
Abstract
Triglyceride-deposit cardiomyovasculopathy (TGCV) is characterized by diffuse narrowing of the coronary arteries because of triglyceride-deposit atherosclerosis. However, the plaque characteristics and prognosis of TGCV in patients with diffuse coronary artery disease remain unclear. This study aimed to describe the morphology of coronary arteries in TGCV using integrated backscatter intravascular ultrasound (IB-IVUS) and assess the effects on clinical outcomes. This single-center, retrospective observational study compared the IB-IVUS findings and clinical outcomes of patients with native coronary lesions of TGCV with those of patients with non-TGCV, all of whom had diffuse coronary artery disease. TGCV was diagnosed as (1) a low washout rate of iodine-123-β-methyl iodophenyl-pentadecanoic acid (BMIPP; <10%) on BMIPP single-photon emission computed tomography and (2) diffuse narrowing of the coronary arteries on coronary angiography. Thirty-one patients with diffuse coronary artery disease who underwent percutaneous coronary intervention were enrolled. Among these patients 10 (32%) were diagnosed with TGCV. IB-IVUS revealed that TGCV lesions had a significantly smaller ratio of the lipid area than non-TGCV lesions (20% ± 0.8% vs 23% ± 0.5%, p = 0.02). Conversely, the ratio of the calcification area tended to be larger. The Kaplan–Meier analysis revealed a significant increase in the rates of major adverse cardiovascular events in the TGCV group (p = 0.01). Patients with diffuse coronary artery disease present TGCV characterized by a smaller ratio of the lipid area. TGCV might be associated with worse clinical outcomes. The study findings may contribute to its early diagnosis and management.
Keywords
Introduction
Diffuse coronary artery disease poses a major therapeutic challenge. In many cases of diffuse coronary artery disease, percutaneous coronary intervention (PCI) or coronary artery bypass grafting cannot fully achieve revascularization and ensure adequate myocardial perfusion. Moreover, patients with severe diffuse coronary artery disease that cannot be treated with revascularization represent a subgroup with a very high mortality rate.1,2
Triglyceride-deposit cardiomyovasculopathy (TGCV) is a rare and persistent cardiovascular disorder caused by impaired hydrolysis of intracellular triglycerides (TGs). This novel disease concept was first identified in 2008 from heart transplant-waiting cases in Japan and was later labeled as an orphan disease in Europe in 2019. 3 The impaired hydrolysis of intracellular TGs causes lipotoxicity and energy failure, resulting in diffuse narrowing, TG-deposit coronary atherosclerosis, and cardiomyocyte steatosis.4,5 In Japan, 991 patients were diagnosed with TGCV in October 2024; however, the potential prevalence of TGCV in Japan is 1 in 3000 patients. 6
TG-deposit atherosclerosis occurs within the endothelial and smooth muscle cells (SMCs); thus, TGCV is characterized by diffuse narrowing of the coronary arteries. A pathological study indicated that TG-deposit atherosclerosis is distinct from the usual cholesterol-deposit atherosclerosis; the former is marked by concentric narrowing formed by TG-deposit SMCs, 7 whereas the latter is characterized by eccentric stenosis initiated by a response to endothelial injury and accumulation of cholesterol-laden macrophages. 8 Previously, we reported the intravascular ultrasound (IVUS) findings of TGCV, noting that patients exhibited smaller plaque eccentricity. 9 However, the characteristics of plaque composition remain unclear, and clinical outcomes have not been thoroughly investigated. Thus, this study aimed to elucidate the characteristics of plaque composition using integrated backscatter (IB)-IVUS and clarify the effect of TGCV on clinical outcomes.
Significance Statement
Triglyceride-deposit cardiomyovasculopathy (TGCV) causes diffuse coronary narrowing and is often underdiagnosed in high-risk populations.
This study revealed that TGCV lesions have a significantly smaller lipid area on integrated backscatter intravascular ultrasound (IVUS) and are associated with worse clinical outcomes.
IVUS findings may help clinicians suspect TGCV during percutaneous coronary intervention, prompting earlier diagnosis and management in affected patients.
Materials and methods
Study design and population
This retrospective single-center observational study analyzed data from our hospital’s coronary angiography database. Figure 1 presents the study flowchart. Among 780 consecutive patients who underwent PCI for the first time between January 2016 and December 2023, 153 were diagnosed with diffuse coronary artery disease. This condition is characterized by stenosis or wall irregularities that affect more than two-thirds of the left or right coronary artery vessel tree. In addition, significant stenosis was defined as a lesion affecting >50% of the lumen. 10 Figure S1 shows examples of diffuse coronary artery disease. Among 153 patients, 31 underwent iodine-123-β-methyl iodophenyl-pentadecanoic acid (BMIPP) myocardial scintigraphy before discharge or as outpatients. BMIPP scintigraphy was performed in patients who had undergone successful catheter-based revascularization. To ensure that the scan reflected stable myocardial metabolism, it was conducted only after at least 3 months had passed since the relief of ischemia. These patients were divided into the TGCV and non-TGCV groups. TGCV was diagnosed as a low washout rate of BMIPP (<10%) on BMIPP single-photon emission computed tomography as well as diffuse narrowing of the coronary arteries observed on coronary angiography. 11 Initially, lesions with coronary artery grafting (n = 1) and those without IVUS data (n = 8) were excluded. Subsequently, IB-IVUS findings on a lesion basis were analyzed, comparing 13 native coronary TGCV lesions and 31 non-TGCV lesions. Intraobserver and interobserver variabilities were determined by analysis of IVUS findings by two independent blinded observers and by the same observer at two different times. Finally, the incidence of major adverse cardiovascular events (MACEs) was assessed between the TGCV (n = 10) and non-TGCV (n = 21) groups on a patient basis.
