
Abstract
Post-traumatic stress disorder (PTSD) is associated with increased cardiovascular risk, in part through effects on traditional risk factors such as hypertension. People with chronic kidney disease (CKD) have elevated cardiovascular risk and a unique cardiovascular risk factor profile compared to the general population. We assessed associations of cardiovascular risk factors with PTSD among men and women with CKD. In this cross-sectional study, we identified adults with incident non-dialysis CKD stages 3–5 from 2009 to 2020 in the Veterans Affairs healthcare system. Prevalent PTSD was defined by the use of at least two PTSD diagnosis codes within 12 months prior to incident CKD. Of 1,443,878 Veterans in the cohort, PTSD was prevalent in 18.5% of women and 9.6% of men, p < 0.0001. In multivariable models, younger age, Black race, hypertension, depression, anxiety, alcohol, and/or substance use disorder, the use of antidepressant medications other than selective serotonin reuptake inhibitors (SSRIs), and higher estimated glomerular filtration rate were associated with increased odds of PTSD in both men and women, with significant interactions by sex for each of these (interaction p < 0.001 for each), except for anxiety (interaction p = 0.11). SSRI antidepressant use was associated with PTSD among men but not women. PTSD was differentially associated with cardiovascular risk factors among men and women with CKD. Further studies of the mechanisms of cardiovascular risk in people with CKD should stratify by sex.
Keywords
Introduction
People with chronic kidney disease (CKD) have disproportionately high rates of psychiatric disorders.1–4 The most extensively studied among them is depression, which is prevalent in 21% of people with CKD and is associated with adverse cardiovascular and kidney outcomes.4–9 This may contribute to the excessively high cardiovascular risk in people with CKD beyond what can be explained by traditional risk factors such as diabetes mellitus, hypertension, and dyslipidemia. 10
Other forms of psychological stress also impact cardiovascular and kidney health.11,12 Post-traumatic stress disorder (PTSD) is associated with an increased risk of cardiovascular disease and incident CKD in the general population, thought to be at least in part related to altered circulating catecholamines, sympathetic nervous system function, and inflammatory pathways contributing to traditional risk factors such as hypertension.12–22 Importantly, there are differences between men and women with PTSD in autonomic activity and inflammation that may affect the associations of PTSD with clinical characteristics and cardiovascular risk factors. 23
People with CKD have a unique cardiovascular risk profile compared to the general population, as well as elevated sympathetic nervous system activity and inflammation that may affect the relationships between PTSD and cardiovascular risk.24–27 However, associations of PTSD with cardiovascular risk factors have not been assessed among men and women with CKD. We therefore hypothesized that PTSD is associated with cardiovascular risk factors among people with CKD and that these associations differ between men and women.
Significance Statement
PTSD is linked to high cardiovascular risk, but associations with cardiovascular risk factors in people with CKD has not been well characterized.
In this large national CKD cohort, PTSD showed distinct, sex-specific associations with multiple cardiovascular risk factors.
These findings suggest that the relationships between PTSD and cardiovascular risk may differ by sex.
Materials and methods
Study design and data source
In this cross-sectional study, we used real-world data about U.S. Veterans who received care in 172 Veterans Affairs (VAs) Medical Centers and 1321 VA outpatient clinics between January 1, 2009 and December 31, 2020. Electronic health record data from routine clinical care were obtained through the VA Corporate Data Warehouse (CDW), accessed through the VA Informatics and Computing Infrastructure, including demographic, clinical, laboratory, and pharmacy data. This study was approved by the Institutional Review Boards at Baylor College of Medicine and the Michael E. DeBakey VA Medical Center.
Participants
This retrospective cross-sectional study included individuals with incident CKD stages 3–5. CKD was defined as two estimated glomerular filtration rate (eGFR) measurements calculated using the creatinine-based race-free CKD Epidemiology Collaboration (CKD EPI) equation 28 <60 mL/min/1.73 m2 collected ≥90 days apart. 29 The index date for the analysis was established as the date of the second qualifying eGFR that defined the onset of CKD. We excluded individuals with kidney failure on chronic dialysis or with a kidney transplant on or before the index date. We further restricted the sample to those with at least one primary care visit or filled prescription within 1 year prior to the index date to identify active users of the VA system.
