
Abstract
Coronary artery calcium scoring (CCS) is a valuable non-invasive method for assessing atherosclerosis and performing risk stratification in patients with suspected coronary artery disease (CAD). Monocyte subsets play distinct roles in chronic inflammation and cardiovascular disease, potentially serving as biomarkers for CCS risk assessment. The aim of this study was to analyze the distribution of monocyte subsets in patients with suspected CAD and determine the association of monocyte subsets with CCS.
A cohort of 182 individuals with suspected CAD was enrolled. Participants were stratified into three groups based on their CCS scores: very low-risk (CCS = 0), low-risk (CCS = 1−99), and moderate–high risk (CCS ≥ 100). Monocyte subsets were categorized according to CD14 and CD16 expression levels into classical, intermediate (intMo), and non-classical monocytes. Absolute counts and frequency distribution of monocyte subsets (FDMS, percentage of CD45+/CD14+/CD16+ events) were analyzed across all participants.
Patients in the moderate–high risk CCS group had significantly higher absolute circulating monocyte counts than those in the other two groups (p < 0.05). Furthermore, the moderate–high risk CCS group had the highest absolute intMo count and FDMS (percentage of CD45+/CD14+/CD16+ events, p < 0.05). Both the absolute intMo count (Model 1: odds ratio [OR] = 1.024, 95% confidence interval [CI]: 1.009−1.040, p = 0.002) and FDMS (percentage of CD45+/CD14+/CD16+ events, Model 2: OR = 1.109, 95% CI = 1.039−1.183, p = 0.002) were identified as independent risk factors for moderate–high risk CCS.
These data suggest that intMo may be a useful biomarker for CCS risk stratification.
Keywords
Introduction
Coronary artery calcification (CAC) is a well-established marker of coronary atherosclerosis in patients with coronary artery disease (CAD). CAC prevalence increases with age and is more commonly observed in elderly individuals with abnormal lipid metabolism, diabetes, and impaired kidney function. CAC also provides additional prognostic information for all-cause mortality beyond traditional risk factors.1,2 Early detection of CAD in asymptomatic individuals is essential to identify optimal treatment windows and mitigate the increased risks associated with advanced stages of this condition. Coronary artery calcium scoring (CCS) is a simple, non-invasive imaging technique performed using electrocardiogram-gated multidetector computed tomography scans to detect and quantify CAC. CCS allows for rapid assessment, which enhances cardiovascular risk prediction in asymptomatic individuals with CAD, making it a valuable tool for atherosclerosis evaluation and risk stratification. The Agatston score is the most commonly used CCS system. 3
Atherosclerosis is a chronic inflammatory condition characterized by inflammatory cell infiltration and foam cell formation, leading to CAD. Blood monocytes have a critical role in initiating and progressing cardiovascular disease (CVD) by releasing inflammatory substances that accelerate coronary stenosis and plaque rupture 4 . Monocyte levels and their phenotypic profile are closely linked to cardiovascular risk in patients with type 2 diabetes mellitus. 5 Furthermore, high monocyte to high-density lipoprotein cholesterol ratio is significantly associated with increased CCS. 6
The current classification of monocytes into three distinct subsets is based on the 2010 International Union of Immunological Societies guidelines. 7 Monocytes are categorized based on expression of the lipopolysaccharide receptor CD14 and the FcγIII receptor CD16 into classical monocyte (cMo: CD14+ CD16−), intermediate monocyte (intMo: CD14+ CD16+), and non-classical monocyte (ncMo: CD14dimCD16+) subsets. 7 These subsets exhibit unique phenotypic and functional traits, resulting in varying roles in inflammation and chronic diseases. The cMo subset is responsible for initiating inflammatory reactions to eliminate necrotic cells, whereas the ncMo subset predominantly mitigates inflammation, facilitating tissue regeneration and recovery. When stimulated by toll-like receptors, intMo simultaneously produces pro-inflammatory and anti-inflammatory cytokines. 8
Different monocyte subsets may have varying impacts on myocardial injury, disease severity, and prognosis in CAD patients. Recent studies have shown that changes in monocyte subsets and distribution correlate with disease severity and prognosis,9–11 but not with the type of myocardial ischemia in CAD patients. 12 However, there is still a lack of comprehensive research investigating the distribution of monocyte subsets in CAC and their potential value as biomarkers for the presence of coronary atherosclerosis as determined by CCS in patients with suspected CAD. Therefore, we conducted a prospective, dual-center study to analyze the distribution of monocyte subsets in CAC and their correlation with CCS.
Methods
Study design and patient population
A total of 182 patients with suspected CAD were recruited for this prospective, dual-center study at Hospital A and Hospital B between April 2023 and October 2023. “Suspected CAD” was defined as presenting clinical symptoms suggestive of CAD (e.g., chest pain, dyspnea, abnormal stress tests, or electrocardiogram findings indicative of ischemia) prompting the need for coronary computed tomography angiography (CTA) for further evaluation. The inclusion criteria were: (1) individuals aged 18 years and older, (2) with suspected CAD as defined above, and (3) indication for coronary CTA as part of diagnostic evaluation. The exclusion criteria were: (1) pre-existing CAD defined as a documented history of CAD, including prior myocardial infarction, coronary revascularization (stenting or bypass surgery), or documented coronary artery stenosis; (2) acute infections: patients with any active infections, such as respiratory or systemic infections, at the time of recruitment; (3) malignant tumors or autoimmune diseases: individuals undergoing treatment for cancers or autoimmune disorders that could impact immune or inflammatory markers; (4) severe hepatic or renal dysfunction, including liver function tests more than three times the upper normal limit or an estimated glomerular filtration rate of less than 30 mL/min/1.73 m2; (5) recent trauma or surgery: patients who underwent major surgery or experienced trauma within the past two weeks; (6) poor imaging quality: participants were excluded if the coronary CTA images were of insufficient quality to assess CAC (e.g., due to motion artifacts or technical issues). The study was approved by the ethics committees of both hospitals (Approval No. 25024058X, 2023-011KY) and all eligible participants provided signed informed consent. All procedures performed in this study were in accordance with the Declaration of Helsinki 1975 (as revised in 2000).
Clinical data, including diagnoses, personal history, laboratory testing, and echocardiography examination, were extracted and recorded in a database. Hypertension was diagnosed based on criteria including a blood pressure reading exceeding 140/90 mmHg, prescription of antihypertensive medication, or a medical diagnosis of hypertension. Similarly, diabetes mellitus was established if fasting blood glucose levels were >126 mg/dL, antidiabetic drugs had been administered, or a medical diagnosis of diabetes mellitus had been made. Dyslipidemia was defined as meeting the criteria for elevated levels of total cholesterol (>200 mg/dL), triglycerides (>150 mg/dL), and low-density lipoprotein cholesterol (>130 mg/dL) or was diagnosed in patients currently receiving lipid-lowering medication.
