
Abstract
There is limited data regarding the correlation between interleukin-22 (IL-22) levels and psoriasis severity or body mass index (BMI). In addition, few studies have investigated the prevalence of different toxigenic strains of Staphylococcus aureus in psoriasis and their association with disease severity and BMI. This cross-sectional study examined the prevalence of S. aureus skin colonization in patients with psoriasis and its correlation with serum IL-22 levels, disease severity, and BMI. S. aureus isolates were identified, and their toxigenic strains were detected by polymerase chain reaction. Serum IL-22 levels were measured using an enzyme-linked immunosorbent assay. A majority of patients (60.2%) demonstrated S. aureus colonization in both lesional and nonlesional skin. In lesional skin, 45.2% of patients were colonized by toxigenic strains, with the SEB strain being the most prevalent (24.7% cases). In contrast, 47.3% of patients showed colonization by nontoxigenic strains in nonlesional skin. Colonization by toxigenic strains was significantly higher in lesional skin, whereas colonization by nontoxigenic strains was markedly higher in nonlesional skin (p = 0.001 for each). Both psoriasis severity and pruritus intensity were significantly greater among patients colonized with toxigenic strains (p = 0.001 each). Mean serum IL-22 levels were also significantly higher in patients with severe disease and pruritus (p = 0.001 each). Moreover, serum IL-22 levels showed strong positive correlations with BMI, psoriasis severity, and pruritus severity (p = 0.002, 0.0001, and 0.0001, respectively). This study highlights significant associations between S. aureus colonization, particularly the toxigenic strain SEB and psoriasis severity, serum IL-22 levels, and BMI. Further large-scale studies are warranted to validate these findings.
Keywords
Introduction
Psoriasis is a chronic inflammatory disease affecting approximately 2%–3% of the population. 1 It is characterized by cutaneous lesions and systemic comorbidities such as cardiovascular diseases and insulin resistance.2,3 Psoriasis has a significant negative impact on patients’ quality of life and imposes considerable economic burdens. 4
The etiopathogenesis of psoriasis is complex and primarily mediated by T-helper 1 (T-h1) and Th17 immune responses, along with autoinflammatory mechanisms.5,6 Among the cytokines produced by activated Th1 cells is interleukin-22 (IL-22), a member of the IL-10 cytokine family. IL-22 promotes keratinocyte proliferation, inhibits cellular differentiation, and enhances antimicrobial defense, suggesting its potential role in the pathogenesis of psoriasis. 7
These pathogenic processes can be triggered by environmental factors, particularly infectious agents. 8 Several studies have demonstrated that both cutaneous dysbiosis and loss of immune tolerance to skin commensal flora contribute to psoriasis pathogenesis.9,10
Staphylococcus aureus has been implicated in the pathogenesis of psoriasis in genetically predisposed individuals. 11 Several studies have reported that S. aureus colonization in patients with psoriasis is approximately 4.5 times higher than colonization in healthy individuals. 12 Moreover, a higher proportion of S. aureus isolates from patients with psoriasis are toxigenic (enterotoxins-producing) strains, which have been significantly correlated with disease severity.13,14
The major staphylococcal toxins include enterotoxins A, B, and C (SEA, SEB, SEC), toxic shock syndrome toxin-1 (TSST-1), and exfoliative toxin. These enterotoxins contribute to psoriasis pathogenesis by acting as superantigens. Superantigens are presented to T-cell receptors at the Vβ region after binding to major histocompatibility complex class II molecules, leading to an exaggerated cellular immune response.15–17
Multiple studies have shown that IL-22 can influence metabolic processes through activation of the Janus kinase–signal transducer and activator of transcription 3 (JAK-STAT3) pathway both in vivo and in vitro.18,19 Shen et al. 20 reported a negative correlation between serum IL-22 levels and body mass index (BMI). However, the direct effect of IL-22 on metabolism remains underexplored.
Despite evidence suggesting the involvement of IL-22 in the pathogenesis of psoriasis, 7 data regarding its correlation with psoriasis severity and BMI are limited. Moreover, although multiple studies have confirmed the predominance of toxigenic S. aureus strains in psoriasis and their correlation with disease severity,12–14,16,17 limited research has examined the prevalence of different toxigenic strains and the correlation of each strain with psoriasis severity and BMI.
Accordingly, we conducted a cross-sectional, within-patient comparative study to evaluate the prevalence of S. aureus skin colonization in patients with psoriasis and to assess its correlation with serum IL-22 levels, disease severity, and BMI. In addition, we aimed to identify the presence of superantigen genes in S. aureus isolates colonizing psoriatic skin to enhance understanding of psoriasis pathogenesis and to explore potential therapeutic targets.
Summary Box
Data assessing the correlation between interleukin-22 (IL-22) levels and psoriasis severity, as well as body mass index (BMI), are lacking.
Few studies have investigated the prevalence of different toxigenic Staphylococcus aureus strains in psoriasis and the correlation of each strain with disease severity and BMI.
The majority of patients (60.2%) exhibited S. aureus colonization on both lesional and nonlesional skin.
This study demonstrated significant associations between S. aureus colonization, particularly toxigenic strain B, and disease severity, serum IL-22 levels, and BMI in patients with psoriasis.
The findings provide a basis for developing therapeutic approaches that target both S. aureus and IL-22 in the management of severe psoriasis.
Further studies are warranted to explore the causal relationship between S. aureus colonization and IL-22 levels in psoriasis.
Materials and methods
Study design
This study was a cross-sectional, within-patient comparative study.
Study setting
This study was conducted in the Dermatology Outpatient Clinic, Kobry El Kobba Hospital, and the Medical Microbiology and Immunology Department, Armed Forces College of Medicine, Cairo, Egypt.
Patients’ recruitment
Adult male and female patients with a clinical and histopathological diagnosis of psoriasis, representing varying degrees of disease severity, were recruited from the Dermatology Outpatient Clinic of Kobry El Kobba Hospital, Cairo, Egypt, between December 2023 and September 2024.
Exclusion criteria:
Patients were excluded if they had one or more of the following conditions:
Dermatologic diseases other than psoriasis or other autoimmune disorders
Treatment for psoriasis at the time of recruitment or any treatment received within the 6 months preceding the study
Signs or symptoms of acute skin infection
Sampling
Sample type:
It was a non-probability convenience sample.
Sample size calculation:
The sample size was calculated based on previously published data by Jassim et al., 21 which reported that 59% of psoriasis lesions showed positive S. aureus colonization. Assuming a 95% confidence level and a 10% precision level, the required sample size for this study was estimated to be 93 patients with psoriasis.
Methods
All patients were subjected to the following steps:
Body surface area (BSA) 22 : Mild, BSA < 5; Moderate, BSA 5–10; Severe, BSA > 10.
Psoriasis area and severity index (PASI): The PASI score was calculated for each patient according to Augustin et al. 23
Ten-point pruritus visual analog scale 24 : Patients were asked to subjectively rate pruritus intensity from 0 to 10, where 0 = no pruritus; >0–<4 = mild pruritus; ≥4–<7 = moderate pruritus; ≥7–<9 = severe pruritus; and ≥9 = very severe pruritus.
Skin swabs: Specimens were collected from both lesional and nonlesional skin to detect the S. aureus colonization. Nonlesional skin was defined as clinically normal skin located at >10 cm away from a psoriatic lesion.
Peripheral venous blood (5–10 mL) was collected from each patient for serum IL-22 measurement. Serum was separated and stored at −80°C until analysis by enzyme-linked immunosorbent assay (ELISA).
