
Abstract
Serum total bile acid (BA) concentration, while linked to cardiovascular disease, lacks established associations with atrial fibrillation (AF). This cross-sectional study investigated the relationship between fasting serum total BA and AF prevalence/classification (paroxysmal vs persistent) in 522 patients aged ≥75 years. Participants were categorized by AF diagnosis and stratified by BA tertiles. Results revealed significantly lower serum total BA concentrations in AF patients compared to sinus rhythm controls. Notably, within the AF group, persistent cases exhibited lower BA levels than paroxysmal cases (3.00 (1.67–5.00) vs 3.80 (2.30–6.40) μmol/L, p = 0.005). Analysis demonstrated a nonlinear L-shaped relationship between BA and AF prevalence (inflection point: 4.08 μmol/L), with lower BA levels independently associated with higher AF risk (adjusted odds ratio = 1.84, 95% CI: (1.03–3.29), p = 0.040). These findings establish an L-shaped correlation, indicating reduced fasting serum total BA as an independent predictor for increased AF risk in the elderly.
Keywords
Introduction
Atrial fibrillation (AF), among the most prevalent cardiac arrhythmias, exhibits a significant age-dependent increase in incidence. 1 AF is associated with serious complications, which include stroke, heart failure, dementia, and renal insufficiency. Given this, AF remains a critical concern for clinicians and patients. Despite its clinical significance, the fundamental mechanisms driving AF initiation and perpetuation are incompletely understood.
Bile acids (BAs), classified as primary (synthesized in the liver) or secondary (generated by gut microbiota biotransformation of primary BAs), are essential regulators of cholesterol homeostasis and lipid metabolism.2–6 Functioning as signaling molecules, BAs modulate glycolipid metabolism through receptors such as the farnesoid X receptor (FXR) and Takeda G-protein receptor 5 (TGR5).7–9 Dysregulated BA metabolism is implicated in various metabolic disorders, such as obesity, diabetes, hypertension, atherosclerosis, and nonalcoholic fatty liver disease.5,10
The relationship between BAs and cardiovascular (CV) risk remains controversial. Elevated BA levels have been linked to cardiac dysfunction, while other evidence suggests a cardioprotective role. 11 Notably, impaired BA excretion correlates with increased coronary artery disease (CAD) incidence and mortality; postmenopausal women with CAD exhibit reduced fecal BA levels, identifying low BA excretion as an independent CAD risk predictor. 12 Conversely, studies report lower serum BA concentrations in heart failure patients compared with controls, alongside specific alterations in secondary BA profiles. 13 Low serum BAs were independently and significantly associated with the presence and severity of CAD. 14
Emerging evidence specifically links BA dysregulation to AF pathophysiology. Patients with AF demonstrate disrupted biotransformation of primary to secondary BAs and reduced fecal secondary BA proportions. 15 Specific BA species exert differential electrophysiological effects: taurocholic acid (TCA) induces atrial arrhythmias, while ursodeoxycholic acid (UDCA) does not. 15 AF is associated with altered BA conjugation profiles (higher non-UDCA conjugates, lower UDCA conjugates). 15 Furthermore, elevated chenodeoxycholic acid (CDCA) concentrations promote atrial myocyte apoptosis and left atrial low-voltage substrate formation. These processes are key factors in AF development. 16 Despite these mechanistic insights, large-scale clinical studies investigating the association between systemic BA levels and AF prevalence are scarce. Therefore, this study aimed to evaluate the relationship between serum total bile acid concentrations and the prevalence of atrial fibrillation.
Summary Box
Serum total bile acid (BA) concentrations are established as biomarkers associated with cardiovascular disease risk.
Atrial fibrillation (AF) is a prevalent age-related arrhythmia, but its specific link to circulating total BA levels remains unexplored.
Risk stratification of AF subtypes (paroxysmal vs persistent) relies on clinical factors, with no known biochemical predictors related to BA metabolism.
The first evidence of an inverse L-shaped relationship between fasting serum total BA and AF prevalence, with an inflection point at 4.08 μmol/L.
Persistent AF patients exhibit significantly lower BA levels than those with paroxysmal AF (3.00 vs 3.80 μmol/L, p = 0.005).
Low BA (<4.08 μmol/L) independently predicts 89% higher AF risk (adjusted OR = 1.84, 95% CI: 1.03–3.29, p = 0.040) in the elderly (≥75 years).
BA reduction may reflect underlying pathophysiological links between hepatointestinal function and AF progression.
Risk stratification tool: Serum BA could serve as a novel biomarker to identify elderly patients at high AF risk, complementing existing clinical scores.
Subtype monitoring: BA dynamics may help track AF progression from paroxysmal to persistent forms, enabling earlier intervention.
Mechanistic targeting: Findings motivate research into BA-mediated pathways (e.g., gut–heart axis) for future AF therapies.
Practical limitation: Validation of the 4.08 μmol/L threshold in multiethnic cohorts is needed prior to clinical adoption.
Methods
Study population
This cross-sectional study included 12,498 consecutive patients admitted to the Department of Cardiology at the First Affiliated Hospital of Xi’an Jiaotong University between January 2013 and December 2020. Exclusion criteria comprised (1) significant cardiac comorbidities (valvular heart disease, cardiomyopathy, coronary artery disease, or congenital heart disease); (2) pregnancy; (3) renal insufficiency (glomerular filtration rate <30 mL/min/1.73 m2) or hepatic insufficiency (serum total bilirubin >3 times the upper limit of normal value); and (4) missing data on total bilirubin, glomerular filtration rate, serum total BA, and left ventricular ejection fraction.
Final cohort and AF classification
After exclusions, 3890 patients were analyzed: 3044 with sinus rhythm (SR) and 846 with atrial fibrillation (AF), according to discharge diagnoses. AF was diagnosed as an electrocardiographic event with P-wave disappearance and absolute irregularity of the RR interval recorded on a 12-lead ECG or on a single-lead ECG recording ≥30-s. 17 Paroxysmal AF was defined as AF episodes lasting >30 s but terminated spontaneously or by intervention within 7 days of onset. 17 Persistent AF was defined as consecutive AF episodes lasting >7 days but <1 year. 17 Among patients with AF (n = 846), 629 had paroxysmal AF, 156 had persistent AF, and 61 were unclassifiable. The elderly subgroup (≥75 years; n = 522) comprised 290 SR patients and 232 AF patients (153 paroxysmal, 60 persistent, 19 unclassifiable; see Figure 1).