This study was approved by the Ethics Committee of Beijing Anzhen Hospital (Approval No.: 2023-011KY), all patients signed written informed consent forms, and the study process complies with the principles of the Declaration of Helsinki.
Monocyte analysis
Sample collection
Peripheral venous blood samples were collected within 24 hours after the patient completes coronary CT examination and before initiating new lipid-lowering/antihypertensive treatment. The sample processing procedure is as follows: 5 mL of peripheral venous blood is collected into ethylenediaminetetraacetic acid (EDTA) anticoagulant tubes, centrifuged within 30 min of standing at room temperature (rotational speed: 1500 rpm, time: 5 min) to separate peripheral blood mononuclear cells, which are then stored in a −80°C ultra-low temperature refrigerator for subsequent flow cytometry detection.
Flow cytometry
Cells were stained with antibodies including CD45 (PE-cy7, Hangzhou CellGene Biotechnology Co., Ltd, Hangzhou, China), CD16 (FITC, Agilent Technologies, Inc., Palo Alto, CA, USA), and CD14 (APC, Agilent Technologies, Inc., Palo Alto, CA, USA). Erythrocytes were lysed using hemolysin (Agilent Technologies, Inc., Palo Alto, CA, USA). Absolute cell counts were conducted using BD TruCount tubes (BD Biosciences, San Jose, USA). Flow cytometry analyses were performed using BD FACSCanto flow cytometers (BD Biosciences, San Jose, USA).
First, 100 µL of whole blood and 20 µL each of CD45, CD16, and CD14 antibodies were added to an absolute counting tube, mixed, and incubated for 15 min at room temperature. Next, 2 mL of hemolysin was added and the tubes were allowed to dry for 10 min, then were centrifuged at 1500g for 5 min to remove cell debris, and washed with 2 mL of phosphate buffered saline (PBS). The samples were then centrifuged at 1500g for 5 min, supernatants were discarded, and cells were resuspended in 500 µL of PBS. Data were recorded using BD FACSDiva software (BD Biosciences, Becton, Dickinson and Company, San Jose, CA, USA, version 8.0.1) and analyzed using FlowJo software (FlowJo, LLC, a subsidiary of BD Biosciences, Ashland, OR, USA, version 10.7.1). Initially, non-hematopoietic cells are excluded by CD45-negative labeling, and red blood cells, platelets, and cell debris are excluded based on side scatter and forward scatter characteristics to ensure that only myeloid-derived mononuclear cells are analyzed. Then, a scatter diagram was generated with CD45-PE/Cy7 as the ordinate and side scatter as the abscissa to identify the monocyte cell population. Finally, dual-color fluorescence staining was carried out within the monocyte gate. The scatter plot represented CD14-APC on the y-axis and CD16-FITC on the x-axis. Monocyte subsets were classified according to the CD14 and CD16 levels as CD14+CD16- cMo, CD14+CD16+ intMo, and CD14 dimCD16+ ncMo. The absolute counts for each subset and FDMS (percentage of CD45+/CD14+/CD16+ events) were then calculated (Figure 1).
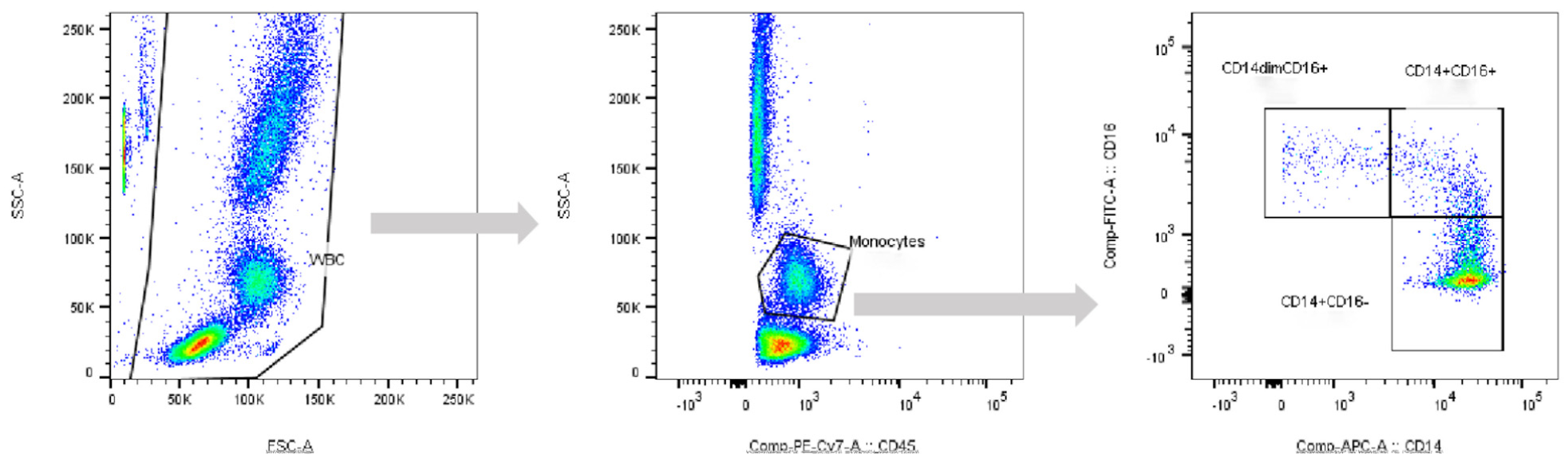
A summary of the cytofluorimetric gating sequence and the markers association (CD45/CD14/CD16) used for the identification and quantification of monocyte subsets.
Coronary artery calcium scoring
CCS was assessed using electrocardiogram-gated multidetector CT scans, with optimal data quality obtained during mid-diastole when cardiac activity was least active. The Agatston algorithm employed a threshold of CT density of >130 Hounsfield units and a minimum of three contiguous imaging pixels >1 mm2 to identify calcific lesions. 3 A weighting factor ranging from 1 to 4 was assigned based on CT density, with the lesion area multiplied by this factor to calculate the CCS value. Total CCS was calculated by aggregating calcified lesions across the left main, left anterior descending, left circumflex, and right coronary arteries, with consideration for racial and ethnic factors.13,14 Each case was evaluated by two skilled readers who were blinded to the clinical and demographic characteristics of the patients. The CAC risk categories were as follows: 0 indicating very low risk, 1–99 indicating low risk, 100–299 indicating moderate risk, and ≥ 300 indicating high risk (Table 1). In this study, patients were categorized into three distinct groups based on their CCS scores: very low-risk (CCS = 0), low-risk (CCS = 1–99), and moderate–high risk (CCS ≥ 100).
