
Abstract
Rheumatoid arthritis (RA) is characterized by persistent synovitis. Conventional inflammatory markers such as C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) inadequately reflect synovial inflammation, particularly under interleukin-6 pathway inhibition. Pentraxin 3 (PTX3), an extrahepatic acute-phase protein produced in inflamed tissues, may better reflect local inflammation and angiogenesis in RA joints. We enrolled 80 RA patients and 80 age-sex-matched healthy controls. Clinical data, inflammatory markers, and disease activity scores (DAS28) were collected. Serum PTX3 levels were quantified by ELISA. Musculoskeletal ultrasound assessed bilateral wrists and metacarpophalangeal/proximal interphalangeal joints for synovial hypertrophy, effusion, color Doppler flow, and bone erosion. Eight patients received tocilizumab at baseline and week 12. PTX3 levels were significantly higher in RA patients than in controls. Serum PTX3 concentrations showed a progressive increase from remission to moderate-to-high disease activity groups. PTX3 showed no significant reduction after tocilizumab treatment. PTX3 correlated positively with CRP, ESR, DAS28-CRP, and rheumatoid factor, but not with anti-cyclic citrullinated peptide antibodies. PTX3 levels were elevated in patients with ultrasound-detected synovial blood flow compared to those without. Receiver operating characteristic analysis demonstrated superior diagnostic performance of PTX3 for predicting synovial blood flow compared to CRP and ESR. In multivariable logistic regression, PTX3 was the only significant predictor of synovial blood flow positivity. PTX3 demonstrates superior diagnostic performance over traditional inflammatory markers in detecting synovial vascularity and independently correlates with disease activity. PTX3 may serve as a valuable complementary biomarker for assessing local synovial inflammation and angiogenesis, particularly when conventional markers are inadequate.
Introduction
Rheumatoid arthritis (RA) is a chronic autoimmune disease characterized by persistent synovitis, cartilage and bone destruction, and progressive disability.1,2 Although C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) are widely used to estimate inflammatory activity, 3 approximately one-third of patients have normal levels of CRP and ESR despite active disease. 4 Thus, these systemic markers may not fully capture the synovial inflammatory load, particularly under interleukin-6 (IL-6) pathway inhibition or intercurrent clinical conditions that affect hepatic protein synthesis.5,6 Therefore, biomarkers that accurately reflect local synovial inflammation and angiogenesis are required.
Pentraxin 3 (PTX3) belongs to the long pentraxin family and is an acute-phase reactant with functional parallels to CRP; 7 however, it is produced locally by various cells within inflamed tissues, including endothelial cells, fibroblast-like synoviocytes, macrophages, and plasma cells. 8 Prior studies have suggested that PTX3 may be more sensitive to inflammatory activation and more tightly coupled to local microenvironmental changes;9,10 however, data linking PTX3 to imaging-based synovial vascularity and treatment dynamics remain limited. We aimed to compare serum PTX3 levels between patients with RA and healthy controls (HCs); examine the associations of PTX3 with CRP, ESR, disease activity score in 28 joints (DAS28)-CRP, rheumatoid factor (RF), anti-cyclic citrullinated peptide (anti-CCP), and ultrasound color Doppler flow; and explore PTX3 dynamics in response to IL-6 receptor inhibition with tocilizumab.
Significance Statement
Serum pentraxin 3 (PTX3) was elevated in patients with rheumatoid arthritis and was independently associated with ultrasound-detected synovial blood flow. PTX3 demonstrated better discriminatory performance than C-reactive protein and erythrocyte sedimentation rate in this cohort, suggesting that it may serve as a complementary biomarker of local synovial inflammation and vascular activity, particularly when conventional inflammatory markers do not adequately reflect disease activity.
Materials and methods
Patients
Eighty patients with RA and 80 age- and sex-matched HCs were included in this study. The patients met the 2010 American College of Rheumatology/European League Against Rheumatism classification criteria for RA. 11 The exclusion criteria included other rheumatic diseases, malignancy, and chronic hepatic, renal, or cardiac diseases. The institutional ethics committee approved the study protocol, and written informed consent was obtained from all participants.
Clinical and laboratory data
Clinical and laboratory data for all patients were collected, including demographic information such as sex, age, and disease duration, as well as disease-specific metrics such as the number of swollen and tender joints and pain levels measured using the visual analog scale. Disease activity was evaluated using the DAS28, and inflammatory markers were monitored using the ESR and CRP levels. In addition, titers of RF and anti-CCP antibodies specific to RA were assessed.