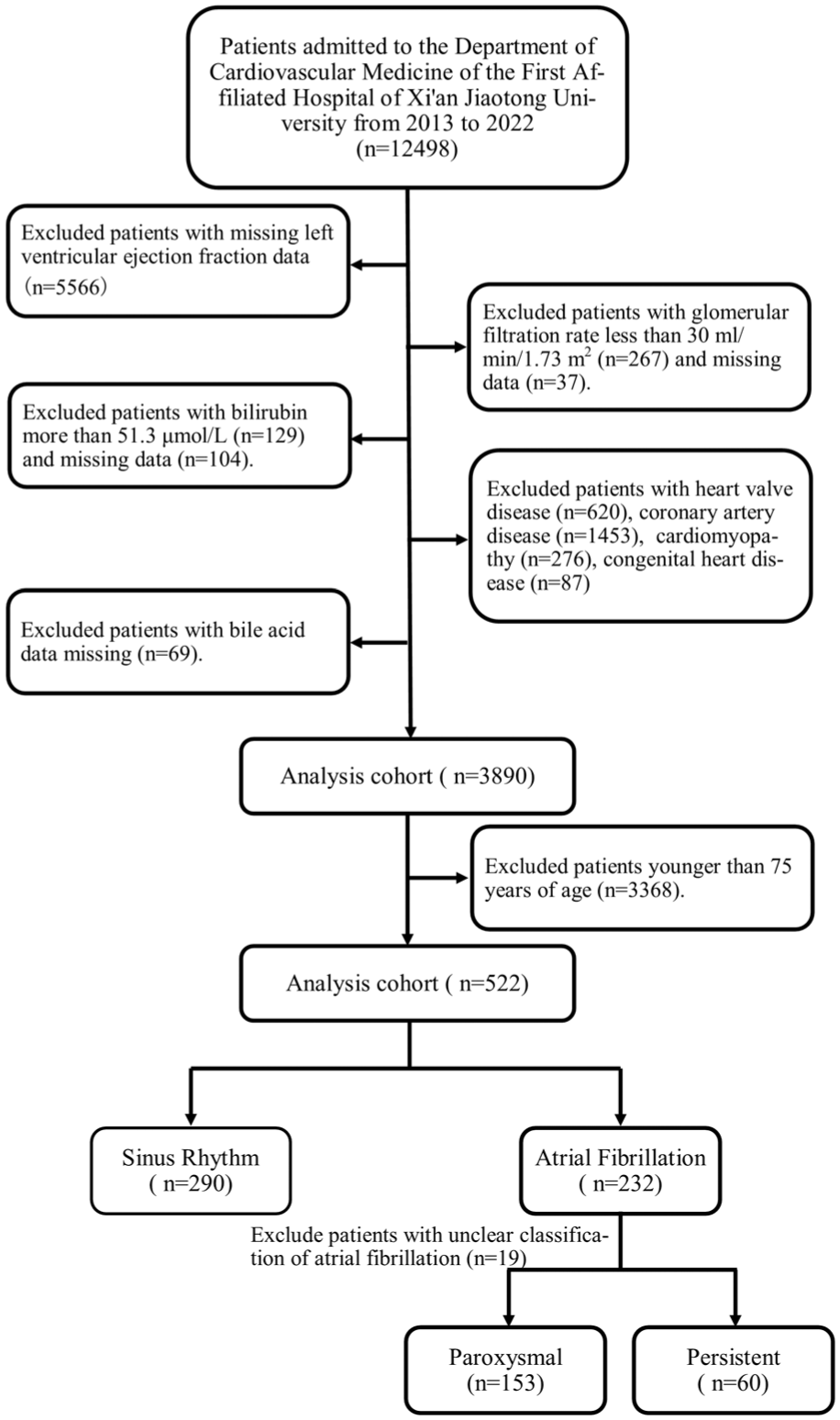
Study flow for the present analysis.
Data collection and ethics
Demographic, clinical, and laboratory data were systematically extracted from medical records. This study was approved by the Medical Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University (XJTU1AF2021LSL-007) and was conducted in accordance with the ethical principles of the Declaration of Helsinki. This was a cross-sectional study, and the data were anonymized to protect privacy when exported from the information base. It was reviewed and agreed by the Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University that it was not necessary to sign an informed consent form.
Laboratory and imaging measurements
Fasting serum total BA concentrations were quantified using an enzymatic cycling assay (Hitachi 7600 analyzer), with an upper reference limit of 10 μmol/L. All measurements underwent strict quality control protocols, demonstrating coefficients of variation <5%. Cardiac ultrasound measurements—obtained from the initial postadmission examination—included: left atrial internal diameter (LAD), left ventricular end-diastolic diameter (LVDd), left ventricular end-systolic diameter (LVDs), and the left ventricular ejection fraction (LVEF). Fasting venous blood samples (collected at admission or the next morning) were analyzed for cardiac function: N-terminal pro-brain natriuretic peptide (NT-pro BNP); lipid metabolism: apolipoprotein B (Apo B), apolipoprotein A (Apo A), total cholesterol (TC), high-density lipoprotein (HDL-C), low-density lipoprotein (LDL-C), triglycerides (TG); renal/hepatic function: glomerular filtration rate, albumin (ALB), total bilirubin, aspartate aminotransferase (AST); coagulation: activated partial thromboplastin time (APTT), international normalized ratio (INR), thrombin time (TT), fibrin degradation products, D-dimer; metabolic: HbA1c; hematologic: complete blood count; other: serum total BA. All assays followed standardized laboratory protocols.
Statistical analysis
Continuous variables were assessed for normality using the Kolmogorov–Smirnov test. If they followed a normal distribution, they were presented as mean ± standard deviation and analyzed using t-tests (two groups) or analysis of variance (ANOVA) (>2 groups). If they did not follow a normal distribution, they were expressed as median (interquartile range) and analyzed using the Mann–Whitney U test (two groups) or Kruskal–Wallis test (>2 groups). Categorical variables were expressed as frequencies (%) and compared using the chi-square (χ2) test. Multivariable logistic regression was used to evaluate the association between serum total bile acid (BA) concentrations and AF risk; results are reported as adjusted odds ratios (ORs) with 95% confidence intervals (CIs). Nonlinear relationships between total BA levels and AF risk were modeled using restricted cubic splines (RCS) with four knots.
