
Abstract
This study aimed to compare the effectiveness of augmented reality (AR)-assisted teaching versus traditional methods in enhancing clinical core competencies among postgraduate medical students. Fifty postgraduate medical students were randomly assigned to either an experimental group (AR-assisted teaching, n = 25) or a control group (traditional teaching, n = 25). Following an identical instructional curriculum, participants underwent objective theoretical and case analysis assessments, completed self-evaluation surveys, and responded to standardized teaching satisfaction questionnaires. Competency evaluations were based on the six Accreditation Council for Graduate Medical Education (ACGME) core competencies: patient care, medical knowledge, system-based practice, practice-based learning and improvement, professionalism, and interpersonal and communication skills. Students in the experimental group outperformed the control group in theoretical knowledge and case analysis (p < 0.05). They also reported significantly greater improvements in self-directed learning ability, learning efficiency, clinical reasoning, and concentration. The experimental group showed higher satisfaction across teaching dimensions, including spatial visualization, interactivity, curriculum design, and perceived learning outcomes. Additionally, scores across all six ACGME core competencies were significantly higher in the experimental group compared to the control group (p < 0.05). AR-assisted teaching offers significant advantages over traditional methods in medical education, leading to enhanced knowledge acquisition, clinical reasoning, learner engagement, and competency development, thereby providing a promising approach for advancing postgraduate clinical training.
Keywords
Introduction
China is working to reform medical education to mitigate the shortage of doctors. 1 Postgraduate medical students are the mainstay of future medical research, and clinical research is one of the most important components of medical research. In recent years, the Chinese government has increased its efforts to train graduate students. As a result, the quality of postgraduate training has received widespread attention. 2 With the continuous progress of medical technology, the requirements for the clinical core competence of postgraduate medical students are increasing, and how to effectively cultivate and improve the clinical core competence of postgraduate medical students has become an urgent problem for medical education. Nevertheless, training programs face the dilemma of trying to supply novel skills, knowledge, and practice models while connecting with often-inefficient models of health care delivery and apprenticeship model of training. 3 As a result, new teaching methods are born.
Augmented reality (AR) is known as a technology that overlays a computer-created image onto the real world that the user sees to provide a composite view. 4 AR is broadly applied in aviation to assist pilots with takeoff, landing, and maneuvers, and it has also been utilized in the field of surgery. 5 As previously reported, AR with 3D-integrated intraoperative imaging is reliable in implementing minimally invasive procedures for a wide range of neurosurgical diseases, with superior accuracy in hardware placement versus free-hand techniques.6,7 Besides, AR has novel clinical applications, for example, its 3D volumetric reconstruction is essential for co-registering radiology, histopathology, and gross anatomy to support radiotherapy planning in cancer patients. 8 In addition, AR is a valid tool for implementing surgical procedures that require low-performance surgical dexterity, and it remains a science largely determined by ergonomics and stereotactic registration. 9 Therefore, in our article, we aimed to make a comparative analysis of the effects of traditional teaching methods and AR technology on improving postgraduate medical students’ clinical core competencies. After completing the lectures, objective assessment tests, subjective self-evaluations, teaching questionnaires, and six Accreditation Council for Graduate Medical Education (ACGME) core competencies were compared in two groups of students.
Traditional teaching methods are commonly used in postgraduate medical education but may have limitations in enhancing clinical core competencies effectively.
Augmented reality (AR) technology has shown potential in various educational fields for improving learning experiences.
Previous studies have explored the use of technology in medical education, but specific comparisons between AR-assisted teaching and traditional methods for postgraduate clinical training are limited.
Students in the AR-assisted teaching group outperformed those in the traditional teaching group in theoretical knowledge and case analysis (p < 0.05).
The AR-assisted teaching group reported significantly greater improvements in self-directed learning ability, learning efficiency, clinical reasoning, and concentration.
Scores across all six ACGME core competencies were higher in the AR-assisted teaching group compared to the traditional teaching group (p < 0.05).
AR-assisted teaching could become a mainstream method in postgraduate medical education, improving the quality of clinical training.
