
Abstract
This study aimed to evaluate the association between intraocular pressure (IOP) and circadian blood pressure (BP) patterns—specifically dipper and nondipper status—in patients with newly diagnosed essential hypertension. A total of 180 participants were enrolled and equally divided into individuals with normal blood pressure (n = 90) and individuals with hypertension (n = 90). Individuals with hypertension were further classified into dipper and nondipper subgroups based on 24-h ambulatory BP monitoring. IOP was assessed using a noncontact tonometer during morning hours (9:00 a.m.–12:00 p.m.). Individuals with hypertension demonstrated significantly higher right and left eye IOP values compared to individuals with normal blood pressure (16.86 ± 3.84 mmHg vs 14.56 ± 2.79 mmHg and 16.69 ± 4.02 mmHg vs 14.43 ± 3.08 mmHg, respectively; both p < 0.001). Among hypertensives, nondippers had significantly higher IOP than dippers (right eye: 17.91 ± 3.93 vs 15.85 ± 3.52 mmHg, p = 0.010; left eye: 17.88 ± 3.98 vs 15.55 ± 3.76 mmHg, p = 0.005). Linear regression analysis identified 24-h systolic BP (β = 0.902, 95% confidence interval (CI): 0.220 to 0.395, p < 0.001) and nondipper status (β = −0.608, 95% CI: −7.294 to −3.218, p < 0.001) as independent predictors of mean IOP in individuals with newly diagnosed and untreated hypertension. Receiver operating characteristic analysis revealed that, in individuals with newly diagnosed and untreated hypertension, a mean IOP ≥ 16.85 mmHg predicted nondipping status with 59.1% sensitivity and 63% specificity (area under the curve = 0.666, p = 0.007). These findings suggest that a nondipping circadian BP profile is independently associated with elevated IOP in individuals with newly diagnosed and untreated hypertension, emphasizing the potential value of ocular pressure monitoring in this population, particularly those without nocturnal BP decline.
Introduction
Hypertension, a pervasive cardiovascular condition characterized by elevated blood pressure (BP), continues to captivate the attention of the medical community because of its far-reaching impact on health. 1 As our understanding of hypertension has expanded, researchers have begun to explore its correlations beyond traditional cardiovascular endpoints. One such intriguing avenue of investigation is the relationship between hypertension and intraocular pressure (IOP), a critical determinant of ocular health.
IOP, the force exerted by fluid within the eye, plays a pivotal role in maintaining the structural integrity of ocular tissues and preserving visual function. 2 The relationship between hypertension and IOP is mediated by several physiological mechanisms. One primary mechanism involves the increased episcleral venous pressure observed in hypertensive individuals, which can hinder aqueous humor outflow, thereby elevating IOP. 3 In addition, hypertension is often associated with systemic vascular endothelial dysfunction, which can impair the autoregulatory capacity of ocular blood vessels, leading to fluctuating IOP levels. 4 Sympathetic nervous system overactivity, common in hypertensive patients, may also contribute to increased aqueous humor production by stimulating the ciliary body. Furthermore, structural changes in the microvasculature due to chronic hypertension, such as increased arterial stiffness and reduced compliance, may directly impact ocular perfusion pressure and, consequently, IOP. 5
Epidemiological data suggest that individuals with hypertension are at a higher risk of developing elevated IOP and glaucoma compared to normotensive individuals.6,7 Experimental studies have also demonstrated that hypertensive animal models exhibit higher IOP levels and increased susceptibility to glaucomatous damage. 8 These findings suggest that the vascular and autonomic dysregulation inherent in hypertension may predispose individuals to ocular hypertension. Therefore, understanding the intricate relationship between systemic hypertension and IOP is crucial for developing comprehensive management strategies for hypertensive patients at risk of ocular complications.
This study aimed to evaluate the correlation between dipper and nondipper BP patterns in hypertensive individuals and their impact on IOP. Dipper and nondipper classifications are critical in understanding nocturnal BP variability. Dippers experience a physiological nocturnal decline in BP of at least 10%, reflecting normal circadian rhythms. In contrast, nondippers exhibit less than a 10% reduction or even an increase in BP during sleep, indicating disrupted circadian regulation.1–3 This distinction is clinically significant as nondipping patterns are associated with higher risks of cardiovascular events, end-organ damage, and overall poorer prognosis compared to dipping patterns.
Analyzing dipper and nondipper BP patterns involves several methodologies, including ambulatory BP monitoring (ABPM), which provides a comprehensive 24-h BP profile. ABPM is widely regarded as the most reliable method for detecting nocturnal BP variations and distinguishing between dipper and nondipper hypertension patterns. Previous studies have elucidated various mechanisms underlying these patterns. For instance, nondipper hypertension is often linked to sympathetic overactivity, impaired baroreflex sensitivity, and increased arterial stiffness. Furthermore, nondippers tend to exhibit higher levels of pro-inflammatory markers and oxidative stress, contributing to vascular endothelial dysfunction. 4 These mechanisms suggest that nondippers may experience more pronounced systemic and ocular vascular dysregulation, potentially leading to higher IOP and an increased risk of glaucoma.
While numerous studies have examined the impact of elevated BP on IOP, limited evidence exists regarding the specific effects of circadian BP patterns—namely, dipper versus nondipper profiles—on IOP among patients with essential hypertension. Given the vascular and autonomic dysregulation associated with nondipping status, it may be hypothesized that patients with a nondipping BP pattern would exhibit significantly higher IOP levels compared to those with a dipping pattern. Therefore, the present study aimed to evaluate the differential impact of circadian BP patterns on IOP in patients with newly diagnosed essential hypertension, with the overarching goal of providing insights for more tailored cardiovascular and ophthalmological risk assessments in this population.
Significance Statement
Blood pressure follows a circadian pattern, and the absence of nocturnal dipping (i.e. nondipping) is associated with increased cardiovascular risk and end-organ damage.
Intraocular pressure (IOP) is influenced by systemic hemodynamic and neurohumoral factors, including blood pressure regulation.
Previous studies have demonstrated a general association between hypertension and elevated IOP, but limited evidence exists on how circadian BP patterns affect ocular pressure.