Anti-IL-6 receptor monoclonal antibody therapy
Patients with moderate-to-high disease activity (DAS28 > 3.2) despite at least 3 months of treatment with conventional synthetic disease-modifying antirheumatic drugs were evaluated for biological therapy. Eight patients received 8 mg/kg of tocilizumab intravenously at weeks 0, 4, 8, and 12. Serum samples were collected at baseline and week 12.
Detection of PTX3 levels in supernatants
Morning fasting venous blood was collected and centrifuged at 3000 rpm for 15 min. Serum was aliquoted and stored at −80°C until analysis. Serum PTX3 levels were measured using a commercial human PTX3 ELISA kit (Hangzhou Lianke Biology Technology, China) following the manufacturer’s instructions.
Musculoskeletal ultrasound assessment
Musculoskeletal ultrasound was performed on both wrists and the second/third metacarpophalangeal and proximal interphalangeal joints. Synovial hypertrophy, joint effusion, color Doppler flow, and bone erosion were evaluated using a standardized semi-quantitative grading scale (0–3) in accordance with the definitions commonly applied in rheumatologic ultrasound practice. 12 The sonographers were blinded to the laboratory results to minimize assessment bias.
Statistical analysis
Statistical analyses were performed using SPSS version 22.0 (IBM Corp., Armonk, NY, USA). Normality was tested using the Shapiro–Wilk test, and group and paired comparisons were performed using appropriate parametric/nonparametric tests (t/Mann–Whitney; paired t/Wilcoxon), Pearson/Spearman correlations, and multiple linear regression to explore factors associated with PTX3. All tests were two-sided with a significance level of α = 0.05; data are reported as the mean ± SD or median (IQR).