Enhanced clinical reasoning and core competencies among medical students may lead to better patient care and outcomes in clinical practice.
The adoption of AR technology in medical education could drive innovation and advancements in teaching methodologies across the healthcare sector.
Materials and methods
Ethics statement
This study was ratified by the Ethics Committee of Second Affiliated Hospital of Nanchang University.
Study subjects
Fifty registered postgraduate medical students in Second Affiliated Hospital of Nanchang University were selected for the study and randomly divided into 25 members of the experimental group and 25 members of the control group by using the random number table method. The data collected mainly included gender and age. Among them, 22 members were male, and 28 members were female. All the study subjects gave informed consent for this study.
Random grouping
In this study, the random number table method was employed for random grouping. First, all the medical postgraduates included in the study were sequentially numbered from 1 to 50. SPSS 26.0 (IBM Corporation, Armonk, NY, USA) was used to generate 50 random numbers (each random number corresponding to a number). The random numbers were then sorted in ascending order. It was stipulated that the research subjects corresponding to the first 25 random numbers were assigned to the control group, and the latter 25 to the experimental group. The generation of random numbers, the recruitment of research subjects, and the grouping were all carried out by a third party not involved in this study.
Experimental methods
Teaching was roughly divided into theoretical teaching and clinical skills teaching.
Theoretical teaching aimed to help trainees build a systematic medical knowledge (MK) framework and lay a foundation for clinical practice. In this study, the core content of theoretical teaching was essentially consistent between the control group and the experimental group, mainly including: (1) Core themes and concepts. Basic MK: Human anatomy (e.g., the three-dimensional anatomical structure of the thyroid gland and major cervical blood vessels and nerves), physiology (e.g., endocrine regulatory mechanisms), pathology (e.g., pathological classification and characteristics of thyroid diseases), etc.; Clinical MK: for example, diagnostic criteria, differential diagnosis, and treatment principles for thyroid diseases (hyperthyroidism, hypothyroidism, thyroid nodules, etc.); principles and clinical applications of nuclear medicine examinations (e.g., thyroid imaging); clinical pathways and guidelines for endocrine and metabolic diseases; Medical imaging: interpretation methods for CT, MRI, and other imaging data, with emphasis on identifying normal anatomical structures and pathological features (e.g., size, margins, and blood flow signals of thyroid nodules). (2) Competency requirements. Trainees were required to develop competencies including knowledge integration (combining basic and clinical MK to understand the correlation between disease mechanisms and clinical manifestations), theoretical application (applying learned theories to analyze typical cases, such as deriving a diagnosis based on patient symptoms and laboratory results), and information acquisition (updating MK through literature retrieval and guideline consultation, fostering self-directed learning awareness).
Furthermore, clinical skills teaching in this study focused on cultivating practical operational abilities and clinical thinking. Both groups received identical skills training, albeit in different teaching formats. The skills mainly included: (1) Basic clinical skills. History taking: structured interview techniques (e.g., collecting symptom evolution, family history, and medication history from thyroid disease patients); Physical examination: for example, thyroid palpation (technique, location, and goiter grading), cervical lymph node examination, and vital sign measurement; Auxiliary examination procedures: standardization of thyroid function blood sampling, and patient positioning and cooperation points for ultrasound examination. (2) Clinical operational skills. Simulated surgical operations: simulation of key steps in thyroid surgery (e.g., incision design, tissue dissection, hemostasis). The experimental group trained using AR-based 3D virtual surgical scenarios, while the control group used traditional specimens/models. Trainees were also assessed on suturing techniques, aseptic operation standards, and correct use of surgical instruments (e.g., gripping and operation of scalpels and hemostatic forceps). (3) Clinical thinking and decision-making. Case analysis and management: developing diagnostic workflows, treatment plans (medication/surgery selection), and post-operative management plans for simulated cases (e.g., thyroid nodules with hyperthyroidism).