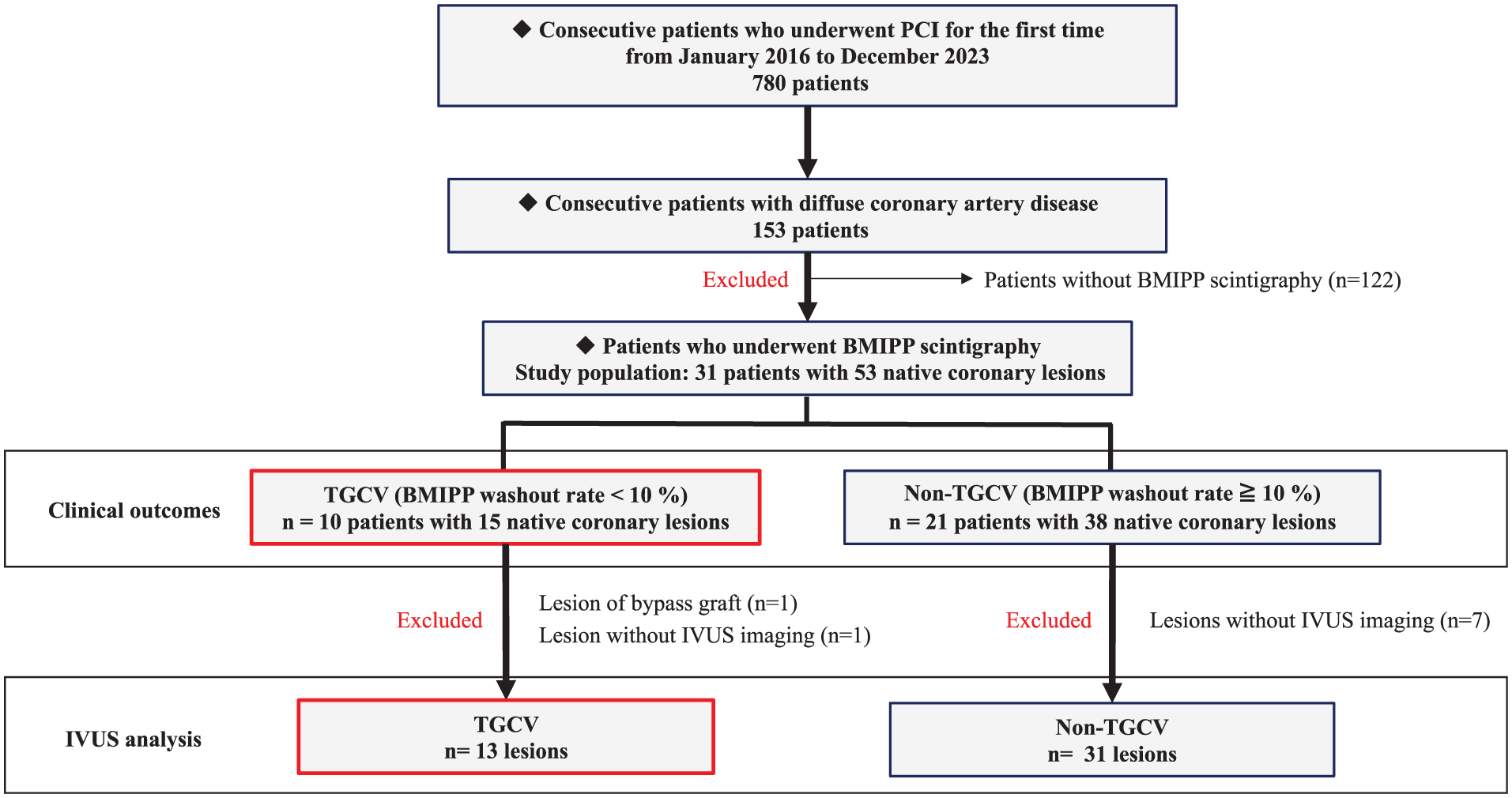
Study flowchart. Among 780 consecutive patients undergoing first-time PCI between January 2016 and December 2023, 153 had diffuse coronary artery disease. Among these 153 patients, 31 underwent BMIPP either before discharge or as outpatients. They were divided into the TGCV and non-TGCV groups. Ten patients were diagnosed with TGCV. The IVUS findings of 13 and 31 native coronary lesions were compared between the TGCV and non-TGCV groups. Lesions of coronary artery grafting (n = 1) and those without IVUS imaging (n = 8) were excluded. The difference in the incidence of major adverse cardiovascular events was assessed between the TGCV (n = 10) and non-TGCV (n = 21) group on a patient basis.
This study was approved by our hospital’s ethics committee. Considering this study’s retrospective design, written informed consent from patients was not obtained because this study only analyzed data that were previously collected as part of routine clinical care.
Angiographic analysis
Quantitative coronary angiography (QCA) was performed using QAngio XA7.3 (Medis Medical Imaging System B.V., Leiden, The Netherlands). The minimal lumen diameter, reference vessel diameter, plaque area percentage, and length of each lesion were quantified using the external diameter of the contrast-filled guiding catheter as the calibration standard.
Measurement of the BMIPP washout rate
Patients underwent BMIPP scintigraphy 20 and 200 min after the intravenous injection of BMIPP for early and delayed data acquisition, respectively. Early and delayed images were imported to create short-axis sum images and adjusted for time–decay correction. The washout rate was calculated using the total counts on the early and delayed short-axis sum images. The washout rate (%) was calculated as follows: (early cardiac counts − −delayed cardiac counts)/early cardiac counts × 100. 12
IVUS and analysis
Figure S2 shows the IVUS measurements and analyses. A mechanical IVUS system (VISIWAVE; Terumo Corporation, Tokyo, Japan or VISICUBE; Ueda Japan Radio Corporation, Tokyo, Japan) equipped with 60-MHz (AltaView) imaging catheters (Terumo Corporation) was used for imaging. The IVUS catheter was advanced to the distal part of the culprit lesion and automatically retracted at a constant rate of 0.5–3.0 mm/s, beginning at least 5 mm distal to the culprit lesion and ending at the aorto-ostial junction. Conventional grayscale IVUS was performed immediately before PCI without preballoon dilatation. Offline grayscale and IB-IVUS analyses were performed using VISIATLAS (Terumo Corporation). Grayscale IVUS and IB-IVUS measurements were conducted along the whole length of the lesion at 1-mm intervals. The proximal/distal reference was defined as the largest lumen proximal/distal to an area of stenosis within the same segment, respectively. Lesions were defined as the accumulation of atherosclerotic plaque relative to a predefined reference. 13 Lesions subjected to PCI were analyzed. The lumen area and external elastic membrane (EEM) were assessed, and the plaque plus media area was calculated as follows: EEM area − lumen area. Plaque eccentricity was calculated using the following formula: (maximum plaque and media thickness − minimum plaque and media thickness)/maximum plaque and media thickness. The cross-sectional area per millimeter was measured for these variables.