Specimens were inoculated onto 10% blood agar and mannitol salt agar (OxoidTM, Basingstoke, Hampshire, UK) plates and incubated at 37°C for 24 h. S. aureus was identified by conventional microbiological methods as described by Shabgah et al. 27 The isolates were then inoculated into Mueller–Hinton broth supplemented with 40% glycerol (OxoidTM, UK) 28 and stored at −80°C until further analysis for toxin genes by polymerase chain reaction (PCR). Detection of Staphylococcal enterotoxins A, B, and C, as well as TSST-1, was performed using a multiplex PCR assay, with the femA gene serving as an internal positive control, according to the method of Witte et al. 29 Genomic DNA was extracted using the QIAamp DNA Mini Kit (Qiagen, Germantown, Maryland, USA) following the manufacturer’s instructions. The primer sequences used in the multiplex PCR are listed in Table 1.
Sequences of the used primers
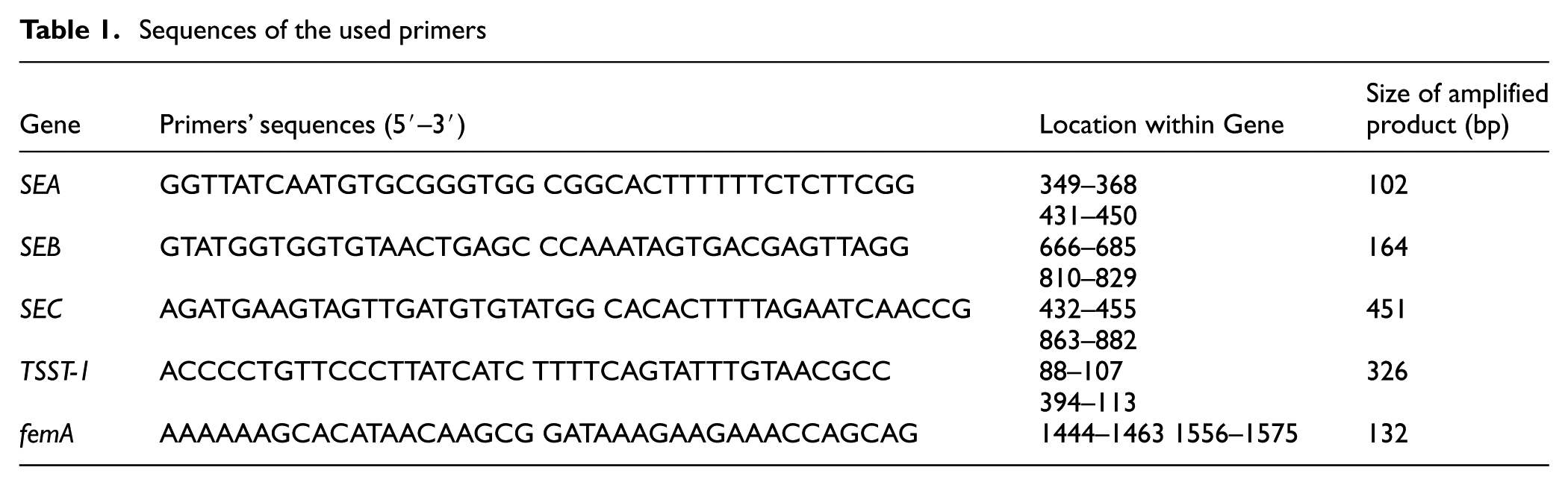
The PCR was performed in a total volume of 50 μL, consisting of 5 μL of 10× primer mixture (0.2 μM of each primer), 0.5 μL of DNA template, and 12.5 µL of PCR Master Mix (Qiagen, Hilden, North Rhine-Westphalia, Germany). The final volume was adjusted to 50 μL with RNase-free water provided in the kit. The PCR conditions included an initial denaturation at 95°C for 15 min to activate HotStart Taq polymerase, followed by 40 amplification cycles consisting of denaturation at 95°C for 45 s, annealing at 55°C for 45 s, and extension at 72°C for 1 min. Amplified PCR products were resolved by electrophoresis on a 2% agarose gel stained with ethidium bromide. DNA bands were visualized under an ultraviolet illumination using a transilluminator. Positive samples produced distinct bright bands on the gel, while negative samples showed no bands, indicating the absence of the corresponding toxin gene (Figure 1).
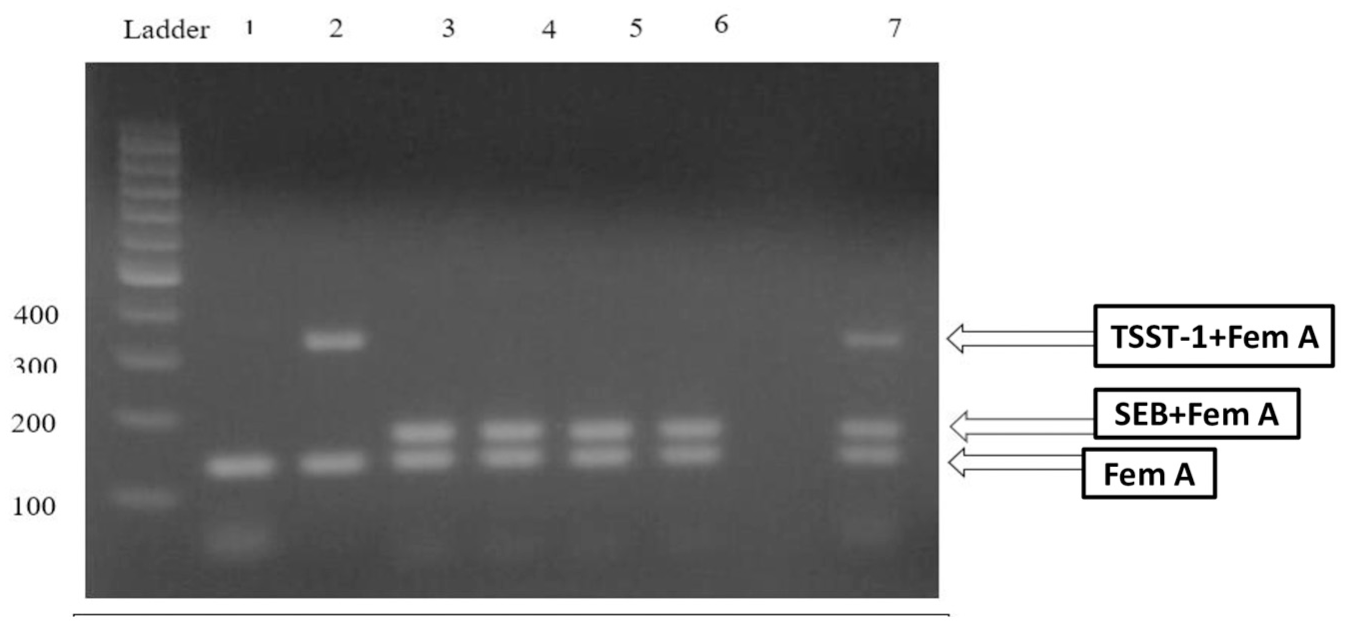
Multiplex PCR amplification products for the S. aureus superantigen genes on agarose gel.
Statistical analysis
The collected data were reviewed, coded, tabulated, and entered into a personal computer using the Statistical Package for the Social Sciences (IBM Corp., Released 2017. IBM SPSS Statistics for Windows, Version 25.0, Armonk, NY, USA). Data were presented, and appropriate analyses were performed according to the type of data obtained for each parameter.