Results
Participant characteristics
Eighty patients with RA and 80 HCs were enrolled in this study. The baseline demographics and clinical characteristics are summarized in Table 1.
Clinical and laboratory data of the enrolled groups.
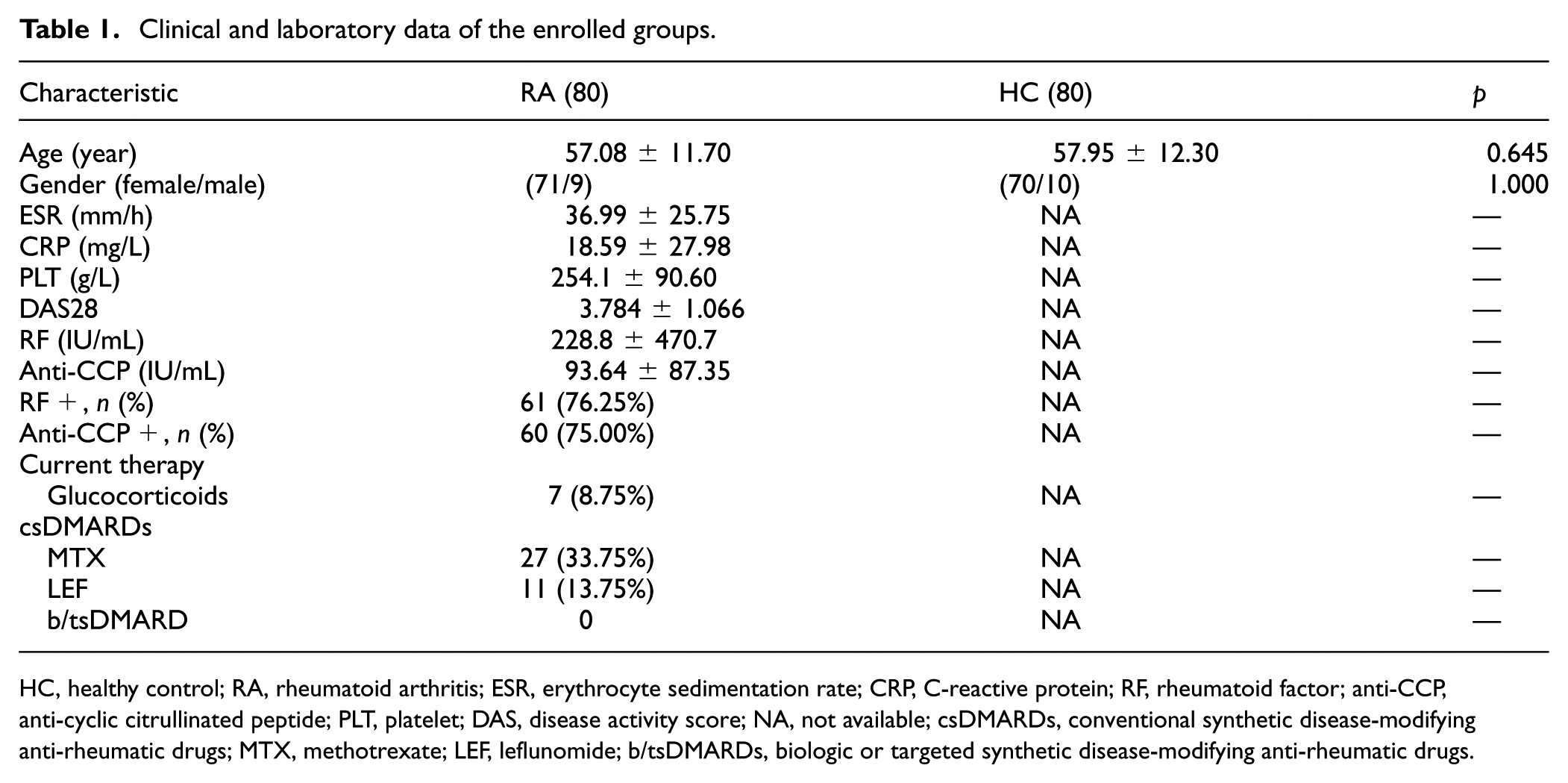
HC, healthy control; RA, rheumatoid arthritis; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; RF, rheumatoid factor; anti-CCP, anti-cyclic citrullinated peptide; PLT, platelet; DAS, disease activity score; NA, not available; csDMARDs, conventional synthetic disease-modifying anti-rheumatic drugs; MTX, methotrexate; LEF, leflunomide; b/tsDMARDs, biologic or targeted synthetic disease-modifying anti-rheumatic drugs.
Increased serum PTX3 in patients with RA and PTX3 dynamics with tocilizumab
Compared to the HCs, the RA group exhibited significantly higher serum PTX3 levels (1259.0 ± 1014.0 pg/mL vs 262.5 ± 131.5 pg/mL, p < 0.0001; Figure 1(a)). Additionally, serum PTX3 levels did not markedly decrease following tocilizumab treatment in the eight patients with RA, with the before and after treatment levels being 1585.0 ± 470.0 pg/mL and 1401.0 ± 307.5 pg/mL (p = 0.4609), respectively (Figure 1(b)).
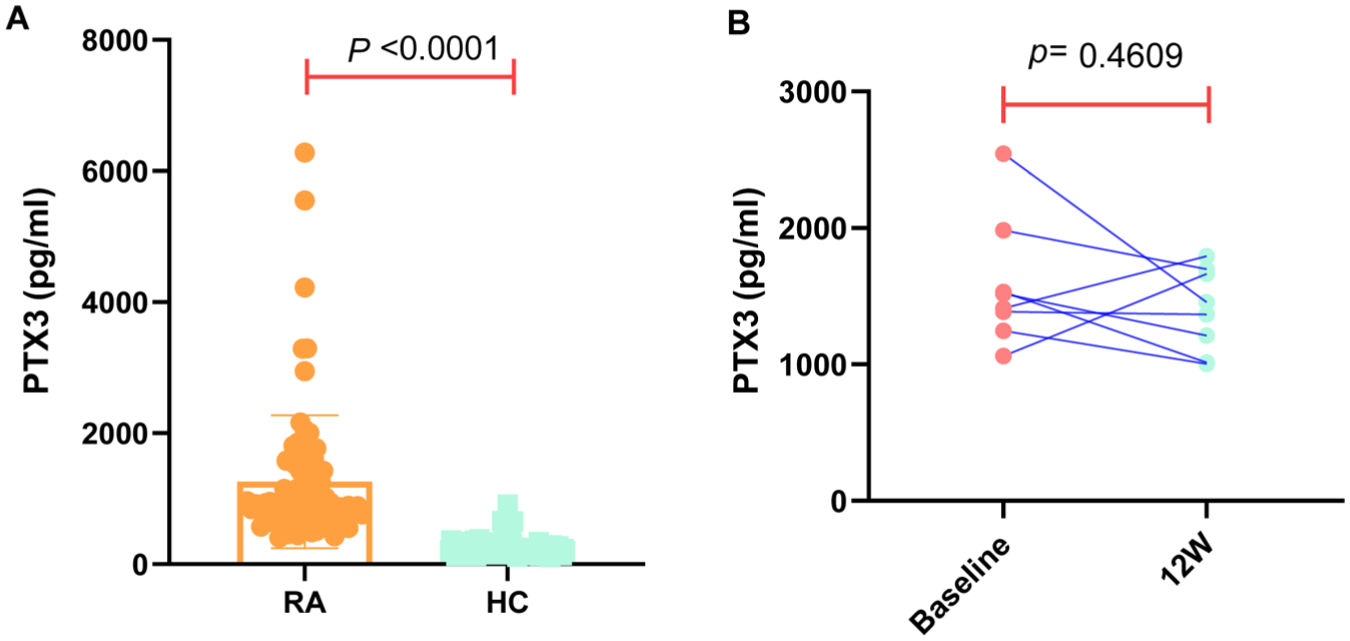
Serum pentraxin 3 (PTX3) levels were elevated in patients with rheumatoid arthritis (RA), and they did not markedly decrease following tocilizumab treatment in the eight patients with RA. (a) PTX3 levels in patients with RA were significantly higher than those in the healthy control group, and (b) Serum PTX3 levels did not markedly decrease following tocilizumab treatment in patients with RA.