Using the IB-IVUS software, the compositional tissue characteristic areas were automatically expressed as colors according to IB values (i.e. red, calcification; yellow, dense fibrous; green, fibrous; blue, lipid; purple, lipid or concealed). 14 Manually tracing and excluding the acoustic shadows of calcification and the guidewire minimized the effects of artifacts. The average percentage of each plaque component in the total plaque area was calculated.
Clinical endpoints
The follow-up period ended in April 2024. The median follow-up period was 518 days. Follow-up was conducted as documented on medical records. MACEs (i.e. after the performance of BMIPP myocardial scintigraphy) were defined as the occurrence of cardiac death, myocardial infarction, and hospitalization due to heart failure after the diagnosis of TGCV or non-TGCV. Cardiac death refers to death caused by a cardiac condition, including acute myocardial infarction, heart failure, fatal arrhythmias, and sudden cardiac death. Meanwhile, myocardial infarction was defined based on the fourth universal definition. 15 Hospitalization for heart failure was identified as an event that required treatment with diuretics, vasodilators, or cardiotonics in cases with decompensated heart failure symptoms.
Statistical analysis
JMP version 16.0 (SAS Institute, Inc., Cary, NC, USA) was used for statistical analyses. Data were analyzed at the patient and lesion levels. The χ2 test or Fisher’s exact test was used to compare categorical variables, where appropriate. Continuous variables were expressed as the median (interquartile range) or mean ± standard deviation, depending on the distribution. Normality was assessed prior to analysis, and Student’s t-test was applied for normally distributed variables, while the Wilcoxon rank-sum test was utilized for non-normally distributed variables. The log-rank test was applied to evaluate differences in the incidence of MACEs between the two groups, with Kaplan–Meier curves visualized to illustrate the time interval until events occurred. Significance was considered at p < 0.05. No imputation was performed for missing values; cases with missing data were excluded from the respective analyses. Multivariable analysis was not conducted due to small sample size. No subgroup or sensitivity analyses were conducted.
Results