The Shapiro–Wilk test was used to assess the normality of continuous data.
Parametric numerical data were expressed as mean, standard deviation (SD), and range.
Nonparametric data were expressed as median and interquartile range. Categorical (nonnumeric) data were presented as frequency and percentage.
The analysis of variance (ANOVA) test was used to assess the statistical significance of differences between the means of more than two study groups. The Bonferroni post hoc test was applied for pairwise comparisons of group means. The Kruskal–Wallis test was used to assess the statistical significance of differences between nonparametric variables across more than two study groups, followed by the Dunn–Bonferroni post hoc test for pairwise comparisons. The McNemar test was used to assess the statistical significance of differences in a qualitative variable measured twice within the same study group. t-Test was used to compare numerical variables of negative and nontoxigenic colonization groups. Correlation analysis (using Spearman’s or Pearson’s method) was performed to assess the strength and direction of association between two quantitative variables. The correlation coefficient (denoted as “r”) represents the strength and direction of the linear relationship between two variables. Spearman’s method was used for nonnormally distributed or data with outliers, while Pearson’s method was used for normally distributed data.
The Chi-square test was used to examine relationships between two qualitative variables. Fisher’s exact test was applied when the expected count was less than five in more than 20% of cells.
Level of significance:
-p > 0.05: Not significant (NS).
-p < 0.05: Significant (S).
-p < 0.01: Highly significant (HS).
Results
This cross-sectional, within-patient comparative study included 93 adult Egyptian patients who were clinically and histopathologically diagnosed with psoriasis.
Clinical characteristics of study participants
Among the study participants, 78 patients (83.9%) were male and 15 patients (16.1%) were female. The patients’ ages ranged from 21 to 71 years, with a mean of 36.6 ± 9.9 years. The BMI ranged from 18.3 to 30.1 kg/m2, with a mean of 25.1 ± 2.56 kg/m2. The duration of psoriasis ranged from 5 months to 4.16 years, with a mean of 19.7 ± 8.95 months. The BSA affected ranged from 5% to 85%, with a mean of 40.31% ± 20.12. The PASI score ranged from 3 to 72, with a mean of 33.56 ± 23.81. The serum IL-22 level ranged from 695.60 to 1055.60 pg/mL, with a mean of 950.16 ± 82.86 pg/mL.
Regarding the clinical variant of psoriasis, 51 patients (54.8%) had plaque psoriasis, 24 patients (25.8%) had guttate psoriasis, and both pustular and inverse psoriasis were observed in nine patients each (9.7% each). In terms of disease severity, 42 patients (45.2%) had severe psoriasis, 37 patients (39.8%) had moderate psoriasis, and 14 patients (15.1%) had mild psoriasis.
Regarding pruritus intensity, 41 patients (44.1%) experienced severe pruritus, 28 patients (30.1%) moderate pruritus, and 24 patients (25.8%) mild pruritus.
S. aureus colonization in lesional and nonlesional skin
Overall, 56 patients (60.2%) demonstrated S. aureus colonization in both lesional and nonlesional skin. In lesional skin, 42 patients (45.2%) were colonized by toxigenic strains, while 14 patients (15.1%) were colonized by nontoxigenic strains. The most prevalent toxigenic strain was SEB, detected in 23 patients (24.7%), followed by SEA in 11 patients (11.8%), SEC in five patients (5.4%), and TSST-1 in three patients (3.2%).
In nonlesional skin, 44 patients (47.3%) were colonized by nontoxigenic strains, while 12 patients (12.9%) were colonized by toxigenic strains. The most prevalent toxigenic strain was SEB in seven patients (7.5%), followed by SEA in three patients (3.2%) and SEC in two patients (2.2%), while the TSST-1 strain was not detected in nonlesional skin.
Colonization by toxigenic strains was significantly higher in lesional skin than in nonlesional skin (p = 0.001, McNemar test). Conversely, colonization by nontoxigenic strains was markedly higher in nonlesional skin than in lesional skin (p = 0.001; McNemar test; Figures 2 and 3).
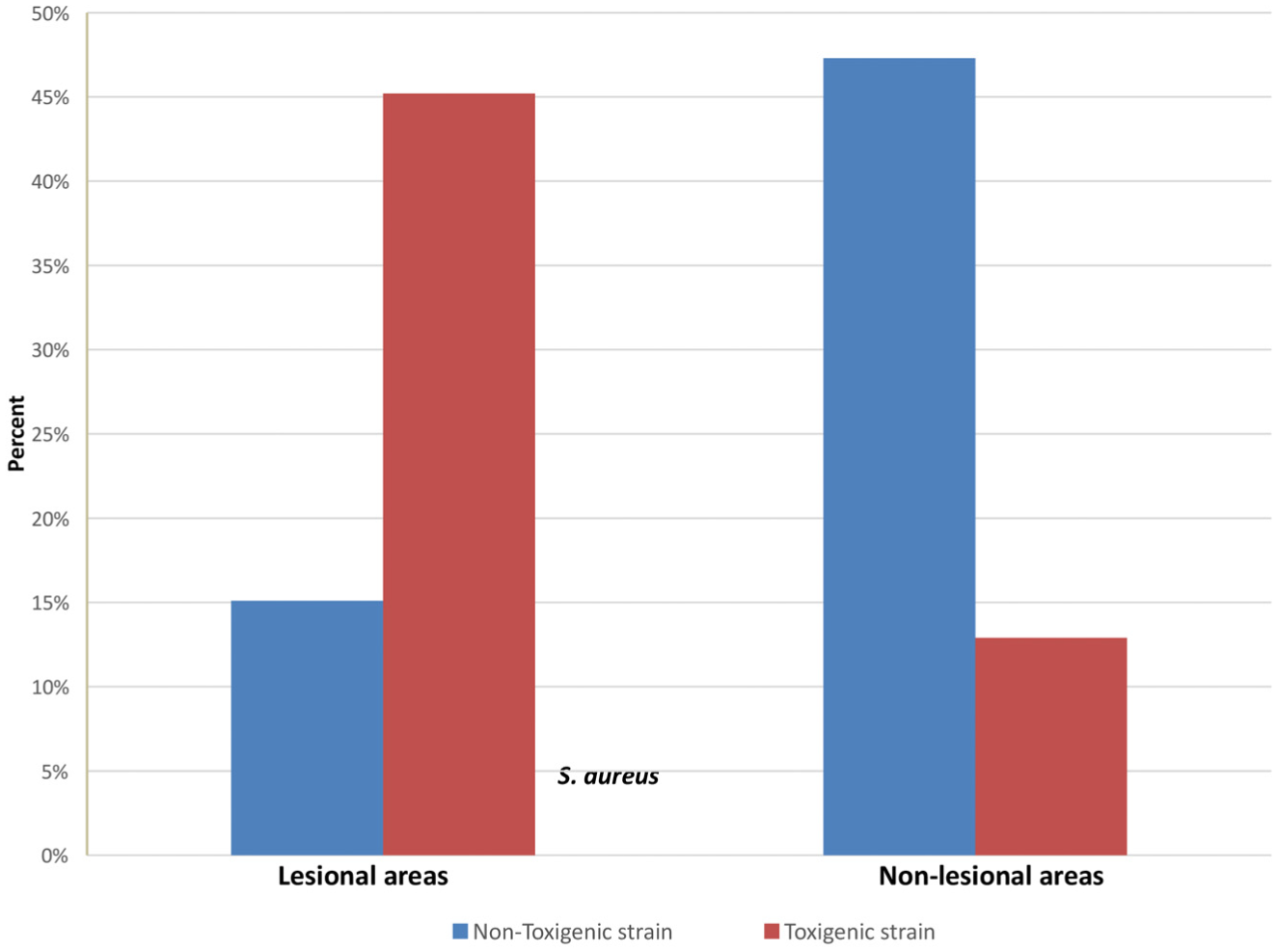
Description of S. aureus colonization among lesional and nonlesional areas.