Results
Baseline characteristics of the total population
The final cohort comprised 3890 patients: 3044 with SR and 846 with AF. Patients with AF were significantly older than SR controls (67 (58–76) years vs 56 (47–66) years, p < 0.001) and exhibited higher prevalence of: sick sinus syndrome (3.55% vs 0.56%, p < 0.001), hyperthyroidism (2.60% vs 0.33%, p < 0.001), chronic obstructive pulmonary disease (3.66% vs 0.69%, p < 0.001), pulmonary hypertension (3.90% vs 0.13%, p < 0.001). chronic kidney disease prevalence was comparable between groups (10.76% vs 9.40%, p = 0.264). AF patients demonstrated: reduced left ventricular ejection fraction (66% (61–69%) vs 68% (65–72%), p < 0.001), significantly enlarged left atrial diameter (38 (33–45) mm vs 31 (29–34) mm, p < 0.001). While median serum total BA levels were marginally higher in AF patients (3.80 (2.30–6.10) μmol/L) vs SR controls (3.60 (2.28–5.90) μmol/L), this difference was not statistically significant (p = 0.440) (complete data in Supplemental Table 1). The study included 785 AF patients (629 paroxysmal, 156 persistent). Patients with persistent AF were older, had larger left atrial internal diameters, and had worse cardiac and renal function than those with paroxysmal AF (all p < 0.05). Interestingly, BA levels were significantly lower in patients with persistent AF (3.45 (1.90–5.40) μmol/L) than in those with paroxysmal AF (3.80 (2.30–6.40) μmol/L) (p = 0.017) (Supplemental Table 2).
Baseline characteristics of the elderly Subgroup (≥75 years)
Given the strong age-dependent risk for AF, we specifically analyzed 522 elderly patients (≥75 years): 290 in SR and 232 with AF. Serum total BA concentrations were significantly lower in AF patients (3.45 (2.20–6.10) μmol/L) compared to SR controls (4.30 (2.80–7.40) μmol/L, p = 0.001) (Table 1). A total of 232 patients with AF, among whom 153 had paroxysmal AF, 60 had persistent AF, and 19 had unspecified AF type. Initial analysis showed that those with persistent AF exhibited lower BA levels (3.00 (1.67–5.00) μmol/L) than those with paroxysmal AF (3.80 (2.30–6.40) μmol/L, p = 0.005; Table 2). To evaluate the robustness of the results, we conducted two sensitivity analyses: First, when all 19 cases with unspecified AF type were assigned to the persistent AF group, the persistent AF group still exhibited significantly lower bile acid levels than the paroxysmal AF group (3.30 (1.70–5.10) μmol/L vs 3.80 (2.30–6.40) μmol/L, p = 0.010). Second, when all 19 unspecified cases were assigned to the paroxysmal AF group, the persistent AF group continued to show lower bile acid levels (3.00 (1.67–5.00) μmol/L vs 3.65 (2.30–6.43) μmol/L, p = 0.006). A significant inverse trend in AF prevalence was observed across increasing bile acid tertiles (Q1(<2.9 μmol/L): 54.49% vs Q2(≥2.9–<5.7 μmol/L): 41.34% vs Q3(≥5.7 μmol/L): 38.07%, p = 0.006), indicating decreasing AF prevalence with increasing BA levels (Table 3). Of particular note, a significant synergistic