In the experimental group, for theoretical teaching, teachers used AR fusion projection technology on the basis of traditional multimedia. Normal anatomical structures as well as clinical data such as CT and MRI collected by clinicians were presented to students as 3D images through the integration of multiple technologies including computer vision, graphics processing, display technology, and input systems using AR technology. When students were learning, based on the virtual-real integration technology of the platform, they could see the operation model in front of them and the virtual image combined with it. The operation image could be kept in front of the students’ eyes through a reality device, helping them better understand complex anatomical structures. For example: in anatomy teaching, students could view a 3D thyroid model floating above the podium through AR devices, clearly displaying the three-dimensional spatial relationships between the gland and the trachea, esophagus, and recurrent laryngeal nerve; in pathology teaching, AR could magnify microscopic pathological structures (e.g., thyroid follicular hyperplasia) into macroscopic dynamic models, intuitively presenting the disease progression. In terms of interaction, students could control the virtual models through gestures or touch operations, achieving 360° rotation to observe anatomical structures from any angle, and could also progressively peel away skin, muscle, and fascia to expose deep neurovascular structures. In terms of clinical skills teaching, teachers in the experimental group used models to present theoretical teaching content in a three-dimensional way, simulate the process of medical skills operation, perform operational demonstrations of skills, and achieve visual interactive three-dimensional scenes. The teacher instructed students to use the AR device and the AI teaching system. According to the changes in the scene, teachers provided real-time guidance and explanation of the operation of students, and students, according to the prompts of the teaching system, synchronized the real operation on the model and practiced in an immersive way, in order to strengthen their diagnostic thinking and clinical operation skills. For example, in thyroid puncture training, AR projected the nodule location, vascular distribution, and puncture path onto the simulated patient’s neck; in surgical teaching, AR combined virtual surgical instruments, tissue tension, and bleeding effects with the physical surgical table to recreate tactile sensations. In terms of interaction, instructors could simultaneously observe student operations through the AR platform, annotate incorrect steps in the virtual scenario, and provide real-time explanations. In the control group, only the traditional multimedia teaching mode was applied to the theoretical teaching, and the clinical skills were taught using traditional specimens and models (see Figure 1 for details).

Scene diagram of medical teaching using augmented reality fusion projection technology. (a) AR medical teaching laboratory; (b) AR simulation teaching platform; (c) Multi-scene integrated AR simulation ward; and (d) AR operation simulation training equipment.
Content of core competency evaluations
The ACGME has identified six core competencies that physicians must possess, including Patient Care (PC), MK, Systems-Based Practice (SBP), Practice-Based Learning (PBL), Professionalism (PROF), and Interpersonal and Communication Skills (ICS). These six core competencies were Level 1 competency indicators. 10
Methodology for evaluating core competencies
An internet-based tool was utilized to design a web-based rating scale for postgraduate medical students of our hospital, with each competency indicator scoring 100 points. At the end of the study, the instructor would score according to his/her learning and working performance. In order to ensure the validity of the data collection, all instructors involved in scoring had undergone unified training to ensure the evaluation was objective and true. Finally, the data would be collected and organized by the management department of the residency training, and analyzed and evaluated by statistical software.
Observation indicators
Upon completion of the course, the objective assessment test and subjective assessment were conducted for all students. The objective assessment consisted of a theoretical knowledge assessment score and a case analysis score out of 100 points each. The examination papers were all set by the supervising teachers. Subjective assessment was conducted through questionnaires, including self-assessment of learning ability and teaching questionnaires. The questionnaires were all self-made by the supervising teachers in our hospital.
The self-assessment of learning ability included four items: self-learning ability, learning efficiency, clinical thinking ability, and learning concentration, with each item for 25 points, totaling 100 points. The Cronbach’s α coefficient of the scale was 0.85, and the content validity index (CVI) was 0.90, indicating good reliability and validity.
The teaching questionnaire included five items: three-dimensional spatial sense, interactivity, curriculum design, knowledge acquisition, and teaching satisfaction, each with 20 points, totaling 100 points. The Cronbach’s α coefficient of the scale was 0.89, and the CVI was 0.95, indicating good reliability and validity.