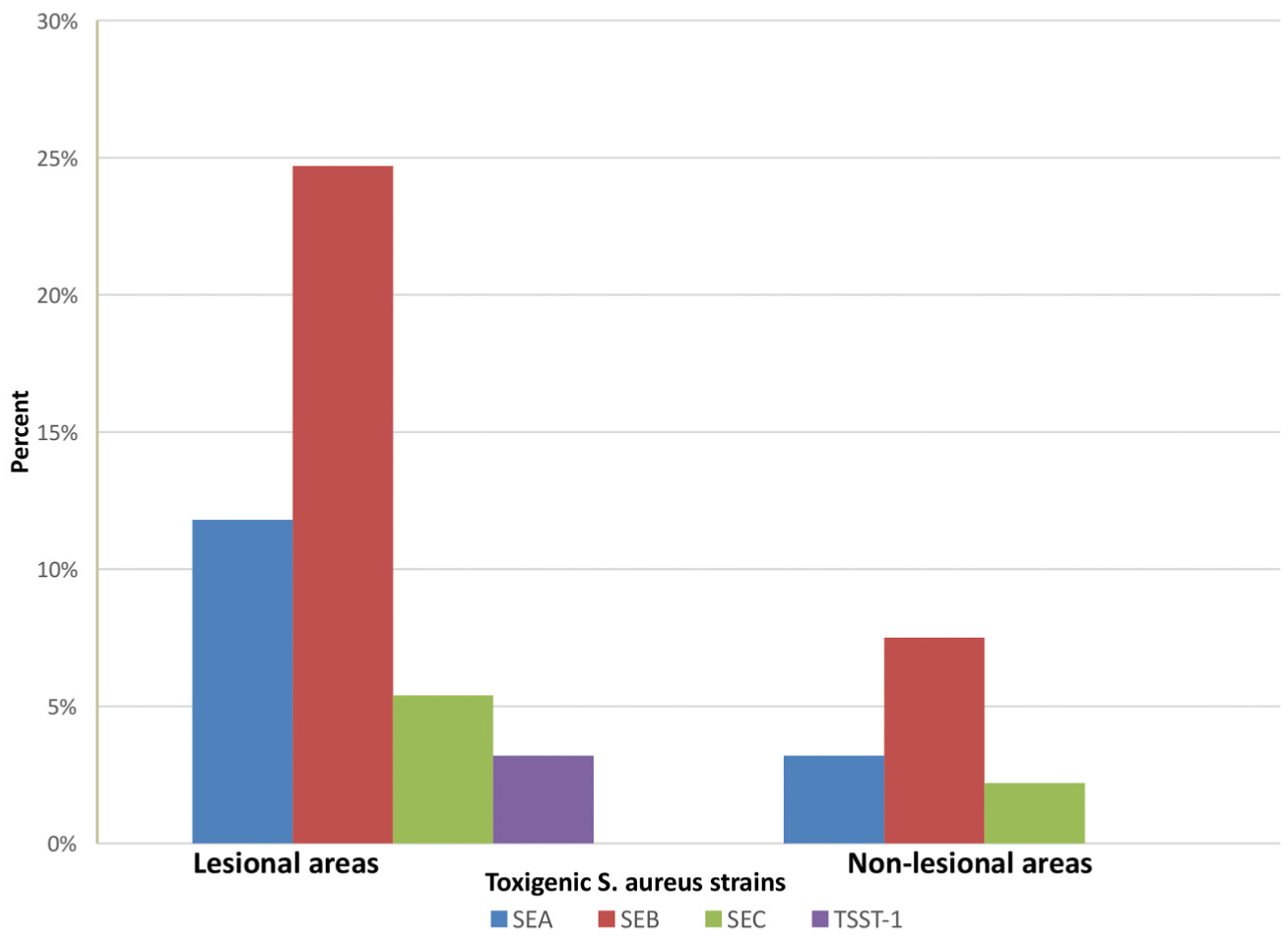
Description of toxigenic S. aureus strains among lesional and nonlesional areas.
Relationship between S. aureus colonization in lesional skin and clinical data
Highly significant differences existed among patients with negative, nontoxigenic, and toxigenic strains colonization in lesional skin regarding psoriasis severity and pruritus intensity. Patients colonized with toxigenic strains exhibited a higher proportion of severe psoriasis and pruritus compared to both noncolonized and nontoxigenic colonized cases (p = 0.001 each; Chi-square test and Fisher’s exact test).
However, no significant difference was observed between these groups regarding the clinical variant of psoriasis (p = 0.08; Fisher’s exact test; Table 2).
Relationship between S. aureus colonization in lesional skin and clinical data of the patients.
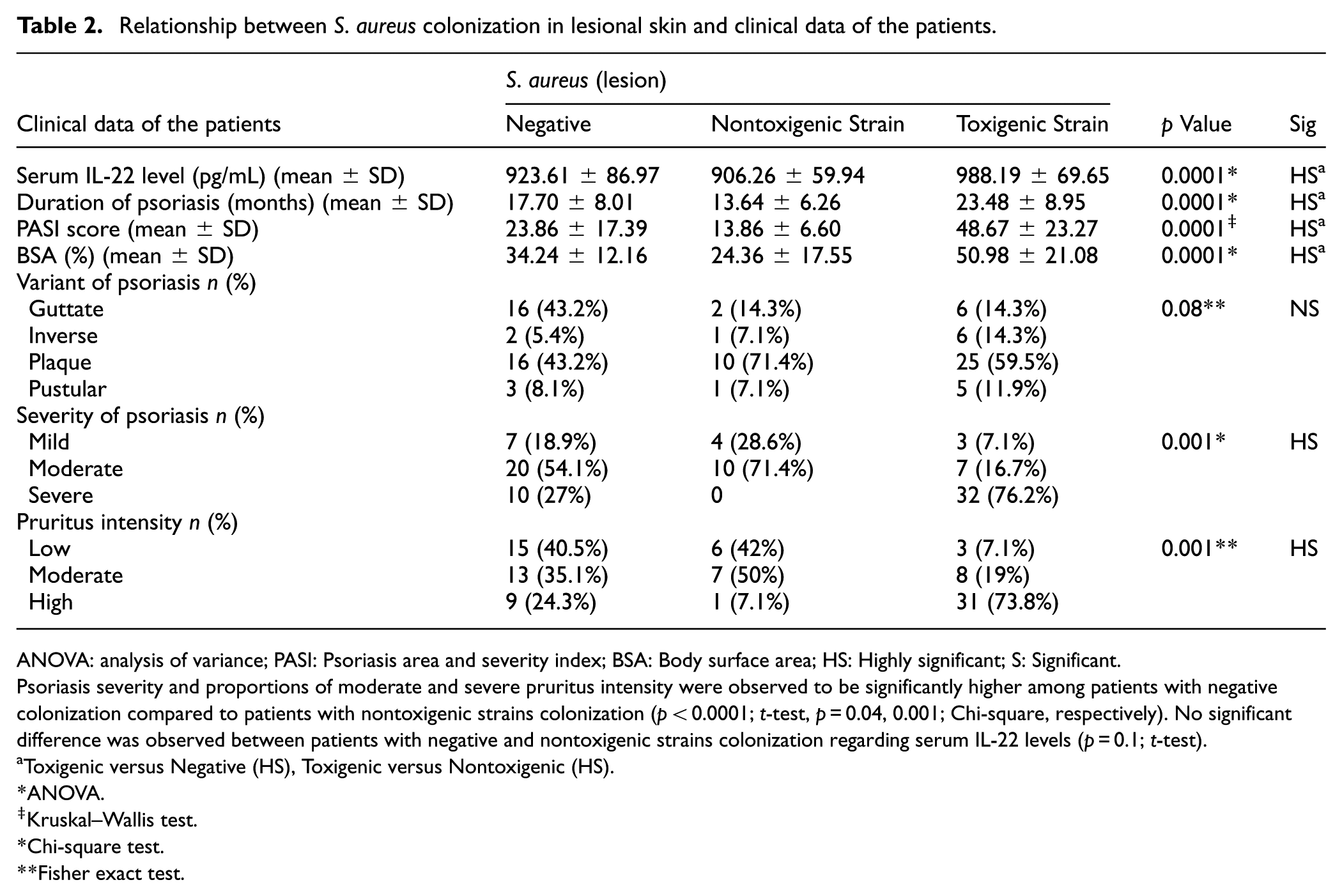
ANOVA: analysis of variance; PASI: Psoriasis area and severity index; BSA: Body surface area; HS: Highly significant; S: Significant.