This study shows that individuals with newly diagnosed and untreated hypertension and a nondipping blood pressure profile exhibit significantly higher intraocular pressure than those with a dipping profile, independent of other confounding variables.
Linear regression analysis identified 24-h systolic BP and nondipping status as independent predictors of mean IOP in individuals with newly diagnosed and untreated hypertension.
A mean IOP cutoff value of ≥16.85 mmHg demonstrated moderate diagnostic accuracy in predicting nondipping status in individuals with newly diagnosed and untreated hypertension.
These findings suggest that IOP measurements may serve as a simple, adjunctive tool for identifying hypertensive patients with altered circadian BP rhythms.
Routine IOP screening in newly diagnosed hypertensives, particularly those suspected of nondipping status, may contribute to early detection of individuals at higher ocular and systemic risk.
Integration of ocular assessments into hypertension management protocols may enhance personalized risk stratification and preventive care.
Materials and method
This cross-sectional, controlled study was conducted between December 2021 and December 2022 at Aksehir State Hospital. A total of 273 adult patients who presented to the cardiology outpatient clinic with elevated BP readings—yet had no prior diagnosis of hypertension—were screened for eligibility. All patients underwent 24-h ABPM as part of routine clinical evaluation. Based on this assessment, patients were classified as either hypertensive or normotensive according to the 2024 ESC Guidelines for hypertension. 9 Ethical clearance was granted by Aksaray University’s Ethics Committee (Decision No: 2021/17-01, Protocol No: 51-SBKAEK Date: 16.12.2021).
Exclusion criteria included a history of open-angle glaucoma, ocular hypertension (defined as IOP ≥ 21 mmHg without optic nerve or visual field changes), previous ocular surgery, current use of antihypertensive medication, and the presence of systemic diseases such as diabetes mellitus, malignancy, rheumatological disease, or chronic kidney disease (defined as eGFR < 60 mL/min/1.73 m2). After applying these exclusion criteria, 93 patients were excluded (42 due to ophthalmologic conditions and 51 because of systemic comorbidities). The final study cohort included 180 participants, divided into 2 equal groups: individuals with hypertension (n = 90) and individuals with normal blood pressure (n = 90). The hypertensive group was further stratified into dipper and nondipper subgroups based on nocturnal BP reduction assessed via ABPM (Figure 1).
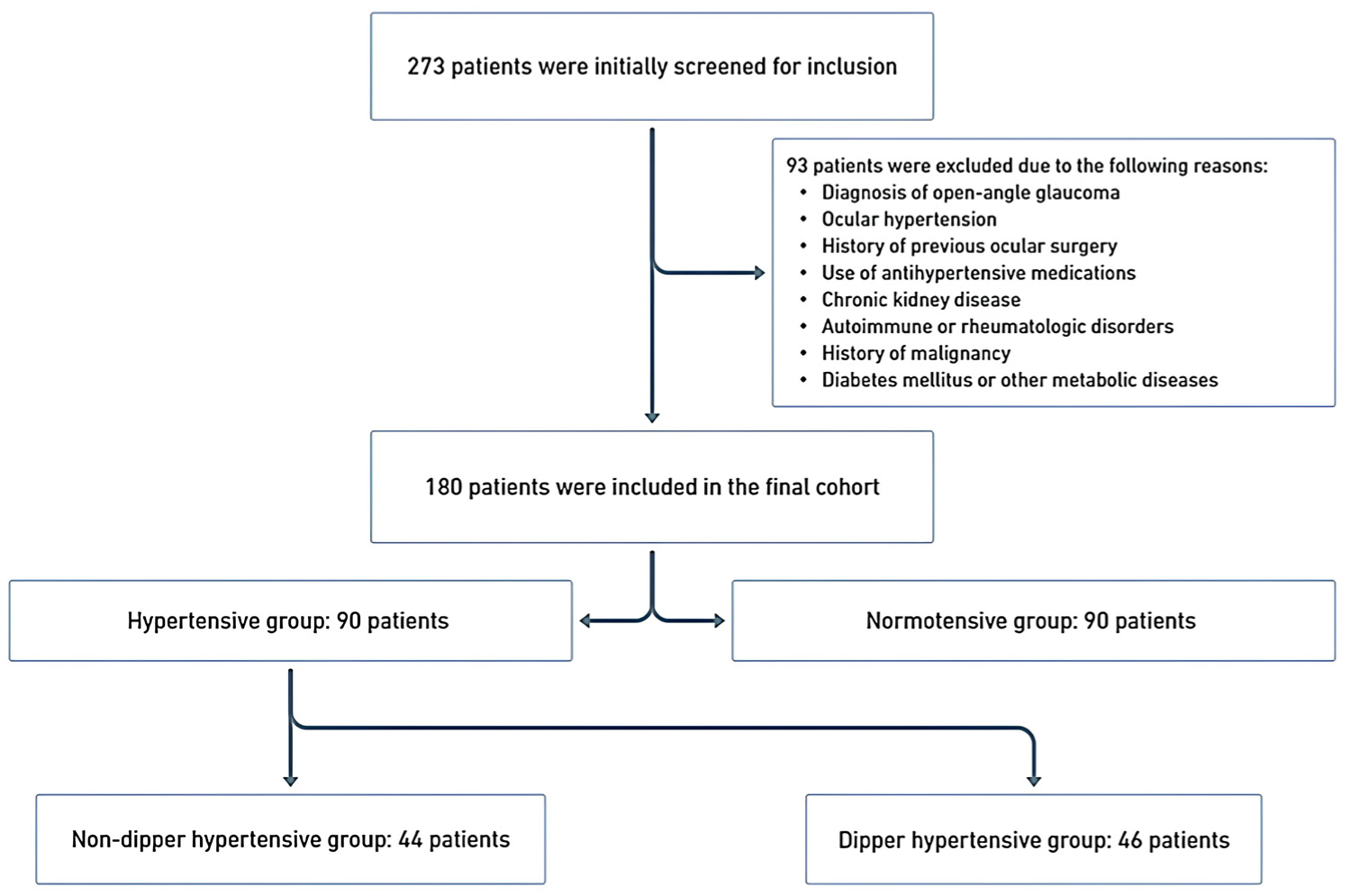
Flowchart illustrating the patient selection process.