Six core competencies were examined in six content areas, including patient consultation, medical knowledge, large SBP, PBL and improvement, PROF, and ICSs. 11
Statistical analysis
All data were processed using SPSS 26.0 statistical software (IBM Corporation, Armonk, NY, USA). The measurement data were expressed in the form of mean ± standard deviation, and comparisons between the two groups were made using the independent samples t-test. Categorical data were expressed as n, which were analyzed adopting the χ2 or Fisher’s exact test. p < 0.05 indicated that the difference was statistically significant.
Results
General data
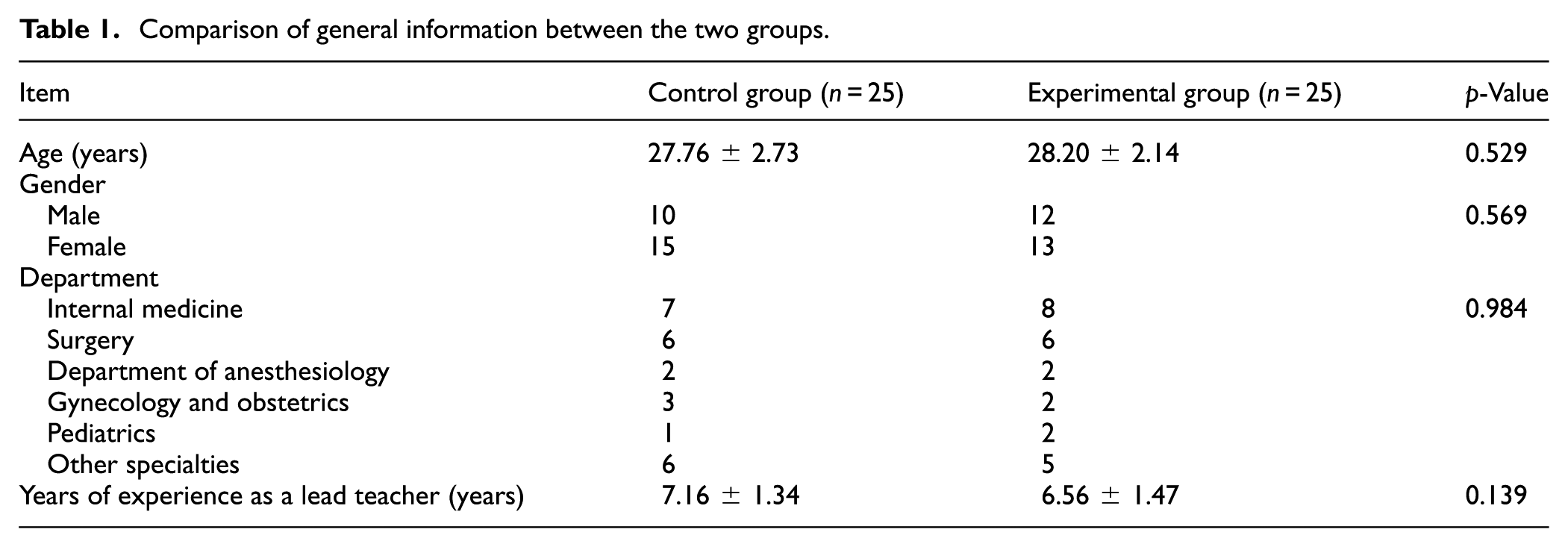
In the experimental group, there were 12 males and 13 females, with an average age of 28.20 ± 2.14 years, and in the control group, there were 10 males and 15 females, with an average age of 27.76 ± 2.73 years. The differences in the general data of patients in the two groups were not statistically significant (p > 0.05; Table 1) and were comparable.
Comparison of general information between the two groups.
Objective assessment scores
In the objective assessment, the theoretical knowledge and case analysis scores in the experimental group were higher in comparison to those of the control group (p < 0.05; Table 2).
Comparison of objective assessment scores between the two groups (point).