The study included 31 patients with diffuse coronary artery disease who underwent PCI. Ten patients (32%) were diagnosed with TGCV (TGCV group). IVUS detected 13 native coronary lesions in the TGCV group and 31 in the non-TGCV group (n = 21 patients; Figure 1). The baseline characteristics of the patients were not significantly different between the two groups, including TG levels (Table 1). The two groups had comparable lesion characteristics, including QCA data (Table 2). For the subsequent lesion-based analysis, the IVUS findings were compared between TGCV and non-TGCV lesions. In the IB-IVUS analysis, the average ratio of the blue area (lipid area) was significantly smaller in TGCV lesions than in non-TGCV lesions (20.1%, 95% CI 19.3%–22.7% vs 23.2%, 95% CI 22.0%–24.3%; p = 0.021). Conversely, the average ratio of the red area (calcification area) tended to be larger in TGCV lesions than in non-TGCV lesions (5.0%, 95% CI 3.1%–5.8% vs 3.1%, 95% CI 2.2%–3.9%; p = 0.053; Figure 2(a)). The quantitative IVUS parameters are shown in Table 3. TGCV lesions had significantly lower mean plaque eccentricity than non-TGCV lesions (0.68 (0.54–0.79) vs 0.81 (0.72–0.86), p = 0.003), with significantly higher mean maximum plaque plus media thickness (1.2 (1.1–1.4) vs 1.4 (1.2–1.5) mm, p = 0.023) and lower mean minimum plaque plus media thickness (0.4 (0.2–0.5) vs 0.2 (0.2–0.4) mm, p = 0.042). The representative IVUS images of the TGCV and non-TGCV groups are compared in Figure 2(b).
Baseline clinical characteristics of the patients.
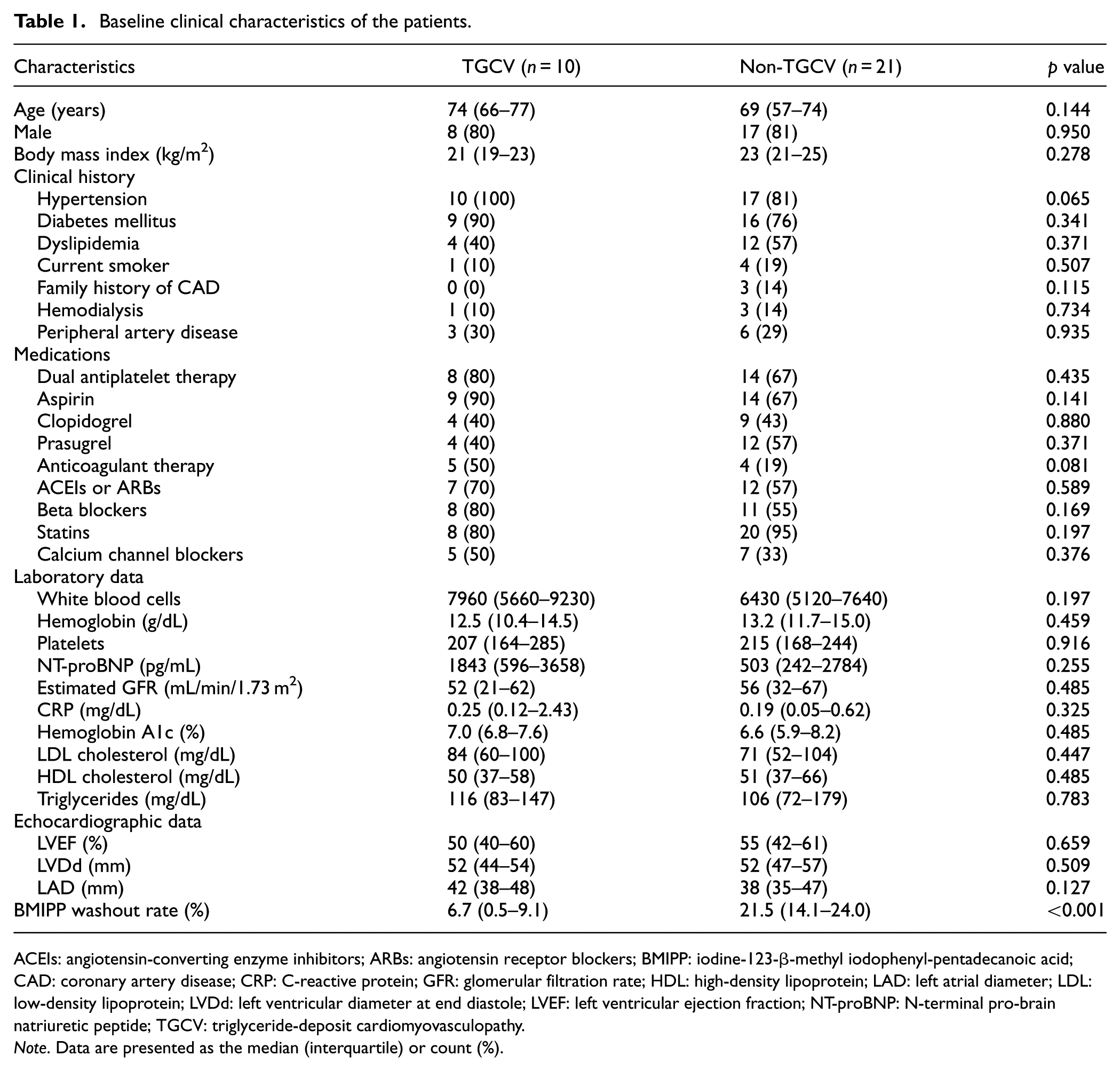
ACEIs: angiotensin-converting enzyme inhibitors; ARBs: angiotensin receptor blockers; BMIPP: iodine-123-β-methyl iodophenyl-pentadecanoic acid; CAD: coronary artery disease; CRP: C-reactive protein; GFR: glomerular filtration rate; HDL: high-density lipoprotein; LAD: left atrial diameter; LDL: low-density lipoprotein; LVDd: left ventricular diameter at end diastole; LVEF: left ventricular ejection fraction; NT-proBNP: N-terminal pro-brain natriuretic peptide; TGCV: triglyceride-deposit cardiomyovasculopathy.
Note. Data are presented as the median (interquartile) or count (%).
Baseline characteristics of TGCV and non-TGCV lesions.
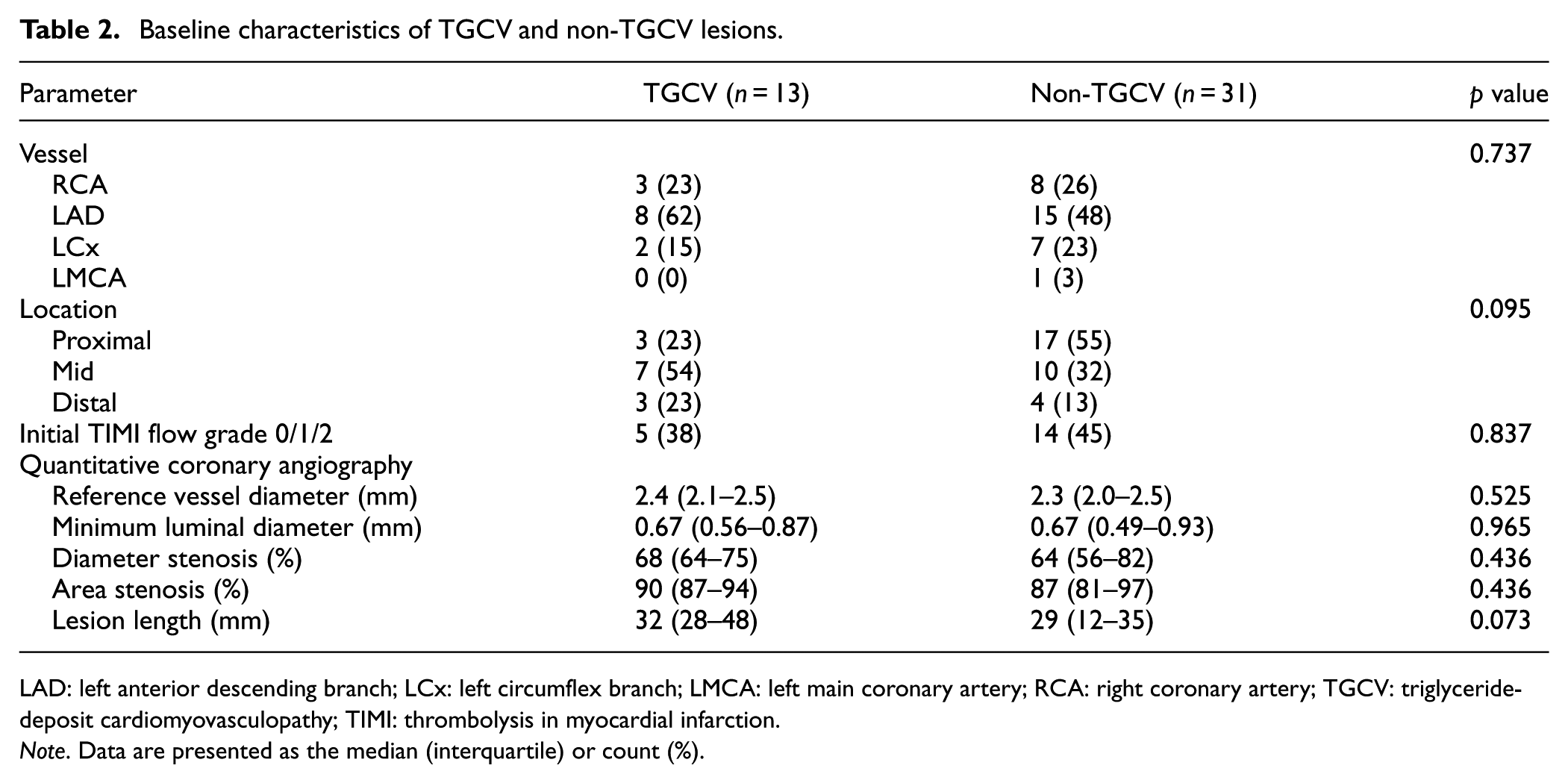
LAD: left anterior descending branch; LCx: left circumflex branch; LMCA: left main coronary artery; RCA: right coronary artery; TGCV: triglyceride-deposit cardiomyovasculopathy; TIMI: thrombolysis in myocardial infarction.