Exposure variables
Baseline demographic characteristics, comorbid health conditions, active medications, and laboratory values were ascertained within 12 months prior to the index date. Comorbidities were identified using International Classification of Diseases, Clinical Modification, Ninth and Tenth revisions (ICD-9-CM and ICD-10-CM, respectively) codes and Current Procedural Terminology codes. Baseline medication prescription data were obtained from outpatient pharmacy fill tables. Outpatient laboratory values were obtained through laboratory tables in the CDW.
Outcome variable
The outcome of interest was a prevalent diagnosis of PTSD at the index date. PTSD was defined by the use of ICD-9-CM code 309.81 or ICD-10-CM codes F43.10 or F43.12 at two or more clinical encounters in the 12 months prior to the index date.
Statistical analysis
Baseline characteristics of people with and without PTSD were compared using standardized mean differences, with a value of <0.1 considered to represent balance between groups. Multivariable logistic regression using PTSD as the dependent variable identified factors associated with PTSD. Multiplicative interaction terms assessed if sex modified the relationship between PTSD and clinical factors, with p < 0.01 used as the level of significance. Analyses were conducted using Stata 18.0 (College Station, TX, USA).
Results
Baseline characteristics
We identified 2,024,099 individuals with non-dialysis CKD stages 3–5. Of those, 580,221 were considered non-active users of the VA system and were excluded. Among the 1,443,878 Veterans included in the analysis, PTSD was prevalent in 143,473 (9.9%). The prevalence of PTSD was 18.5% among women and 9.6% among men, p < 0.0001. Compared to individuals without PTSD, those with PTSD were generally younger and more likely to be women and Black (Table 1). Higher eGFR and higher rates of hypertension, depression, anxiety, alcohol, and/or substance use disorder, selective serotonin reuptake inhibitor (SSRI) antidepressant use, and non-SSRI antidepressant use were observed among those with PTSD.
Baseline characteristics of the cohort.
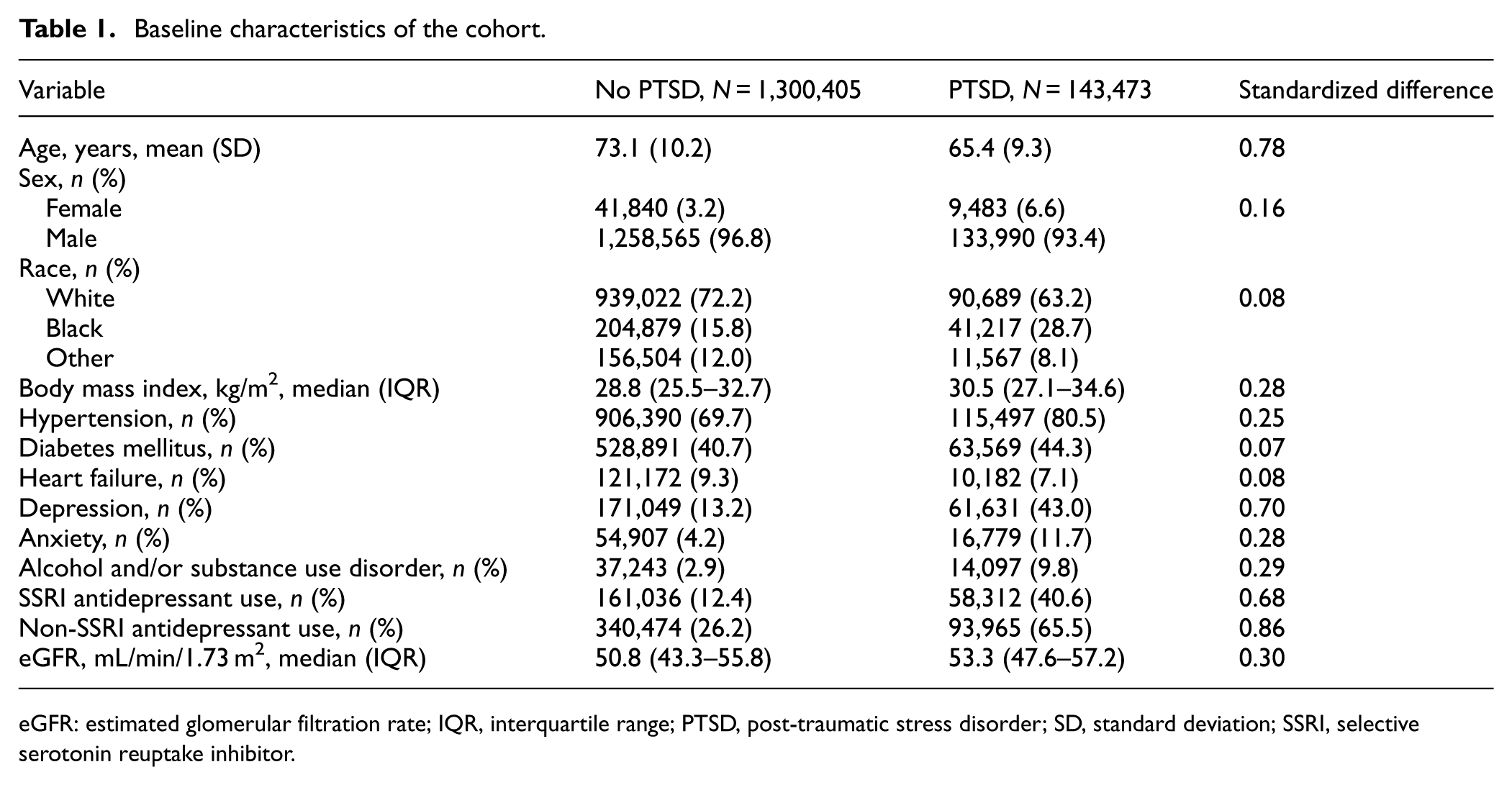
eGFR: estimated glomerular filtration rate; IQR, interquartile range; PTSD, post-traumatic stress disorder; SD, standard deviation; SSRI, selective serotonin reuptake inhibitor.
Associations of cardiovascular risk factors with PTSD
In multivariable models, younger age, Black race, hypertension, depression, anxiety, alcohol, and/or substance use disorder, non-SSRI antidepressant use, and higher eGFR were associated with increased odds of PTSD in both men and women (Figure 1). SSRI antidepressant use was associated with PTSD among men but not women. Heart failure and diabetes mellitus were associated with a lower odds of PTSD among both men and women Veterans. There were significant interactions by sex, such that Black race, hypertension, depression, non-SSRI antidepressant use, and eGFR were more strongly associated with PTSD among men than women, and alcohol and/or substance use was more strongly associated with PTSD among women than men (interaction p < 0.001 for each).