Self-assessment of learning ability
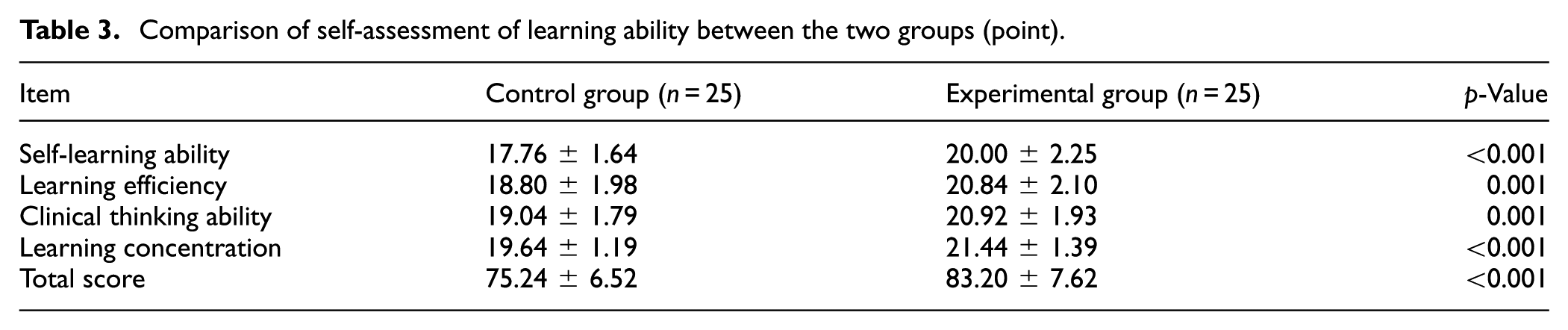
In the subjective assessment of learning ability, the experimental group scored higher than the control group in the four areas of self-learning ability, learning efficiency, clinical thinking ability, and learning concentration, and the experimental group’s overall score was also higher than that of the control group (p < 0.05; Table 3).
Comparison of self-assessment of learning ability between the two groups (point).
Teaching questionnaires
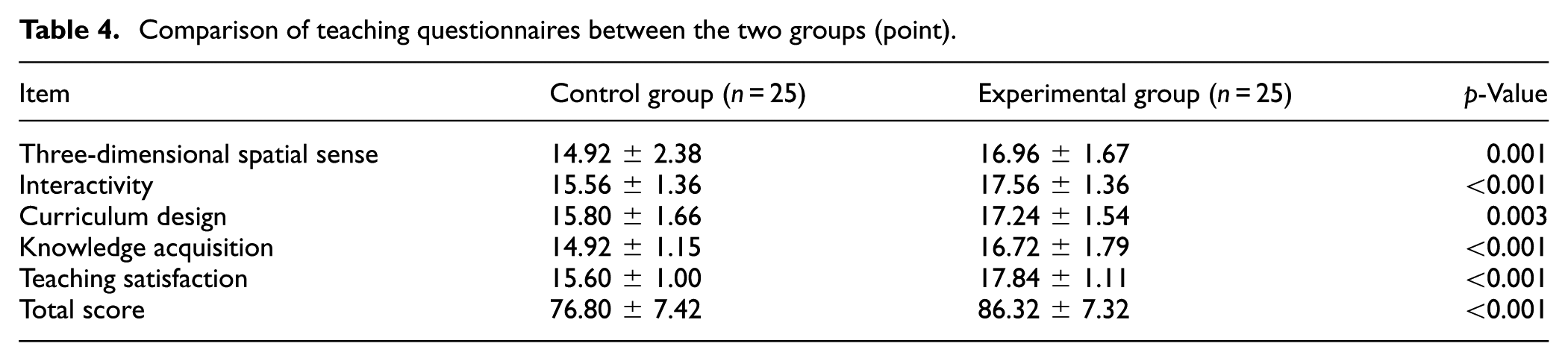
The experimental group scored higher overall on teaching than the control group, and also scored higher on five aspects: three-dimensional spatial sense, interactivity, curriculum design, knowledge acquisition, and teaching satisfaction compared to the control group (p < 0.05; Table 4).
Comparison of teaching questionnaires between the two groups (point).