Psoriasis severity and proportions of moderate and severe pruritus intensity were observed to be significantly higher among patients with negative colonization compared to patients with nontoxigenic strains colonization (p < 0.0001; t-test, p = 0.04, 0.001; Chi-square, respectively). No significant difference was observed between patients with negative and nontoxigenic strains colonization regarding serum IL-22 levels (p = 0.1; t-test).
Toxigenic versus Negative (HS), Toxigenic versus Nontoxigenic (HS).
ANOVA.
Kruskal–Wallis test.
Chi-square test.
Fisher exact test.
In addition, psoriasis severity and proportions of moderate and severe pruritus intensity were observed to be significantly higher among patients with negative colonization compared to patients with nontoxigenic strains colonization in lesional skin (p < 0.0001; t-test, p = 0.04, 0.001; Chi-square, respectively).
Highly significant differences existed among patients with negative, nontoxigenic, and toxigenic strains colonization in lesional skin regarding serum IL-22 levels. Patients colonized with toxigenic strains exhibited higher serum IL-22 levels compared to both noncolonized and nontoxigenic colonized cases (p = 0.0001; ANOVA).
However, no significant difference was observed between patients with negative and nontoxigenic strains colonization in lesional skin regarding serum IL-22 levels (p = 0.1; t-test).
Relationship between S. aureus toxigenic strains in lesional skin and clinical data
A significant difference was observed among patients colonized by SEA, SEB, SEC, and TSST-1 strains in lesional skin regarding serum IL-22 levels, PASI score, and BSA (p = 0.01, 0.002, and 0.001, respectively; ANOVA and Kruskal–Wallis test).
However, no significant differences were found between these groups regarding disease duration and clinical variant of psoriasis (p = 0.05 and 0.35, respectively; Fisher’s exact test; Table 3).
Relationship between S. aureus toxigenic strains in lesional skin and clinical data of the patients.
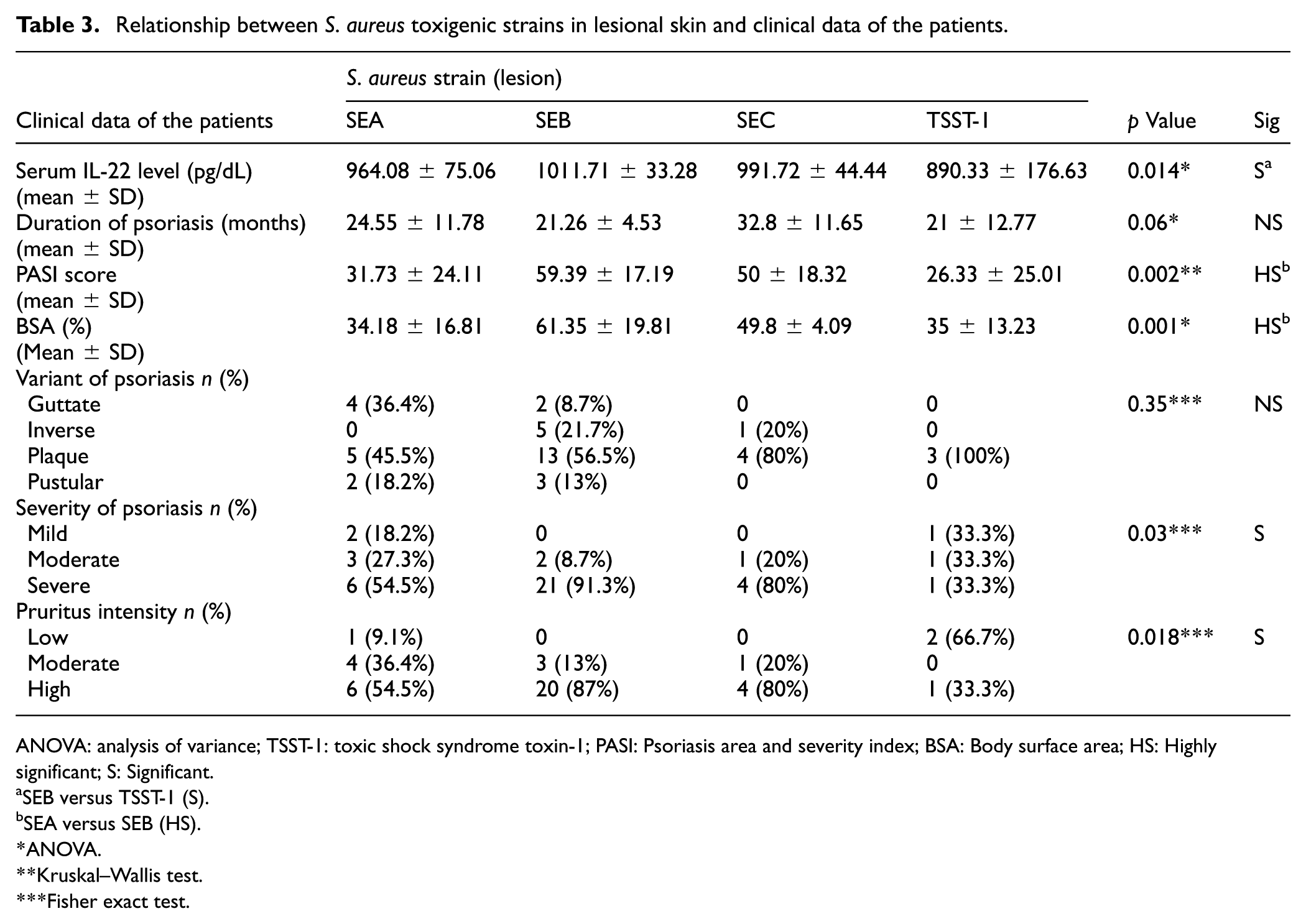
ANOVA: analysis of variance; TSST-1: toxic shock syndrome toxin-1; PASI: Psoriasis area and severity index; BSA: Body surface area; HS: Highly significant; S: Significant.