interaction was observed between advanced age (≥75 years) and low bile acid levels (Q1), as evidenced by a relative excess risk due to interaction (RERI) of 2.46 (95% CI: 0.29–4.63, p = 0.013), an attributable proportion (AP) of 0.42 (95% CI: 0.16–0.69, p = 0.001), and a synergy index (SI) of 2.05 (95% CI: 1.11–3.77, p = 0.011), indicating that the combined risk exceeded the sum of individual effects. In contrast, no significant interaction was found between age and higher bile acid levels (Q3) (Table 4).
Baseline characteristics by cardiac rhythm status in elderly patients (≥75 years): SR versus AF.
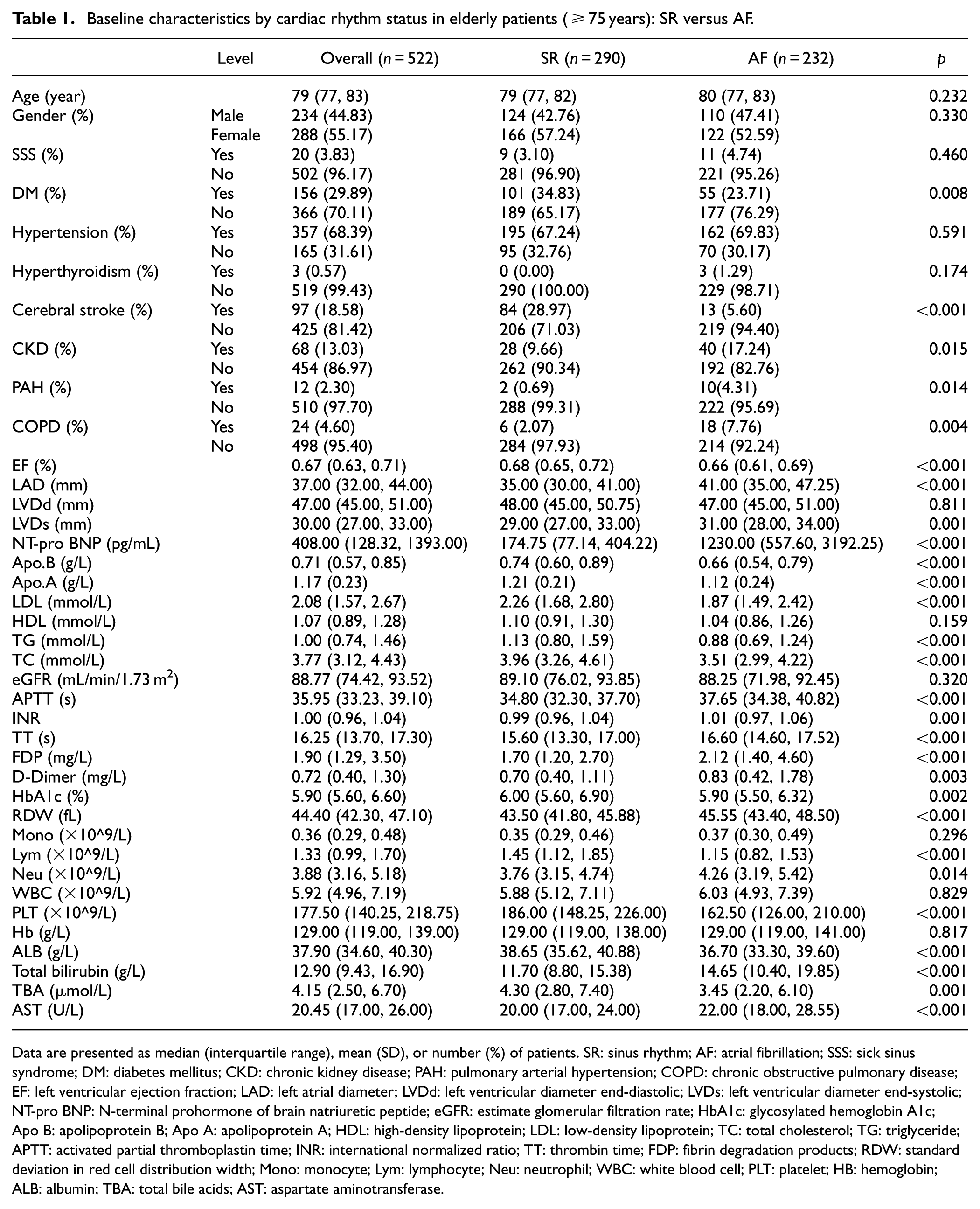
Data are presented as median (interquartile range), mean (SD), or number (%) of patients. SR: sinus rhythm; AF: atrial fibrillation; SSS: sick sinus syndrome; DM: diabetes mellitus; CKD: chronic kidney disease; PAH: pulmonary arterial hypertension; COPD: chronic obstructive pulmonary disease; EF: left ventricular ejection fraction; LAD: left atrial diameter; LVDd: left ventricular diameter end-diastolic; LVDs: left ventricular diameter end-systolic; NT-pro BNP: N-terminal prohormone of brain natriuretic peptide; eGFR: estimate glomerular filtration rate; HbA1c: glycosylated hemoglobin A1c; Apo B: apolipoprotein B; Apo A: apolipoprotein A; HDL: high-density lipoprotein; LDL: low-density lipoprotein; TC: total cholesterol; TG: triglyceride; APTT: activated partial thromboplastin time; INR: international normalized ratio; TT: thrombin time; FDP: fibrin degradation products; RDW: standard deviation in red cell distribution width; Mono: monocyte; Lym: lymphocyte; Neu: neutrophil; WBC: white blood cell; PLT: platelet; HB: hemoglobin; ALB: albumin; TBA: total bile acids; AST: aspartate aminotransferase.
Comparative baseline characteristics of paroxysmal versus persistent atrial fibrillation in elderly patients ≥75 years.
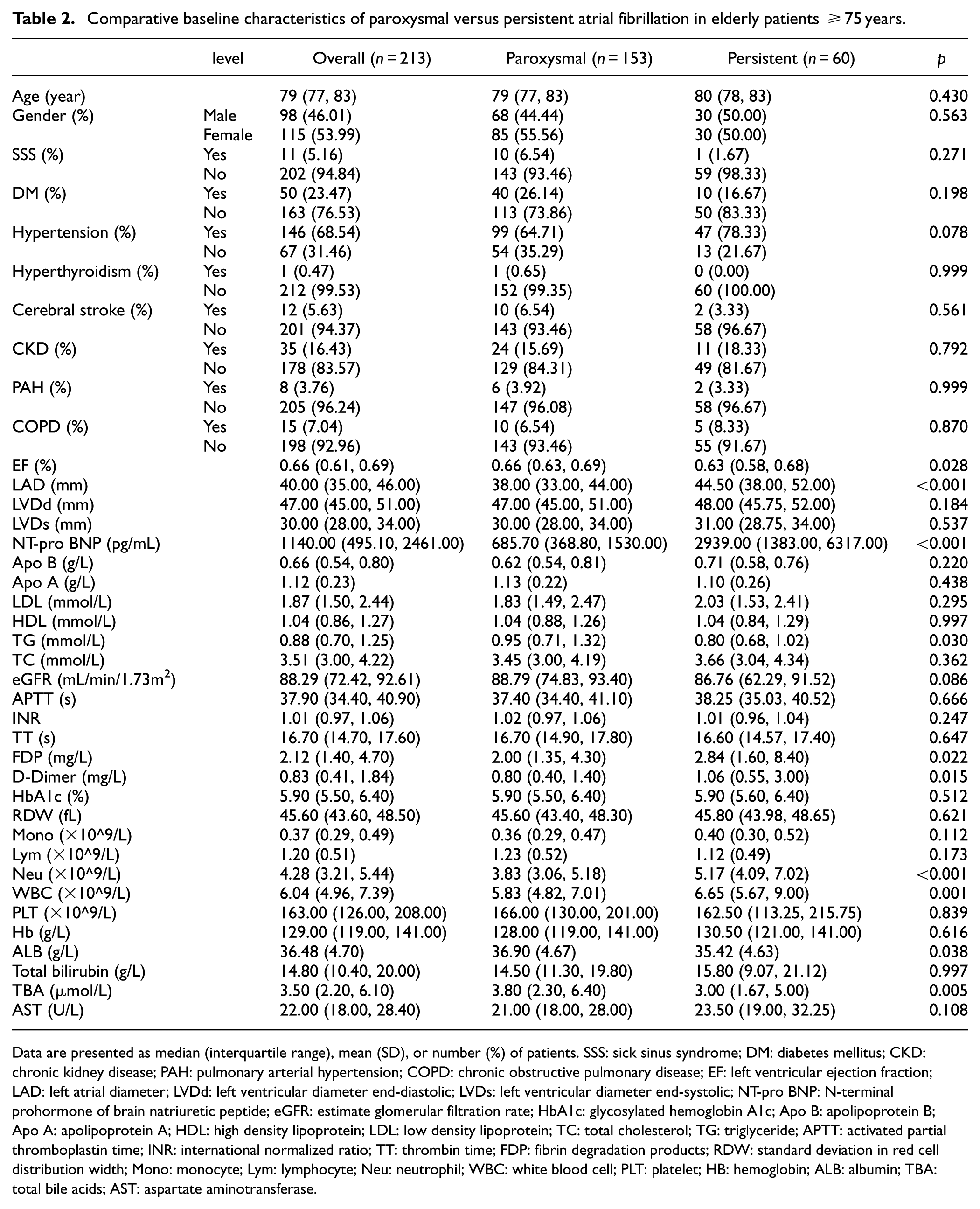
Data are presented as median (interquartile range), mean (SD), or number (%) of patients. SSS: sick sinus syndrome; DM: diabetes mellitus; CKD: chronic kidney disease; PAH: pulmonary arterial hypertension; COPD: chronic obstructive pulmonary disease; EF: left ventricular ejection fraction; LAD: left atrial diameter; LVDd: left ventricular diameter end-diastolic; LVDs: left ventricular diameter end-systolic; NT-pro BNP: N-terminal prohormone of brain natriuretic peptide; eGFR: estimate glomerular filtration rate; HbA1c: glycosylated hemoglobin A1c; Apo B: apolipoprotein B; Apo A: apolipoprotein A; HDL: high density lipoprotein; LDL: low density lipoprotein; TC: total cholesterol; TG: triglyceride; APTT: activated partial thromboplastin time; INR: international normalized ratio; TT: thrombin time; FDP: fibrin degradation products; RDW: standard deviation in red cell distribution width; Mono: monocyte; Lym: lymphocyte; Neu: neutrophil; WBC: white blood cell; PLT: platelet; HB: hemoglobin; ALB: albumin; TBA: total bile acids; AST: aspartate aminotransferase.