Association of serum PTX3 with systemic inflammation and disease activity in patients with RA
The results showed a positive correlation between serum PTX3 levels in patients with RA and key inflammatory markers, including CRP (r = 0.3228, p = 0.0035), ESR (r = 0.3141, p = 0.0046), and DAS28-CRP (r =0.3307, p = 0.0027) as components (Figure 2(a)–(c)). Furthermore, when patients were stratified by disease activity levels, serum PTX3 concentrations showed a progressive increase from remission to moderate-to-high disease activity groups (Figure 2(e)). The median PTX3 levels were 777.11 pg/mL in the remission group (n = 13), 965.17 pg/mL in the low disease activity group (n = 9), and 1089.36 pg/mL in the moderate-to-high disease activity group (n = 58). Significant differences were observed between the remission group and moderate-to-high disease activity group (p = 0.0051), while no statistically significant differences were found between remission and low disease activity groups (p = 0.071) or between low and moderate-to-high disease activity groups (p = 0.307). We also present a multivariable linear regression analysis where PTX3 is the dependent variable, and the predictors include DAS28-CRP, age, gender, RF, and CCP. For each variable, we present the unstandardized coefficient. DAS28-CRP is the only variable significantly associated with PTX3 after adjustment for the other covariates (p = 0.004; Table 2).
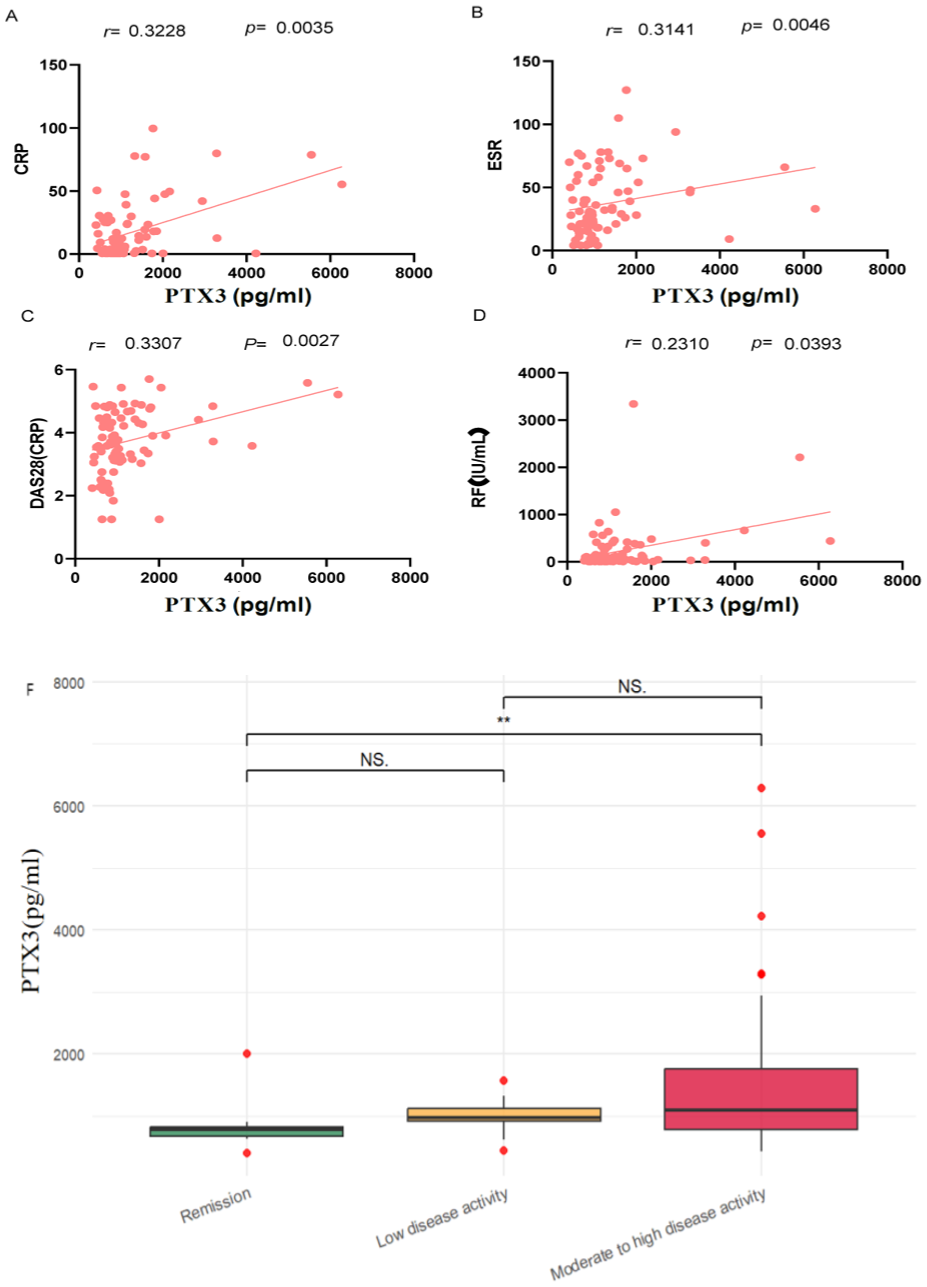
Correlation of serum pentraxin 3 (PTX3) levels with C-reactive protein (CRP) (a), erythrocyte sedimentation rate (ESR) (b), and Disease Activity Score in 28 joints CRP (DAS28-CRP) (c), and rheumatoid factor (RF) (d) in patients with rheumatoid arthritis was evaluated. Comparison of serum PTX3 levels among different disease activity groups (e). Significant positive correlations were found between PTX3 levels and clinical parameters, including CRP (a), ESR (b), DAS28-CRP (c), and RF (d). Significant difference was observed between remission and moderate-to-high disease activity groups (e).
Multivariable linear regression models of PTX3 with clinical variables in patients with RA.
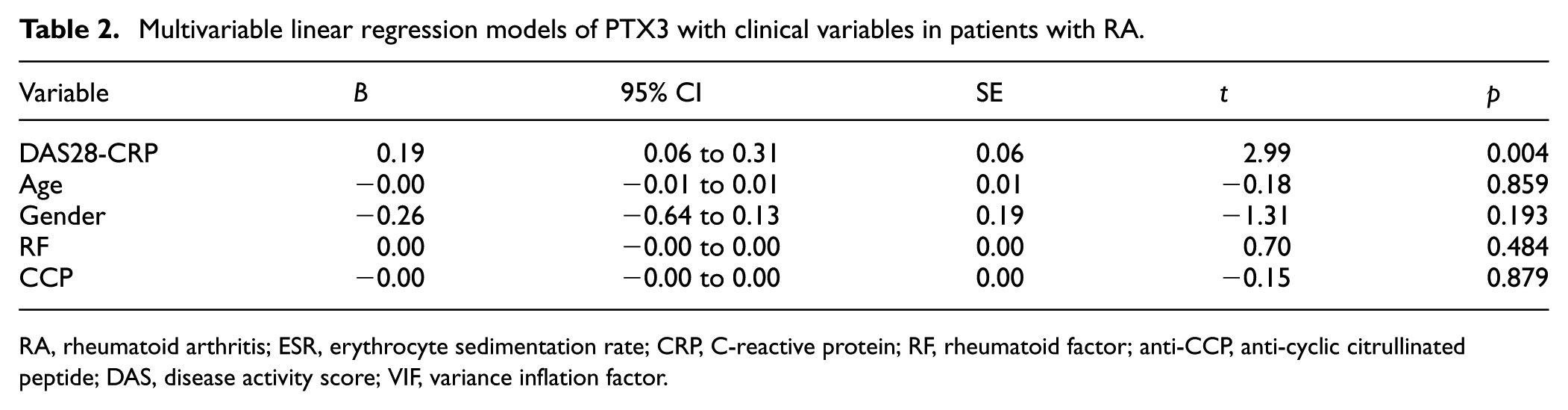
RA, rheumatoid arthritis; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; RF, rheumatoid factor; anti-CCP, anti-cyclic citrullinated peptide; DAS, disease activity score; VIF, variance inflation factor.