SEB versus TSST-1 (S).
SEA versus SEB (HS).
ANOVA.
Kruskal–Wallis test.
Fisher exact test.
Relationship between serum IL-22 level and clinical characteristics
Highly significant differences were observed in serum IL-22 levels among patients with varying psoriasis severity and pruritus intensity. Post hoc pairwise comparisons revealed statistically significantly higher mean IL-22 levels among patients with severe psoriasis compared with those with mild or moderate disease, and among patients with severe pruritus compared with those with mild or moderate pruritus (p = 0.001 each; ANOVA). However, no significant difference was found in serum IL-22 levels among patients with different clinical variants of psoriasis (p = 0.59; ANOVA; Table 4).
Relationship between serum IL-22 levels and clinical characteristics.
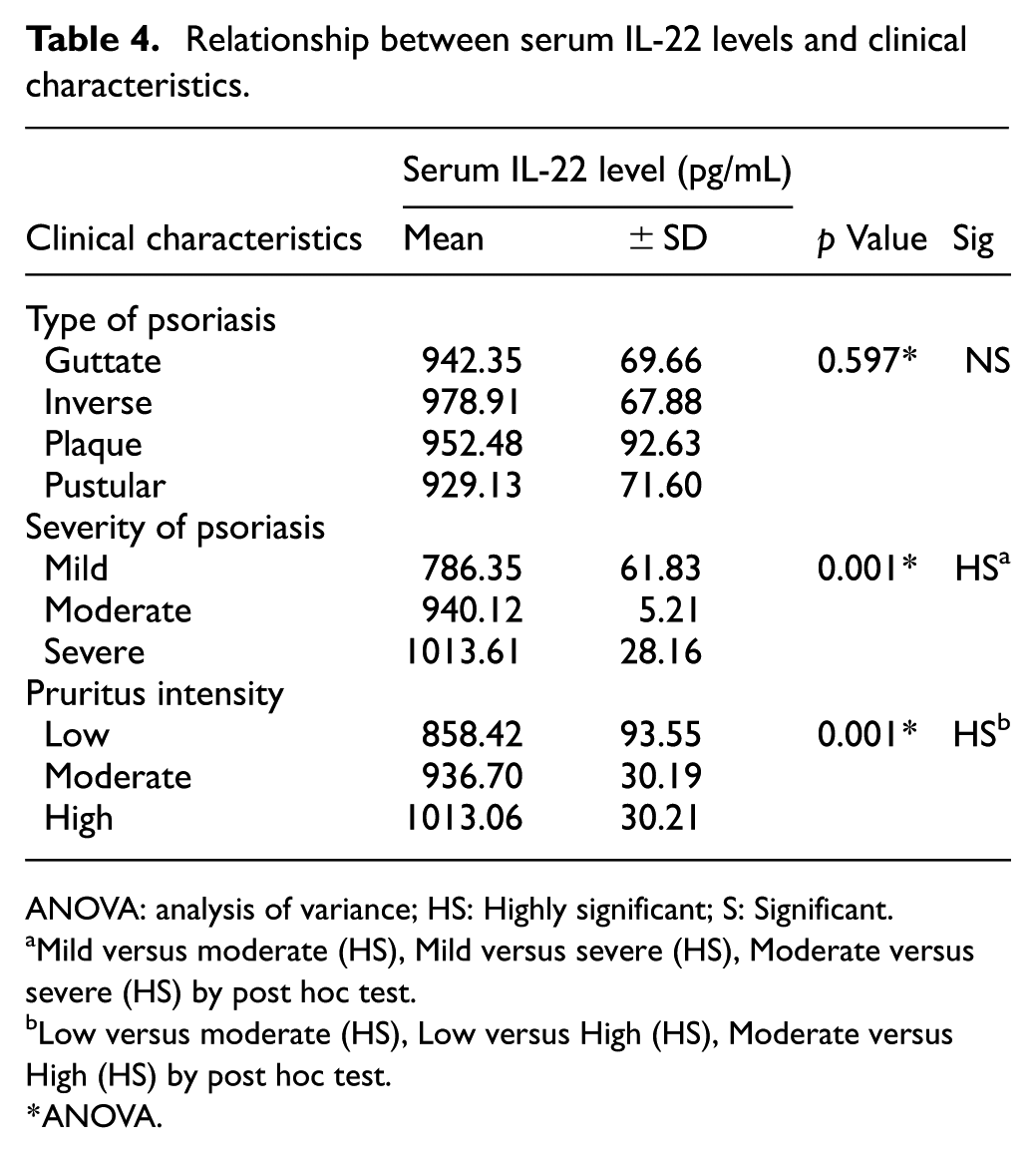
ANOVA: analysis of variance; HS: Highly significant; S: Significant.
Mild versus moderate (HS), Mild versus severe (HS), Moderate versus severe (HS) by post hoc test.
Low versus moderate (HS), Low versus High (HS), Moderate versus High (HS) by post hoc test.
ANOVA.
Correlations of serum IL-22 levels with clinical data
Strong positive and highly significant correlations were observed between serum IL-22 levels and BMI, PASI score, psoriasis severity, and pruritus intensity (p = 0.002, 0.0001, 0.0001, and 0.0001, respectively; Pearson’s and Spearman’s correlation coefficients). However, no significant correlations were found between serum IL-22 levels and either age or duration of psoriasis (p = 0.08 each; Pearson correlation coefficient; Table 5).
Correlations of serum IL-22 levels with each of clinical data of the patients.