Note. Data are presented as the median (interquartile) or count (%).
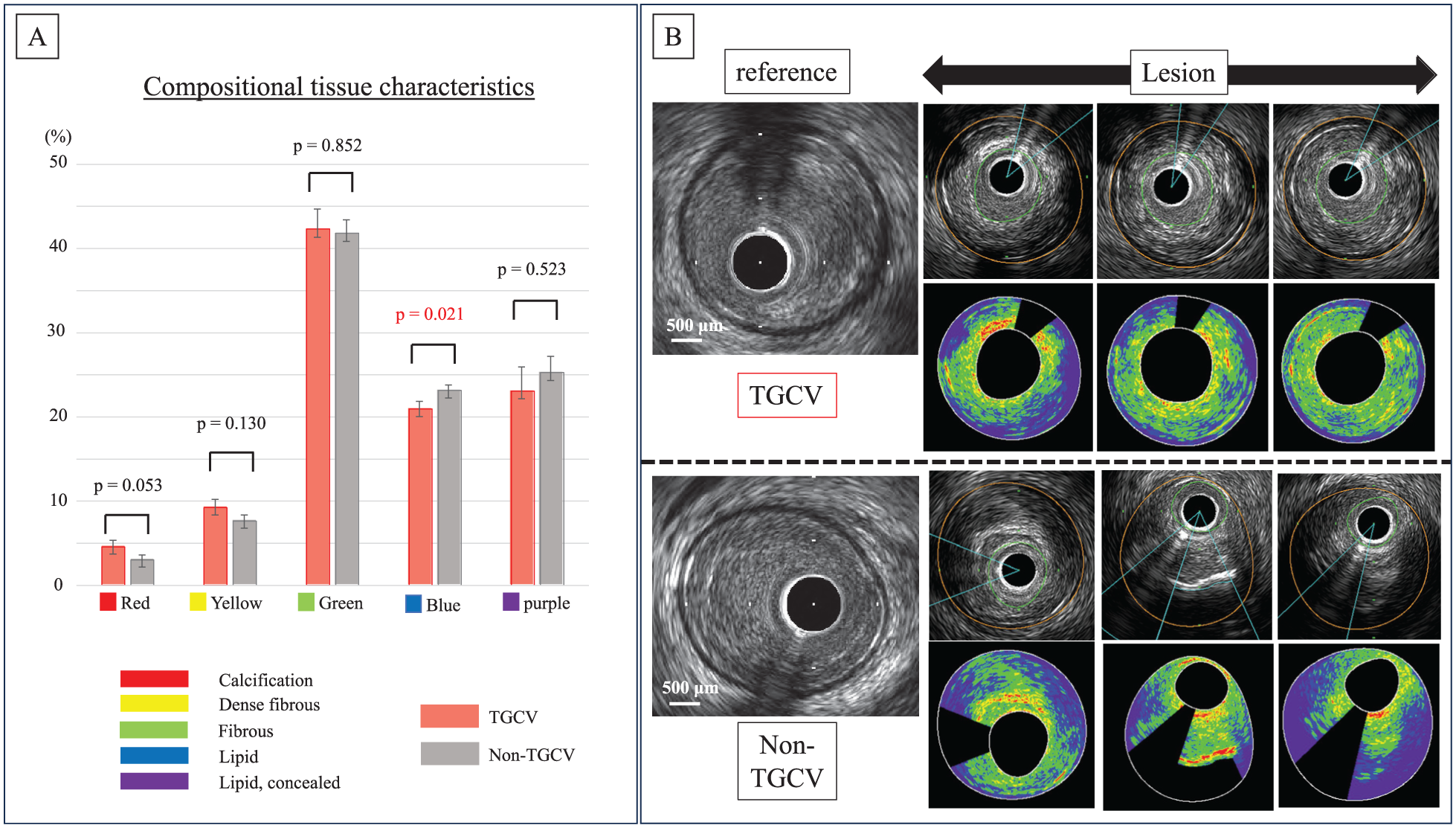
Compositional tissue characteristics and representative lesions of TGCV versus non-TGCV. (a) Compositional tissue characteristics in the IB-IVUS analysis: The average ratio of the blue area (lipid area) was significantly smaller in TGCV lesions than in non-TGCV lesions (20.1%, 95% CI 19.3%–22.7% vs 23.2%, 95% CI 22.0%–24.3%; p = 0.021). Conversely, the average ratio of the red area (calcification area) tended to be larger in TGCV lesions than in non-TGCV lesions (5.0%, 95% CI 3.1%–5.8% vs 3.1%, 95% CI 2.2%–3.9%; p = 0.053). (b) Representative right coronary artery lesions of TGCV versus non-TGCV: TGCV lesions exhibited smaller lipid areas and lower plaque eccentricity than non-TGCV lesions.
Intravascular ultrasound findings.