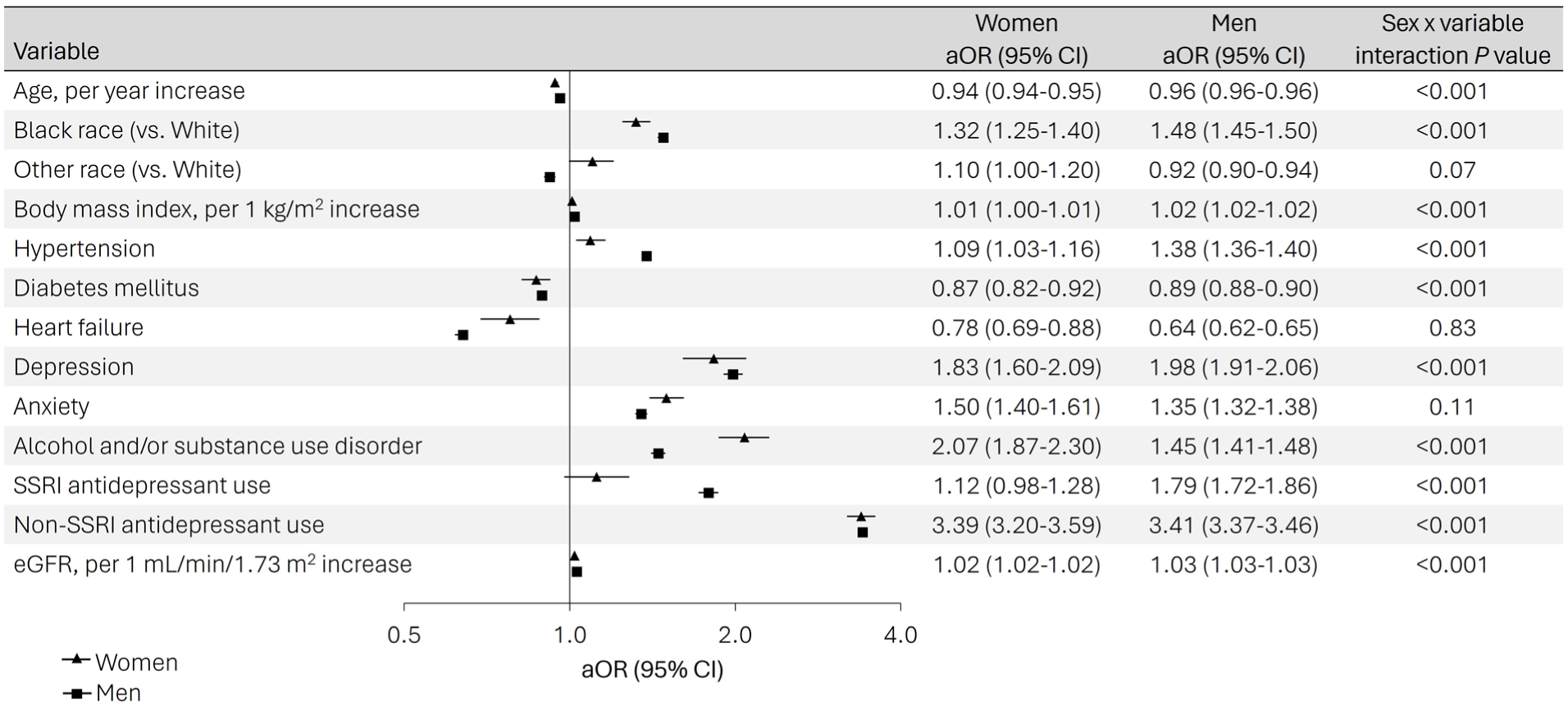
Factors associated with PTSD differed between men and women with CKD.
Discussion
In this national sample of Veterans with non-dialysis CKD stages 3–5, PTSD was common and associated with multiple cardiovascular risk factors. Men and women Veterans had important differences in their cardiovascular risk profiles and the associations of demographic characteristics, comorbid medical and mental health conditions, and medication use with PTSD. This suggests that the relationship between PTSD and cardiovascular disease may differ markedly between men and women with CKD.
We identified that the prevalence of PTSD was approximately 10% in the entire cohort, but was much higher among women than men. The prevalence of PTSD in this study was slightly lower than estimates of 14.3% in the VA primary care population. 30 The association of PTSD with younger age and higher eGFR may explain the slight differences in these estimates, as a sample with CKD selects for an older population with lower eGFR than would be found in the primary care setting. Although the prevalence of PTSD among people with CKD has not been a primary focus of prior studies, one prospective cohort of 272 Veterans with CKD stages 2–5 reported PTSD in 9 (3.3%) as ascertained by the Mini International Neuropsychiatric Interview. 6 However, it is unclear whether prospective studies underrepresent people with PTSD who might be less likely to consent for participation to avoid confronting memories of traumatic events. On the other hand, the use of diagnosis codes to identify PTSD can lead to misclassification if PTSD is present but unaccounted for in the codes selected for clinical encounters. This is particularly of concern in people with higher overall medical complexity and morbidity; if a person’s clinical visits were focused on other active health problems, their clinicians may have been less likely to list diagnosis codes for PTSD.