CCS ranges, risk classification, and patient distribution.
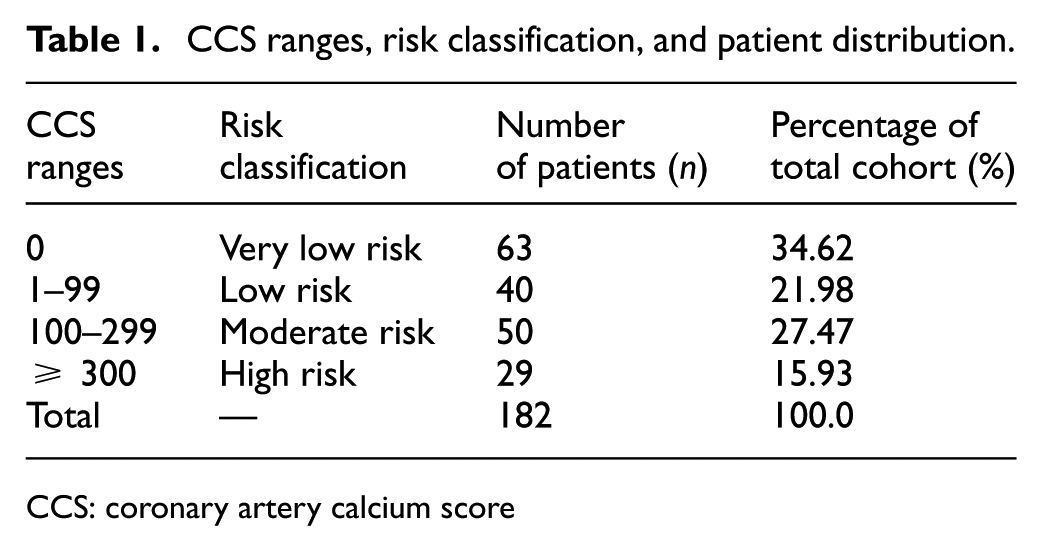
CCS: coronary artery calcium score
Statistical analysis
Data were analyzed utilizing SPSS software (SPSS 22.0, SPSS Inc., Chicago, IL, USA). Descriptive statistics were used to summarize normally distributed continuous variables as mean ± standard deviation and non-normally distributed continuous variables as median (interquartile range). Frequencies and ratios were used to summarize categorical variables. ANOVA was performed to assess differences between groups for normally distributed data, while the Kruskal–Wallis test was used for non-normally distributed data. We conducted multivariable logistic regression analysis to determine independent predictive factors for moderate–high CCS risk. This analysis included variables that exhibited significant associations with CCS in univariate analysis, as well as variables of clinical significance. To enhance the rigor of statistical reporting, we used false discovery rate—adjusted p-values (calculated via the Benjamini–Hochberg method) for all inter-group comparison and regression analysis results. Forest plots were created using GraphPad Prism (version 10, GraphPad Software, Inc., CA, USA). The prediction of moderate–high CCS risk was assessed using receiver operating characteristic (ROC) analysis. Statistical significance was defined as a p-value of <0.05 in two-sided testing.
Results
Baseline demographic data
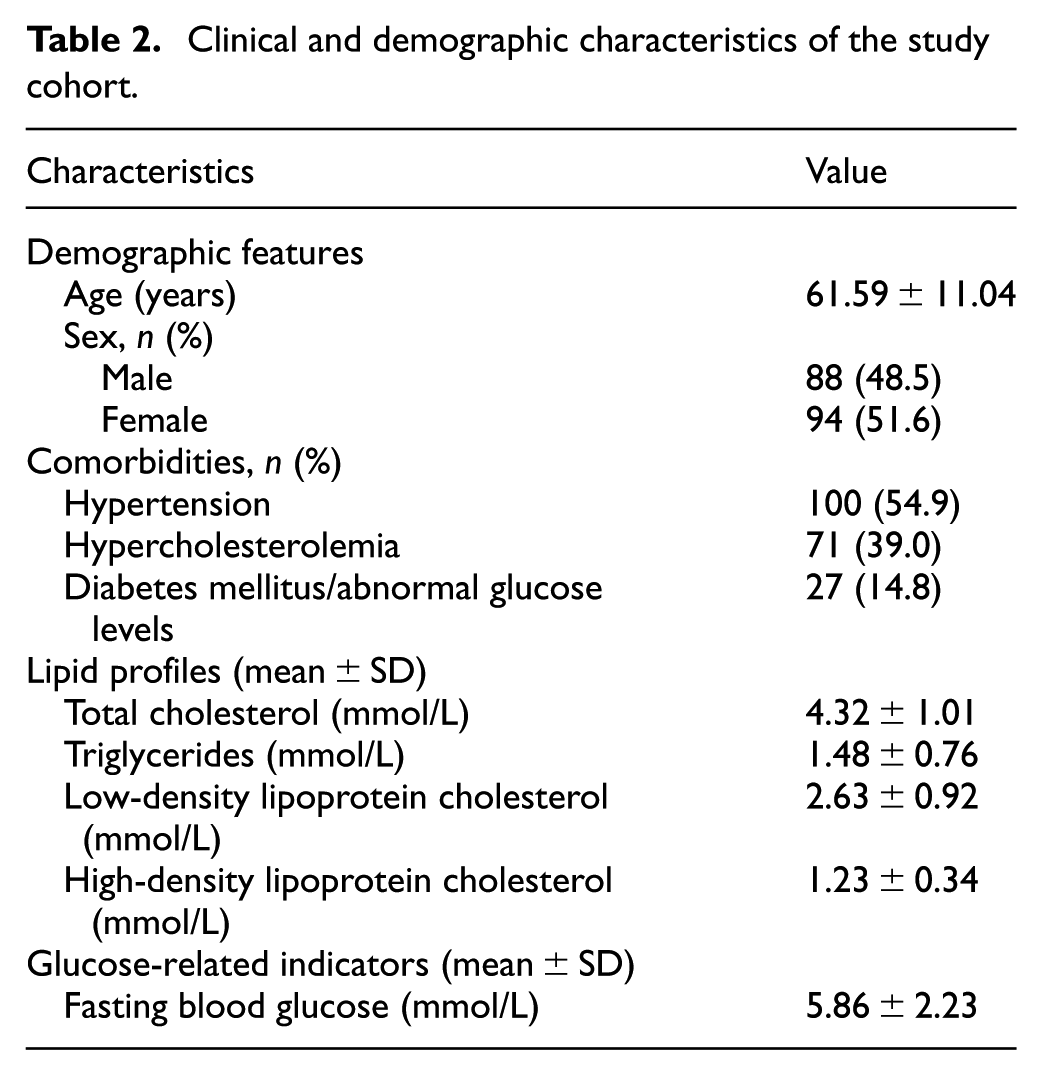
A total of 182 patients meeting the inclusion criteria were enrolled in this study, including 88 males (48.4%). The specific clinical demographics of these 182 patients are summarized in Table 2. Among these patients, 63 cases were classified as very low-risk, 40 as low-risk, and 79 as moderate–high risk CCS. Baseline patient characteristics, clinical data, and laboratory results are detailed in Table 3 according to CCS classification. The moderate–high risk CCS group had a significantly higher proportion of males, as well as elevated rates of smoking, alcohol consumption, hypertension, and lipid abnormalities, compared with the other groups. Serum levels of fasting glucose, triglycerides, and creatinine were also elevated, while creatinine clearance was reduced in the moderate–high risk CCS group.