Blood pressure measurement using ambulatory blood pressure monitoring
BP was continuously monitored utilizing a Mobil-O-Graph Arteriography device (I.E.M. GmbH, Stolberg, Germany). The monitoring covered a period of 24 h and was conducted on the nondominant arm. Measurements were obtained at 15-min intervals during the day (from 7 a.m. to 10 p.m.) and at 30-min intervals during the night (from 10 p.m. to 7 a.m.). A qualified daytime and nighttime measurement was defined as having at least 14 valid readings and at least 7 valid readings during the awake and asleep periods, respectively. 10 The patients were instructed to adhere to their usual daily activities and maintain a stationary posture during the measurement process. Mean values for systolic BP (SBP), diastolic BP (DBP), and overall BP were computed separately for daytime, nighttime, and the entire 24-h period.
Diagnosis of hypertension
The diagnosis of hypertension (HT) was established based on the following criteria: a 24-h mean SBP exceeding 130 mmHg and/or a DBP surpassing 80 mmHg; a daytime mean SBP greater than 135 mmHg and/or a DBP higher than 85 mmHg; and a nighttime SBP exceeding 120 mmHg and/or a DBP surpassing 70 mmHg. 9 When there was an average reduction of more than 10% in nocturnal SBP and DBP compared to daytime levels, the patient was classified as “dipper HT.” 11
Laboratory measurements
Blood samples were collected during outpatient clinic visits for complete blood analysis and serum biochemistry analysis. The complete blood analysis included parameters such as hemoglobin levels, white blood cells, neutrophils, platelets, and lymphocytes. Serum biochemistry included measurements of total cholesterol, high-density lipoprotein (HDL) levels, low-density lipoprotein (LDL) levels, serum creatinine levels, fasting blood glucose levels, and triglyceride levels. Estimated glomerular filtration rate (eGFR) was calculated using the CKD-EPI formula.
Ocular examination and IOP measurements
Each patient underwent a thorough ocular examination, including visual acuity assessment, slit-lamp examination, fundus examination, and tonometry. IOP was measured using a noncontact tonometer (NCT-10, Shin Nippon, Japan). The same experienced technician took the measurements to apply consistent and accurate techniques and to reduce the risk of measurement errors. To enhance the reliability of the results and consider any potential variability in measurements, the average IOP was calculated based on three separate measurements. Considering the diurnal variations and to obtain accurate and reliable results, IOP measurements were taken specifically between 9:00 a.m. and 12:00 p.m.
Statistical analysis
All statistical analyses were performed using SPSS 29.0 (SPSS, Inc., Chicago, IL, USA). The normality of the distribution of the numerical variables was assessed using the Kolmogorov–Smirnov test. Descriptive statistics for the numerical variables were presented as mean ± standard deviation and median (25th–75th percentile), while categorical data were expressed as numbers and percentages. Two-group comparisons of numerical variables were conducted using the independent samples t-test or Mann–Whitney U test, depending on the assumptions of the parametric test. Categorical variables were analyzed using the Chi-square test. To explore the bivariate relationships between continuous variables, Pearson correlation coefficients were computed. Linear regression analysis was used to predict the mean IOP. The stepwise regression analysis method was used to identify the most predictive model in the regression analysis. Receiver operating characteristic (ROC) curve analysis was also conducted to determine the diagnostic cutoff value for nondipping HTs. A p value of <0.05 was considered to indicate statistical significance in all evaluations.