Positive correlation between serum PTX3 levels and RF levels
The results revealed a positive correlation between the serum PTX3 and RF levels (r = 0.2310, p = 0.0393; Figure 2(d)). However, no statistically significant differences in PTX3 levels were found among groups that were positive for other autoantibodies, including CCP.
Association between serum PTX3 levels and joint blood flow in patients with RA
Synovial hyperplasia, effusion, synovial blood flow, and bone erosion were assessed in 80 patients with RA who underwent comprehensive joint ultrasonography. PTX3 levels were significantly higher in the group with joint blood flow (44 patients) than in the group without it (36 patients; 1519.0 ± 1202.0 pg/mL vs 941.6 ± 599.2 pg/mL, p = 0.0004; Figure 3(a)). However, no differences in PTX3 levels were observed among patients with synovial hyperplasia, effusion, or bone erosion. The receiver operating characteristic (ROC) curves demonstrate the discriminatory performance of three inflammatory biomarkers—PTX3, CRP, and ESR—in predicting ultrasound synovial blood flow positivity in RA patients. PTX3 showed superior diagnostic performance with an area under the curve (AUC) of 0.7273 (p = 0.0005), indicating good discriminatory ability and statistical significance. In contrast, both CRP and ESR demonstrated poor predictive performance, with AUC values of 0.5464 (p = 0.4772) and 0.5205 (p = 0.7533), respectively, which are close to 0.5 and statistically nonsignificant, suggesting no better than random chance in predicting synovial blood flow positivity. The pairwise comparisons between ROC curves revealed significant differences in predictive performance. PTX3 significantly outperformed both CRP (p = 0.0197) and ESR (p = 0.0073) in discriminating synovial blood flow status. However, no significant difference was observed between CRP and ESR (p = 0.6117), both of which showed similarly poor diagnostic accuracy (Figure 3(b)).
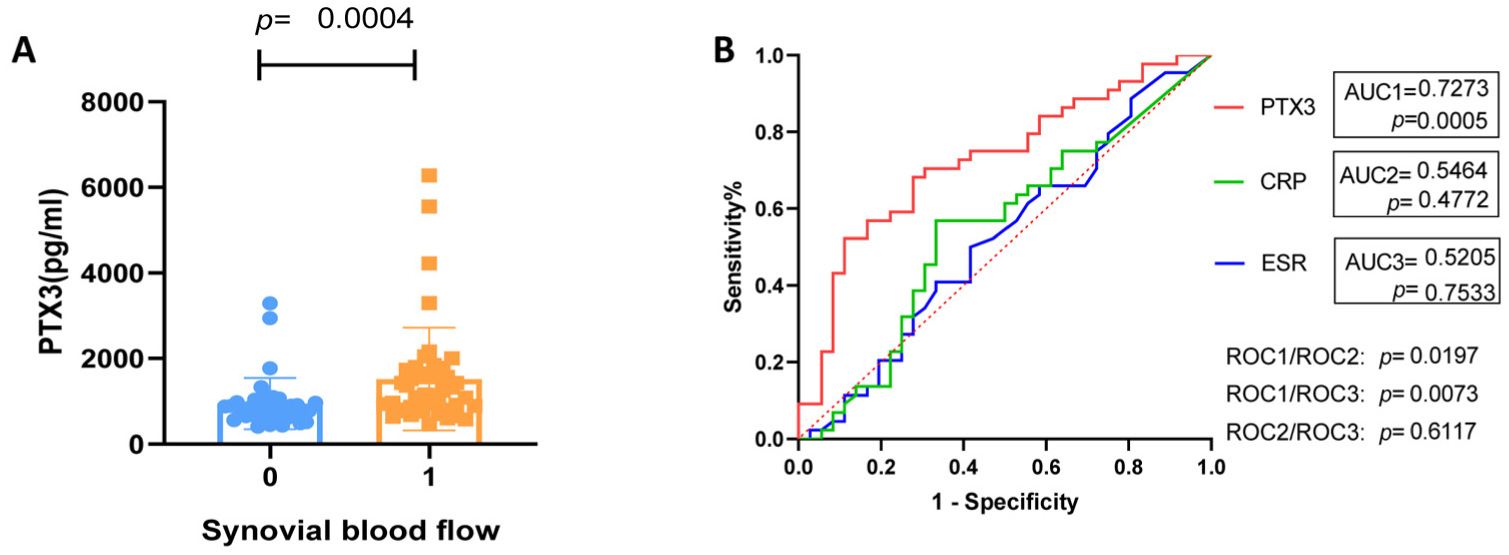
Associations between serum pentraxin 3 (PTX3) levels and joint blood flow in patients were assessed using joint ultrasonography. PTX3 levels were higher in the group with joint blood flow than in the group without joint blood flow (a). PTX3 showed superior diagnostic performance with an area under the curve (AUC) of 0.7273, indicating good discriminatory ability and statistical significance (b).