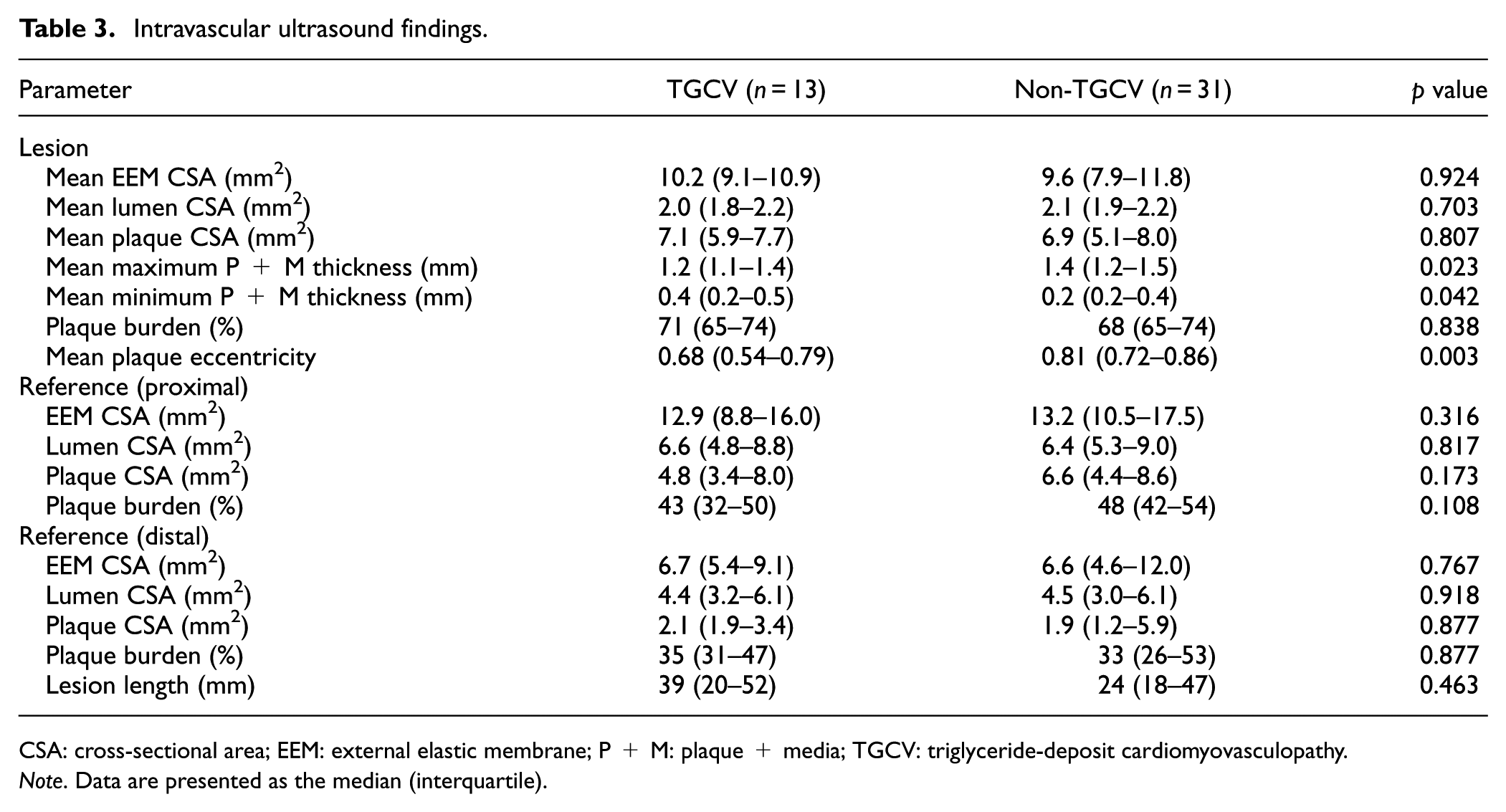
CSA: cross-sectional area; EEM: external elastic membrane; P + M: plaque + media; TGCV: triglyceride-deposit cardiomyovasculopathy.
Note. Data are presented as the median (interquartile).
A total of 7 (23%) patients experienced MACEs, including five in the TGCV group and two in the non-TGCV group. The Kaplan–Meier analysis found a significant difference in the incidence of MACEs between the two groups (log-rank test, p = 0.011; Figure 3). Table S1 summarizes the baseline characteristics and clinical outcomes of the 10 patients with TGCV. Among these patients, two died because of heart failure and three were admitted because of heart failure.
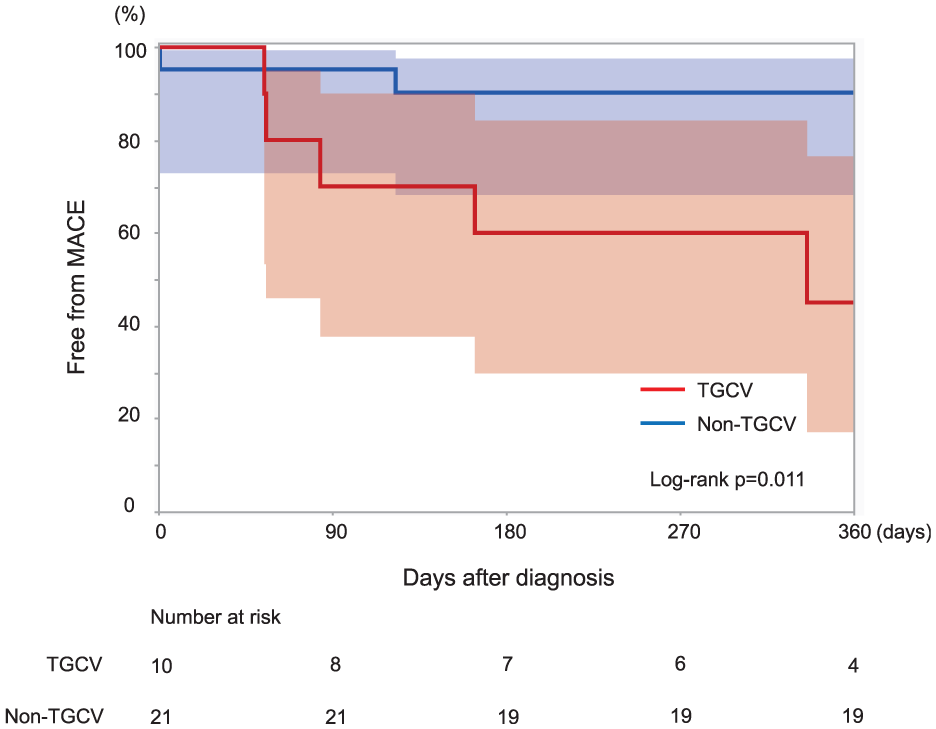
Clinical outcomes between TGCV and non-TGCV. Kaplan–Meier curves illustrating the occurrence of MACEs within 1 year in the TGCV group (red line) and non-TGCV group (blue line). A significant difference was noted in the incidence of MACE between the TGCV and non-TGCV groups in the Kaplan–Meier analysis (log-rank test, p = 0.011).
Mean intraobserver difference for the lumen area was 0.25 ± 0.30 mm2; mean interobserver difference was 0.50 ± 0.60 mm2. For the vessel area, mean intra- and interobserver differences were 0.90 ± 1.0 and 1.8 ± 2.0 mm2, respectively. Mean intraobserver difference for the lesion length was 3.0 ± 3.5 mm; mean interobserver difference was 6.0 ± 7.0 mm. For plaque eccentricity, mean intra- and interobserver differences were 0.07 ± 0.08 and 0.15 ± 0.18, respectively. Mean intraobserver difference for the blue area was 2.0% ± 2.5%; mean interobserver difference was 4.0% ± 5.0%.
