding to 66%, 35%, and 23% at 2, 6, and 12 h, respectively (p < 0.001). Endoscopy performed within 3 h was also associated with a significantly reduced LOS in low-risk patients with nonvariceal UGIB (p < 0.001). Our data indicate that although earlier endoscopy does not improve clinical outcomes, the earlier it is performed, the more likely stigmata are identified, and in certain types of patients (especially low-risk), the earlier discharge.
Introduction
Acute upper gastrointestinal bleeding (UGIB) occurs with an incidence between 30 and 150/100,000 adults/year. 1 Since diagnostic endoscopy alone does not appear to affect outcomes 2 while therapeutic endoscopy has been shown to reduce mortality in patients with acute nonvariceal UGIB, the use of endoscopy has evolved from a purely diagnostic focus to the current situation in which endoscopy is performed largely to perform therapy. Given these considerations, a controversial issue revolves around the most appropriate timing of endoscopy – including for both nonvariceal bleeding and variceal bleeding.
Current expert recommendations in UGIB are that “patients with UGIB should undergo endoscopy within 24 h of admission” (based on low-quality evidence) 3 ; “for patients who are hemodynamically stable and without serious comorbidities, endoscopy should be performed as soon as possible in a nonemergent setting to identify the substantial proportion of patients with low-risk endoscopic findings who can be safely discharged”; and “in patients with higher risk clinical features (e.g. tachycardia, hypotension, bloody emesis, or nasogastric aspirate in hospital), endoscopy within 12 h may be considered to potentially improve clinical outcomes.” Although this recommendation was also based on low-quality evidence, there remains controversy in this area. It has also been proposed that no evidence exists that very early endoscopy (within a few hours of presentation) can reduce the risk of rebleeding or improve survival.4,5
During the time period of the study, we developed an organized approach to UGIB, adopting an expectation that in all patients with evidence of active UGIB, endoscopy be performed as early as possible and practicable. Thus, in an effort to understand whether this approach has merit, we examined our experience in a large cohort of patients with both nonvariceal and variceal UGIB.
Patients and materials and methods
This retrospective cohort study of patients at Parkland Memorial Hospital and University of Texas Southwestern Medical Center admitted from the emergency room (ER) with acute UGIB from April 2006 to September 2011. During this time, the unit developed a prospective registry in which all patients were entered. The study was approved by the University of Texas Southwestern Institutional Review Board and met all criteria for good clinical practice.
UGIB was defined as witnessed or reported hematemesis, melena, or hematochezia, in the context of a drop in hematocrit of 4 points below baseline or a hematocrit below normal (36 for men or 33 for women). All patients underwent endoscopy and were 18 years of age or older. When UGIB was identified, it was judged by the responsible physician to be proximal to the ligament of Treitz. Patients with middle or lower gastrointestinal bleeding (defined as bleeding distal to the ligament of Treitz) or who were pregnant were excluded.
The primary aim was to determine to effect of time to endoscopy in patients with nonvariceal and variceal UGIB on specific clinical outcomes, which included the following: stigmata of bleeding, transfusions, rebleeding events, surgery, mortality, ICU admission, readmission (within 42 days), weekday versus weekend admission, and length of stay (LOS). A pre-specified secondary aim was also to determine whether the time of the endoscopy predicted the detection of stigmata of bleeding in each of the nonvariceal and variceal bleeding groups. Also studied was the effect of endoscopic therapy in patients with stigmata of bleeding on clinical outcomes in patients undergoing endoscopy within the different time intervals. Data were obtained at pre-endoscopy, at the time of endoscopy, and post-endoscopy (see Supplemental Table 1). For nonvariceal bleeding, a Rockall score of <5 was used to define a low-risk group and a score of >5 was defined as a high-risk group. 6 As per routine practice, proton pump inhibitors, octreotide, and antibiotics were administered as recommended 3 per the primary teams’ orders.
Statistical analysis
The time (h) from ER admission to the endoscopic procedure was analyzed as in the primary analyses. Details of the statistical analysis are included in Supplemental Information.