In the multivariable logistic regression model (Table 3), PTX3 was the only significant predictor of synovial blood flow positivity (OR = 1.0015, p = 0.0086). Traditional inflammatory markers, including CRP (p = 0.1253) and ESR (p = 0.9766), as well as disease activity parameters DAS28-CRP (p = 0.7306), RF (p = 0.3244), and anti-CCP (p = 0.6872), showed no significant associations.
Multivariable logistic regression of ultrasound synovial blood flow positivity in RA.
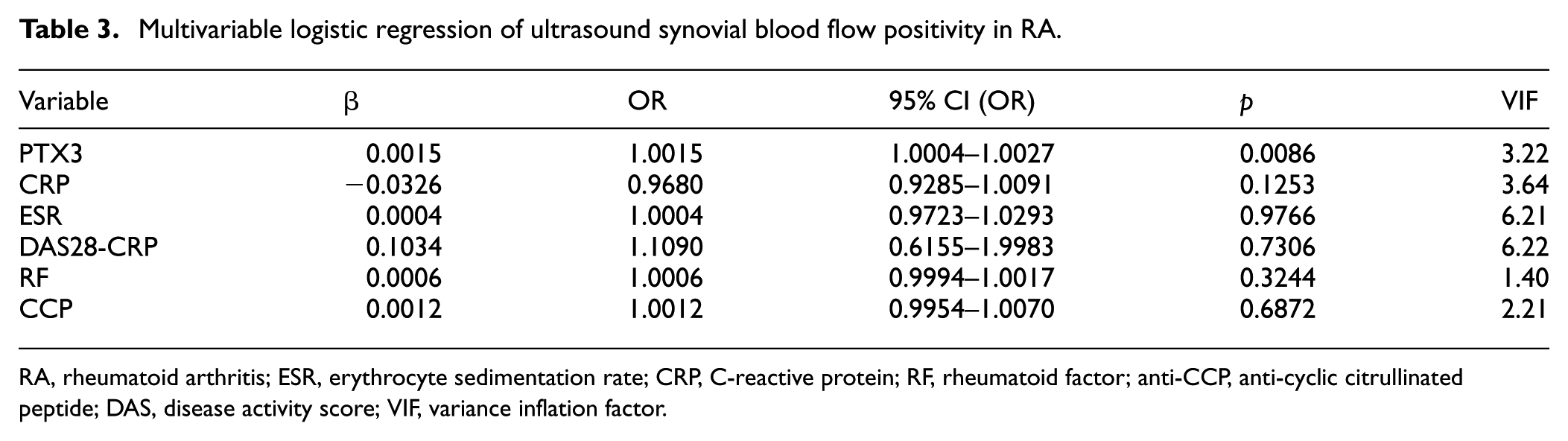
RA, rheumatoid arthritis; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; RF, rheumatoid factor; anti-CCP, anti-cyclic citrullinated peptide; DAS, disease activity score; VIF, variance inflation factor.