The independent associations of demographic and clinical characteristics, including both traditional (e.g., age and hypertension) and non-traditional (e.g., depression) cardiovascular risk factors with PTSD differed between men and women Veterans. These differences may be attributable to known sex differences in trauma exposure (particularly military sexual trauma), coping mechanisms, comorbid anxiety or depression, and neurohormonal signaling.23,31,32 These differences support that the pathophysiology of PTSD and its relationship to cardiovascular health may differ between men and women. SSRI use was associated with PTSD among men but was not associated with PTSD among women. This is likely because of higher SSRI use among women for indications other than PTSD, such as depression.
We also found that diabetes mellitus and heart failure were associated with a lower odds of PTSD. This is most likely an artifact of identifying prevalent PTSD by the use of at least two PTSD diagnosis codes within 1 year prior to meeting criteria for CKD. Individuals who had multiple medical comorbidities or were generally more medically complex may have been less likely to be actively treated for PTSD if their clinicians’ attention was mostly geared toward adjusting their glucose-lowering medications or guideline-directed medical therapy.
This study has several strengths. The identification of CKD was based on laboratory values and was therefore consistent with guideline-based definitions and did not rely on diagnosis codes. The sample size was large. Although the cohort was male-predominant, it still included 51,323 women, so it was adequately powered to assess the relationships of interest in subgroups by sex. This study also has important limitations. Veterans have a high risk of PTSD related to their military service, so these findings may not be generalizable to other populations. The use of diagnosis codes to identify comorbidities is inherently limited. Some Veterans may receive some of their medications outside of the VA system.
In summary, we showed that PTSD was prevalent among approximately 10% of Veterans with CKD, with a much higher prevalence of 18.5% among women compared to 9.6% among men. Cardiovascular disease risk factors were differentially associated with PTSD among men and women. Future studies should stratify by sex when evaluating associations of PTSD with cardiovascular risk and outcomes in people with CKD.
Footnotes
Acknowledgements
The opinions expressed reflect those of the authors and not necessarily those of the Department of Veterans Affairs, NIH, or the U.S. government. Support for VA/CMS data provided by the Department of Veterans Affairs, VA Health Services Research and Development Service, VA Information Resource Center (Project Numbers SDR 02-237 and 98-004).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: LPG is supported by a VA Clinical Sciences Research and Development Career Development Award (IK2CX00 2368). SDN is also supported by NIH/NHLBI K24 HL161414-01A and the Garabed Eknoyan MD Endowed Professorship. This work was supported in part by the Houston VA Health Services Research and Development Center for Innovations grant (CIN13-413).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: LPG receives research funding from Calliditas Therapeutics and the Texas Health Resources Foundation outside of the submitted work. SDN reported receiving personal fees from ACI clinical, AstraZeneca (data safety and monitoring board), Bayer, Boehringer Ingelheim/Eli Lilly and Co, GSK, Intercept (event adjudication committee), Vertex (event adjudication committee), and Vifor; receiving grants from Keryx; and receiving research funding from the Department of Veterans Affairs Health Services Research and Development and Calliditas Therapeutics outside the submitted work. The remaining authors have nothing to disclose.
Data availability statement
A data use agreement is required for accessing and using data from the Veterans Health Administration. Our data use agreements do not permit us to share patient-level source data derivatives with individuals and institutions not covered under the data use agreements. The databases used in this study are accessible to other researchers by contacting the data providers and acquiring data use agreements/licenses.