Results
We identified 1275 patients with UGIB, including 288 patients with variceal UGIB and 987 patients with nonvariceal UGIB (Supplemental Figure 1). Of the 987 patients with nonvariceal UGIB, 932 patients were low-risk (<5 Rockall score) and 55 patients were high-risk (>5 Rockall score). Clinical characteristics of the nonvariceal and variceal groups were typical of those for patients with UGIB (Table 1). Clinical features (melena, hematemesis, and hematochezia) were essentially indistinguishable between the nonvariceal and variceal groups. Vital signs and laboratory abnormalities on admission were also typical of those with UGIB. Lesions identified in the nonvariceal UGIB (as in section “Patients and materials and methods”) group included typical abnormalities, including inflammatory lesions (esophagitis, gastritis/duodenitis, ulcer disease, etc.), mass lesions, miscellaneous lesions (Mallory-Weiss tear, angioectasias, etc.) were typical of those with UGIB.
Demographic and clinical characteristics.
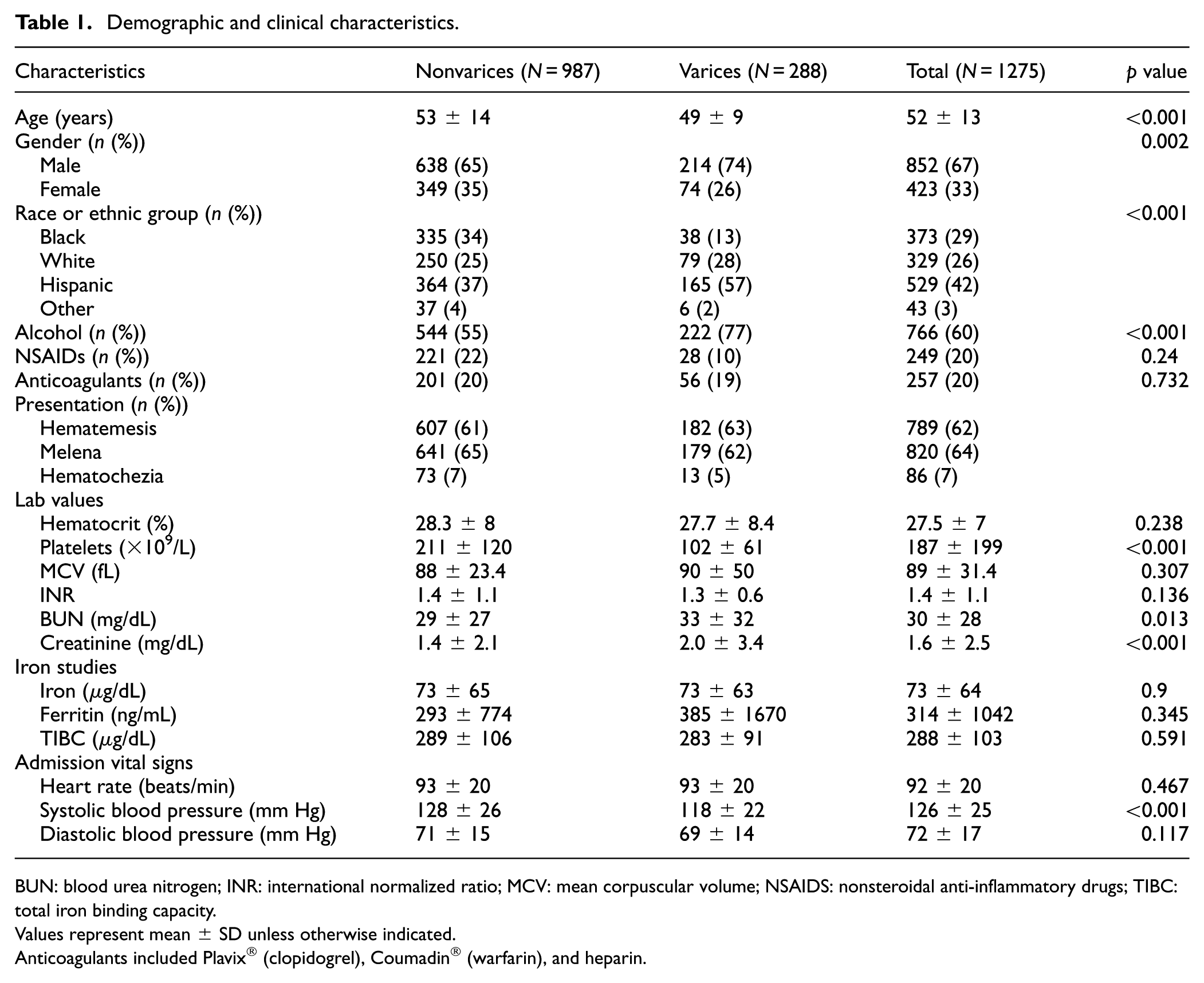
BUN: blood urea nitrogen; INR: international normalized ratio; MCV: mean corpuscular volume; NSAIDS: nonsteroidal anti-inflammatory drugs; TIBC: total iron binding capacity.