Comparative characteristics of elderly subjects (≥75 years) grouped by serum total bile acid levels.
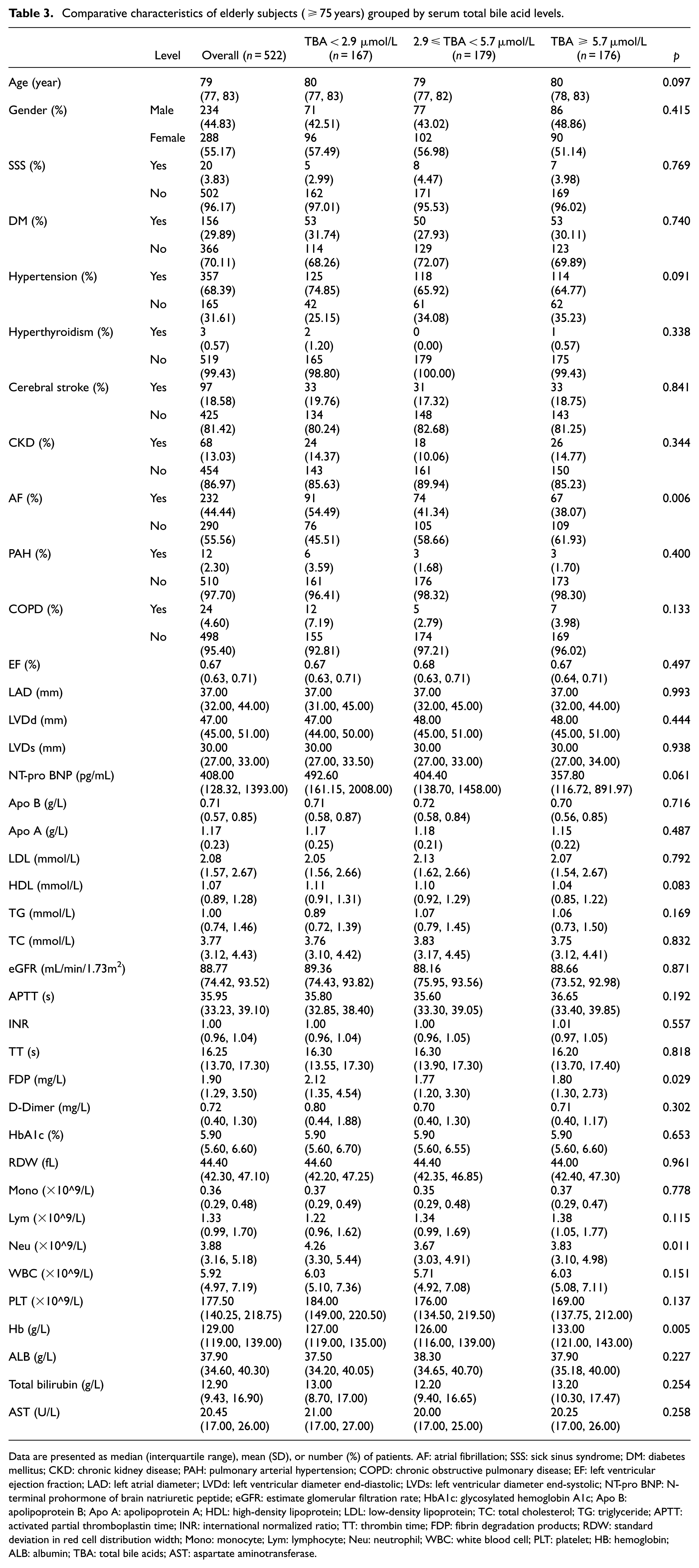
Data are presented as median (interquartile range), mean (SD), or number (%) of patients. AF: atrial fibrillation; SSS: sick sinus syndrome; DM: diabetes mellitus; CKD: chronic kidney disease; PAH: pulmonary arterial hypertension; COPD: chronic obstructive pulmonary disease; EF: left ventricular ejection fraction; LAD: left atrial diameter; LVDd: left ventricular diameter end-diastolic; LVDs: left ventricular diameter end-systolic; NT-pro BNP: N-terminal prohormone of brain natriuretic peptide; eGFR: estimate glomerular filtration rate; HbA1c: glycosylated hemoglobin A1c; Apo B: apolipoprotein B; Apo A: apolipoprotein A; HDL: high-density lipoprotein; LDL: low-density lipoprotein; TC: total cholesterol; TG: triglyceride; APTT: activated partial thromboplastin time; INR: international normalized ratio; TT: thrombin time; FDP: fibrin degradation products; RDW: standard deviation in red cell distribution width; Mono: monocyte; Lym: lymphocyte; Neu: neutrophil; WBC: white blood cell; PLT: platelet; HB: hemoglobin; ALB: albumin; TBA: total bile acids; AST: aspartate aminotransferase.
Interaction of age and bile acids for atrial fibrillation risk.