Results
The study involved 180 participants who were equally divided into individuals with normal BP and individuals with hypertension (Table 1). Age and gender distributions were not significantly different (p = 0.720 and p = 0.549, respectively). Clinical parameters such as body mass index (BMI), LDL level, HDL level, triglyceride level, hemoglobin level, white blood cell count, and platelet count were comparably distributed across both groups, confirming the absence of confounding factors attributable to these variables. In individuals with hypertension, glucose (p = 0.100) and creatinine (p = 0.085) levels were marginally elevated.
Comparison of demographic, clinical, and laboratory characteristics of the study population.
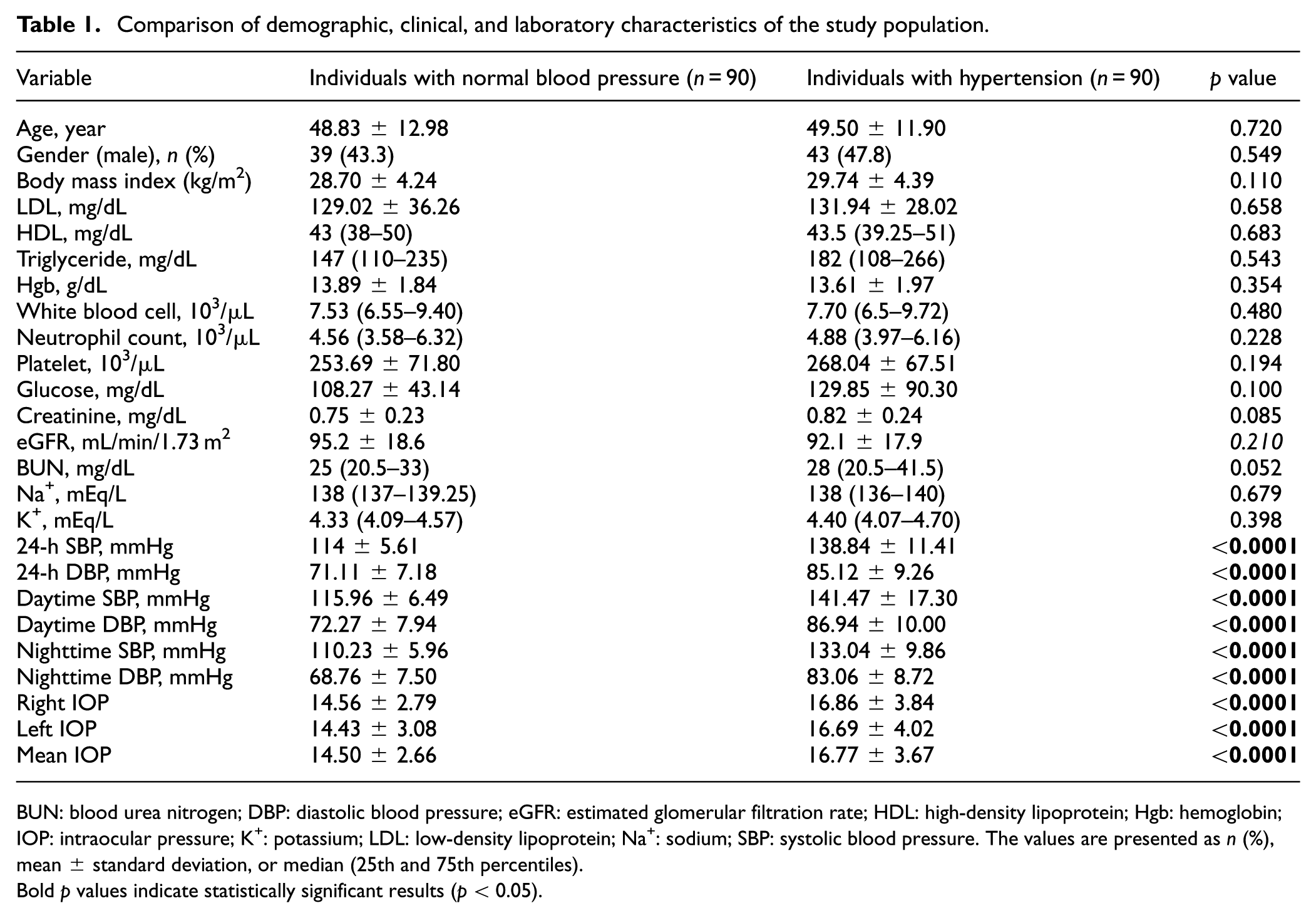
BUN: blood urea nitrogen; DBP: diastolic blood pressure; eGFR: estimated glomerular filtration rate; HDL: high-density lipoprotein; Hgb: hemoglobin; IOP: intraocular pressure; K+: potassium; LDL: low-density lipoprotein; Na+: sodium; SBP: systolic blood pressure. The values are presented as n (%), mean ± standard deviation, or median (25th and 75th percentiles).
Bold p values indicate statistically significant results (p < 0.05).
A main finding of the current study was the significant increase in SBP and DBP in the hypertensive group across all measured intervals (24 h, daytime, and nighttime; p < 0.001 for all). IOP measurements revealed significant elevations in both right (16.86 ± 3.84 mmHg) and left (16.69 ± 4.02 mmHg) eyes in hypertensive patients compared to their normotensive counterparts (14.56 ± 2.79 mmHg and 14.43 ± 3.08 mmHg, respectively) (p < 0.001)
Further stratification of individuals with hypertension into dipper and nondipper subgroups yielded comparable distinctions. The age and gender distributions showed no significant differences (p = 0.819 and p = 0.680, respectively). Additionally, clinical parameters, including BMI, LDL levels, HDL levels, triglyceride levels, hemoglobin levels, white blood cell count, and platelet count, were similarly distributed across both groups, indicating that these variables did not introduce any confounding factors. Nondippers exhibited significantly elevated nighttime SBP, aligning with the established definition of this subgroup. IOP in the right and left eye was markedly greater in the nondippers (17.91 ± 3.93 mmHg and 17.88 ± 3.98 mmHg, respectively) compared to the dippers (15.85 ± 3.52 mmHg and 15.55 ± 3.76 mmHg, respectively) (p = 0.01 and p = 0.005, respectively) (Table 2).
Comparison of demographic, clinical, and laboratory characteristics between the dipper and nondipper groups.
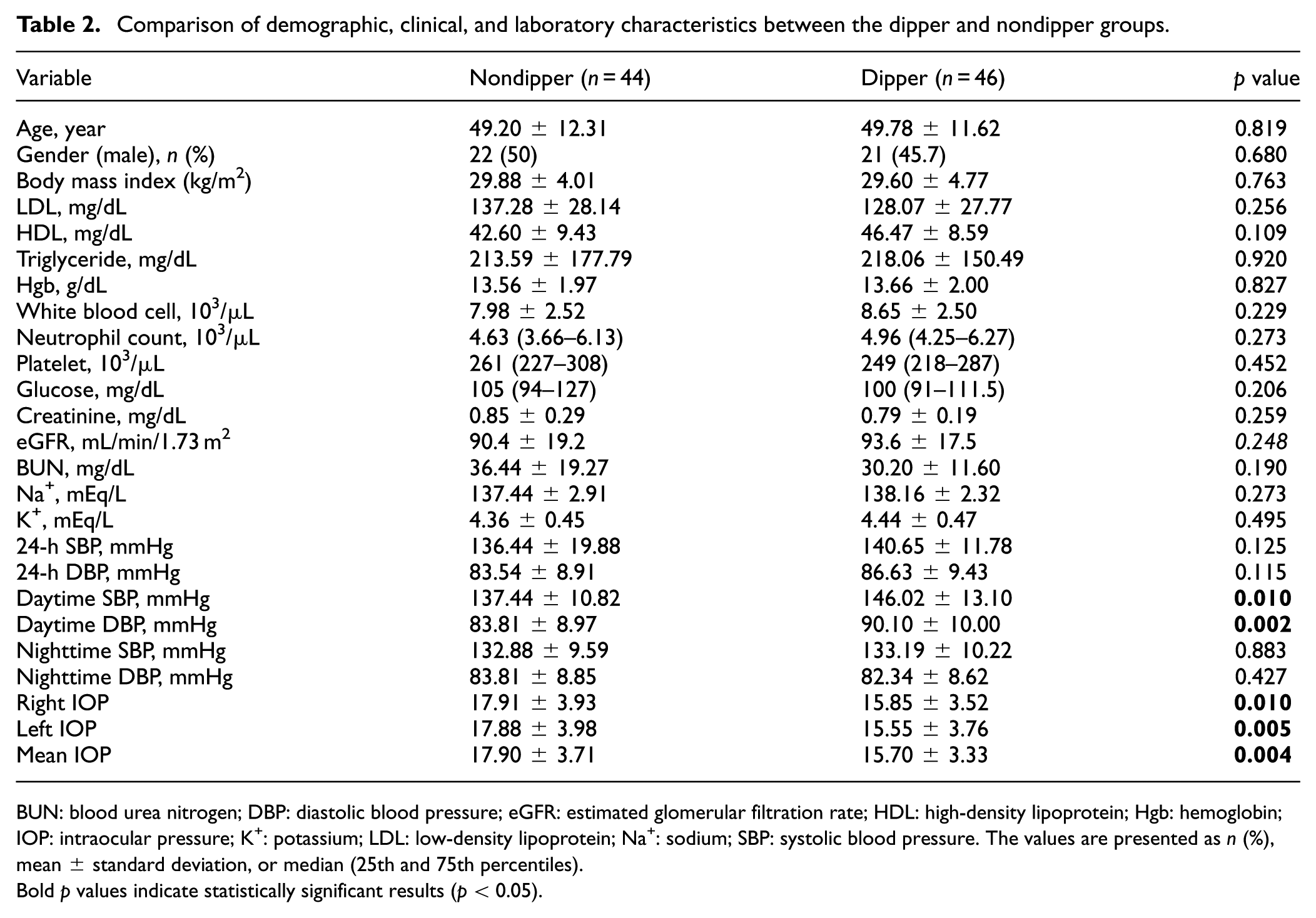
BUN: blood urea nitrogen; DBP: diastolic blood pressure; eGFR: estimated glomerular filtration rate; HDL: high-density lipoprotein; Hgb: hemoglobin; IOP: intraocular pressure; K+: potassium; LDL: low-density lipoprotein; Na+: sodium; SBP: systolic blood pressure. The values are presented as n (%), mean ± standard deviation, or median (25th and 75th percentiles).