Values represent mean ± SD unless otherwise indicated.
Anticoagulants included Plavix® (clopidogrel), Coumadin® (warfarin), and heparin.
Fifty-five percent and 69% of patients in the nonvariceal and variceal groups, respectively, underwent endoscopy within the first 24 h from ER admission, and the most frequent time to endoscopy was 12–24 h (Supplemental Figures 1 and 2). Overall, the average time to endoscopy in nonvariceal UGIBers was 28 h, and 23 h in variceal bleeders. Median times to endoscopy were 22 and 18 h in these groups, respectively. The median time to endoscopy in the low-risk (n = 932) and the high-risk nonvariceal (n = 55) group was 23 and 18 h, respectively. There was a similar distribution of time to endoscopy in the low-risk and high-risk nonvariceal groups (Supplemental Figure 3).
Time to endoscopy did not significantly affect the majority of clinical outcomes, including transfusion requirements, rebleeding events, surgery, mortality, ICU admission, readmission, or weekday versus weekend admission in both the nonvariceal (both low and high-risk groups) and variceal groups (Tables 2 and 3). However, in patients with nonvariceal bleeding, LOS was significantly decreased when endoscopy was performed within 0–3 h as compared to >12–24 h (2 vs 3 days (p = 0.004)), including in low-risk patients (Table 3). There was also an overall reduction in LOS in the low-risk nonvariceal group when endoscopy was performed earlier (Table 2).