Clinical and demographic characteristics of the study cohort.
Baseline clinical and laboratory characteristics according to CCS.
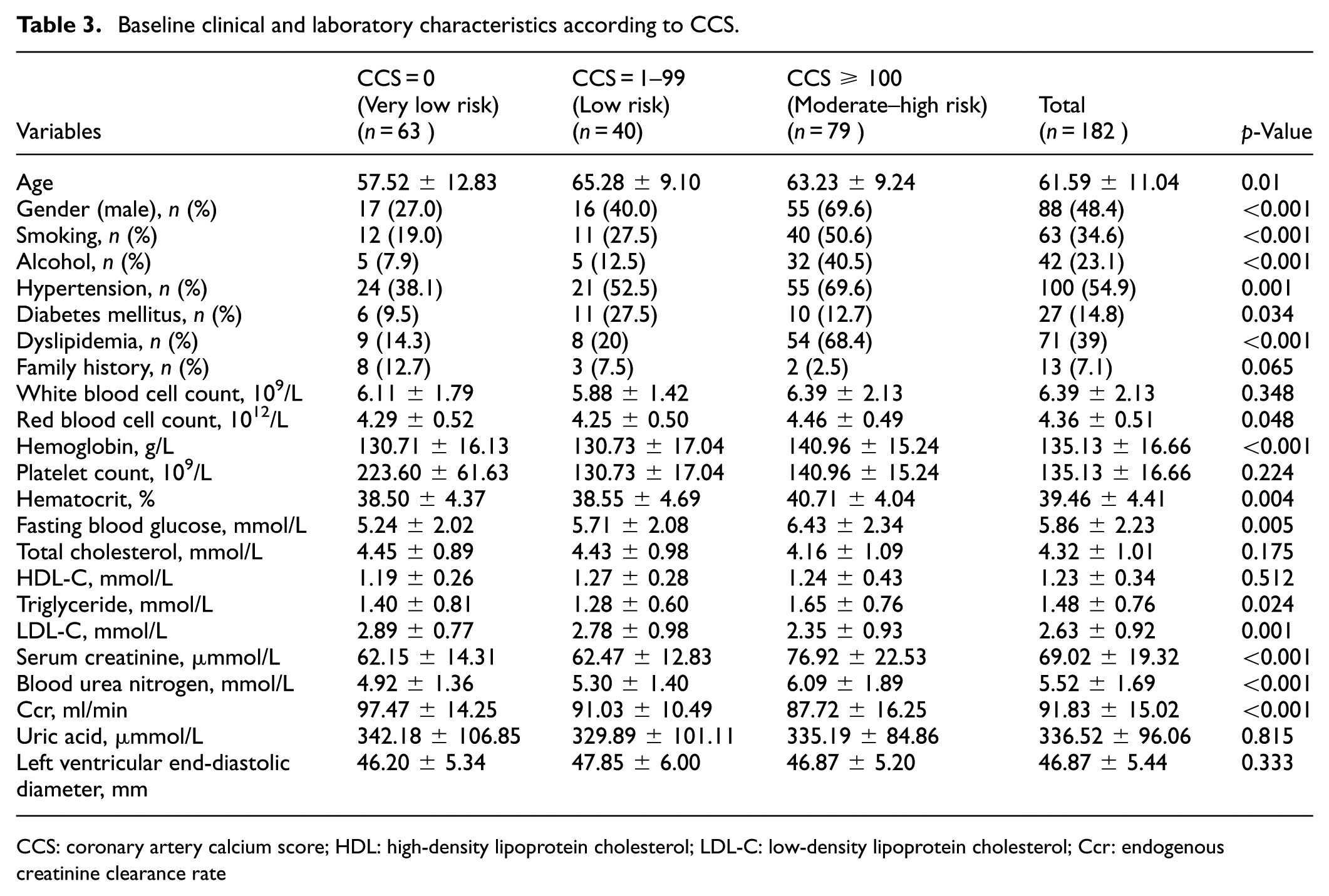
CCS: coronary artery calcium score; HDL: high-density lipoprotein cholesterol; LDL-C: low-density lipoprotein cholesterol; Ccr: endogenous creatinine clearance rate
Circulating monocyte subset levels in different CCS groups
Circulating monocyte subset levels differed by CCS risk stratification (Figure 2, Table 4). No statistically significant differences were found in all indicators between the very low-risk and low-risk groups (all pairwise p > 0.05) after the Bonferroni correction. The moderate–high risk CCS group had the highest levels of total monocyte absolute count, intMo FDMS (percentage of CD45+/CD14+/CD16+ events) and absolute count, and ncMo absolute count, all of which were significantly higher than those in the very low-risk group (all pairwise p < 0.05); this group also had the lowest cMo FDMS (percentage of CD45+/CD14+/CD16+ events), which was significantly different from the low-risk group (pairwise p = 0.04). In contrast, the absolute counts and FDMS (percentage of CD45+/CD14+/CD16+ events) of cMo and ncMo (except ncMo absolute count) showed no significant overall intergroup differences or meaningful pairwise comparisons.