Core competency scores
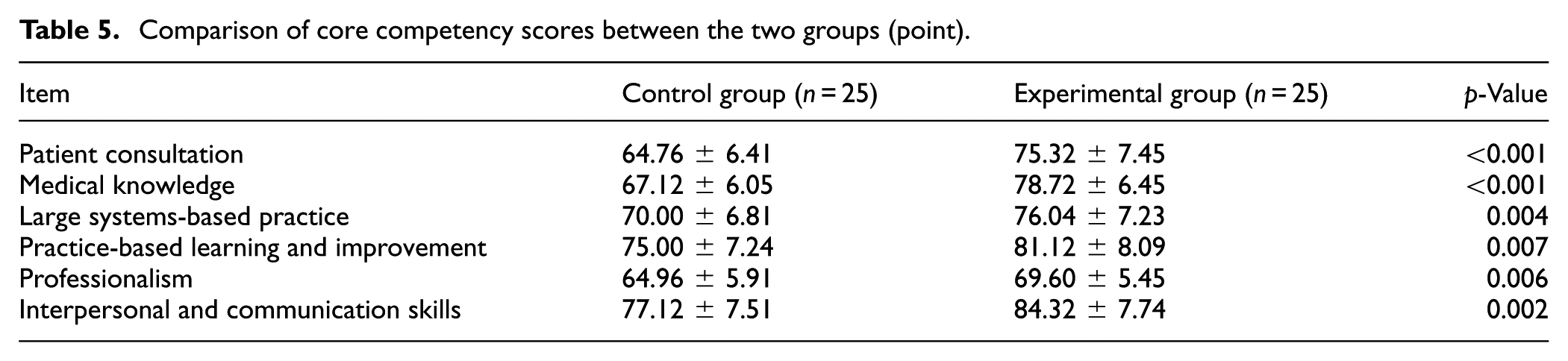
The experimental group scored higher than the control group on patient consultation, medical knowledge, large system-based practice, PBL and improvement, PROF, and ICSs (p < 0.05; Table 5).
Comparison of core competency scores between the two groups (point).
Discussion
The basic medical and health personnel team construction lags behind in China, and the insufficient number of qualified general practitioners limits the improvement of basic medical and health services. 12 As the backbone of the future medical field, postgraduate medical students’ clinical core competence is directly related to medical quality and patient safety. Therefore, it is particularly important to effectively cultivate and enhance the clinical core competencies of medical graduate students. In this article, we purposed to make a comparative analysis of the effects of traditional teaching methods and AR technology on improving postgraduate medical students’ clinical core competencies.
Medical students need to work in teaching hospitals to gain clinical experience. However, the constant evolution of healthcare has also changed the way students are educated. 13 Currently, lecture-based learning is commonly used in medical education, where the teacher is the main body and the content is lecture-centered. This approach often involves indoctrination-style teaching in large classes, which can be dull and lacks innovation. 14 AR technology as a combination of digital content and the real environment of interactive visualization technology, can simultaneously focus on the virtual world and the real world and real-time interaction, which through the computer-generated virtual images and through the display will be superimposed on the image of the reality of the scene, can be 360° to observe the three-dimensional structure of the virtual things, to enhance the observer’s real feelings. AR technology has attracted attention in the medical field because of its advantages such as combining reality and reality, real-time interaction, and the ability to add virtual things to the real environment.15,16 In this research, postgraduate medical students were randomized into the experimental group (AR technology) and the control group (traditional teaching) to compare the differences in the effectiveness of teaching and learning.