Bold p values indicate statistically significant results (p < 0.05).
According to the bivariate linear correlation analysis, the mean IOP was positively correlated with 24-h SBP (r = 0.363, p < 0.001), 24-h DBP (r = 0.213, p = 0.004), daytime SBP (r = 0.303, p < 0.001), daytime DBP (r = 0.196, p = 0.008), nighttime SBP (r = 0.367, p < 0.001), and nighttime DBP (r = 0.251, p = 0.001). However, the mean IOP was negatively correlated with nondipper/dipper status (r = -0.367, nondipper (0) → dipper (1), p < 0.001) (Table 3).
Bivariate correlation analysis based on mean IOP in all patients.
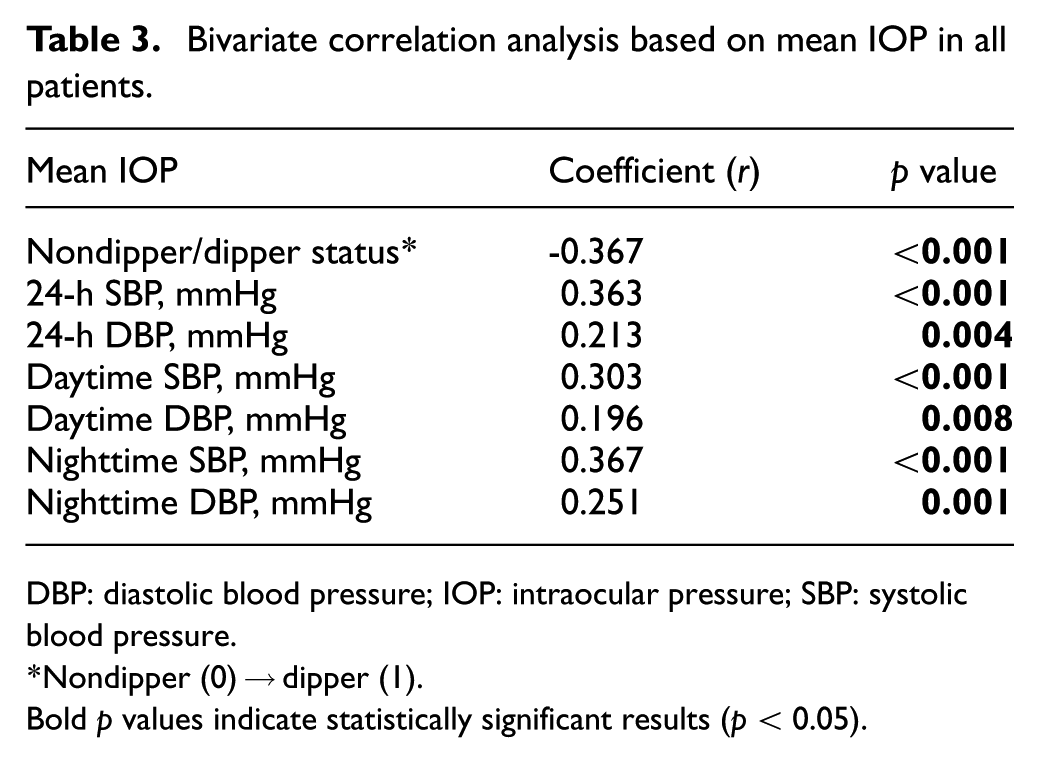
DBP: diastolic blood pressure; IOP: intraocular pressure; SBP: systolic blood pressure.
Nondipper (0) → dipper (1).
Bold p values indicate statistically significant results (p < 0.05).
The linear regression analysis conducted to predict the mean IOP revealed the following variables as significant predictors: 24-h SBP (24-h SBP) with a coefficient (β) of 0.902 and a 95% confidence interval (CI) of 0.220 to 0.395 (p < 0.001); nondipper/dipper status (β = -0.608, 95% CI -7.294 to -3.218, nondipper (0) → dipper (1), p < 0.001); neutrophil count (β = -0.483, 95% CI -1.729 to -0.653, p < 0.001); and nighttime DBP (nighttime DBP) (β = -0.342, 95% CI -0.320 to -0.057, p = 0.006). The coefficient of determination (R2) for the linear regression model was 0.70 (Table 4).