Discussion
RA is a chronic inflammatory disease characterized by persistent synovitis. 2 Conventional systemic acute-phase reactants, such as CRP and ESR, are influenced by multiple factors and may not align with the synovial inflammatory burden, particularly under IL-6 pathway inhibition or concurrent clinical conditions. 13 Thus, biomarkers that better capture local synovial inflammation are required. Unlike CRP, which is predominantly synthesized in the liver upon IL-6 stimulation and reflects systemic inflammation, PTX3 is rapidly induced at sites of inflammation by both immune and non-immune cells. 8 PTX3 has been increasingly implicated in rheumatic diseases, including RA, systemic sclerosis, and vasculitis, suggesting its potential utility as a locally informative acute-phase reactant. 14
This study demonstrated that serum PTX3 levels are significantly higher in patients with RA than in HCs and that PTX3 levels correlate with systemic inflammatory markers and disease activity. Notably, in multivariable linear regression analysis, DAS28-CRP emerged as the only independent predictor of PTX3 levels. These findings are consistent with those of previous studies but extend them by demonstrating the independent relationship between disease activity and PTX3. Sharma et al. 15 showed that PTX3 is inducible and highly expressed in the serum and synovial fluid of patients with RA, supporting the role of long-chain pentraxin in inflammatory pathobiology. Luchetti et al. 16 reported that, unlike hepatic acute-phase reactants such as CRP and ESR, PTX3 is extrahepatically synthesized, implying that synovial tissue may be a principal source of RA and may confer greater specificity for local disease processes. Weitoft et al. 17 observed elevated PTX3 concentrations in the serum of patients with RA, although they did not detect any differences in synovial fluid levels.
A pivotal finding of our study is the superior diagnostic performance of PTX3 in detecting synovial vascularity compared to conventional inflammatory markers. PTX3 demonstrated excellent discriminatory ability for ultrasound-detected synovial blood flow with an AUC of 0.7273, significantly outperforming both CRP and ESR. Furthermore, patients with ultrasound-detected joint blood flow had significantly higher PTX3 levels than those without. Critically, in multivariable logistic regression, PTX3 was the only significant predictor of synovial blood flow positivity. This represents a fundamental advance in understanding the clinical utility of PTX3, as it demonstrates not only correlation but also independent predictive value for local synovial inflammation.
The treatment-response analyses in this study further elucidate the biological context. Following IL-6 receptor inhibition, CRP levels declined markedly, consistent with its hepatic, IL-6–driven synthesis, whereas PTX3 showed only modest changes over 12 weeks. This pattern suggests ongoing, non–IL-6–dependent local inflammatory activity and/or tissue-level kinetics that maintain PTX3 production, supporting its role as a marker of local rather than systemic inflammatory processes.
The mechanistic basis for PTX3’s superior performance likely relates to its tissue-specific production by endothelial cells, fibroblast-like synoviocytes, macrophages, and plasma cells within inflamed synovium (Boutet et al., 2021). 18 The closer alignment of PTX3 with ultrasound color Doppler vascularity, compared to traditional markers, supports the interpretation that PTX3 more accurately reflects synovial inflammatory and angiogenic activity. This is concordant with tissue-level data showing PTX3 upregulation linked to immune cell infiltration, ectopic lymphoid structures, and pathways of tissue damage. Our ultrasound findings externally validate these tissue observations using a noninvasive clinical measure, bridging histological evidence and clinically interpretable imaging.
These findings have important clinical implications. The ability of PTX3 to independently predict synovial blood flow when conventional markers fail suggests it could serve as a valuable complementary biomarker, particularly in scenarios where CRP and ESR levels are discordant with clinical suspicion of active synovitis. This may be especially relevant in patients receiving IL-6 pathway inhibition, where CRP may be suppressed despite ongoing local synovial inflammation. The superior diagnostic performance of PTX3 positions it as a potentially transformative biomarker for monitoring disease activity and treatment response in RA.
The limitations of this study include the single-center design and modest sample size; the use of HCs without the inclusion of other inflammatory arthritis, which limits the assessment of disease specificity; and the lack of synovial fluid or tissue measurements in parallel with serum assays. The tocilizumab subgroup was small, which constrained the inferences regarding treatment responsiveness. Future studies should include larger multicenter cohorts, disease controls, integrated analyses of serum, synovial fluid, and tissue, and longitudinal imaging to determine the specificity, responsiveness, and prognostic value of PTX3.
In conclusion, PTX3 appears to play a meaningful role in RA immunopathology and shows promise as a complementary acute-phase biomarker for assessing disease activity, particularly when systemic markers are discordant with clinical or imaging findings. Prospective studies are warranted to validate its clinical utility and to clarify its mechanistic links to synovial inflammation and angiogenesis.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from the Jinhua Municipal Central Hospital project (JY2023-2-12, JY2019-1-05); 2023 Jiaxing Key Disciplines of Medicine, Rheumatology and Autoimmunology (Supporting Subject) 2023-ZC-016.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.