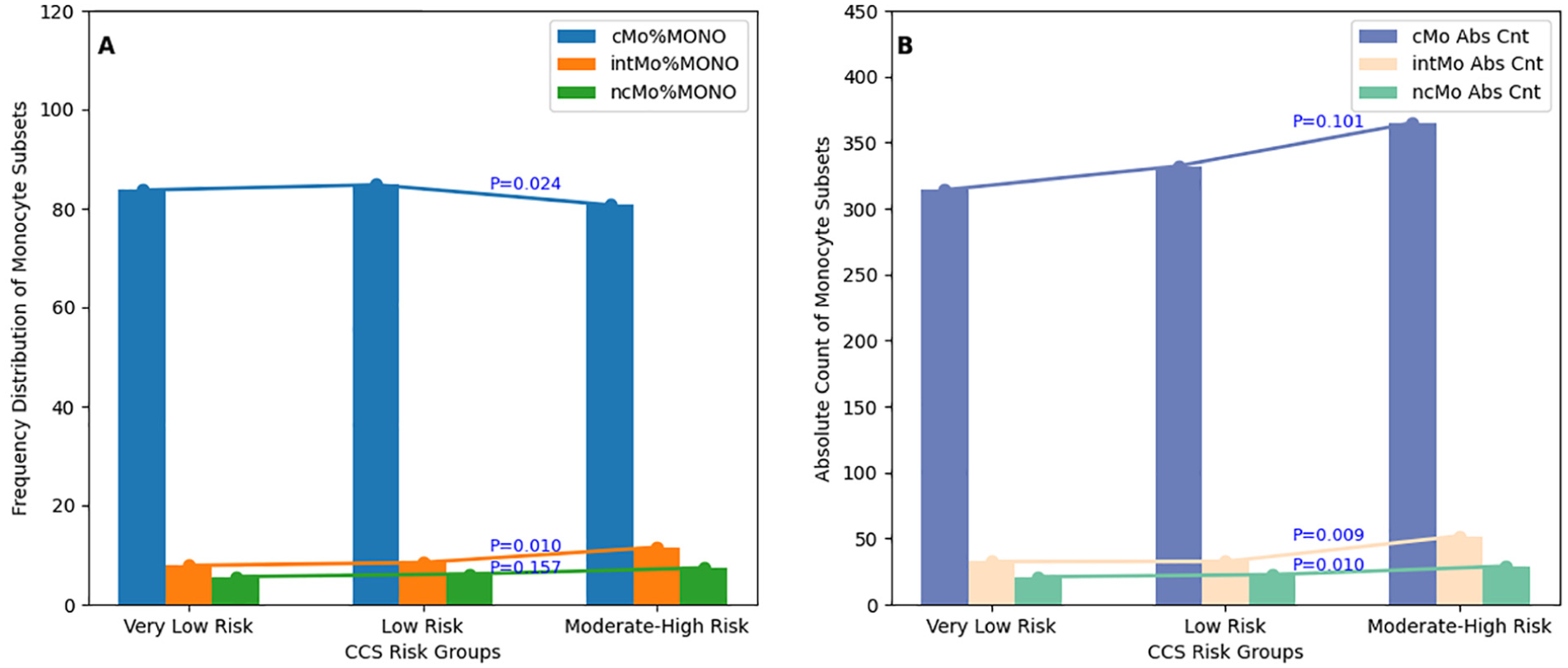
A summary of the distribution of monocyte subsets across different CCS risk groups. A. Comparison of monocyte subsets FDMS (percentage of CD45+/CD14+/CD16+ events) by CCS risk groups. B. Comparison of monocyte subsets absolute count by CCS risk groups.
Circulating monocyte subsets according to CCS.
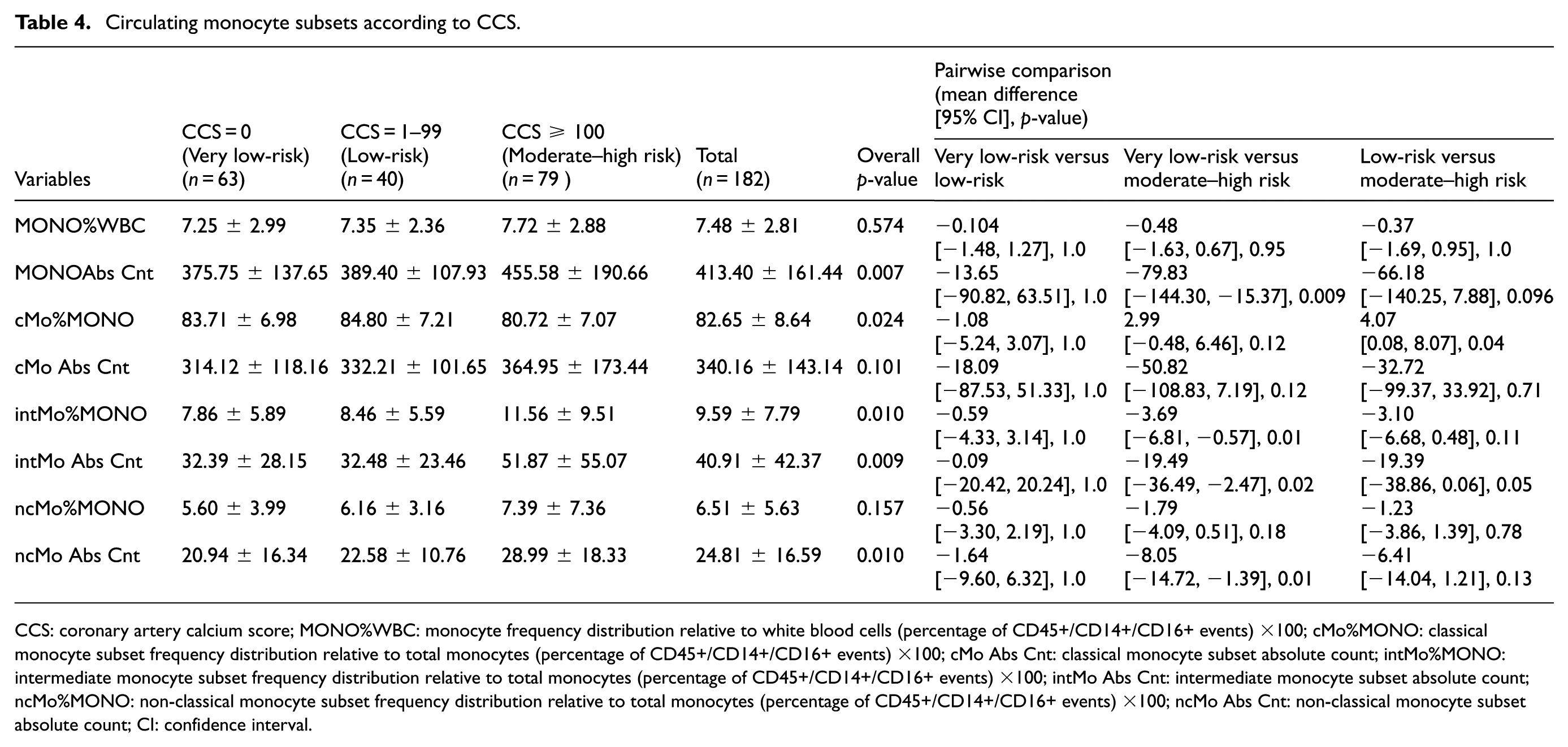
CCS: coronary artery calcium score; MONO%WBC: monocyte frequency distribution relative to white blood cells (percentage of CD45+/CD14+/CD16+ events) ×100; cMo%MONO: classical monocyte subset frequency distribution relative to total monocytes (percentage of CD45+/CD14+/CD16+ events) ×100; cMo Abs Cnt: classical monocyte subset absolute count; intMo%MONO: intermediate monocyte subset frequency distribution relative to total monocytes (percentage of CD45+/CD14+/CD16+ events) ×100; intMo Abs Cnt: intermediate monocyte subset absolute count; ncMo%MONO: non-classical monocyte subset frequency distribution relative to total monocytes (percentage of CD45+/CD14+/CD16+ events) ×100; ncMo Abs Cnt: non-classical monocyte subset absolute count; CI: confidence interval.