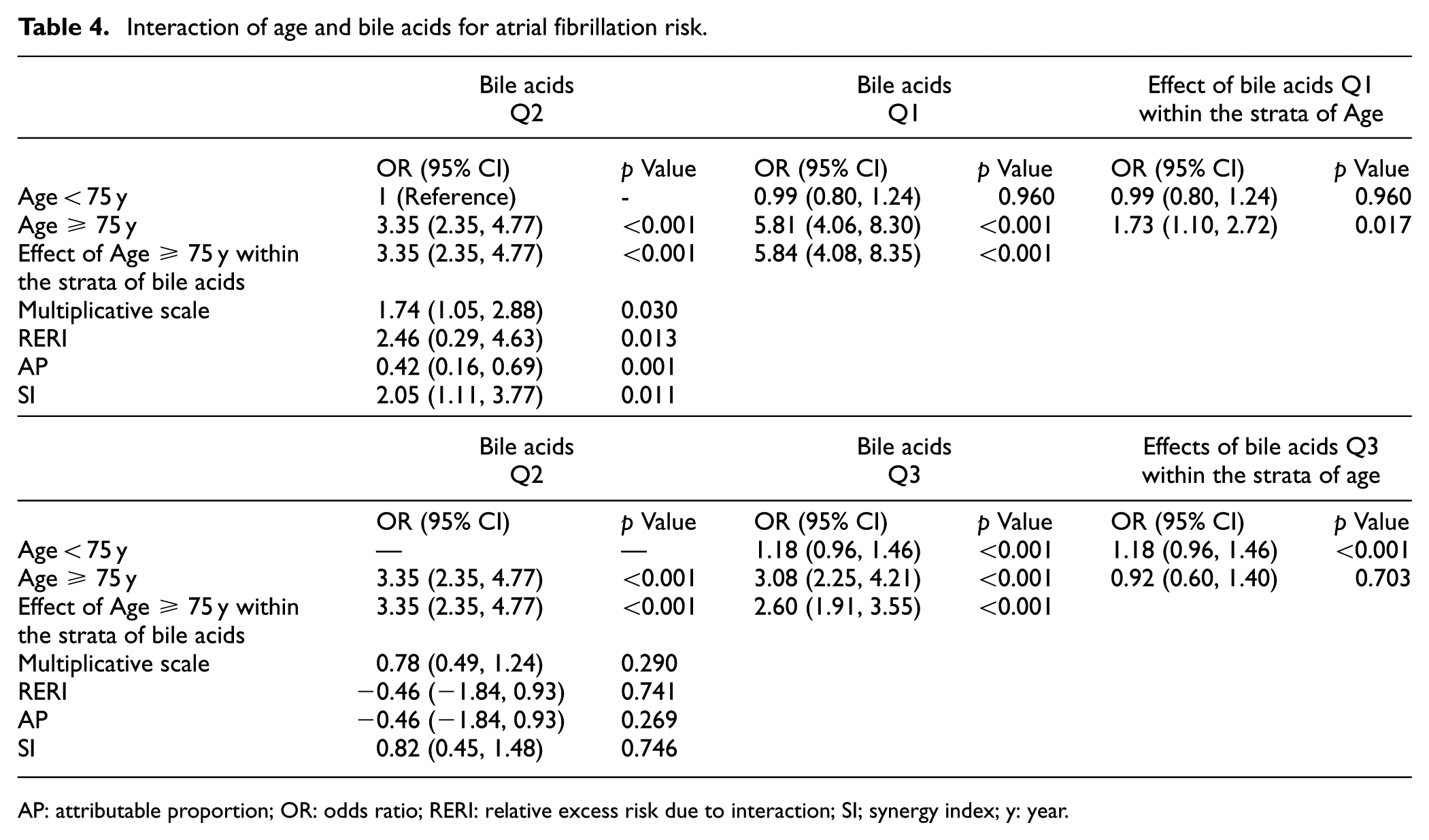
AP: attributable proportion; OR: odds ratio; RERI: relative excess risk due to interaction; SI; synergy index; y: year.
Association between bile acid levels and AF prevalence in the elderly subgroup (≥75 years)
Using the moderate BA concentration group as reference, logistic regression revealed significantly elevated AF risk in the low BA group across progressive adjustment models: Model 1 (unadjusted): OR = 1.70, 95% CI: 1.11–2.60, p = 0.015; Model 2 (age/sex-adjusted): OR = 1.67, 95% CI: 1.08–2.57, p = 0.020; Model 3 (fully adjusted): OR = 1.84, 95% CI: 1.03–3.29, p = 0.040 (Figure 2 and Supplemental Table 5). No significant risk difference was observed in the high versus moderate BA group. Restricted cubic spline analysis confirmed an L-shaped relationship (p < 0.001). AF risk decreased sharply with increasing BA concentrations below 4.08 μmol/L (inflection point). Risk reduction plateaued at higher BA levels. This nonlinear association remained significant after comprehensive adjustment for demographics (age, sex), comorbidities (sick sinus syndrome, diabetes, hypertension, hyperthyroidism, stroke, chronic kidney disease, pulmonary hypertension, chronic obstructive pulmonary disease), cardiac parameters (LVEF, LAD), metabolic marker (LDL cholesterol; Figure 3).
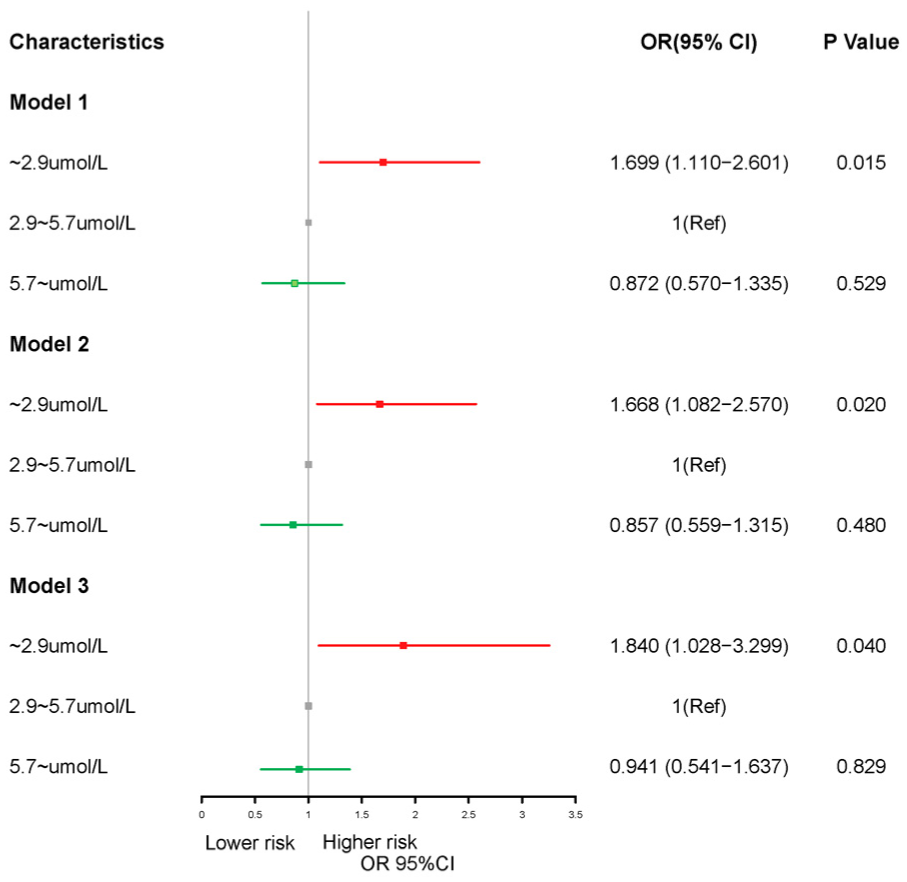
Odds ratios for atrial fibrillation by bile acid concentration group in logistic regression models.