Linear regression analysis of independent variables associated with mean intraocular pressure in patients with hypertension.*
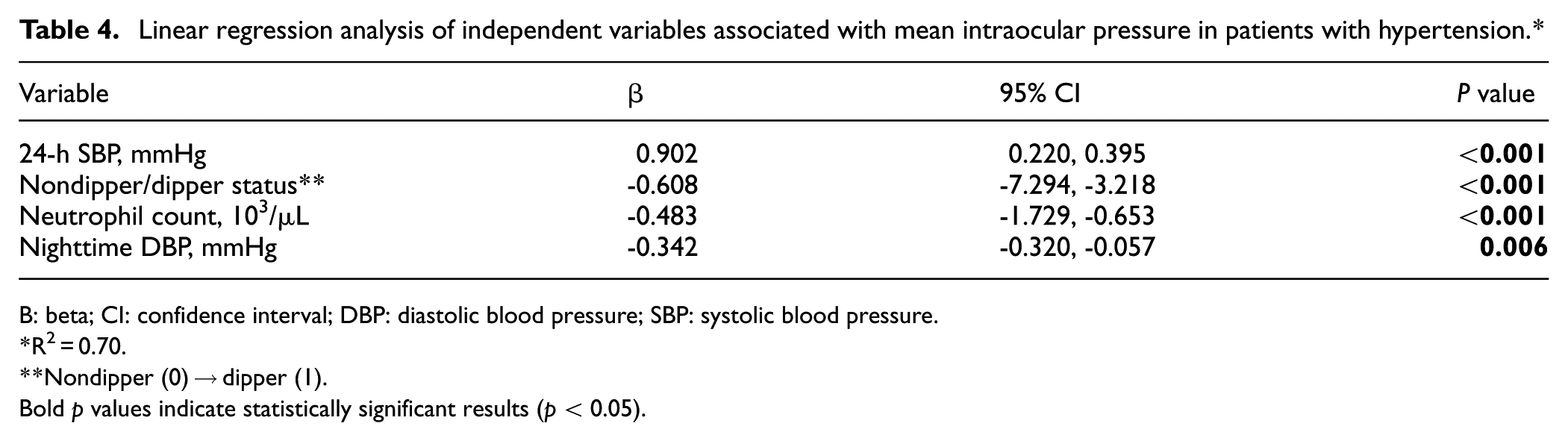
B: beta; CI: confidence interval; DBP: diastolic blood pressure; SBP: systolic blood pressure.
R2 = 0.70.
Nondipper (0) → dipper (1).
Bold p values indicate statistically significant results (p < 0.05).
According to the ROC analysis, the optimal cutoff values of mean IOP, right eye IOP, and left eye IOP for predicting a nondipping BP pattern were 16.85, 17.05, and 16.4 mmHg, respectively, with corresponding sensitivities of 59.1%, 61.4%, and 61.4%, and a specificity of 63% for all measurements. The corresponding area under the curve (AUC) values were 0.666 (p = 0.007), 0.636 (p = 0.026), and 0.680 (p = 0.003), respectively, as illustrated in Figure 2/Table 5.
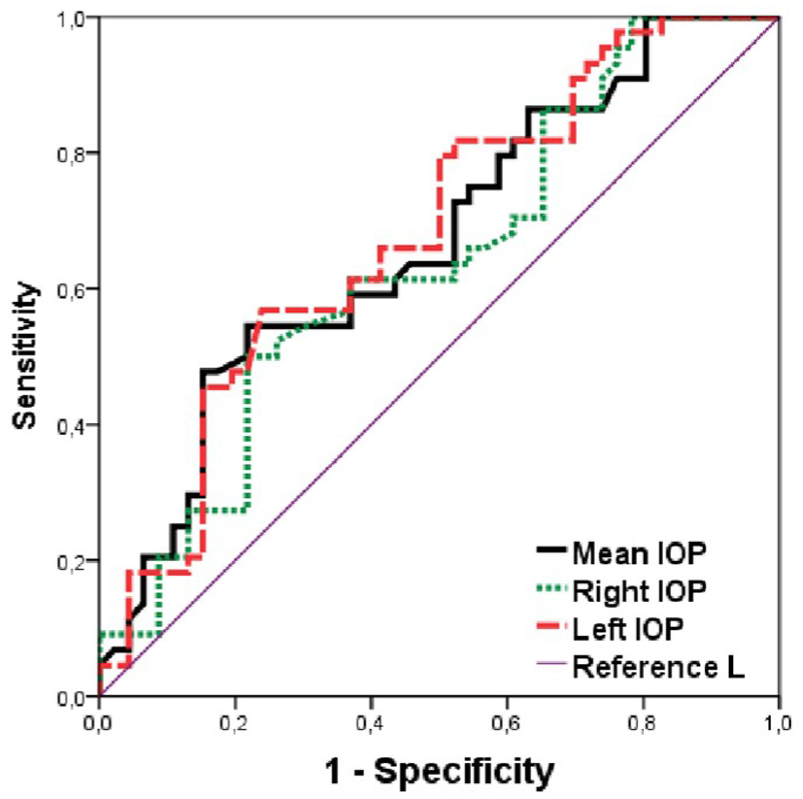
ROC analysis depicting the sensitivity and specificity of IOP in the prediction of nondipping BP patterns. Mean IOP, Right IOP, and Left IOP are compared against the reference line, which is the diagonal line from the origin to the top right corner. The closer the curve is to the top left corner, the better the performance of the IOP measure. ROC, receiver operating characteristic; IOP, intraocular pressure; BP, blood pressure.
ROC Analysis Depicting the Sensitivity and Specificity of IOP in the Prediction of Nondipping BP Patterns.