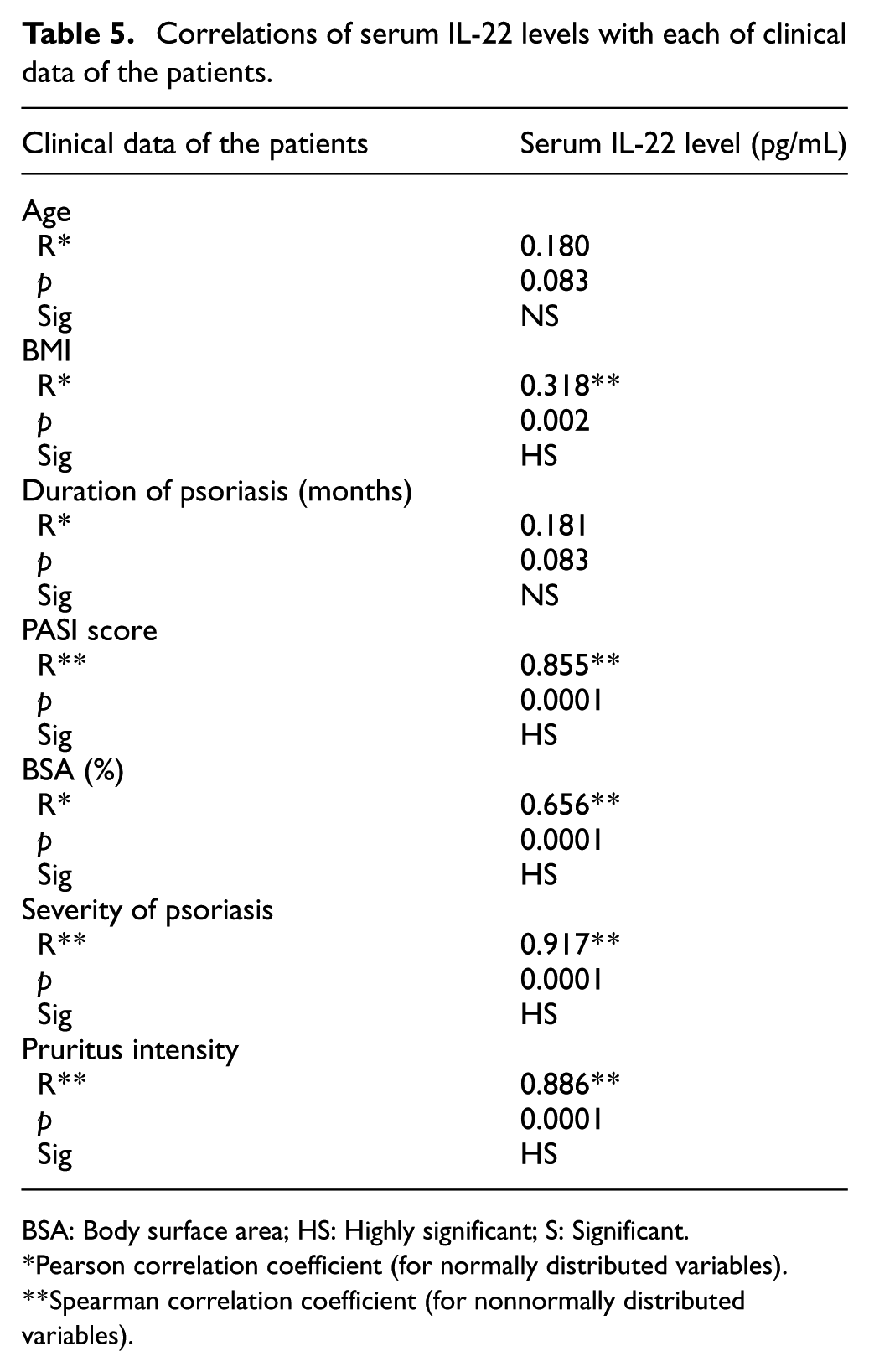
BSA: Body surface area; HS: Highly significant; S: Significant.
Pearson correlation coefficient (for normally distributed variables).
Spearman correlation coefficient (for nonnormally distributed variables).
Discussion
In this cross-sectional, within-patient comparative study, we enrolled 93 adult Egyptian patients with psoriasis to evaluate the prevalence of S. aureus skin colonization in patients with psoriasis and its correlation with serum IL-22 levels, disease severity, and BMI. In addition, we aimed to detect the presence of superantigen genes in S. aureus colonizing the skin.
According to our findings, the majority of patients (60.2%) demonstrated S. aureus colonization in both lesional and nonlesional skin. In lesional skin, 45.2% of patients were colonized by toxigenic strains, whereas in nonlesional skin, 47.3% were colonized by nontoxigenic strains.
These findings may be explained by the heterogeneity and instability of the microbiome of both lesional and nonlesional psoriatic skin compared with healthy skin. 28 Dysbiosis disrupts skin homeostasis and increases susceptibility to cutaneous invasion by infectious pathogens. 29 Such pathogens, including S. aureus, are implicated in the initiation and persistence of psoriatic lesions in genetically predisposed individuals 30 through Th17 polarization and proinflammatory effects.31,32
Evidence regarding S. aureus colonization in lesional and nonlesional skin in psoriasis remains inconsistent. Several studies support our findings, confirming colonization of both lesional and nonlesional skin.12,28,33–35 However, Fahlén et al. 36 reported contrasting results, observing significantly lower staphylococcal colonization in psoriatic skin compared to healthy skin.
The current study demonstrated a significantly higher prevalence of toxigenic strains in lesional skin compared with nonlesional skin (p = 0.001), with SEB being the most prevalent strain (24.7%). Conversely, nontoxigenic strains were significantly more prevalent in nonlesional skin (p = 0.001). These findings may be attributed to the exaggerated cellular immune response induced by staphylococcal enterotoxins, which act as superantigens.15–17 Enterotoxins can activate the STAT3 pathway, 37 leading to the activation and proliferation of γδ T-cells and subsequent production of IL-17 and IL-22 cytokines in psoriatic skin. 38
Consistent with our current findings, Fouad et al. 39 also reported a higher prevalence of the SEB strain in psoriatic skin compared to healthy controls. In contrast, both El Ferezli et al. 40 and Jassim et al. 21 found a higher prevalence of the SEA strain, while Atefi et al. 14 reported a predominance of the TSST-1 strain in psoriatic skin relative to healthy controls.
These discrepancies may be attributed to variations in methodological approaches, including differences in laboratory techniques, sampling methods (swab, punch biopsy, or adhesive tape), and control of cofounding factors. Culture-based sampling methods typically yield lower detection rates than PCR methods. Moreover, microbial colonization is influenced by temperature, urban or rural environments, geographical location, hygienic practices, anatomical sampling site, and individual variations.41,42
Our study also revealed a highly significant difference in BMI among patients with negative, nontoxigenic, and toxigenic strains colonization in lesional skin, with significantly higher mean BMI observed among patients colonized by toxigenic strains compared to noncolonized patients (p = 0.009). This finding suggests a direct association between BMI and staphylococcal colonization. The relationship may be explained by the influence of proinflammatory cytokines, including leptin, IL-6, and tumor necrosis factor α, produced by adipose tissue. These cytokines promote a subclinical inflammatory state and cytokine imbalance, impairing immune functions and enhancing bacterial colonization in patients with obesity.43,44 These findings are supported by previous studies reporting a higher risk of nasopharyngeal S. aureus colonization among individuals with obesity.45–48
The present study demonstrated a significant direct correlation between S. aureus lesional colonization and psoriasis severity, irrespective of its clinical variant. This result was indicated by highly significant differences among patients with negative, nontoxigenic, and toxigenic strain colonization in lesional skin regarding disease duration, PASI scores, and BSA%, with significantly higher mean values for all variables among patients colonized by toxigenic strains compared with both noncolonized and nontoxigenic colonized patients (p = 0.0001 for each). Furthermore, highly significant differences were observed among these groups regarding psoriasis severity and pruritus intensity, with a higher proportion of severe cases and cases exhibiting intense pruritus among patients colonized by toxigenic strains (particularly, SEB) compared with noncolonized or nontoxigenic colonized cases. However, no significant differences were found among these groups concerning the clinical variant of psoriasis (p = 0.08), suggesting that lesional S. aureus colonization is related to disease activity rather than clinical variant, consistent with the findings of Fouad et al. 39
Similarly, significant differences were observed among patients colonized by SEA, SEB, SEC, and TSST-1 in lesional skin regarding psoriasis severity and pruritus intensity, with a higher proportion of severe and highly pruritic cases among those colonized by SEB strains compared with other strains.
These findings may be attributed to the exaggerated immune and inflammatory responses within psoriatic lesions induced by S. aureus and its toxins.15–17,30–32,37,38 These results align with those of Tomi et al., 13 Göçmen et al., 49 and Fouad et al., 39 who also reported significant correlations between the presence of S. aureus isolates or their toxins and PASI scores.