Discussion
To our knowledge, this study is the first to investigate the characteristics of plaque composition and clinical outcomes of TGCV in patients with diffuse coronary artery disease. This study has some notable findings. First, IB-IVUS showed that the average ratio of the lipid area was significantly smaller in TGCV lesions than in non-TGCV lesions. Conversely, the average ratio of the calcification area tended to be larger in TGCV lesions. In addition, IVUS revealed that TGCV lesions had significantly lower plaque eccentricity, consistent with our previous findings. Second, TGCV might be associated with a higher risk of MACEs than non-TGCV among patients with diffuse coronary artery disease.
In Japan, 991 patients were diagnosed with TGCV in October 2024. However, in the present study, 10 out of 31 (32%) patients with diffuse coronary artery disease were diagnosed with TGCV. The observed high prevalence of TGCV in our cohort may be partly explained by selection bias. As a tertiary care university hospital, our institution frequently receives referrals for patients with advanced or complex coronary artery disease. In addition, BMIPP scintigraphy was predominantly performed in patients with particularly advanced diffuse coronary artery disease, potentially enriching the population with TGCV. However, it is also important to consider that TGCV remains an underrecognized and underdiagnosed condition, and its actual prevalence may be higher than previously thought. Recently, a study showed that TGCV was diagnosed in 20% of consecutive patients on hemodialysis with suspected coronary artery disease, and TGCV was significantly and independently associated with a higher risk to 5-year cardiovascular mortality. 16 In a separate study, 26 out of 62 patients with chronic heart failure (41.9%) were diagnosed with TGCV, and a reduction in the BMIPP washout rate was identified as a prognostic factor for patients with heart failure regardless of the presence of TGCV. 17 These findings indicate that TGCV might be latent in a considerable number of high-risk patient populations, such as those with diffuse coronary artery disease, individuals on hemodialysis, and patients with chronic heart failure. Moreover, the existence of TGCV appears to be another factor that worsens the prognosis within these vulnerable groups.
In patients with TGCV, the insufficiency of adipose TG lipase activity results in impaired hydrolysis of intracellular TGs. TGCV is classified into two subtypes depending on the presence and absence of a genetic mutation of PNPLA2 encoding adipose TG lipase, namely primary and idiopathic TGCV, respectively. 11 Primary TGCV develops from homozygous mutations; however, the heterozygote phenotype is unknown. A recent study in Japan identified only seven patients with primary TGCV, whereas ∼40,000–50,000 patients potentially have idiopathic TGCV. 6 The cause of idiopathic TGCV is currently unknown.
The pathogenesis of TGCV revolves around TG accumulation in the coronary arteries and cardiomyocytes. Consequently, patients with TGCV experience diffuse coronary artery disease, heart failure, and arrhythmia resistant to standard therapies, including lipid-lowering drugs and PCI. Recently, both basic and clinical studies have identified tricaprin as an effective treatment for TGCV. A registry study has reported remarkable long-term survival and durable recovery of heart failure in patients with TGCV treated with supplemental tricaprin. 18 Therefore, TGCV should be diagnosed while still at an early stage, and cardiovascular disease exacerbations should be prevented. To the best of our knowledge, this in vivo study is the first to describe the characteristics of plaque composition in patients with TGCV through IB-IVUS. These IB-IVUS findings may assist in the early diagnosis of TGCV. In countries where BMIPP scintigraphy is not available, the characteristic IB-IVUS findings described in this study—combined with our previously reported IVUS features of smaller plaque eccentricity and increased medial thickness 9 —may help identify patients in whom TGCV is suspected. While proton magnetic resonance spectroscopy can assess myocardial TG metabolism and may serve as an alternative diagnostic tool, its availability and technical complexity limit widespread use. Therefore, a stepwise approach may be feasible: first, screening with IVUS to identify patients at higher likelihood of TGCV, followed by targeted proton magnetic resonance spectroscopy evaluation in selected cases.
IB-IVUS has been developed for the quantitative tissue characterization of coronary plaques. IB-IVUS classifies plaque components into four categories based on echo intensity: red (calcification), yellow (dense fibrous tissue), green (fibrous tissue), and blue (lipid). 14 Previous studies that compared IB-IVUS findings with histopathological assessments have demonstrated that the blue region corresponds specifically to extracellular lipid accumulation and necrotic core formation, indicating advanced atherosclerotic lesions. 19 Furthermore, the lipid area in IB-IVUS was reported to be associated with future coronary events and procedural complications, such as slow flow during PCI. 20 In this study, the significantly low proportion of the lipid area in plaques associated with TGCV is an intriguing finding. Conventional atherosclerosis begins with endothelial injury, followed by macrophage infiltration and foam cell formation, resulting in the accumulation of extracellular lipid pools within the intima. As the disease advances, the apoptosis of foam cells results in the development of necrotic cores, 8 which appear as blue regions on IB-IVUS. Meanwhile, TGCV is characterized by the intracellular accumulation of TGs, particularly within vascular SMCs. These differences in accumulated lipid species and localization between TGCV and non-TGCV could influence echo attenuation, and this distinct pathophysiological feature could explain the observed differences in IB-IVUS findings. We hypothesize that intracellular TG droplets may scatter ultrasound more strongly, leading to an increased return of reflected signals and consequently a reduction of the blue-coded lipid area on IB-IVUS. This mechanism could be analogous to the phenomenon observed in hepatic steatosis, where intracellular fat droplets in hepatocytes scatter ultrasound and result in the “bright liver” appearance. 21 However, it is important to recognize that many TGCV patients exhibit concomitant TGs and cholesterol deposition. 22 Current intravascular imaging such as IB-IVUS are unable to discriminate between TG and cholesterol components. Raman spectroscopy and multimodal IVUS–Raman imaging have shown potential to provide molecular-level characterization of arterial lipid species. Such techniques may eventually enable differentiation between TGs and cholesterol deposition.