Univariate and multivariate logistic regression analyses of moderate–high CCS risk
In the univariate analysis, age, male gender, hypertension, dyslipidemia, smoking, and absolute intMo count were significantly correlated with an increased likelihood of moderate–high risk of CCS (Figure 3). In the subsequent multivariate logistic regression analysis, two models were employed to assess the factors influencing moderate–high CCS risk. Both Models 1 and 2 incorporated age, male gender, diabetes mellitus, hypertension, dyslipidemia, and smoking as variables. Model 1 also included absolute intMo count, while Model 2 included intMo FDMS (percentage of CD45+/CD14+/CD16+ events). Male gender, dyslipidemia, and intMo levels remained significant in both models.
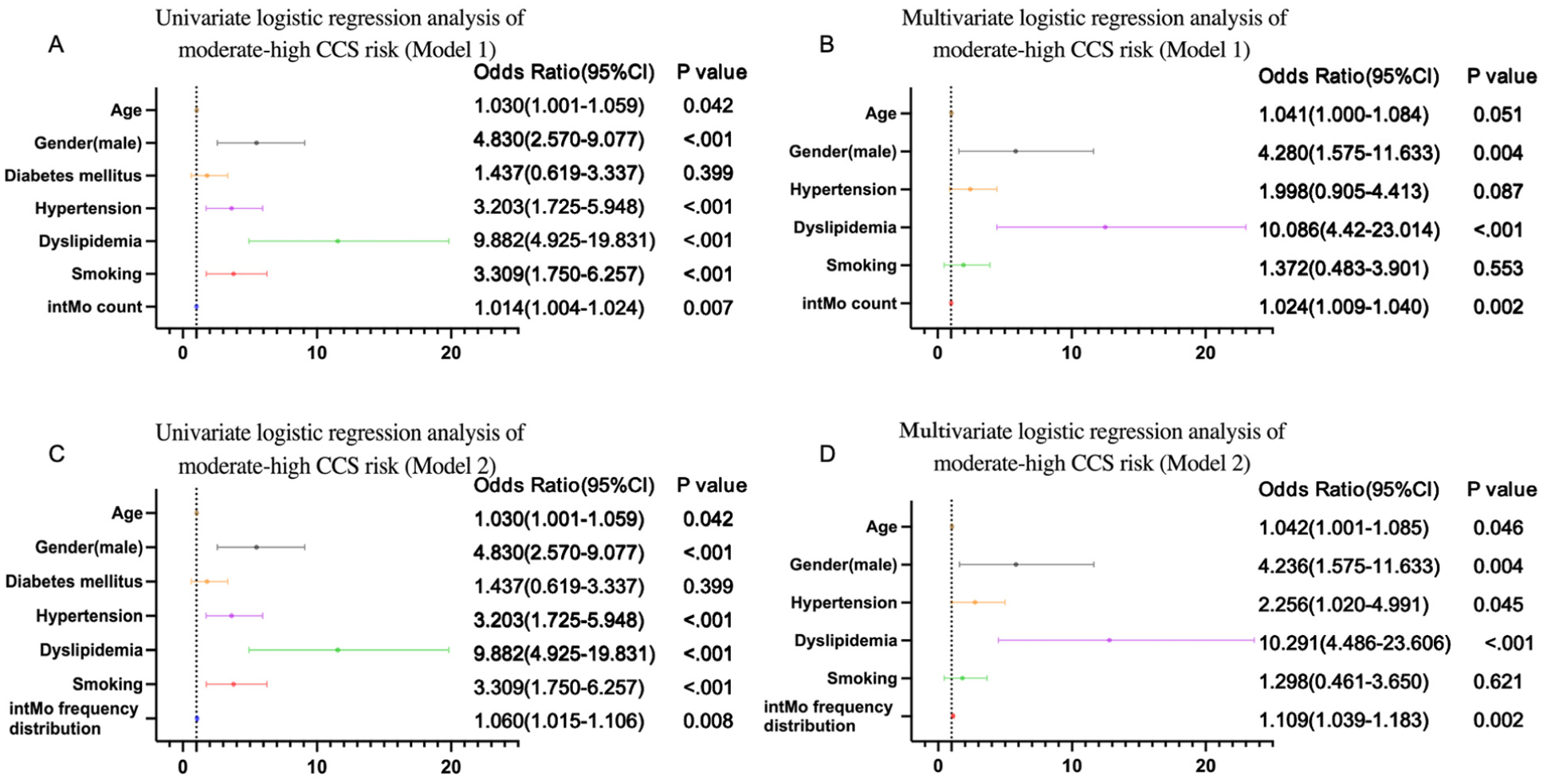
Univariate and multivariate logistic regression analysis of moderate–high CCS risk. Model 1: A and B. Model 2: C and D.
The best absolute intMo count and intMo FDMS (percentage of CD45+/CD14+/CD16+ events) cutoff value for predicting moderate–high risk of CCS
ROC curve analysis identified an absolute intMo count threshold of >27.5 and an intMo FDMS (percentage of CD45+/CD14+/CD16+ events) cutoff of 6.75 as predictive cutoff markers for moderate–high CCS risk, with corresponding sensitivities, specificities, and AUC values detailed in Figure 4.