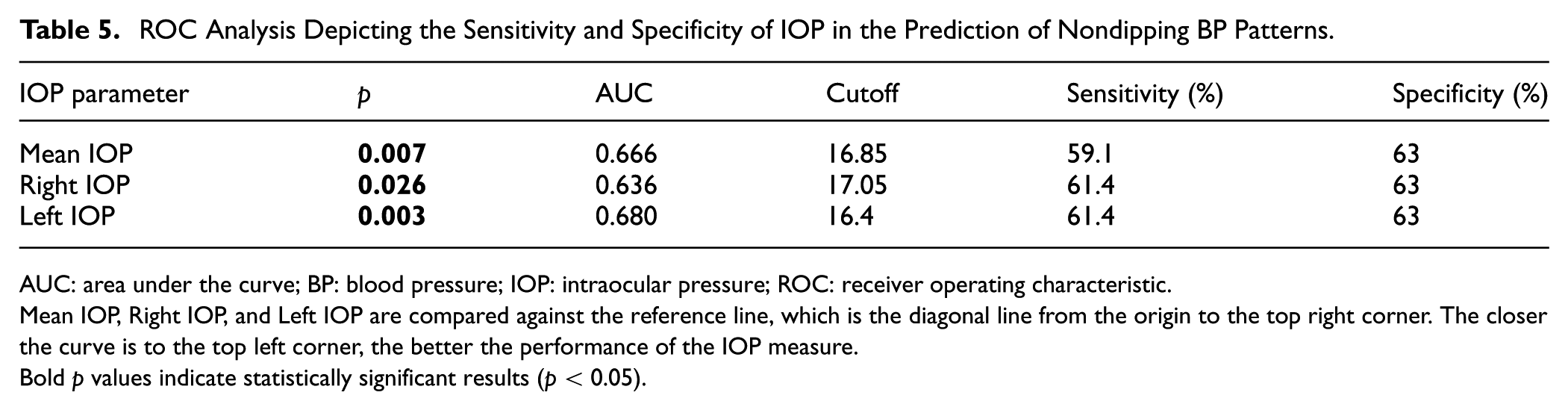
AUC: area under the curve; BP: blood pressure; IOP: intraocular pressure; ROC: receiver operating characteristic.
Mean IOP, Right IOP, and Left IOP are compared against the reference line, which is the diagonal line from the origin to the top right corner. The closer the curve is to the top left corner, the better the performance of the IOP measure.
Bold p values indicate statistically significant results (p < 0.05).
Discussion
The main findings of the current study revealed that IOP increased in individuals with essential hypertension compared with individuals with normal BP. Furthermore, IOP values increased even further in the nondipper HT subgroup compared to those in the dipper HT subgroup. Increased IOP was independently associated with a nondipping circadian BP pattern in patients with essential HT. In this regard, the emergence of new cutoff values for the right, left, and mean IOPs in the ROC analysis may prove to be as useful as a simple and reproducible diagnostic tool in the estimation of the nondipper/dipper status of patients with newly diagnosed essential HT. As such, the findings of the study may contribute further to the current literature regarding HT and IOP. To the best of our knowledge, this is the first study conducted on the relationship between IOP and the circadian pattern of BP in patients with essential HT.
The circadian variation is largely governed by neuroendocrine mechanisms. 5 Previous studies have demonstrated that, compared with the dipper pattern, the nondipper HT pattern is linked more closely to cardiovascular morbidity and mortality owing to more extensive end-organ injury.12,13,14 Exposure to a greater BP burden in the long term is associated with more impaired endothelial functioning and widespread vascular inflammation, which may primarily account for the greater deleterious effects of the nondipping HT pattern than of the dipping pattern. Higashi et al. 15 demonstrated that endothelial vasodilatation was impaired due to a decrease in nitric oxide in nondipper HT patients compared with dippers. In another study by Huang et al., 16 flow-mediated vasodilatation was poorer in the brachial artery in HT patients with a nondipping circadian BP pattern than in those with a dipping pattern. Özen and Karahan 17 proposed that a nondipping BP pattern influenced coronary slow flow in HT patients with normal epicardial coronary arteries. In their study, Kaya et al. 18 showed higher C-reactive protein levels in nondipper HT patients than in dippers. Similarly, Tosu et al. 19 demonstrated greater C-reactive protein, uric acid, red cell distribution width, inflammation, and oxidative stress markers, in nondipper HT patients than in dipper HT patients. In their study, Elçik et al. 20 showed that a nondipping circadian pattern in HT patients was an independent predictor of coronary artery disease progression.
Previous studies have demonstrated a positive correlation between BP and elevated IOP and between the presence of HT and elevated IOP.21–24 In the studies by McLeod et al. and Zhao et al., increased SBP was associated with increased IOP.24,25 Likewise, Shiose 26 reported that obesity and systolic hypertension with aging were significantly associated with increased IOP. Furthermore, Yasukawa 27 demonstrated that not only systolic but also DBP and the presence of essential hypertension were positively related to ocular hypertension. In addition, this relationship was more robust and significant when considering SBP levels than DBP levels. In this study, patients with newly diagnosed essential hypertension were recruited to eliminate the potential confounding effects of antihypertensive medication status and to avoid the need for further complex statistical analyses. However, further stratified analyses in the study by Yasukawa et al. regarding the confounding effects of antihypertensive medication status may have contributed to the consistent positive association between BP and IOP.
In another study by Karadağ et al., healthy normotensive individuals were divided into 2 subgroups on the basis of 24-h ABPM readings: a group with dippers and a group with a nondipper BP pattern. They reported no significant change in IOPs between the two subgroups despite a notable decrease in ocular pulse amplitude in the nondippers. 28 However, a significant increase in IOP was observed in the nondipper essential hypertension group in the current study. The similar findings in terms of IOP values between the nondipper and dipper subgroups in the study by Karadağ et al. may be attributed solely to the inclusion of healthy normotensive subjects and a relatively small study population. On the other hand, both healthy normotensive subjects and patients with newly diagnosed essential hypertension were included in the present study, and results comparable to those of previous studies were obtained.
There is no clear-cut pathogenetic explanation underlying the relationship between circadian variation in BP and IOP changes in essential HT patients. Hypotheses on this issue revolve mainly around potential vascular dysregulation, including increased ultrafiltration of aqueous humor owing to escalated pressure in the ciliary artery and restricted aqueous humor removal due to increased episcleral venous pressure.22,29 In addition, it is further hypothesized in the present study that deterioration in aortic elasticity, autonomic dysfunction, endothelial function, and vascular inflammation, which are more prevalent in nondipper HT patients than in dipper HT patients, are likely to incur aqueous humor overfiltration and/or ill resorption, leading to a greater increase in IOP in nondipper essential HT patients than in dipper HT patients.2,6,12,30–34 It may be speculated that since nondipping BP patterns pose much greater potential cardiovascular, inflammatory, and neuroendocrine risks on human homeostasis, the observed greater IOP values in the nondipper group would partially be explained by these escalated cardiovascular, neuroendocrine, and inflammatory risks imposed by the nondipping circadian BP pattern.