In our study, postgraduate medical students in both groups were examined by objective assessment tests, subjective self-evaluation and questionnaires, and six core competency content examinations in six areas, including patient consultation, medical knowledge, large SBP, PBL and improvement, PROF, and ICSs. The corresponding findings demonstrated that the theoretical knowledge and case analysis scores were higher, the scores and overall scores in the four areas of self-learning ability, learning efficiency, clinical thinking ability, and learning concentration were higher, the overall ratings to teaching, with all five aspects of three-dimensional spatial sense, interactivity, curriculum design, knowledge acquisition, and teaching satisfaction were rated higher, as well as the six core competency content scores of patient consultation, medical knowledge, large system-based practice, PBL and improvement, PROF, and ICSs, were higher in the experimental group versus the control group. These confirm the feasibility and superiority of AR technology applications in teaching and learning activities. With the assistance of AR technology, the clinical thinking and self-learning abilities of the students can be improved, and the students can closely follow the teaching ideas and teaching rhythm in the teaching activities, and it is easier for them to summarize, digest and absorb the knowledge after the class, and at the same time, the interest in learning has been increased, and the students are mobilized to mobilize their subjective initiative, attracting them to learn actively, and the learning efficiency and concentration degree of students have been improved. Similar to our finding, an article has revealed that the AR field provides opportunities for educators in the medical education field to create rich and engaging courses that supply students opportunities for learning and experiencing the learning content/material. 17 Another study has confirmed that the holistic AR system is useful, has promising developmental potential, and has broad potential applications in educational and clinical settings. 18
Based on the findings of this study, compared with traditional teaching methods, AR technology enhances the educational experience in the following aspects. First, regarding spatial comprehension, traditional teaching relies on static images, requiring students to mentally construct three-dimensional structures, which is prone to causing cognitive confusion. AR intuitively presents spatial hierarchies through dynamic 3D models, making abstract knowledge concrete. Existing studies have confirmed that AR improves students’ spatial orientation ability for complex anatomical structures.19,20 Second, regarding learning engagement, traditional teaching is predominantly lecture-based, with students passively memorizing content and lacking personalized feedback. AR enables students to actively manipulate virtual models, achieving “learning by doing.” Research has shown that both engagement and satisfaction in the AR group were higher than those in the traditional group. 21 Third, regarding the integration of theory and clinical practice, traditional teaching often leads to a disconnect between knowledge and skills, resulting in a longer mastery cycle. AR directly translates abstract theories into actionable clinical scenarios, thereby accelerating the process of skill proficiency. The systematic review by Abu Halimah et al. 22 reported that AR can improve surgical technical performance by 35%, operational accuracy by 29%, and procedural knowledge by 32% among medical students. Furthermore, the meta-analysis by Xiong et al. 23 confirmed that AR enhances the effectiveness of fundamental laparoscopic skills training, with global operative assessment of laparoscopic skills (GOALS) and objective structured assessment of technical skills (OSATS) scores both superior to traditional methods, while also reducing learners’ subjective workload. In summary, AR provides a more effective pathway than traditional teaching for medical education by enhancing spatial cognition, stimulating active learning, and bridging the gap between theory and practice.
This study has the following limitations. Firstly, it is a single-center, small-sample trial, and no prior sample size calculation was conducted, which may lead to insufficient statistical power and affect the generalizability of the results. Secondly, the study only evaluated short-term teaching effects, and the sustained impact of AR teaching remains unclear. Thirdly, the implementation of AR technology relies on specific hardware devices and software systems, and the compatibility and generalizability among different devices require validation. Whether the findings of this study are applicable to medical institutions with limited resources still needs further exploration. In the future, multi-center, large-sample, long-term follow-up randomized controlled trials are required to further verify the true effects of AR-assisted teaching in cultivating the clinical core competencies of medical postgraduates.
In summary, this research underlines that reaching AR technology can deepen students’ understanding of knowledge, improve theoretical and skills assessment results, increase learning interest and thinking ability, and gain higher teaching satisfaction, which greatly improves the quality of teaching and clinical core competence. This article highlights that the AR-based teaching models could serve as effective traditional methods for improving postgraduate medical students’ clinical core competencies. Optimizing the use and continued use of digital learning tools could potentially reform the medical education sector.
Footnotes
Ethical considerations
This study was ratified by the Ethics Committee of Second Affiliated Hospital of Nanchang University.
Consent to participate
All the study subjects gave informed consent for this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Science and Technology Plan of Jiangxi Provincial Health Commission (Grant Number 202310493), the Jiangxi Provincial Natural Science Foundation (20232BAB206130, 20252BAC250083) and Nanchang University's University-Wide Research Project on Educational Reform in Graduate Education (JXYJG-2025-061).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.