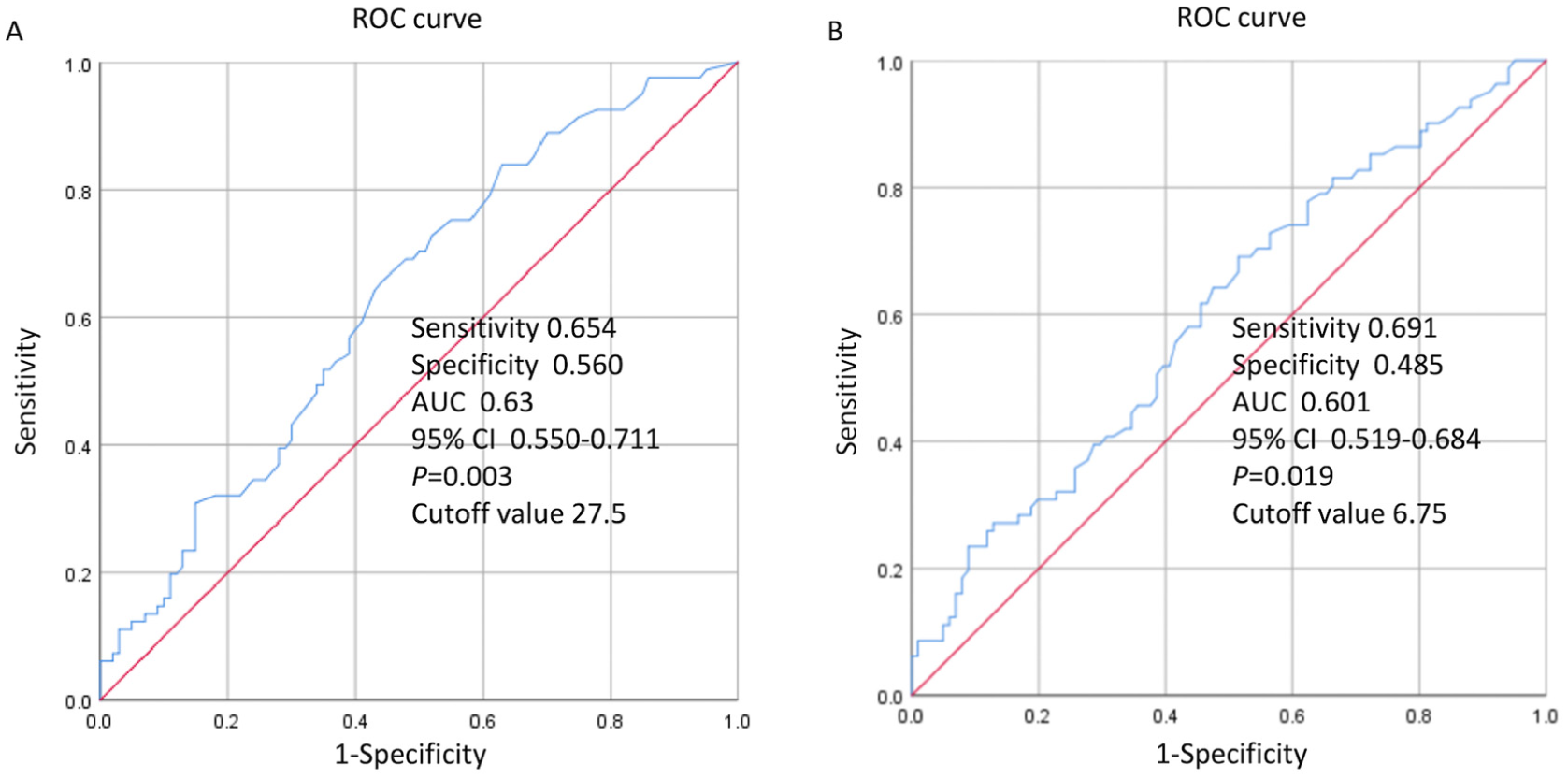
ROC analysis performed to predict moderate–high CCS risk. A. The best intMo count cutoff value. B. The best intMo FDMS (percentage of CD45+/CD14+/CD16+ events) cutoff value.
Discussion
There is currently a lack of research on the relationship between monocyte subsets and CCS. Our study identified the intMo subset as a potential predictive biomarker for CCS in patients with suspected CAD. The absolute count and FDMS (percentage of CD45+/CD14+/CD16+ events) of the intMo subset were higher in the moderate–high risk CCS group than in other groups. Additionally, both the absolute count and FDMS (percentage of CD45+/CD14+/CD16+ events) of the intMo subset were identified as independent CCS predictors.
CAC is a reliable indicator of both coronary atherosclerosis and vascular age. 15 CAC has superior predictive precision in forecasting the onset of CAD and cardiovascular events in both asymptomatic and symptomatic individuals than traditional cardiovascular risk factors.16,17 Moreover, numerous guidelines and consensus statements concur on the predictive value of CAC in evaluating CVD risk.18,19 Several studies now show that CAC can continue to be effective for risk stratification up to 15 years after testing.20,21 Furthermore, CCS may serve as a method for reevaluating the risk of atherosclerotic CVD in individuals initially deemed to have intermediate risk. CCS may improve prediction of undetected coronary stenosis in patients with a history of stroke or transient ischemic attack, surpassing the capabilities of traditional risk factors. 22 Moreover, the absence of CAC (CCS of 0) is a significant negative risk indicator in clinical settings, effectively identifying patients with a very low 10-year risk. 23 However, the diagnostic effectiveness of a CCS of 0 is reduced in younger individuals. In a cohort of symptomatic patients under 60 years of age, a significant proportion of obstructive CAD cases occurred in individuals without detectable CAC, and this was associated with higher mortality and myocardial infarction risks. 24 In addition, the CAC Consortium found that patients with extensive CAC (CCS ≥ 1000) have a distinct very high-risk phenotype with mortality rates comparable to those of high-risk secondary prevention patients. 25
Coronary artery atherosclerosis is characterized by a persistent inflammatory process that includes endothelial dysfunction and lipid metabolism dysregulation. Inflammatory cytokines play a critical role in the pathogenesis of CAD, with growing evidence of their potential utility as biomarkers. Circulating monocytes are integral to the initiation and progression of atherosclerosis via active secretion of cytokines, chemokines, and other factors. 26 Monocyte count is also an independent predictor of major adverse cardiovascular events. 27 A high monocyte count can predict a high thrombus burden in acute ST-elevation myocardial infarction (STEMI) patients, helping to guide anti-thrombotic therapy and improve outcomes after primary percutaneous coronary intervention. 28 Our study found a statistically significant increase in monocyte count within the moderate–high risk group for CCS, compared with the other two groups, which is consistent with data from previous studies.