Although IOP measurements were obtained at a single time point between 9:00 a.m. and 12:00 p.m., this period corresponds to the well-established circadian peak of IOP, which typically occurs during early morning hours due to nocturnal aqueous humor dynamics and hormonal fluctuations. Therefore, this window was purposefully selected to capture the physiological apex of IOP values.35–37
More importantly, the present hypothesis does not rely on a direct temporal overlap between IOP and nocturnal BP readings. Instead, it is proposed that the observed morning IOP elevation may reflect the downstream effects of nocturnal systemic dysregulation, particularly in nondipper hypertensive patients. In such individuals, impaired autonomic control, vascular stiffness, and endothelial dysfunction—factors associated with the nondipping pattern—are likely to disrupt ocular autoregulation, resulting in elevated IOP during its circadian peak.38,39
While continuous 24-h IOP monitoring would provide valuable complementary data, current clinical practice rarely includes such protocols because of logistical and technical constraints. Although the study is based on a cross-sectional design, a plausible mechanistic link between systemic hemodynamic alterations and ocular pressure regulation is suggested, offering a hypothesis-generating perspective that may inform future longitudinal and mechanistic investigations.
Yasukawa et al. 27 reported in their large-scale study that a 10 mmHg increase in SBP and DBP caused an IOP increase of approximately 0.32 mmHg and 0.41 mmHg, respectively. Consistent with the study by Yasukawa and colleagues, the current research also demonstrated that IOP was higher in the hypertensive group compared to the control group. Furthermore, considering that no statistically significant differences were observed between the dipper and nondipper groups in terms of 24-h mean BP and other confounding factors, the higher IOP observed in the nondipper group compared to the dipper group suggests a novel hypothesis that warrants further investigation in future studies.
Considering the well-established role of nondipping BP patterns in promoting systemic vascular, autonomic, and inflammatory dysfunction, it is plausible that the elevated IOP observed in nondipper hypertensive patients may be partially attributed to these underlying mechanisms. This hypothesis is further supported by evidence linking neutrophil-driven inflammation with both circadian BP dysregulation and increased IOP.
The negative association between neutrophil count and IOP in linear regression analysis presents a compelling contrast to the existing literature on systemic inflammation and ocular pressure. While some studies have reported positive correlations between neutrophilic markers and IOP—such as Ozgonul et al. 40 in glaucoma patients and Lee et al. 41 in metabolic dysfunction—other well-designed investigations have failed to demonstrate any significant relationship. Notably, Xu et al. 42 found no independent association between white blood cell counts and IOP in their large multiethnic cohort, while Karahan et al. 43 observed no meaningful correlation between neutrophil and IOP. Similarly, Ikezaki et al. 44 conducted rigorous adjustments for confounders in a Japanese population and found neutrophil counts bore no association with IOP measurements. This striking inconsistency across studies suggests the relationship between systemic inflammation and ocular pressure may be highly context-dependent, potentially varying by population characteristics, underlying metabolic conditions, or methodological approaches. The current finding of an inverse relationship with IOP in non-dipper hypertensives introduces yet another dimension to this complex interplay, possibly indicating unique inflammatory-hemodynamic adaptations in this specific patient subgroup.
One of the main limitations of the present study is that IOP was measured using an NCT rather than the Goldmann applanation tonometer, which is considered the gold standard for IOP measurement. However, the aforementioned method of measurement is compatible with most of the previous studies in which NCTs were utilized.27,45,46 Furthermore, the inability to measure CCT and the absence of gonioscopic evaluation are other limitations. Additionally, the current study relied on single-time-point IOP measurements taken between 9:00 a.m. and 12:00 p.m., which may not fully capture the diurnal variations in IOP. Also, the analysis does not capture the long-term variability in BP or IOP, nor does it account for the monthly, yearly, or visit-to-visit fluctuations that could provide a more comprehensive understanding of these relationships. As a result, the data may not reflect the true variability of BP or IOP, especially in distinguishing between nondipper and dipper groups.
Another limitation of the study is its cross-sectional design and limited sample size. Hence, future research with larger cohorts is essential to validate and expand upon the present results. The present study has several important strengths. First, it specifically included individuals with newly diagnosed and untreated hypertension, thereby minimizing the potential confounding effects of antihypertensive medications. Second, the use of 24-h ambulatory blood pressure monitoring allowed for accurate classification of circadian blood pressure patterns, particularly dipper and nondipper status. Third, the study provides novel evidence regarding the association between nondipping blood pressure patterns and IOP, contributing to the existing literature on cardiovascular and ocular interactions. Finally, the standardized measurement of IOP during the same time window for all participants increased the internal consistency of the study.
Conclusion
The study reported that IOP is elevated in patients with newly diagnosed essential hypertension compared with healthy normotensive subjects. Furthermore, compared with those of dippers, the nondipping circadian BP pattern results in further increases in IOP in these essential HT patients. However, further research with larger cohorts is needed to validate the current results.
Footnotes
Ethical considerations
This study was approved by the Ethics Committee of Aksaray University (Ethics Code: 2021/17-01, Protocol No: 51-SBKAEK Date: 16.12.2021) on December 16, 2021. This research was conducted ethically in accordance with the World Medical Association Declaration of Helsinki.
Consent to participate
All participants provided written informed consent prior to enrollment in the study.
Author contributions
Conceptualization, Muhammet Salih Ateş and Cihan Büyükavşar; Data curation, Cihan Büyükavşar; Formal analysis, Muhammet Salih Ateş; Investigation, Muhammet Salih Ateş; Methodology, Muhammet Salih Ateş and Cihan Büyükavşar; Project administration, Cihan Büyükavşar; Resources, Muhammet Salih Ateş; Software, Muhammet Salih Ateş; Supervision, Cihan Büyükavşar; Validation, Muhammet Salih Ateş; Visualization, Cihan Büyükavşar; Writing—original draft, Muhammet Salih Ateş and Cihan Büyükavşar; Writing—review & editing, Muhammet Salih Ateş and Cihan Büyükavşar.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.*