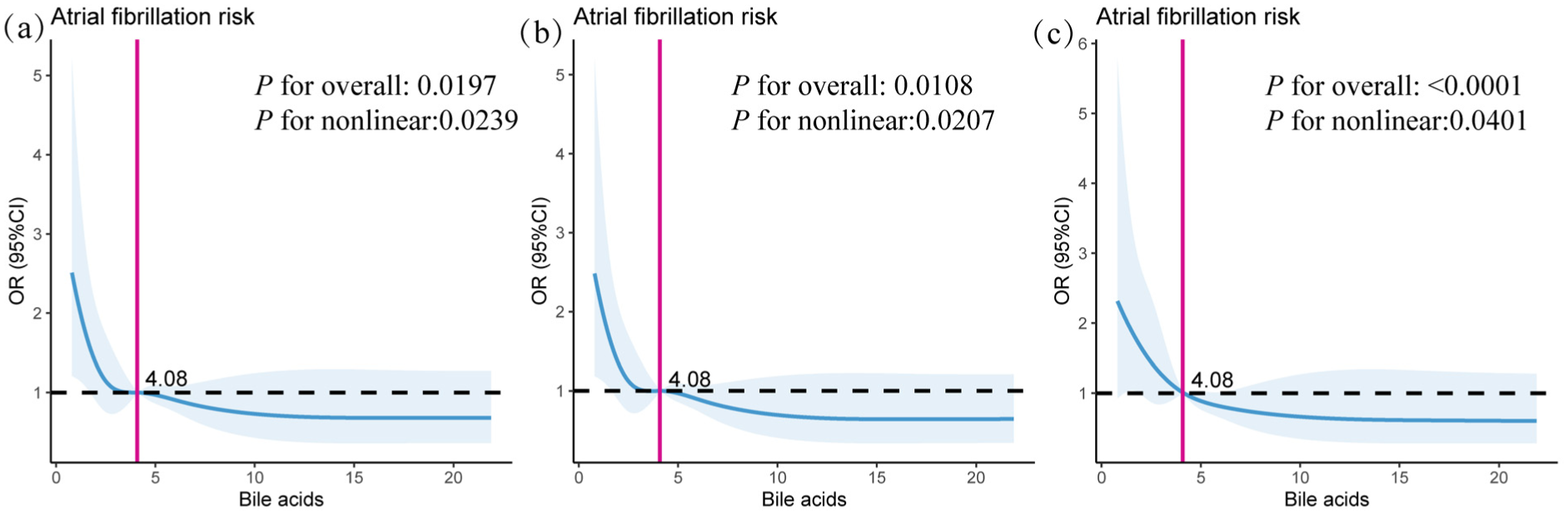
Restricted cubic spline curve showing L-shaped BA-AF risk association (inflection point = 4.08 μmol/L). Solid lines represent the odds ratio, dashed lines represent the 95% confidence intervals. (a) OR (95% CI) was unadjusted. (b) OR (95% CI) was adjusted by age, gender. (c) OR (95% CI) was adjusted by sick sinus syndrome, diabetes mellitus, hypertension, hyperthyroidism, cerebral stroke, chronic kidney disease, pulmonary hypertension, chronic obstructive pulmonary disease, EF, LAD, LDL.
Discussion
In this cross-sectional study of 522 elderly patients (≥75 years), we observed a significant nonlinear association between serum BA concentrations and AF prevalence. Specifically, restricted cubic spline analysis revealed an L-shaped relationship (inflection point: 4.08 μmol/L), indicating that the protective effect of BA against AF plateaus beyond this threshold while extremely low BA levels (<2.9 μmol/L) independently predicted 1.84-fold higher AF risk (95% CI: 1.03–3.29) after comprehensive adjustment. These findings suggest that low bile acid levels may serve as an important risk modifier specifically in the elderly population, potentially offering a novel biomarker for refined AF risk stratification in older adults.
While elevated circulating BAs have long been associated with cardiotoxicity (including bradyarrhythmias, cardiac arrest, and hypotension through direct cardiomyocyte effects), recent evidence suggests potential cardioprotective roles in coronary artery disease.14,18 Our findings add nuance to this paradox: although high total BA concentrations correlated with reduced AF prevalence in elderly patients, they did not emerge as an independent protective factor. Crucially, we identified low total BA levels as an independent AF risk predictor, where AF risk declined as BA concentrations increased, a pattern that contradicts classical cardiotoxicity models. This apparent contradiction may reflect differential effects of BA species. Notably, AF patients exhibit altered BA composition: elevated arrhythmogenic non-UDCA conjugates (e.g., taurocholic acid) and reduced protective UDCA conjugates. 15 Experimental data confirm that UDCA and its taurine conjugate lack pro-arrhythmic properties even at high concentrations. 15 Thus, BA composition, rather than merely its total concentration, may determine cardiovascular outcomes. This could explain divergent findings between coronary artery disease (where total BA may be protective 14 ) and atrial fibrillation (where specific pro-arrhythmic species dominate). Future studies should prioritize characterizing BA compositional shifts in cardiovascular pathologies.