Outcomes by time to endoscopy in nonvariceal and variceal bleeding.
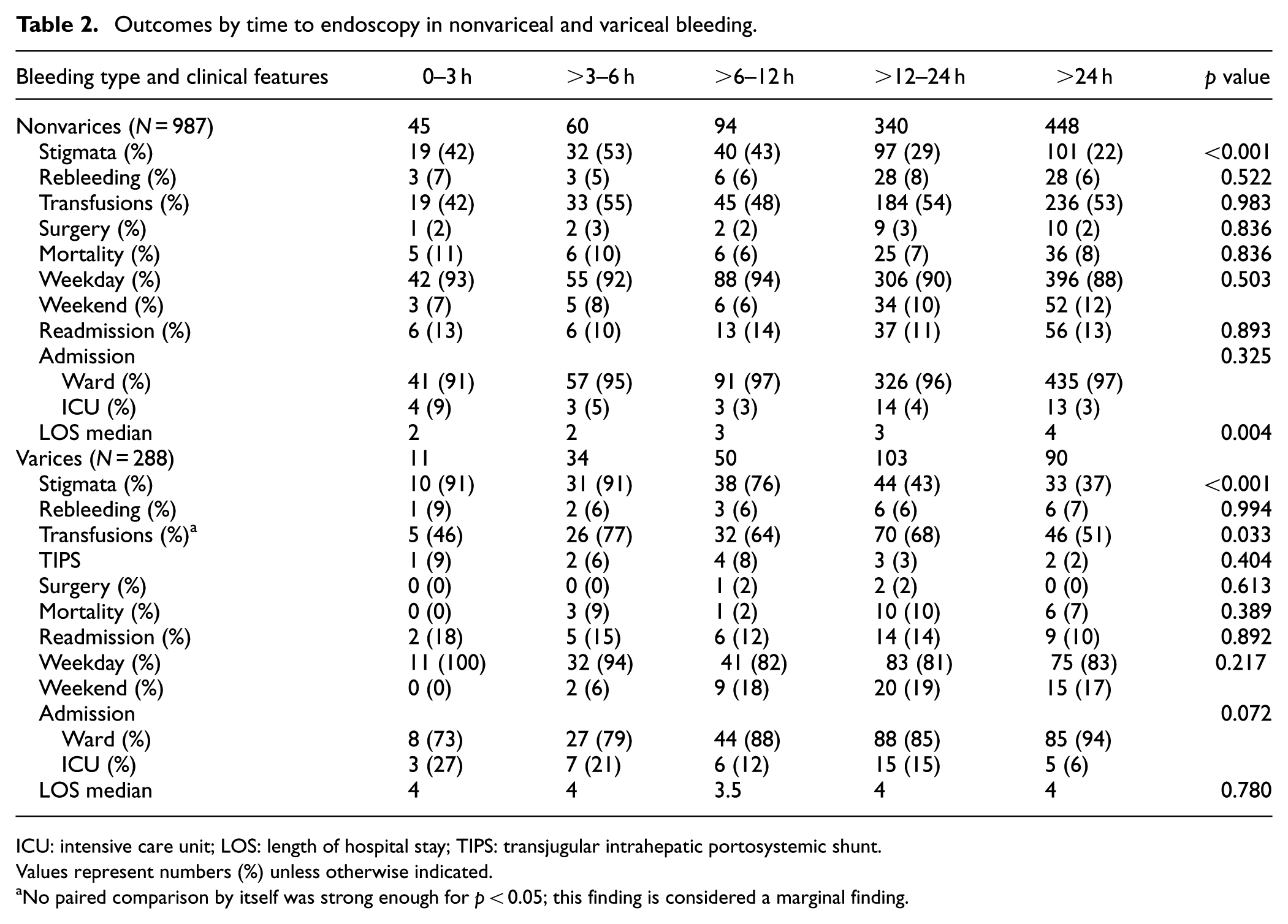
ICU: intensive care unit; LOS: length of hospital stay; TIPS: transjugular intrahepatic portosystemic shunt.
Values represent numbers (%) unless otherwise indicated.
No paired comparison by itself was strong enough for p < 0.05; this finding is considered a marginal finding.
Outcomes by time to endoscopy in low versus high risk nonvariceal bleeding.
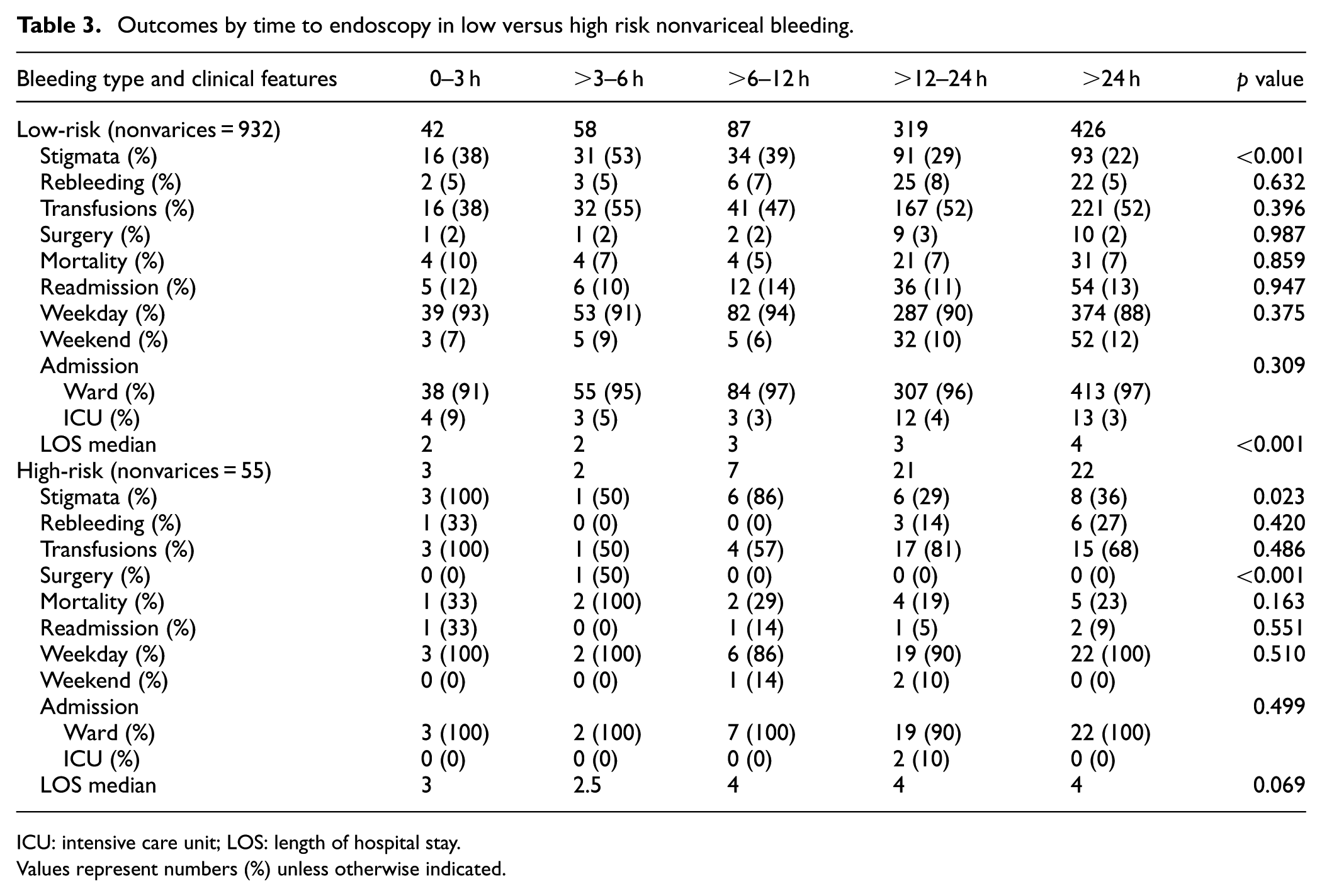
ICU: intensive care unit; LOS: length of hospital stay.
Values represent numbers (%) unless otherwise indicated.
Logistic regression analysis (as defined in section “Patients and materials and methods”) revealed that the time to endoscopy was an independent predictor of the presence of stigmata of bleeding (p < 0.001) in both the nonvariceal and variceal groups after adjusting for multiple clinical variables and the longer the time to endoscopy, the less the likelihood of observing stigmata of bleeding (p < 0.001; Supplemental Figure 4). Only male gender, a Rockall score >5, and having a duodenal ulcer (OR = 2.040; 95% CI 1.620–2.461, p < 0.001) were associated with a significantly higher odds of having stigmata of bleeding.