A recent study revealed that focal coronary artery disease was predominantly lipid-rich, whereas diffuse coronary artery disease exhibited a higher prevalence of calcification. 23 In the present study, which focused on patients with diffuse coronary artery disease, TGCV lesions had a relatively higher ratio of the calcification area than other diffuse coronary artery lesions. These findings indicate that intracellular TG accumulation may contribute to the differences in the tissue characteristics of these plaques.
Despite the lower proportion of the blue region, which is typically associated with clinical outcomes, several potential factors may contribute to the poor prognosis observed in TGCV. In this study, patients with TGCV showed a high incidence of heart failure-related mortality and hospitalizations. A previous study in patients with heart failure reported that lower BMIPP washout ratio is associated with poorer clinical outcomes, and has suggested that impaired myocardial fatty acid utilization, as reflected by a low BMIPP WOR, may contribute to adverse prognosis. 17 Based on this, we hypothesize that, in addition to the involvement of the epicardial coronary arteries, TGCV may also affect the coronary microcirculation. Such microvascular involvement could further contribute to adverse outcomes, and future studies are warranted to investigate this possibility.
Limitations
This study has some limitations. First, this was a single-center, retrospective, observational study. Because only 44 lesions were evaluated, the findings may not completely represent all the morphological features of coronary artery disease in patients with TGCV. In particular, the limited sample size may have reduced the statistical power to detect significant differences. The trend toward greater calcification in the TGCV group might have reached statistical significance with a larger cohort. Therefore, the conclusions drawn from this study should be interpreted with caution and regarded as preliminary. Furthermore, due to the limited sample size, we were unable to perform a multivariable analysis to adjust for potential confounding factors. This limitation prevents a definitive conclusion regarding the independent association between TGCV and MACEs. Thus, the findings should be validated in future studies with a larger sample size. Second, the selection of patients with BMIPP scintigraphy data could indicate bias. BMIPP scintigraphy was performed only on 31 out of 153 (20%) patients with diffuse coronary artery disease because it was limited to those who had achieved successful revascularization, were clinically stable at ∼3 months post-PCI, and were generally able to undergo the test in an outpatient setting. Therefore, BMIPP scintigraphy was not representative of the general population. Third, BMIPP scintigraphy, a key tool for diagnosing TGCV, is only available in Japan; thus, alternative screening methods are needed in other countries. Therefore, we hope that our IVUS findings of coronary artery disease of TGCV can help in its early detection during PCI. A recent study reported that micro-computed tomography provided near histological level of resolution. 24 These noninvasive imaging modalities may quantify the media thickness and should thus be explored. Fourth, given the limited resolution of IVUS, optical coherence tomography has been proposed as a high-resolution imaging method for plaque characterization. Finally, this study did not evaluate the duration of diabetes mellitus, which could have affected the findings of coronary artery disease.
Conclusions
IB-IVUS revealed that TGCV lesions exhibited a smaller average ratio of the lipid area than non-TGCV lesions, whereas the average ratio of the calcification area tended to be larger. These coronary IB-IVUS findings in TGCV may facilitate early disease detection. In patients with diffuse coronary artery disease, TGCV might be associated with a higher risk of MACEs than non-TGCV. Thus, in these patients, TGCV must be considered and diagnosed first. Once diagnosed, strict and continuous follow-up is essential to monitoring disease progression.
Supplemental Material
sj-docx-1-imj-10.1177_10815589251393918 – Supplemental material for Integrated backscatter intravascular ultrasound features of diffuse coronary artery disease with triglyceride-deposit atherosclerosis
Supplemental material, sj-docx-1-imj-10.1177_10815589251393918 for Integrated backscatter intravascular ultrasound features of diffuse coronary artery disease with triglyceride-deposit atherosclerosis by Takayuki Nakano, Hiroki Ikenaga, Ken-Ichi Hirano, Mikio Shigehara, Ayano Osawa, Yuichi Morita, Tasuku Higashihara, Noriaki Watanabe, Yoshiharu Sada and Yukiko Nakano in Journal of Investigative Medicine
Supplemental Material
sj-pdf-2-imj-10.1177_10815589251393918 – Supplemental material for Integrated backscatter intravascular ultrasound features of diffuse coronary artery disease with triglyceride-deposit atherosclerosis
Supplemental material, sj-pdf-2-imj-10.1177_10815589251393918 for Integrated backscatter intravascular ultrasound features of diffuse coronary artery disease with triglyceride-deposit atherosclerosis by Takayuki Nakano, Hiroki Ikenaga, Ken-Ichi Hirano, Mikio Shigehara, Ayano Osawa, Yuichi Morita, Tasuku Higashihara, Noriaki Watanabe, Yoshiharu Sada and Yukiko Nakano in Journal of Investigative Medicine
Supplemental Material
sj-pdf-3-imj-10.1177_10815589251393918 – Supplemental material for Integrated backscatter intravascular ultrasound features of diffuse coronary artery disease with triglyceride-deposit atherosclerosis
Supplemental material, sj-pdf-3-imj-10.1177_10815589251393918 for Integrated backscatter intravascular ultrasound features of diffuse coronary artery disease with triglyceride-deposit atherosclerosis by Takayuki Nakano, Hiroki Ikenaga, Ken-Ichi Hirano, Mikio Shigehara, Ayano Osawa, Yuichi Morita, Tasuku Higashihara, Noriaki Watanabe, Yoshiharu Sada and Yukiko Nakano in Journal of Investigative Medicine
Footnotes
Acknowledgements
We thank the Japan TGCV study group, of which the principal investigator is Ken-ichi Hirano, for providing the insights and expertise to our research.
Ethical considerations
This study was approved by our hospital’s ethics committee.
Author contributions
Takayuki Nakano: conceptualization, software, formal analysis, investigation, writing—original draft. Hiroki Ikenaga: supervision, methodology, writing—review and editing. Ken-ichi Hirano: supervision, writing—review and editing. Mikio Shigehara: investigation. Ayano Osawa: investigation. Yuichi Morita: investigation, supervision. Tasuku Higashihara: investigation, supervision. Noriaki Watanabe: investigation, supervision. Yoshiharu Sada: investigation, supervision. Yukiko Nakano: supervision, project administration.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data and study materials will not be made available to other researchers for purpose of reproducing the results or replicating the procedures.
Supplemental material
Supplemental material for this article is available online.