BA-induced arrhythmogenesis operates through ion channel modulation and receptor-mediated pathways, with effects critically dependent on molecular composition. Sodium taurocholate (TCA) exerts dose-dependent proarrhythmic effects by: (1) suppressing L-type calcium currents, inhibiting phase 0 depolarization; (2) reducing delayed rectifier potassium currents, impairing phase 4 repolarization—collectively depressing sinoatrial node automaticity and potentially causing bradycardia or asystole.19,20 Taurocholate affects the calcium activity of cardiomyocytes and thus impairs their contractile properties. TCA concentration-dependently induced atrial extra contractions, whereas UDCA was not effective. At the cellular level, TCA depolarizes resting membrane potentials, enhances Na+/Ca2+ exchanger currents to trigger afterdepolarizations, 15 and downregulates T-type calcium channels, slowing conduction velocity and prolonging PR intervals. 21 Crucially, UDCA counteracts these effects by preserving T-type channel density 21 and demonstrates no arrhythmogenic activity even at high concentrations. 15 Beyond ion channels, BAs activate nuclear receptors with divergent effects: muscarinic receptors (MR) primarily mediate arrhythmogenesis,22,23 while FXR and TGR5 predominantly regulate metabolic functions linked to atherosclerosis and hypertension.24,25 During the aging process, the composition of the gut microbiota and the patterns and concentrations of microbial bile acid metabolism change with advancing age. The effects of bile acids are further modulated by inflammation in elderly patients.26,27 Within the aging population, altered bile acid metabolism may lead to increased cardiac sensitivity to bile acids, particularly during episodes of AF. 28 Moreover, studies have shown that the FXR–FGF15/19 signaling pathway is downregulated in elderly men and aged male mice. This downregulation may contribute to the development of arrhythmias. 29 This mechanistic duality underscores why BA composition, rather than total concentration, determines electrophysiological outcomes. The potent proarrhythmic properties of TCA versus the protective profile of UDCA highlight the clinical necessity to evaluate specific BA species. Current limitations include insufficient characterization of individual BA electrophysiological effects and isomer-specific actions. Future research must prioritize deconvoluting these mechanisms to develop targeted interventions for BA-related arrhythmias.
Although this is the first study to report an L-shaped relationship between baseline BA levels and AF prevalence, several limitations warrant consideration. First, this cross-sectional study identifies a significant correlation between bile acid levels and atrial fibrillation risk; however, due to the study design, causal inference cannot be drawn. Prospective studies are needed to further elucidate the directionality and underlying mechanisms of this association. Second, despite controlling for potential confounders through multivariate adjustment, residual confounding cannot be ruled out. Furthermore, the study assessed only the effect of total BA levels on AF risk and did not address potential alterations in BA composition associated with AF. Therefore, future studies should incorporate bile acid subtyping to clarify the specific roles of TCA, UDCA, and other bile acids in atrial remodeling and arrhythmogenesis in elderly patients.
Conclusion
We observed an L-shaped, inverse association between fasting serum total BA levels and AF prevalence, which was especially evident in patients aged ≥75 years. This suggests that low BA levels may represent a novel risk factor for AF in the elderly population.
Supplemental Material
sj-docx-2-imj-10.1177_10815589251393974 – Supplemental material for L-Shaped association of fasting serum total bile acids with atrial fibrillation risk in the elderly
Supplemental material, sj-docx-2-imj-10.1177_10815589251393974 for L-Shaped association of fasting serum total bile acids with atrial fibrillation risk in the elderly by Qian Li, Shanshan Li, Rong Fan, Yi Zhao, Hui Liu, Tao Wang and Tao Zheng in Journal of Investigative Medicine
Supplemental Material
sj-docx-3-imj-10.1177_10815589251393974 – Supplemental material for L-Shaped association of fasting serum total bile acids with atrial fibrillation risk in the elderly
Supplemental material, sj-docx-3-imj-10.1177_10815589251393974 for L-Shaped association of fasting serum total bile acids with atrial fibrillation risk in the elderly by Qian Li, Shanshan Li, Rong Fan, Yi Zhao, Hui Liu, Tao Wang and Tao Zheng in Journal of Investigative Medicine
Supplemental Material
sj-docx-4-imj-10.1177_10815589251393974 – Supplemental material for L-Shaped association of fasting serum total bile acids with atrial fibrillation risk in the elderly
Supplemental material, sj-docx-4-imj-10.1177_10815589251393974 for L-Shaped association of fasting serum total bile acids with atrial fibrillation risk in the elderly by Qian Li, Shanshan Li, Rong Fan, Yi Zhao, Hui Liu, Tao Wang and Tao Zheng in Journal of Investigative Medicine
Supplemental Material
sj-docx-5-imj-10.1177_10815589251393974 – Supplemental material for L-Shaped association of fasting serum total bile acids with atrial fibrillation risk in the elderly
Supplemental material, sj-docx-5-imj-10.1177_10815589251393974 for L-Shaped association of fasting serum total bile acids with atrial fibrillation risk in the elderly by Qian Li, Shanshan Li, Rong Fan, Yi Zhao, Hui Liu, Tao Wang and Tao Zheng in Journal of Investigative Medicine
Supplemental Material
sj-docx-6-imj-10.1177_10815589251393974 – Supplemental material for L-Shaped association of fasting serum total bile acids with atrial fibrillation risk in the elderly
Supplemental material, sj-docx-6-imj-10.1177_10815589251393974 for L-Shaped association of fasting serum total bile acids with atrial fibrillation risk in the elderly by Qian Li, Shanshan Li, Rong Fan, Yi Zhao, Hui Liu, Tao Wang and Tao Zheng in Journal of Investigative Medicine
Supplemental Material
sj-tif-1-imj-10.1177_10815589251393974 – Supplemental material for L-Shaped association of fasting serum total bile acids with atrial fibrillation risk in the elderly
Supplemental material, sj-tif-1-imj-10.1177_10815589251393974 for L-Shaped association of fasting serum total bile acids with atrial fibrillation risk in the elderly by Qian Li, Shanshan Li, Rong Fan, Yi Zhao, Hui Liu, Tao Wang and Tao Zheng in Journal of Investigative Medicine
Footnotes
Appendix
Acknowledgements
We acknowledged the contributions of Biospecimen Information Resource Center, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, China for creating and updating the clinical database.
Ethics considerations and informed consent
This study was approved by the Medical Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University (XJTU1AF2021LSL-007) and was conducted in accordance with the ethical principles of the Declaration of Helsinki. This was a cross-sectional study, and the data were anonymized to protect privacy when exported from the information base. It was reviewed and agreed by the Ethics Committee of the First Affiliated Hospital of Xi’an Jiaotong University that it was not necessary to sign an informed consent form.
Consent for publication
Not applicable.
Author contributions
Qian Li, Shanshan Li, Rong Fan, Yi Zhao, Hui Liu, Tao Wang and Tao Zheng designed the study. Hui Liu extracted the data. Qian Li, Shanshan Li, Rong Fan, Yi Zhao, Tao Wang and Tao Zheng analyzed and interpreted the data. Qian Li drafted the manuscript. Shanshan Li and Tao Zheng revised the manuscript. All authors gave final approval of the final version to be published.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Research Fund of the First Affiliated Hospital of Xi’an Jiaotong University (2021ZXY-21).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The anonymized participant data that support the findings of this study are available on request from the corresponding author. Proposals will be reviewed on the basis of scientific merit, ethical review, available resources and regulatory requirements. After approval of a proposal, anonymized data will be made available for reuse. A steering committee will have the right to review and comment on any draft papers based on these data before publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.