Outcomes of patients with stigmata of bleeding were also assessed (Supplemental Table 2). Lesions with stigmata of bleeding were identified in 29% of the nonvariceal group and in 54% of the variceal group (Supplemental Figure 1). In patients with nonvariceal bleeding lesions, there was an association with timing to endoscopy and the likelihood of endoscopic therapy; for example, 100% of patients with stigmata of bleeding identified at 0–3 h underwent endoscopic therapy, while 63% of those identified >24 h after presentation underwent endoscopic therapy. However, this did not translate into changes in clinical outcomes. Notably, endoscopic therapy was performed with nearly equivalent frequency in patients with varices, regardless of the time from presentation to endoscopy.
Multivariable binary logistic regression was used to evaluate the relationship between the time to endoscopy and identification of stigmata of bleeding, as described in the section “Patients and materials and methods.” This analysis yielded an area under the receiver operating characteristic of 0.80 (Supplemental Figure 5).
Discussion
We have demonstrated that the time to endoscopy was an independent predictor of identifying stigmata of bleeding (p < 0.001) and that increases in time to endoscopy significantly reduced the likelihood of identifying stigmata of bleeding. Further, early endoscopy was associated with reduced LOS, especially in patients with nonvariceal bleeding. However, the timing of endoscopy did not appear to affect mortality, even when patients were stratified by the severity of bleeding.