Recent studies have further elucidated the molecular basis of monocyte diversity, differentiation and functional heterogeneity in human physiological homeostasis and disease states. Komaravolu et al. confirm that the differentiation of cMo to ncMo is a continuous process orchestrated by specific transcriptional programs, rather than a discrete cell state transition. Notably, this study highlighted that intMo lack specific differential activation regulons and act as a transitional cell population sharing core regulons with both cMol and ncMo, which is the key molecular feature underlying the dual functional characteristics of intMo in inflammation and vascular homeostasis. These findings provide a critical transcriptional regulatory basis for understanding monocyte subset functional diversity in vascular homeostasis and explain intMo’s unique role as a transitional mediator between cMo-driven inflammatory activation and ncMo-mediated vascular repair in coronary atherosclerosis. 29
Early researchers thought that vascular calcification was a passive and inevitable result of aging. Today, it is seen as an active process linked to developmental, inflammatory, and metabolic issues. 30 Monocytes/macrophages can express CYP27B1 (the gene encoding 1α-hydroxylase) to convert 25-hydroxyvitamin D3 into its active form, 1,25-dihydroxyvitamin D3, which promotes calcium salt deposition and accelerates vascular calcification. 31 Monocytes/macrophages also release pro-inflammatory factors, such as TNF-α, IL-1b, and IL-6, that can accelerate inflammation and promote vascular calcification. These factors promote differentiation of vascular cells into chondrocytes and osteoblasts, while also increasing production of oxygen free radicals and expression of bone morphogenetic protein.32,33 Furthermore, macrophages secrete osteogenic proteins, including runt-related transcription factor 2, tissue non-specific alkaline phosphatase, and bone morphogenetic protein 2, which facilitate the osteogenic process.33–35 These pathways are all involved in vascular calcification.
Previous research studies suggest that intMo may be associated with inflammatory reactions, may predict risk, and may be related to plaque types in CVDs. In STEMI patients, the intMo subset is important for myocardial healing. While higher intMo numbers are linked to better outcomes, increased cMo levels are associated with poorer outcomes.36–38 In addition, the intMo subset can predict adverse cardiovascular events 2 years after acute myocardial infarction and is the only subset capable of independently predicting CVD risks during a 3-year follow-up in patients undergoing elective coronary angiography.39–42 An elevated intMo count in coronary arteries is a predictor of poor prognosis for CVD, and monocyte subset counts are significantly correlated with Framingham risk scores. 43 In CAD patients, intMo is associated with high CAD (quantified using the Gensini Score), with a robust sex-dependent positive correlation in female patients. 44 In patients with stable CAD, intMo was associated with MACE at the 4-year follow-up. 45
Moreover, different monocyte subsets may be linked to specific plaque types; intMo levels correlate with mixed and calcified plaques, and cMo levels correlate with non-calcified plaques. 46 Furthermore, intMo levels have also been associated with vulnerable plaque features in asymptomatic coronary artery plaques. 47 Yamamoto et al. identified a correlation between intMo count and plaque vulnerability in CAD patients. 48 While Meeuwsen et al. found no specific subset linked to plaque vulnerability in their study of 175 patients, their data suggested that the intMo subset may be associated with vulnerable plaque features, such as calcification. 49 The identification of CD16+ monocytes in the bloodstream, suggestive of a subset with heightened susceptibility to atherosclerosis, emerged as a standalone prognostic indicator for accelerated CAC progression in human immunodeficiency virus-infected individuals at low risk for acquired immunodeficiency syndrome development. 50 Our study also found higher levels of intMo in the moderate–high risk CCS group, indicating that intMo may be a predictive biomarker for CAD. A recent study introduced AtheroSpectrum, a tool that identifies gene expression profiles in inflammatory macrophage foam cells linked to atherosclerosis. It found two types of foaming programs: homeostatic and pathogenic, with the latter associated with atherosclerosis development. 51 This suggests that classification of macrophage foam cells within different monocyte subsets may enhance the ability to predict the risk and severity of atherosclerosis.
While the ROC curve analysis for both intMo count and FDMS (percentage of CD45+/CD14+/CD16+ events) showed statistically significant results (p < 0.05), the AUC values (0.60−0.63) indicate only modest predictive power. Given the low sensitivity and specificity, we acknowledge that intMo alone may not serve as a highly effective marker for identifying moderate-to-high risk CCS. Although traditional risk factors such as male gender (OR = 4.236), hypertension (OR = 2.256), and dyslipidemia (OR = 10.291) displayed higher ORs compared with intMo (OR = 1.024−1.109), the combination of intMo with these established risk factors may still enhance the risk stratification for moderate-to-high CCS. Therefore, we propose that intMo be used in conjunction with traditional risk factors, which may significantly improve predictive accuracy.
Limitations
This study had a limited sample size and used a dual-center cross-sectional design. Therefore, future research should focus on multi-center studies with larger sample sizes to better assess the relationship between monocyte subsets and CCS. The correlation that we observed between the intMo subset and moderate–high CCS risk did not establish a causal relationship with CVD. Additionally, the clinical relevance of different monocyte subsets for guiding coronary angiography and revascularization therapy is unclear without coronary angiography data. Repeat blood sampling and coronary angiography were not performed due to logistical constraints and the cross-sectional nature of the study. Therefore, follow-up data are needed to confirm whether monocyte subsets are risk factors for CAD and to develop models for predicting CAD in high-risk individuals. Finally, it would be appropriate to verify whether the expression level of monocyte markers, such as activation and adhesion molecules, as well as chemokine receptors, present on the intMo subset, is significantly and independently associated with the degree of coronary calcification.
Conclusion
In conclusion, the absolute count and ratio of the intMo subset were significantly associated with an increased risk of moderate–high CCS risk in patients with suspected CAD. These results suggest that intMo may be a potential biomarker for CCS risk stratification.
Footnotes
Acknowledgements
The authors would like to thank for the support from the Ministry of Science and Technology of the People’s Republic of China, State Science and Technology Support Program (No. 2011BAI11B05; 82370412) and the Beijing Lab for Cardiovascular Precision Medicine, Beijing, China (PXM2019_014226_000023).
Ethical considerations
The study was approved by the ethics committees of the two participating hospitals (Approval No. 25024058X and 2023-011KY). All procedures performed in this study were in accordance with the Declaration of Helsinki 1975 (as revised in 2000).
Consent to participate
The written informed consent was obtained from the participants or their guardians before enrollment in this study.
Consent for publication
The written informed consent was obtained from the participants or their guardians.
Author contributions
G.L.,: Conceptualization, Methodology. L.Y.,: Writing – Original draft preparation. T.F.,: Data curation, Visualization, Investigation. T.Z.,: Supervision. L.Z., and L.W.,: Software, Validation. L.Z.,: Writing – Reviewing and Editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science and Technology of the People’s Republic of China, State Science and Technology Support Program (No.2011BAI11B05; 8) and the Beijing Lab for Cardiovascular Precision Medicine, Beijing, China (PXM2019_014226_000023).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare no conflict of interest.
Data availability statement
Data can be obtained by contacting the corresponding author, Dr. Lin Zhao, MD, PhD, at