The higher colonization rate of toxigenic strains, particularly the SEB strain, among patients with severe pruritus may be explained by the presence of the S. aureus-expressed V8 protease, which activates sensory neurons in the skin through protease-activated receptor 1 signaling, thereby inducing pruritus. This mechanism was demonstrated by Deng et al. 50 in patients with atopic dermatitis. Further studies are warranted to explore how microbial agents residing on the skin influence cutaneous sensory responses 51 across various dermatological conditions, including psoriasis.
This study revealed a significantly higher mean age among patients colonized by toxigenic strains compared with noncolonized patients (p = 0.007), indicating that S. aureus toxigenic strain colonization markedly increased with patient age. This finding could be attributed to variations in hygienic conditions, geographical factors, and occupational exposures that tend to change with age, as supported by Park et al., 52 who reported that S. aureus colonization rates in acute lesions of atopic dermatitis increased with age. Further studies are required to validate this finding in patients with psoriasis.
According to this study, psoriasis severity and proportions of moderate and severe pruritus intensity were observed to be significantly higher among patients with negative colonization compared to patients with nontoxigenic strains colonization in lesional skin (p < 0.0001, p = 0.04, 0.001, respectively).
In addition, serum IL-22 levels were higher in patients with negative colonization compared to patients with nontoxigenic strains colonization with an insignificant difference between these groups (p = 0.1).
These findings could be explained according to Fouad et al., 39 who reported that nontoxigenic strains are generally considered part of the commensal human flora and do not cause harmful effects under normal conditions. However, there is no evidence suggesting that nontoxigenic S. aureus strains are beneficial for psoriasis, unlike toxigenic strains.
On the other hand, Chen et al., 53 reported much evidence suggesting the association of alterations of skin microbiota with the pathogenesis of psoriasis and disease flares.
These conflicting data could be attributed to lack of standardized sampling and profiling protocols. 53 Therefore, Quan et al., 54 recommended further studies to better characterize the microbiome of psoriatic lesions and to establish standardized protocols of sampling methods.
This study also demonstrated highly significant differences among patients with negative, nontoxigenic, and toxigenic strain colonization in lesional skin regarding serum IL-22 levels. Moreover, significant differences were observed in serum IL-22 among patients colonized by SEA, SEB, SEC, and TSST-1 strains in lesional areas.
These findings can be explained by the immunological role of IL-22 in cutaneous immunity against S. aureus infection, primarily through the stimulation of antimicrobial peptide synthesis 55 and the enhancement of T-cell and neutrophil chemotaxis. 56 Moreover, IL-22 has been implicated in the pathogenesis of psoriasis, where it promotes keratinocyte proliferation, inhibits cellular differentiation, and enhances antimicrobial defense. 7 Experimental studies have further shown that IL-22 contributes to the maintenance of the psoriatic skin inflammation in murine models. 57
The present results are consistent with the findings of Fouad et al., 39 who reported significantly higher IL-22 levels among patients colonized with toxigenic strains. Similarly, Niebuhr et al. 58 and Wawrzycki et al. 59 observed elevated IL-22 levels following SEB stimulation in in vitro studies using T-cells isolated from patients with psoriasis. Overall, these data suggest a potential role of SEB in the induction of IL-22 production.
Furthermore, this study identified a strong positive correlation between serum IL-22 levels and clinical severity of psoriasis, evidenced by highly significant correlations between serum IL-22 levels and PASI scores, psoriasis severity, and pruritus intensity. In addition, highly significant differences were observed in serum IL-22 levels among patients with varying degrees of disease severity and pruritus, underscoring the potential contribution of IL-22 to both inflammatory activity and symptom intensity in psoriasis.
These findings could be explained by increased levels of bioactive IL-22 in psoriatic lesions resulting from the synergistic effect of both reduced levels of IL-22 binding protein, which suppresses IL-22 activity, and elevated levels of IL-22 itself.60–62
Cordoro et al. 63 identified increased lesional expression of IL-22 in children with psoriasis compared with nonlesional skin. Moreover, Guttman-Yassky et al. 64 reported that fezakinumab, an IL-22 monoclonal antibody, reduced pruritus in patients with moderate-to-severe atopic dermatitis. These findings suggest a potential link between IL-22 and pruritus, warranting further studies to verify the effect of IL-22 on itching in psoriasis.
In the present study, serum IL-22 levels showed highly significant positive correlations with BMI, indicating a potential metabolic effect of IL-22. This effect may be mediated through activation of the JAK-STAT3 signaling pathway.18,19 This finding aligns with Harder et al., 65 who reported significant positive correlations between serum IL-22 levels and BMI in a Korean population. Furthermore, Gu et al. 66 found that serum IL-22 levels were significantly elevated in patients with metabolic syndrome compared to healthy controls.
Conversely, these results contradict the findings of Shen et al., 20 who reported a negative correlation between serum IL-22 levels and BMI in a Chinese population. This inconsistency underscores that the relationship between serum IL-22 levels and obesity remains incompletely understood, given the limited and conflicting data available. 66 Some studies, including the present one, support a positive correlation, suggesting a pathogenic role of IL-22,65,66 whereas others, such as Shen et al., 20 suggest a protective role of IL-22 against obesity. Furthermore, IL-22 appears to exert both pathogenic and protective roles in inflammation, depending on the context, including the tissue involved, cytokine milieu, oxygen availability, metabolic state, and presence of other inflammatory mediators. 67
This study has some limitations. First, its cross-sectional design restricts the ability to establish a causal relationship between S. aureus colonization and elevated serum IL-22 levels in patients with psoriasis. Second, the relatively small sample size may limit the generalizability of the findings. Third, the study relied on conventional culture-based techniques for bacterial identification, which may not capture the full spectrum of microbial diversity as effectively as advanced genomic methods. The lack of evaluation of other microbial agents constitutes an additional limitation. Further longitudinal studies involving larger and more diverse populations, as well as the use of advanced microbial identification methods, are required to clarify the causal relationship between S. aureus colonization and serum IL-22 levels in psoriasis.
Conclusion
This study demonstrated significant associations between S. aureus colonization, particularly toxigenic strains producing SEB and disease severity, serum IL-22 levels, and BMI in patients with psoriasis. The findings also highlight potential therapeutic innovations targeting both S. aureus and IL-22 for the management of severe psoriasis. However, further studies with larger sample sizes are warranted to validate these findings.
Footnotes
Acknowledgements
The authors would like to acknowledge Taylor & Francis Editing Services for their assistance in editing this manuscript.
Author note
The institution where the research was conducted: Armed Forces College of Medicine (AFCM), Cairo, Egypt.
Ethical considerations
The study proposal was revised and approved by the Armed Forces College of Medicine Ethical Review Committee/Institutional Review Board (IRB No. 345, 25/11/2023). Data confidentiality was strictly maintained throughout the study. Written informed consent was obtained from all participants before enrollment. The study design adhered to the principles outlined in the revised Declaration of Helsinki for biomedical research ethics.
Consent to participate
Written informed consent was obtained from all patients prior to enrollment.
Consent for publication
The authors affirm that human research participants provided informed consent for publication.
Author contributions
All authors contributed equally to the study conception and design. Material preparation, data collection, and analysis were performed by A.I. D., M. A. K., R. A. and F.Y. F. The first draft of the manuscript was written by R. A. and F.Y. F. and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The corresponding author serves as an Associate Editor of the International Journal of Women’s Dermatology, a member of the Committee on Publication Ethics (COPE)—Diversity, Equity, and Inclusion Subcommittee, and a COPE Advisor. The author is also a member of the European Association of Science Editors (EASE). All other authors declare no conflict of interest.
Data availability statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.