The optimal timing of endoscopy for patients with UGIB remains an extremely controversial topic7–14 and one of the major issues in this field is whether early endoscopy improves outcomes. A meta-analysis of three randomized-controlled trials in patients with nonvariceal UGIB, comprising 528 patients, found no significant reduction in rebleeding (OR = 0.71; 95% CI 0.28–1.81), surgery (OR = 1.16; 95% CI 0.39–3.51), or mortality (OR = 0.70; 95 CI 0.14–3.57) with urgent (<12 h) endoscopy compared with later (>12 h) endoscopy. 15 One of these RCT studies reported significantly shorter hospital stays and lower costs with very early (1–2 h) versus elective (1–2 days) endoscopy. 8 A randomized controlled trial also failed to demonstrate a mortality benefit in patients undergoing early endoscopy (<6 h) compared to standard endoscopy within 24 h for nonvariceal UGIB. 5 Other analyses that assessed urgent (<8 h) versus early (6 or 8–24 h) endoscopy16–18 reported no group differences in clinical outcomes. In contrast, other studies have suggested that delaying endoscopy is associated with a higher mortality; one study found a higher risk of mortality in high-risk UGIB patients having endoscopy >13 h after presentation, 19 while another study suggested that patients who were hemodynamically unstable benefited from earlier endoscopy. 14 A study that focused on therapeutic endoscopy found that earlier endoscopy (<12 h) was not associated with a lower mortality or need for surgery compared with later endoscopy (>12 h). 20 In a large retrospective study from Hong Kong that examined the timing of endoscopy, it was found compared with urgent (t ≤ 6) and late endoscopy (24 < t ≤ 48) among patients who have received therapeutic endoscopies, early endoscopy (6 < t ≤ 24) was associated with superior outcomes, especially among patients with nonvariceal bleeding. 21 Notably, there is wide variation in findings of these studies – likely as a result of substantial differences in baseline features of patients, endoscopic-related factors, type of therapeutic interventions, and/or co-interventions. Further, few of these studies have included patients with variceal bleeding.
Importantly, in contrast to previous studies, our study included patients with variceal bleeding. We found no difference in patients with variceal and nonvariceal bleeding in terms of outcome. However, there were two important advances noted here in patients with variceal bleeding. First, identification of stigmata of bleeding was more common in those with early endoscopy; patients having endoscopy within 6 h had a >90% likelihood of having stigmata of bleeding, while those having endoscopy 24 h after presentation had only a 37% likelihood of having stigmata of bleeding (Tables 2 and 3). Additionally, the time to discharge of patients with variceal bleeding having early endoscopy (within 3 h) was shorter (3 days) than those having later endoscopy (4 days).
Interestingly, the current recommendations that endoscopy should be performed within 24 h were not always met, despite our attempts to create an organized approach to UGIB. The reasons for this are multifactorial and include a number of practical reasons, such as the availability of care providers, an intent to “stabilize” the patient prior to endoscopy, and others. Interestingly, this finding is consistent with a previous study that examined the use of endoscopy and outcomes for acute UGIB. 22
We recognize the limitations of our study. Perhaps the most important is that it was retrospective in nature. This could have introduced any of several potential biases. The most important concern is that patients with aggressive bleeding may not have undergone endoscopy early, so that they could be “stabilized” prior to endoscopy. Thus, any potential impact of early endoscopy in these patients may have been missed. However, the bleeding team approach here collected data in real time, helping to eliminate this potential bias. In addition, this study reports on data, that is, >10 years old. However, with the exception of introducing restrictive transfusion strategies, management of UGIB has not changed appreciably in the last two decades. Finally, this study was performed in a single academic center, which could limit its generalizability – and our practice of routine performance of early endoscopy should be noted.
In summary, although early endoscopy did not appear to improve the important clinical outcome of mortality, early endoscopy appeared to have several benefits, including better identification of putative bleeding lesions and a reduction in hospital LOS.
Supplemental Material
sj-docx-1-imj-10.1177_10815589251386727 – Supplemental material for Time to endoscopy and its effect on outcomes in acute nonvariceal and variceal upper gastrointestinal bleeding
Supplemental material, sj-docx-1-imj-10.1177_10815589251386727 for Time to endoscopy and its effect on outcomes in acute nonvariceal and variceal upper gastrointestinal bleeding by Emely Eid, Alan Elliott and Don C. Rockey in Journal of Investigative Medicine
Footnotes
Acknowledgements
We thank Rafia Bhore for helpful discussions in preparation for the statistical analyses and Rebecca Chason for assistance with data acquisition.
Author contributions
Emely Eid – study concept and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; statistical analysis. Alan Elliott – analysis and interpretation of data; statistical analysis. Don C. Rockey – study concept and design; acquisition of data; analysis and interpretation of data; drafting of the manuscript; critical revision of the manuscript for important intellectual content; statistical analysis. All authors have approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor of the manuscript
Dr. Don C. Rockey is acting as the submission’s guarantor (i.e. the person who takes responsibility for the integrity of the work as a whole, from inception to published article).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.